[SPECON] Burn Rehabilitation
1/154
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
155 Terms
What is the most common cause of burns in children (1-5 years)?
Scalds and hot liquids
What is the most common cause of burns in adolescents and adults?
Accidents from hot liquids
What population has the highest prevalence of burns?
Males between 16-40 years old
Aside from the age groups already mentioned, what is the leading cause of burns in other age groups?
Fires in homes and structural dwellings
What is the most common cause of death associated with burns?
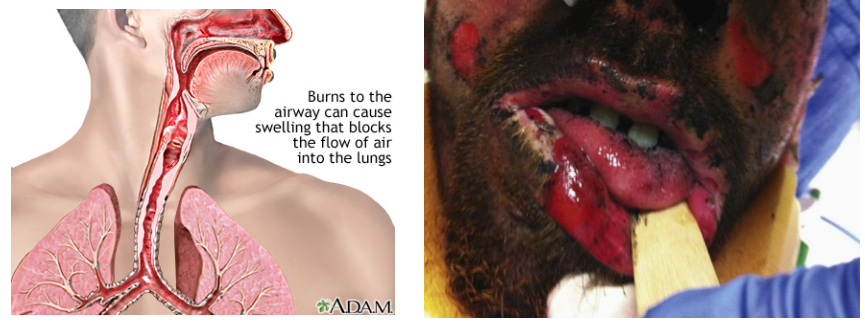
Inhalation injury
What are the percentages of the age groups most commonly involved with burns?
<1 year
2-14 years
25-44 years
<1 year (24%)
2-14 years (25%)
25-44 years (25%)
What type of burns are most common?
Scale burns (43%)
When were majority of wounds commonly treated?
24 hours of the injury (89%)
What is the fatality rate of burns?
9%
What is the most common cause of death due to burns?
Multiple organ system disruption (MOSD) (40%)
*inhalation still top
What are the significant factors associated with mortality rate due to burns?
%TBSA (total body surface area)
Inhalation injury
Involvement of the head, lower extremity, and perineum
What is the relationship between %TBSA and mortality rate?
Increased TBSA = increased mortality rate
Among the significant factors associated with mortality in burns, which is the worse one?
%TBSA (total body surface area)
Inhalation injury
Involvement of the head, lower extremity, and perineum
Inhalation injury
What are the risk factors for burns?
Occupations that increase exposure to fire
Poverty, overcrowding, and lack of safety measures
Placement of young girls in household roles such as cooking and care of small children
Underlying medical conditions including epilepsy, peripheral neuropathies, and physical and cognitive disabilities
Alcohol abuse and smoking
Easy access for chemicals used for assault (such as acid violence attacks)
Use of kerosene as a fuel source for non-electric domestic appliances
Inadequate safety measures for liquefied petroleum gas and electricity
This is the usual fuel source of low-income households that act as a risk factor for burns.
Kerosene
Read: In the Philippines (2010-2012):
883 fires
43% of fires occurred in the first 4 months of the year (summer time)
Highest incidence occurs at 12:01 - 3:00 am (everyone was asleep)
What was the most common cause of fires in the Philippines in 2010-2012?
Faulty electrical wiring and neglected open flames
What areas were most commonly affected by fires in the Philippines in 2010-2012?
Residential areas
What was the worst fire in Philippine history?
Ozone Disco Fire

This is the largest organ of the body.
Follow Up Question: What are the functions of this organ?
Skin
Protective shield against heat, light, injury, and infection
Regulation of body temperature
Storage of fat and water (can lead to dehydration)
Prevents entry of bacteria
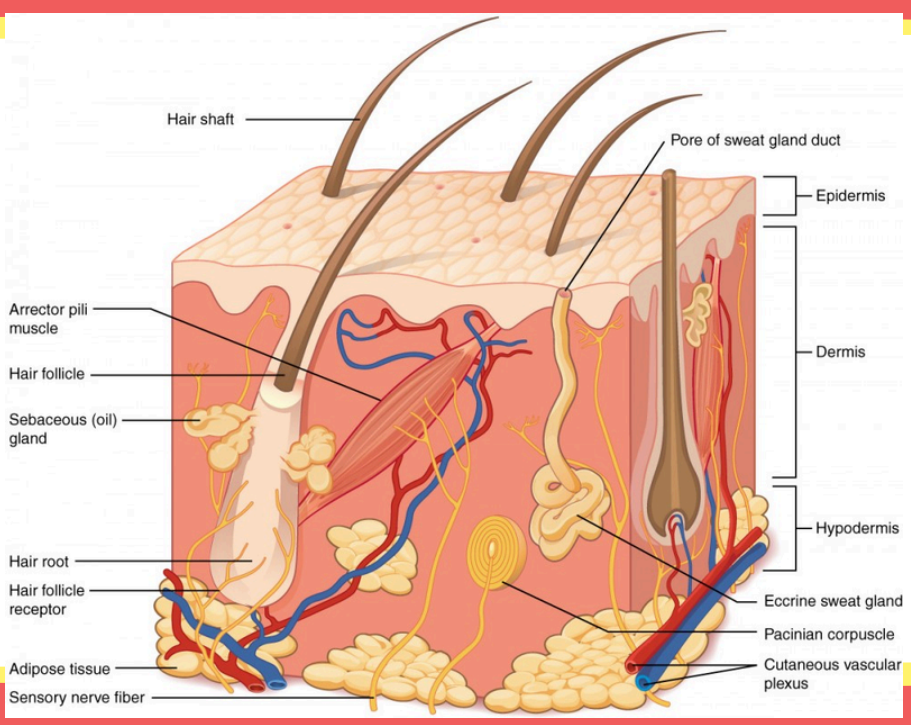
This structure secretes sebum to lubricate and waterproof the skin and hair.
Sebaceous (oil) gland
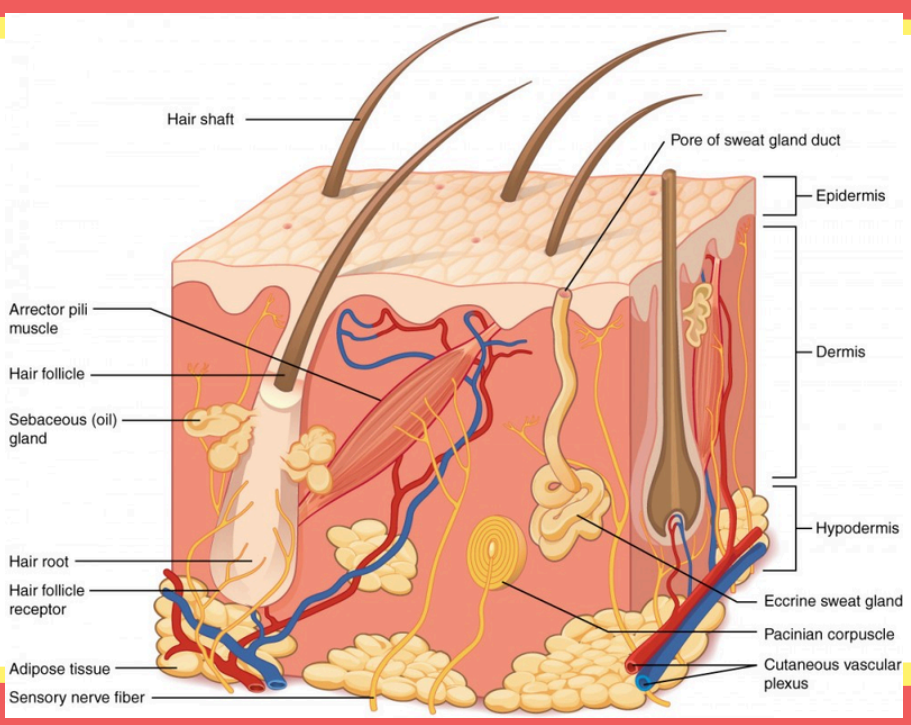
This produces sweat to cool the body down through evaporation.
Eccrine sweat glands
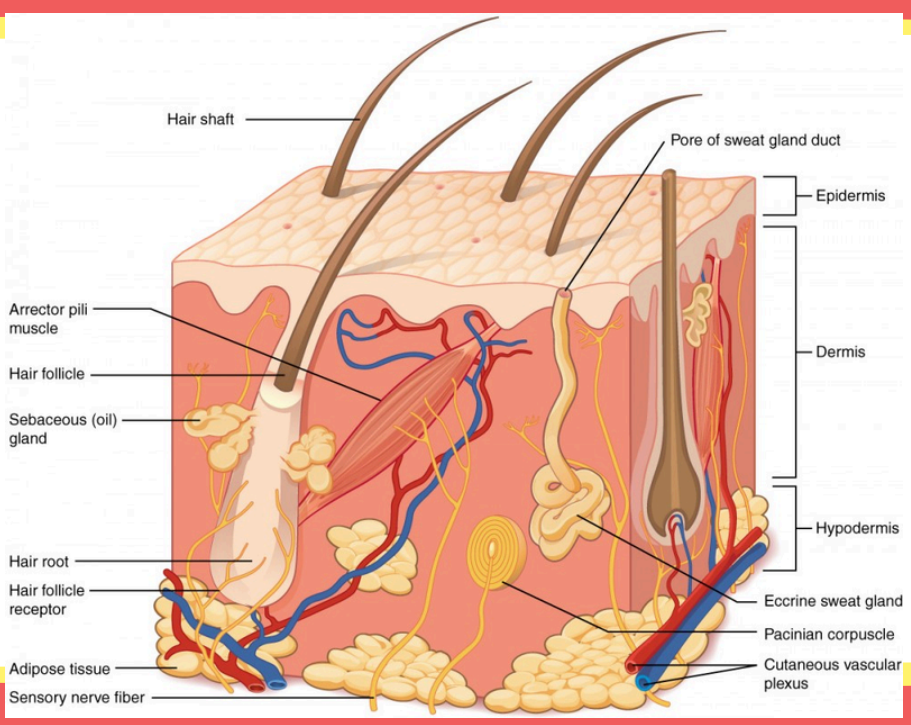
These small muscles that pull hair upright to create "goosebumps".
Arrector pili muscle
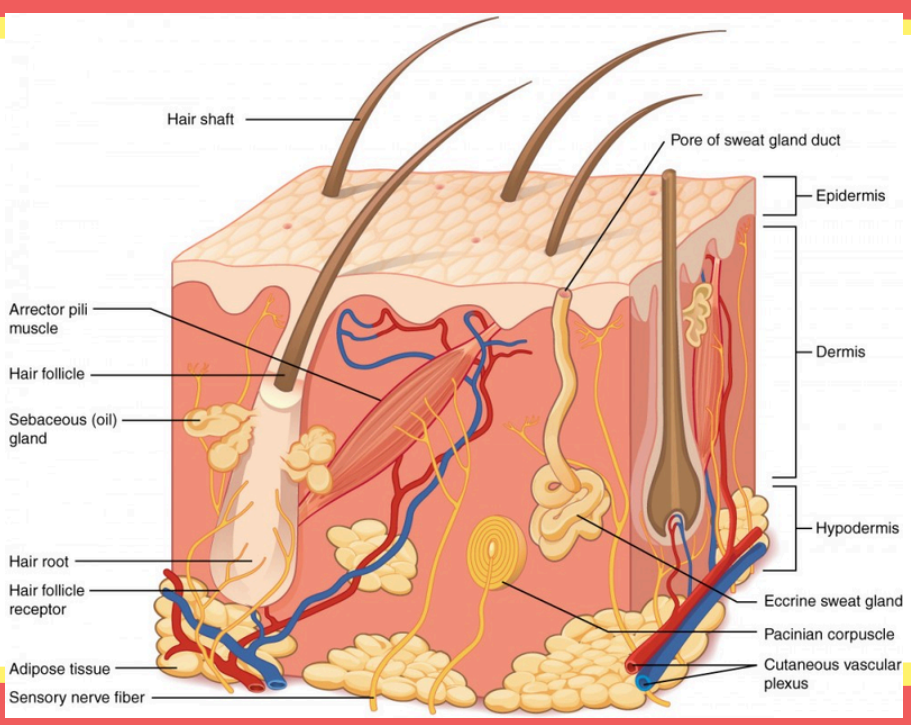
These are sensitive nerve endings that detect when a hair moves.
Hair follicle receptor
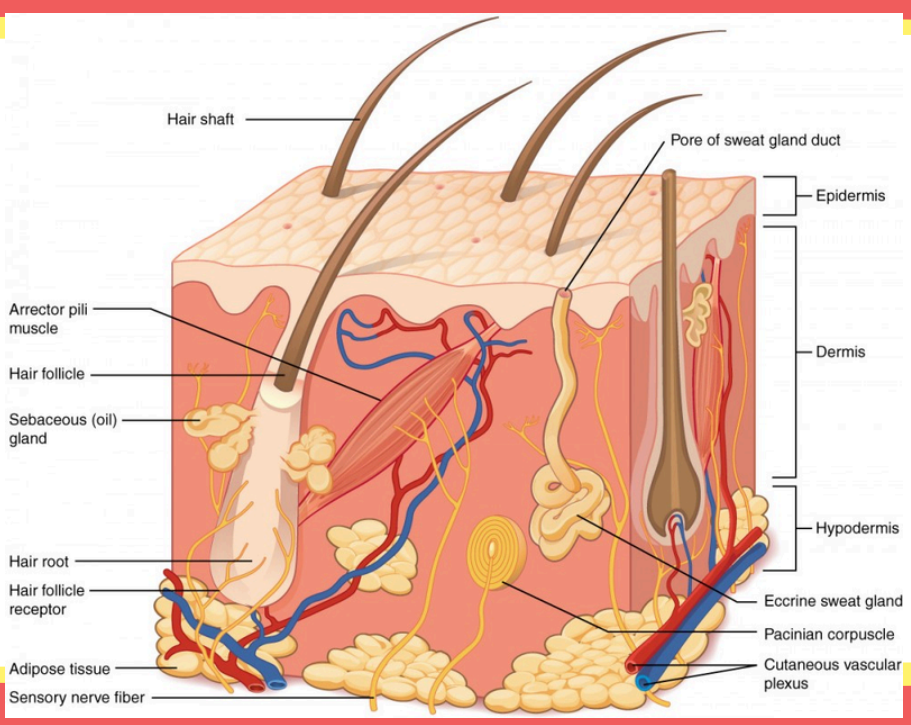
This is where the fatty tissue that stores energy and acts as a shock absorber is.
Adipose tissue
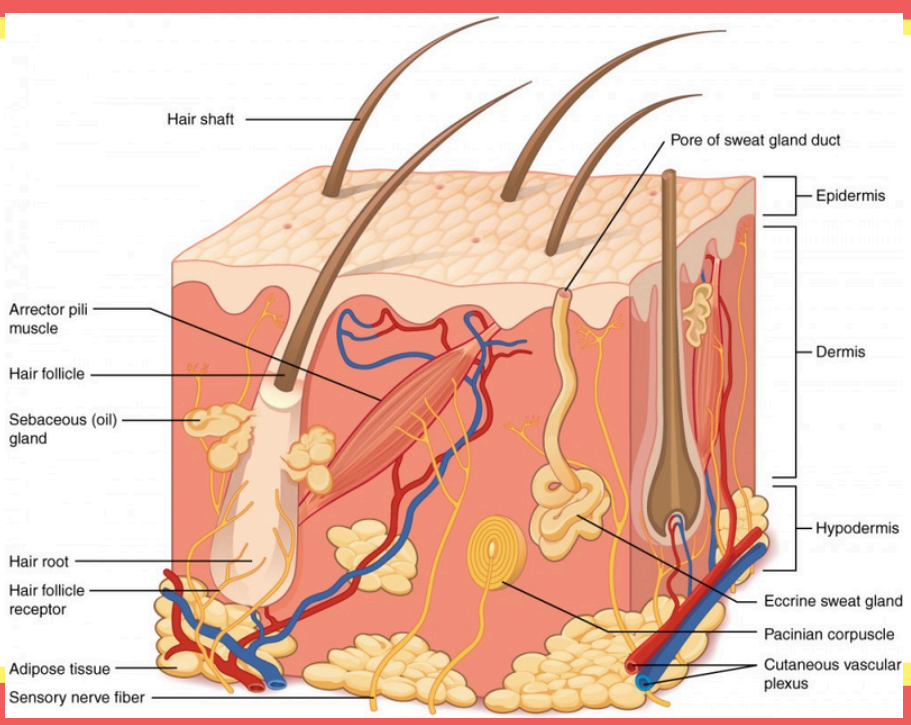
This is a network of blood vessels that supplies nutrients and helps regulate body temperature.
Cutaneous vascular plexus
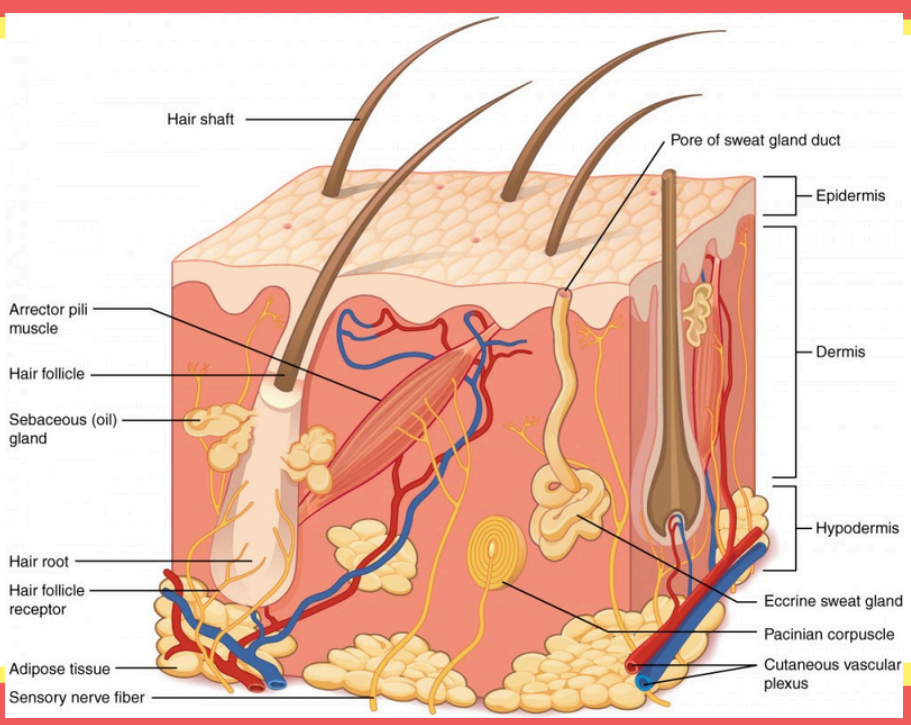
This is the opening on the surface where sweat is released.
Pore of sweat gland
This is the surface or outer layer of the skin that serves as a barrier between our body and the environment.
Epidermis
What are the layers of the epidermis?
Stratum corneum
Stratum lucidum
Stratum granulosum
Stratum spinosum
Stratum germinativum or stratum basale
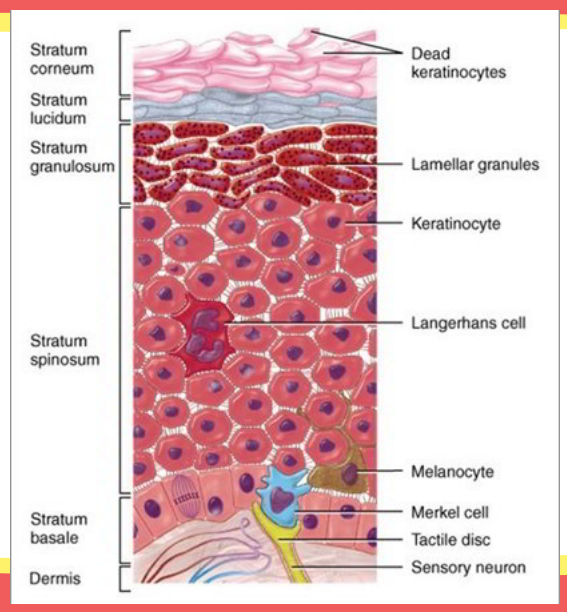
This is the layer of the skin where cells are produced.
Stratum germinativum or basale
This is the layer of skin beneath the epidermis.
Follow Up Question: How many times thicker is it than the epidermis?
Dermis
20-30 times thicker
The dermis is comprised of what and contains what?
Contains epidermal appendages
Comprised mainly of interwoven collagen and elastin fibers
What are the two layers of the dermis?
Papillary layer
Reticular layer
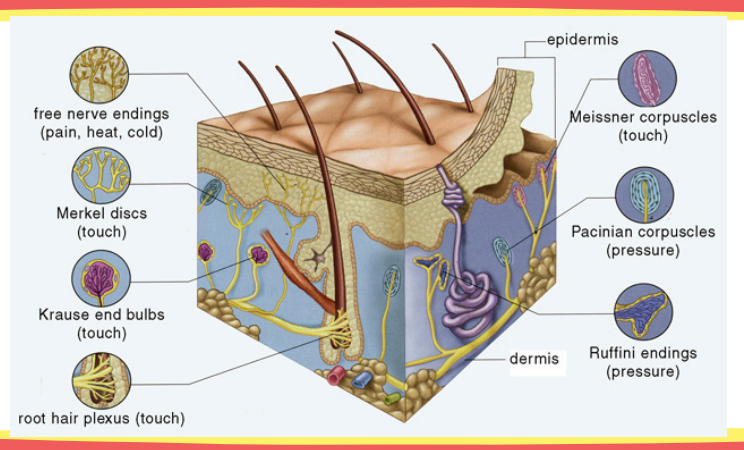
Identify its location and function: free nerve endings
Location: epidermis and dermis
Function: pain and itch
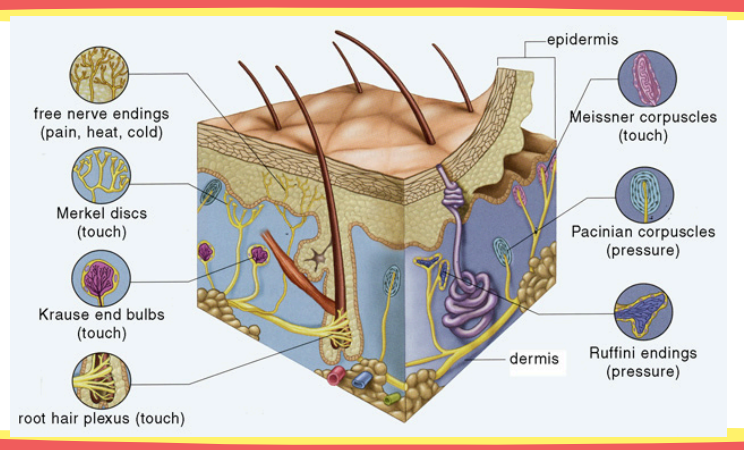
Identify its location and function: Merkel’s disks
Location: epidermis (stratum spinosum)
Function: touch
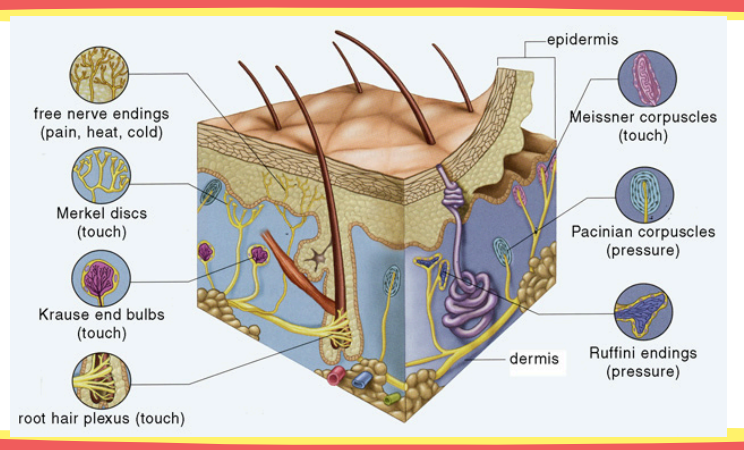
Identify its location and function: Meissner’s corpuscles
Location: papillary dermis
Function: touch
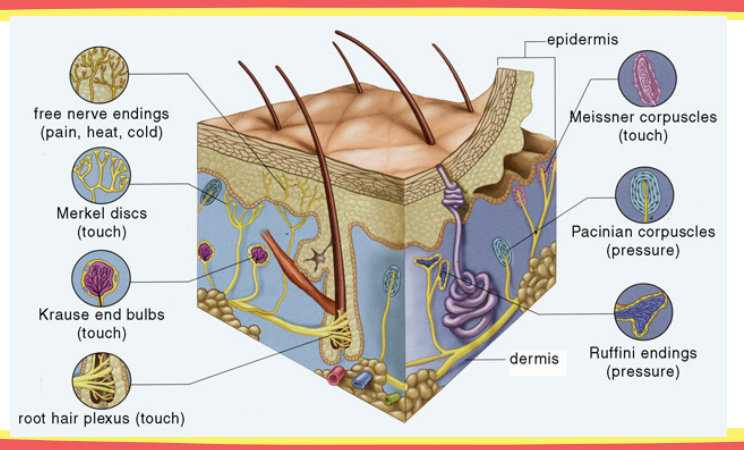
Identify its location and function: Ruffini’s endings
Location: papillary dermis
Function: warm receptors
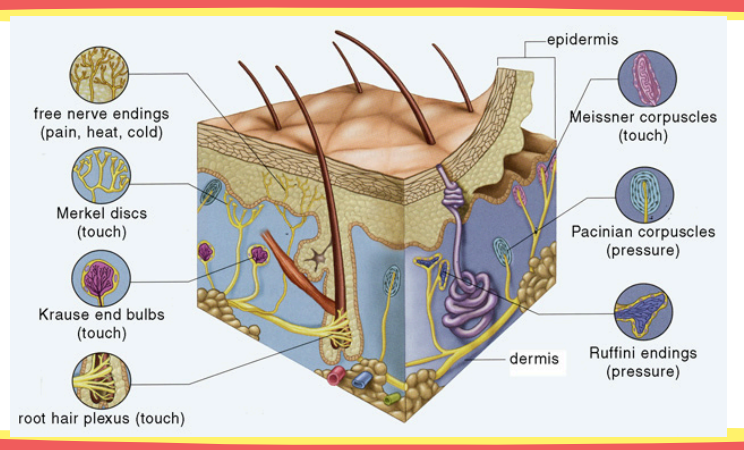
Identify its location and function: Krause end bulb
Location: papillary dermis
Function: cold receptors
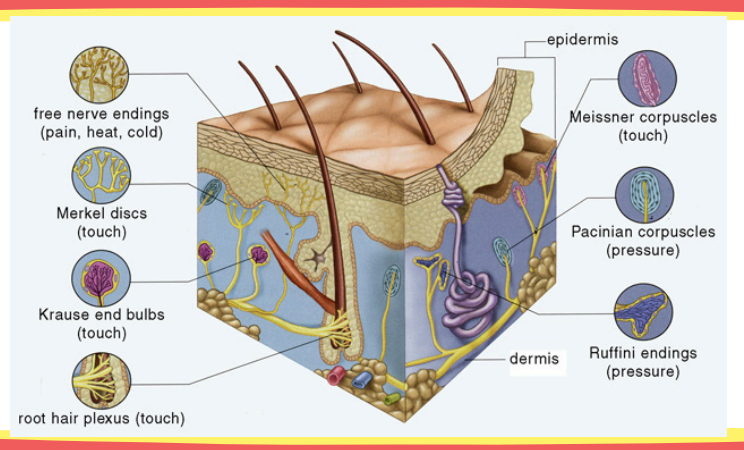
Identify its location and function: Pacinian corpuscles
Location: reticular dermis
Function: pressure and vibration receptors
This is the layer that lies below the dermis.
Follow Up Question: What does it consist of?
Hypodermis or subdermis
Loose connective tissue, elastin, and fat
What are the functions of the hypodermis?
Padding and insulation (because of the fat)
What is the mechanism of injury of burns?
Alteration of vascular integrity (injured cell releases its content, leading to the release of cytokines) → vasodilation occurs due to the release histamine, migrating of blood to the tissues → edema occurs and usually leads to LOM (which can also occur due to contractures)
What does skin destruction depend on?
Temperature
Length of time he was burned
Type of insult (flame, liquid, chemical, electrical)
Extremes of age — skin is affected easier
What are the types of burns?
Thermal burns
Electrical burns
Chemical burns
What are the usual causes of thermal burns?
Scalds, flame, and contact
This makes up 70% of burns in children and occurs due to spilling hot drinks or liquids, or hot water in baths.
Follow Up Question: How deep are the burns that this lead to?
Scalds
Causes superficial to superficial thickness burns

This makes up 50% of adult burns and is associated with an inhalation injury and other concomitant trauma.
Follow Up Question: How deep are the burns that this lead to?
Flame
Deep or full thickness

The depth of heat injury in contact burns depends on what factors?
Follow Up Question: How deep are the burns that this lead to?
Degree of heat exposure and depth of heat penetration
Deep dermal or full thickness
This is the most devastating type of burn.
Electrical burns
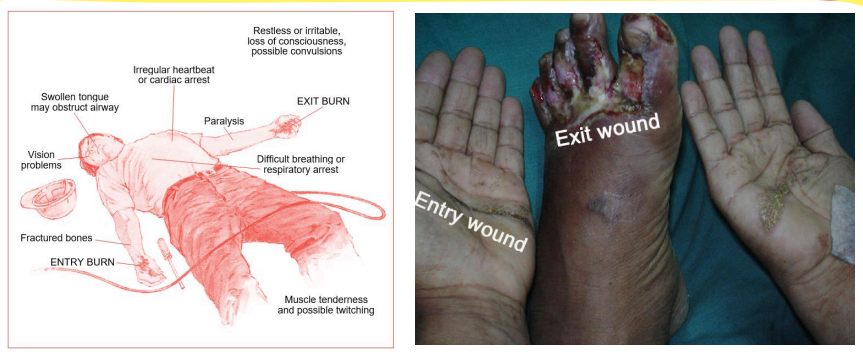
Fill in the Blanks: In electrical burns, an electrical current will travel through the body from one point to another, creating “______” or “______” points.
Follow Up Question: Electrical burns vary according to what?
In electrical burns, an electrical current will travel through the body from one point to another, creating “entry” or “exit” points.
Type of current
Intensity of the current
Area of the body that the current passes through
From most resistant to least resistant, what is the ranking of electrical resistance of the tissues of the body?
Bone
Cartilage
Tendon
Skin
Muscle
Blood
Nerve
[electricity usually travels where there is less resistance]
What are the two types of electrical burns and how many volts of current travel through the body?
Follow Up Question: What do the electrical burns lead to?
Low-voltage electrical burns (500-1000 volts of current)
V-fib
High-voltage electrical burns (greater than 1000 volts)
Apnea, deep tissue destruction, renal failure
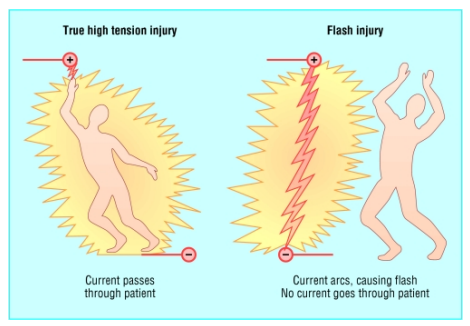
Differentiate a true from a flash high-voltage electrical burn.
True — electricity really went through the patient
Flash — only happened beside the patient
In electrical burns, this often results in amputation.
Follow Up Question: What is most commonly affected or amputated?
Extensive muscle and soft tissue necrosis
UE most common, usually the (R) UE
In high voltage electrical burns, these problems may not be present initially but may occur late after.
PNS and CNS problems
What are the complications associated with electrical burns due to being struck by lighting?
Myelopathy and encephalopathy
Sensorineural and mechanical hearing loss

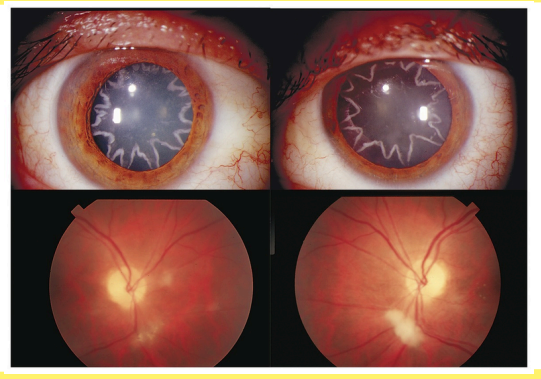
What are the ocular complications associated with electrical burns?
Cataracts
Macular holes
What are the cardiac manifestations of electrical burns?
Immediate cardiac arrest
Pseudo infarction
Myocardial ischemia without necrosis
Dysrhythmia
Conduction abnormalities
Acute hypertension
Nonspecific ECG abnormalities
Sinus tachycardia
What are other manifestations of electrical burns?
Diaphragm paralysis
Inhibition of the breathing centers in the midbrain
Extensive fluid loss
Loss of consciousness
Impaired recall and PTSD
Blood clotting
Compartment syndrome
Rhabdomyolysis
This occurs secondary to injured muscles, leading to increased pressure inside the extremity.
Compartment syndrome
This condition is a serious, potentially fatal condition involving rapid skeletal muscle breakdown, releasing toxic contents like myoglobin into the bloodstream, which causes kidney damage.
Follow Up Question: How is it treated?
Rhabdomyolysis
Treated through dialysis or increasing fluid intake
These usually occur as a result of an industrial accident, but it may occur with household chemical products.
Chemical burns
Which one more commonly causes burns? Alkali or acidic products?
Alkali products

These are one of the leading causes of death, accounting for more than half of the burn-related deaths per year.
Follow Up Question: How are they classified?
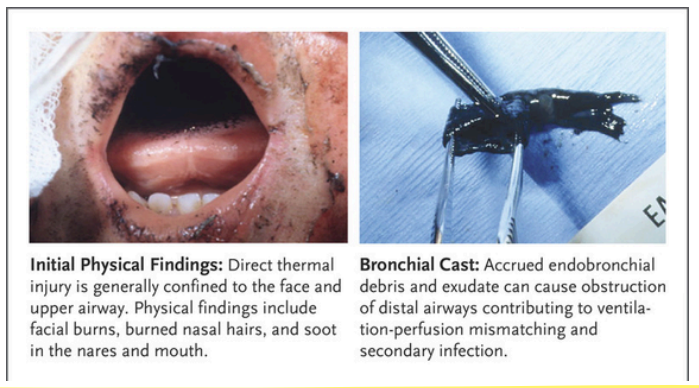
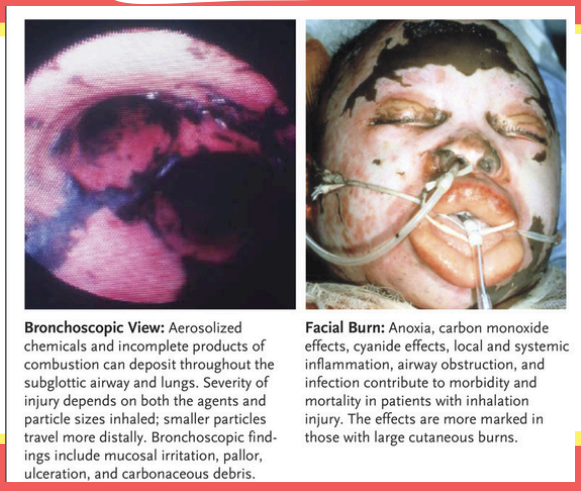
Inhalation injuries
Carbon monoxide poisoning, heat, or smoke inhalation injuries
What are the signs of inhalation injuries?
Facial burn
Singed nasal burn
Harsh cough
Hoarseness
Abnormal breath sounds
Respiratory distress
Carbonaceous sputum — black sputum
Hypoxemia
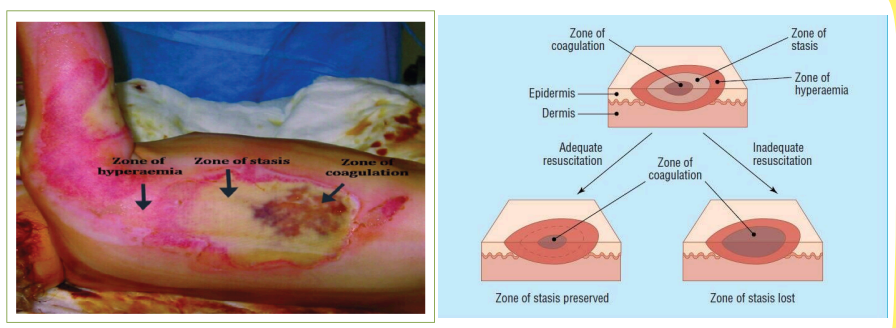
What are the three zones of local response?
Zone of coagulation
Zone of stasis
Zone of hyperemia
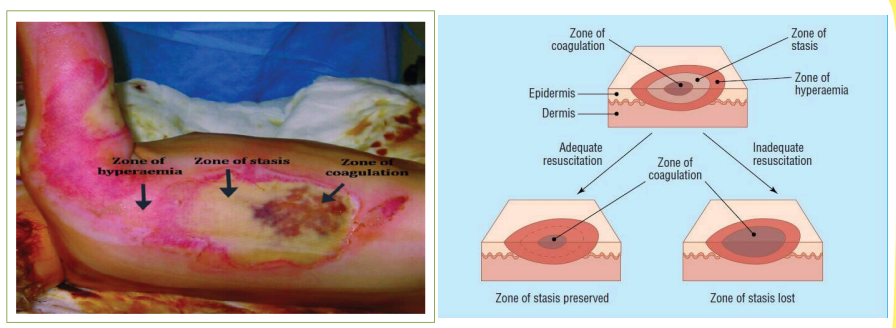
This zone occurs at the point of maximum damage and is characterized by irreversible tissue loss.
Zone of coagulation
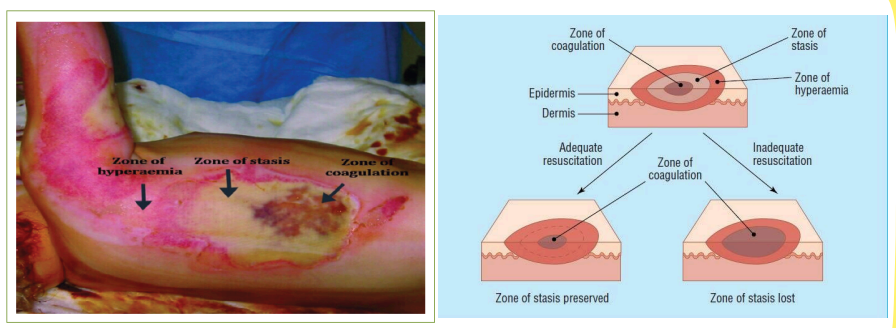
This zone is characterized by decreased tissue perfusion.
Follow Up Question: What is the goal of this zone?
Zone of stasis
To increase perfusion
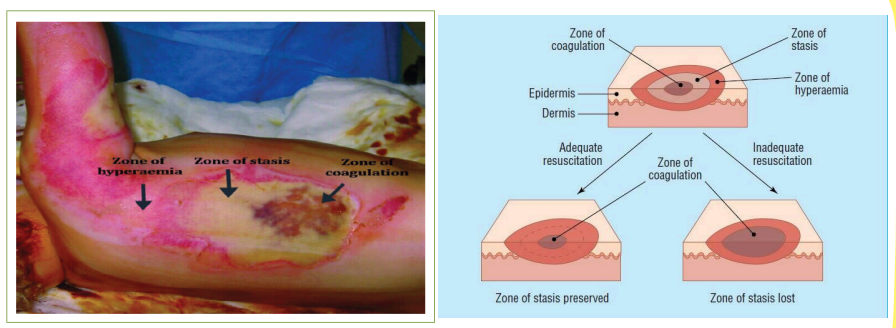
This is the outermost zone, where the tissue will recover unless there is severe sepsis.
Zone of hyperemia
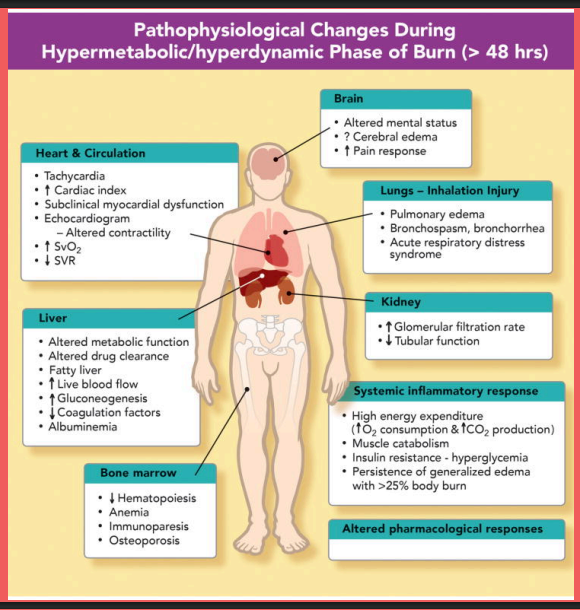
Read: Pathophysiological changes during hypermetabolic/hyperdynamic phase of burn (>48 hr)
What is the old classification of burns?
First degree
Second degree
Third degree
Fourth degree
Identify the classification based on the old classification:
Superficial injury
Red and sometimes painful
Follow Up Question: Until what layer is the extent of cell damage?
First degree
Epidermis
Identify the classification based on the old classification:
Skin may be red and blistered and swollen
Very painful
Follow Up Question: Until what layer is the extent of cell damage?
Second degree
Epidermis and parts of the dermis
Identify the classification based on the old classification:
Whitish, charred, or translucent
Follow Up Question: Until what layer is the extent of cell damage?
Third degree
Epidermis and dermis
What sensation is lost in third degree burns?
Pin prick sensation on the burned area (due to affected free nerve endings)
Identify the classification based on the old classification:
Deep and potentially life-threatening
Follow Up Question: Until what layer is the extent of cell damage?
Fourth degree
Skin and underlying tissues
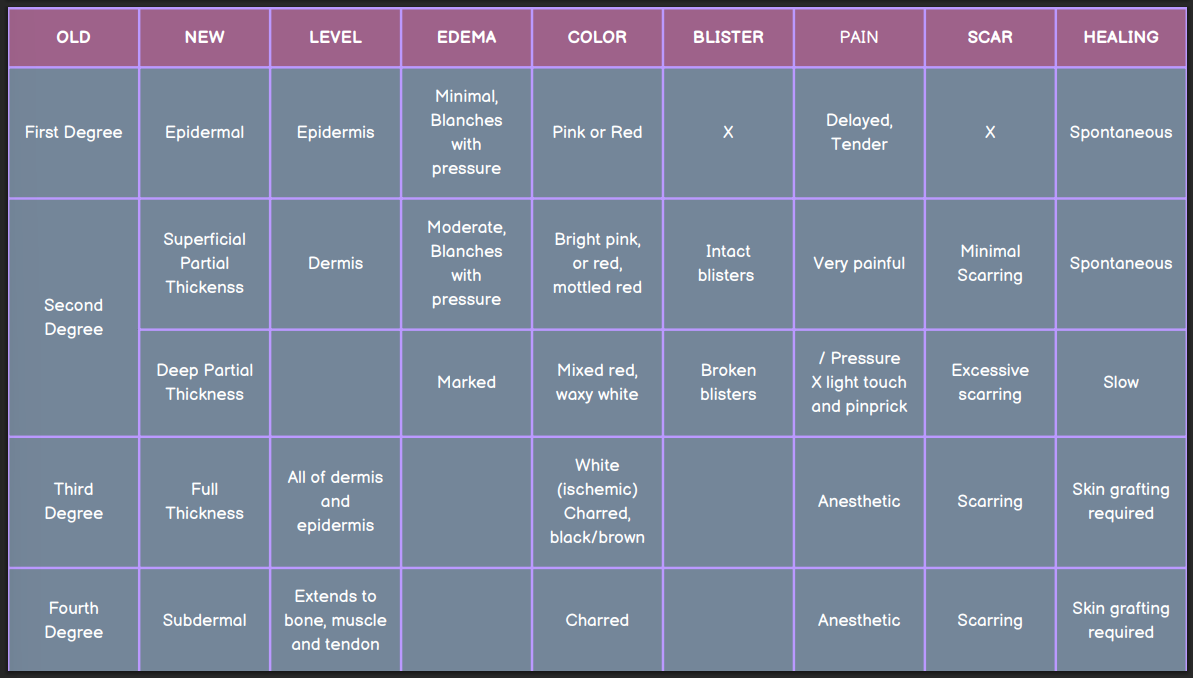
What is the new classification of burns?
Epidermal
Superficial partial thickness
Deep partial thickness
Full thickness
Subdermal
Identify the classification based on the new classification:
Skin appears to be red or erythematous
Dry surface
Absent blisters
Minimal edema
Follow Up Question: Until where is the cell damage?
Epidermal
Epidermis

Fill in the Blanks: In epidermal burns, there is a ______ in the development of pain.
Follow Up Question: When does it peel off and desquamates and how is the healing and scar tissue formation?
In epidermal burns, there is a delay in the development of pain.
3-4 days; spontaneous healing with no scar tissue
Identify the classification based on the new classification:
Intact blisters
Blanching
Moderate erythema
Extremely painful
Follow Up Question: Until where is the cell damage?
Superficial partial thickness
Epidermis into the papillary layer of the dermis

How is the desquamation, healing, and scarring of superficial partial thickness burns?
Follow Up Question: How long does it take to completely heal?
Desquamation occurs due to topical agents, residual skin color occurs due to destruction of melanocytes, and minimal scarring
7-10 days
Identify the classification based on the new classification:
Most of the nerve endings, hair follicles, and sweat ducts are injured
Mixed or waxy white
Marked edema
Follow Up Question: Until where is the cell damage?
Deep partial thickness
Epidermis and papillary dermis with damage to the reticular layer
Deep partial thickness burns will have findings on the sensory test due to damage to the nerve endings. What sensations are diminished and what are spared?
Light touch or sharp/dull pressure; retains deep pressure
What is the main problem in patients with deep partial thickness burns?
Dehydration (large amount of evaporative water loss [15-20x])
How does healing and scarring occur and when does it heal in deep partial thickness burns?
Hypertrophic scar formation and re-epithelialization within 3-5 weeks if not infected
Identify the classification based on the new classification:
Presence of eschar
Follow Up Question: What is the extent of cell damage and what structures are destroyed and damaged?
Full thickness
Epidermal and dermal layers completely destroyed
Hair follicles are completely destroyed
All nerve endings are destroyed
Damage to the peripheral vascular system

This is a hard, parchment-like, black or brown covering of the area.
Eschar
Identify the classification based on the new classification:
Complete destruction of all tissue from the epidermis to the subcutaneous tissue
Follow Up Question: What does this occur due to?
Subdermal burn
Prolonged contact with a heat source or contact with electricity

When muscles and bones are burned in a subdermal burn, what are these subjected to?
Necrosis
What is the main implication of subdermal burns in terms of the patient’s safety?
No sensation
When is skin grafting required for burns?
In third and fourth degree burns.
Getting the total body surface area (TBSA) is more practical in the emergent triage of a patient with an acute burn injury. How do we get the patient’s TBSA?
Using the Rule of 9 — divide the body into areas of 9%
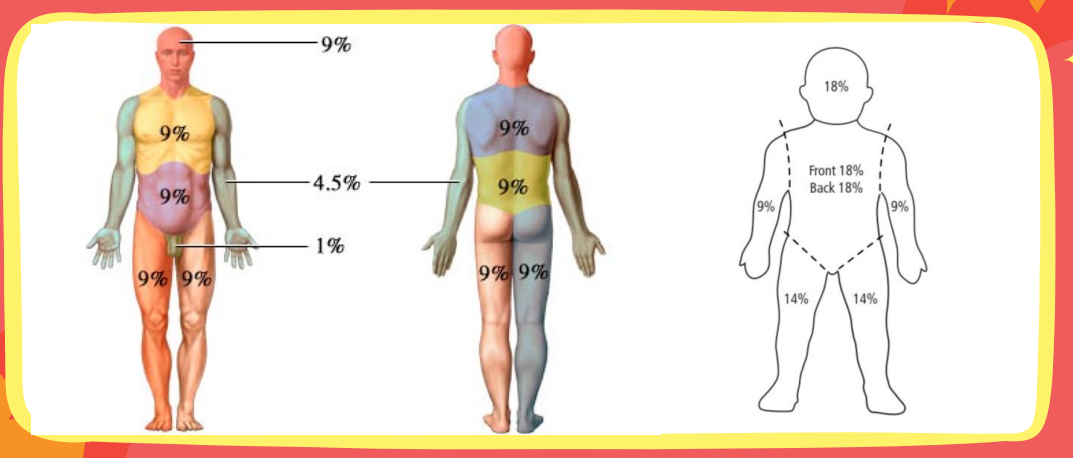
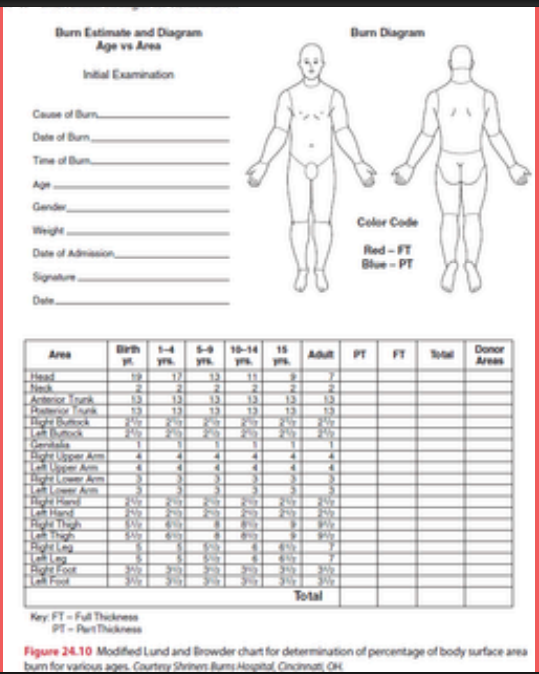
This tool divides the body into much smaller areas and gives the sizes that are associated with differently aged patients, accounting for a continuum age and to accommodate for growth of different body segments. It is a more accurate mean to determine the extent of burns.
Modified Lund and Browder Method
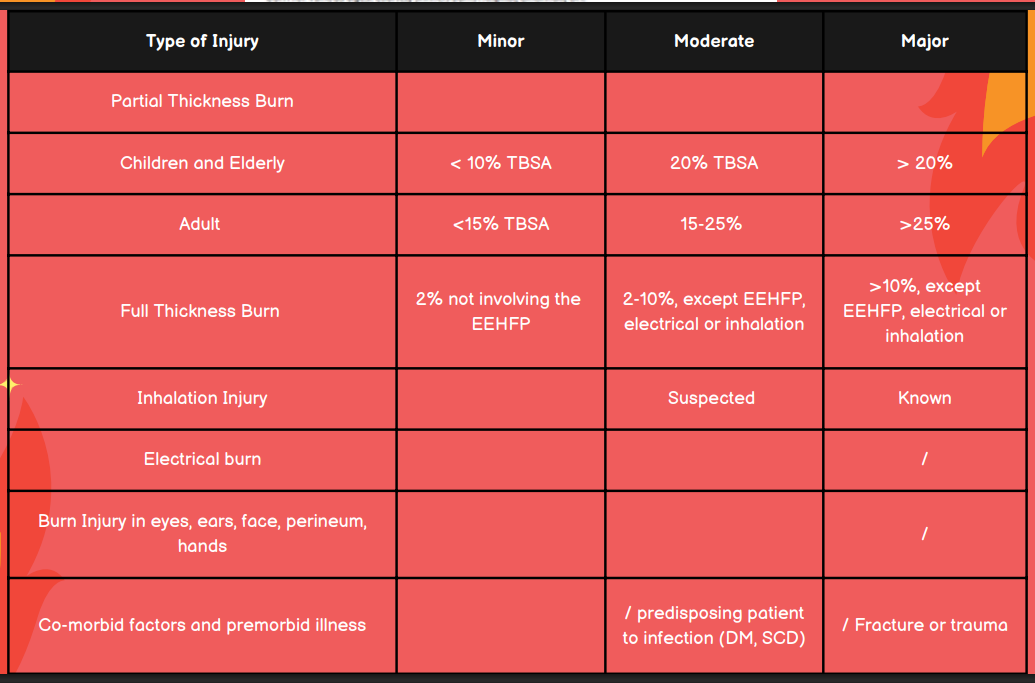
What is the TBSA for minor, moderate, and major burn injuries in children and elderly?
Minor: <10% TBSA
Moderate: 10-20% TBSA
Major: >20%
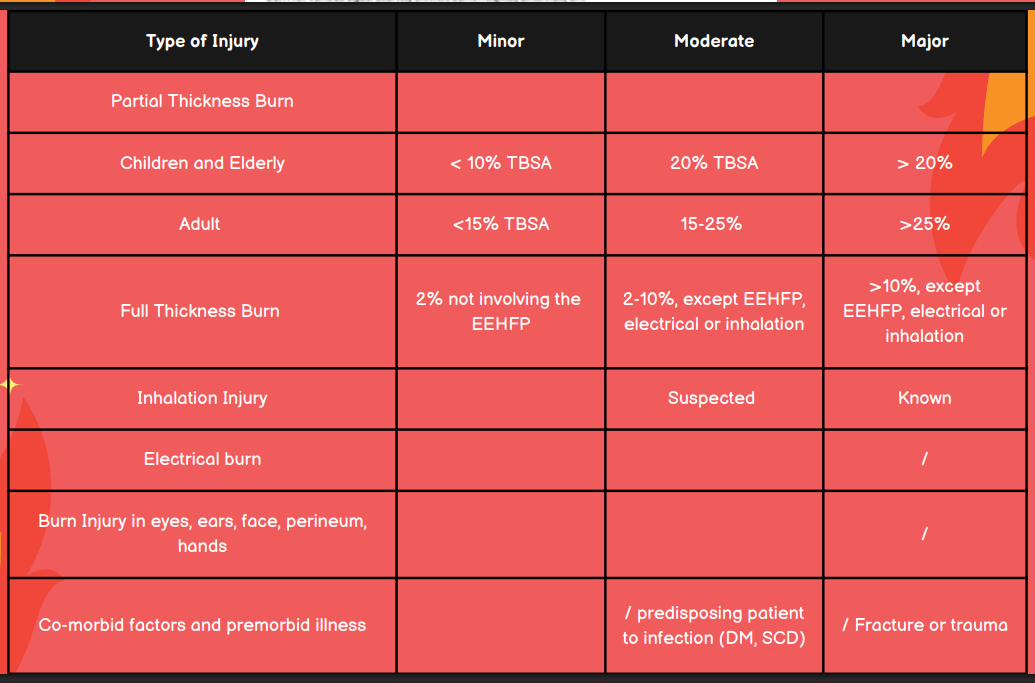
What is the TBSA for minor, moderate, and major burn injuries in adults?
Minor: <15%
Moderate: 15-25%
Major: >25%
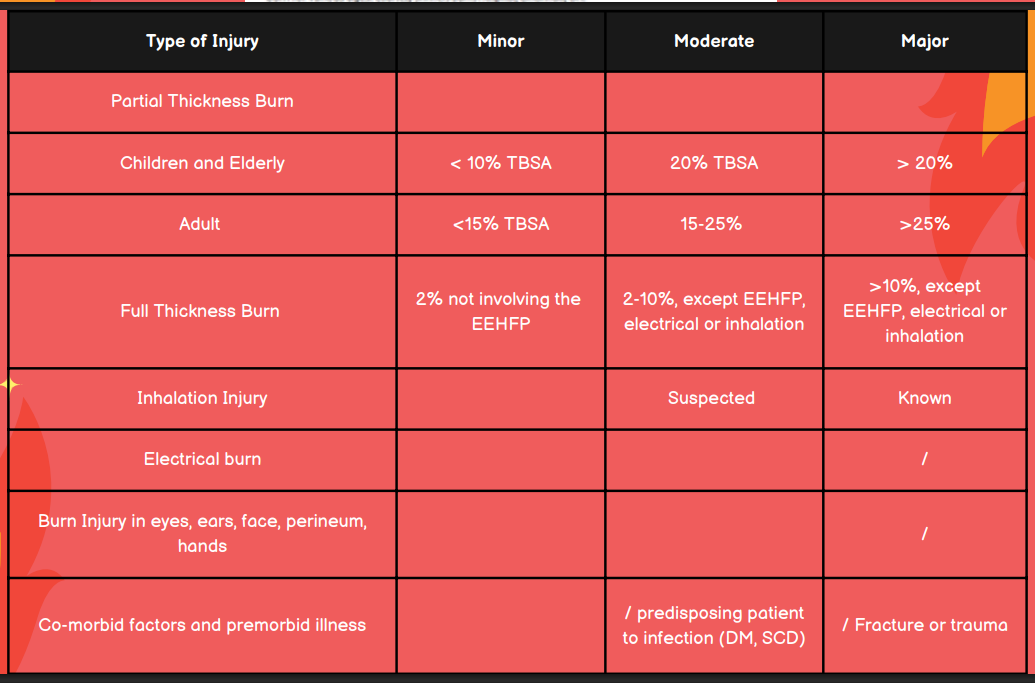
In terms of full thickness burns, differentiate a mild, moderate, and major burn injury.
Minor: 2% not involving the EEHFP
Moderate: 2-10%, except EEHFP, electrical, or inhalation
Major: >10% except EEHP, electrical, or inhalation
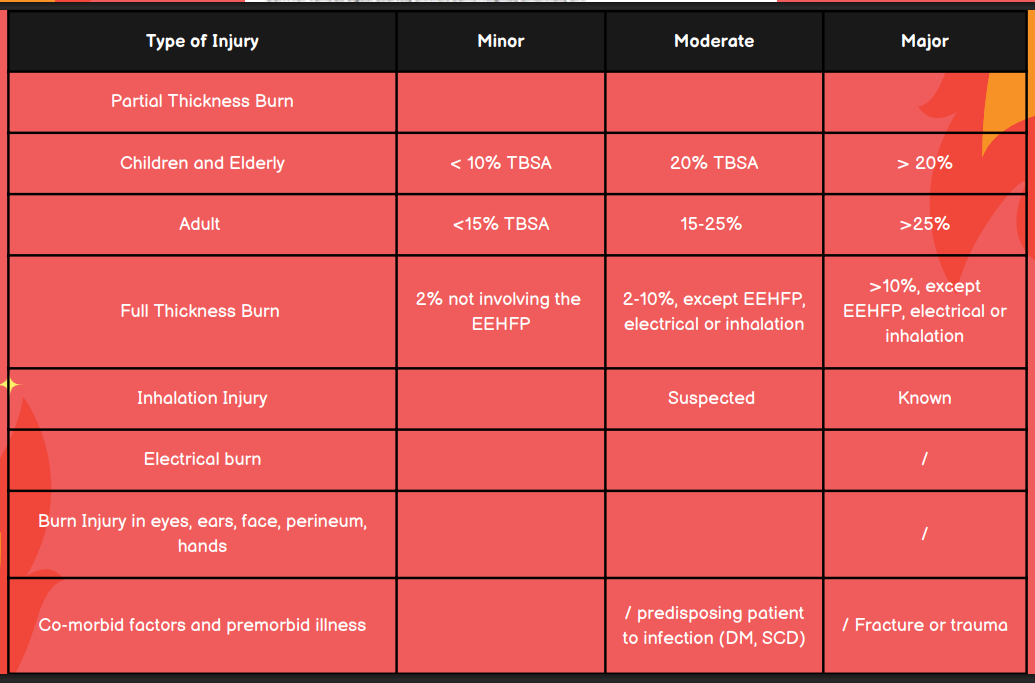
Is the burn injury minor, moderate, or major in a patient with suspected inhalation injury?
Moderate
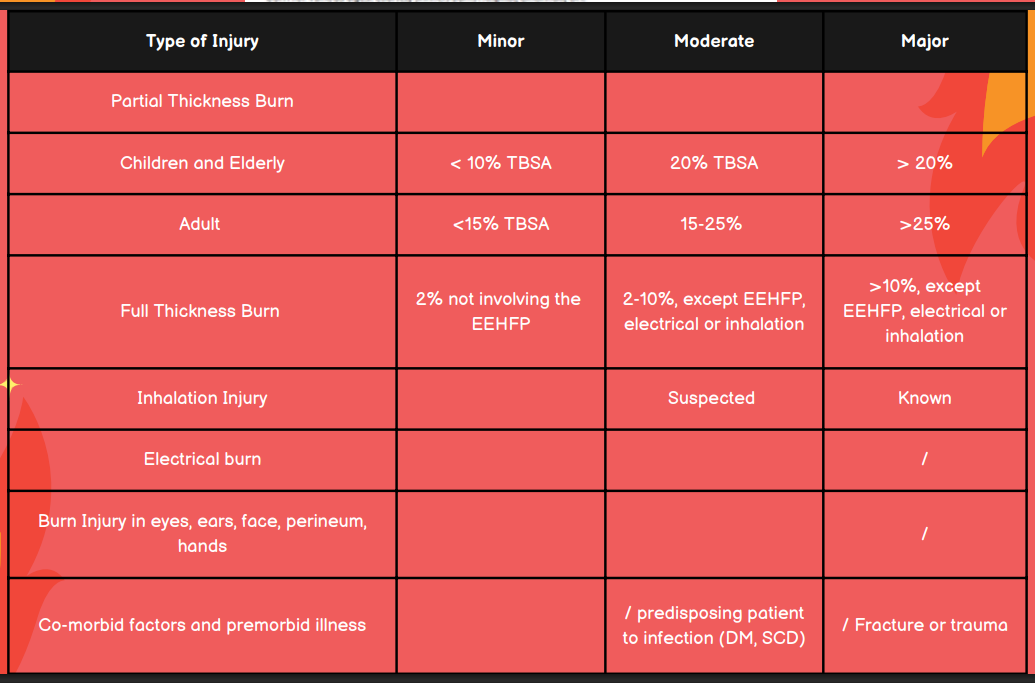
Is the burn injury minor, moderate, or major in a patient with known inhalation injury?
Major
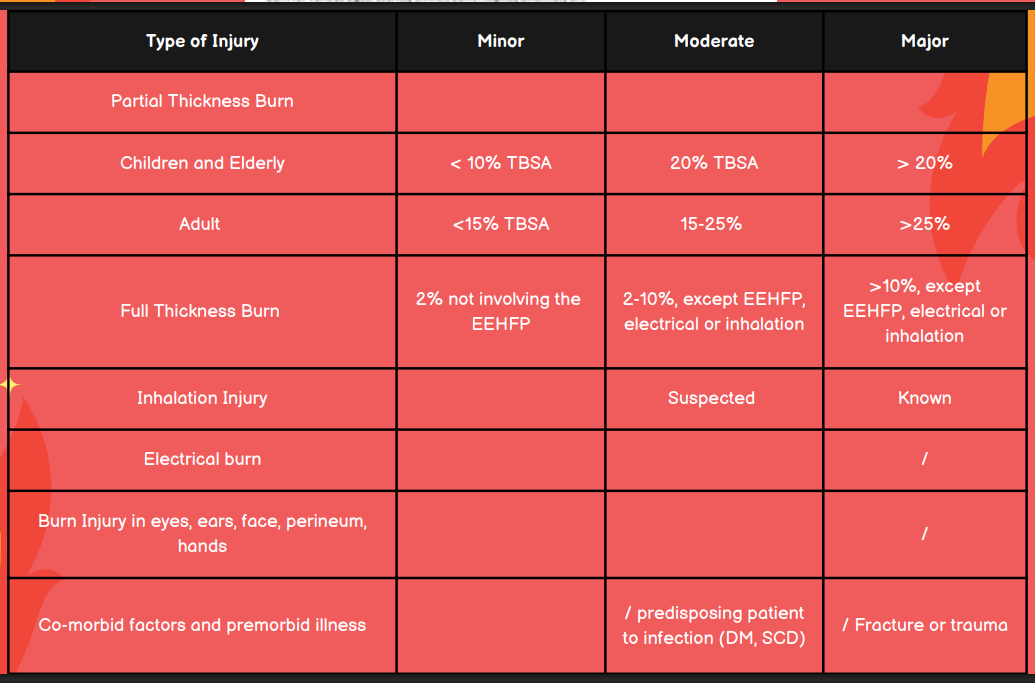
Is the burn injury minor, moderate, or major in a patient with an electrical burn?
Major
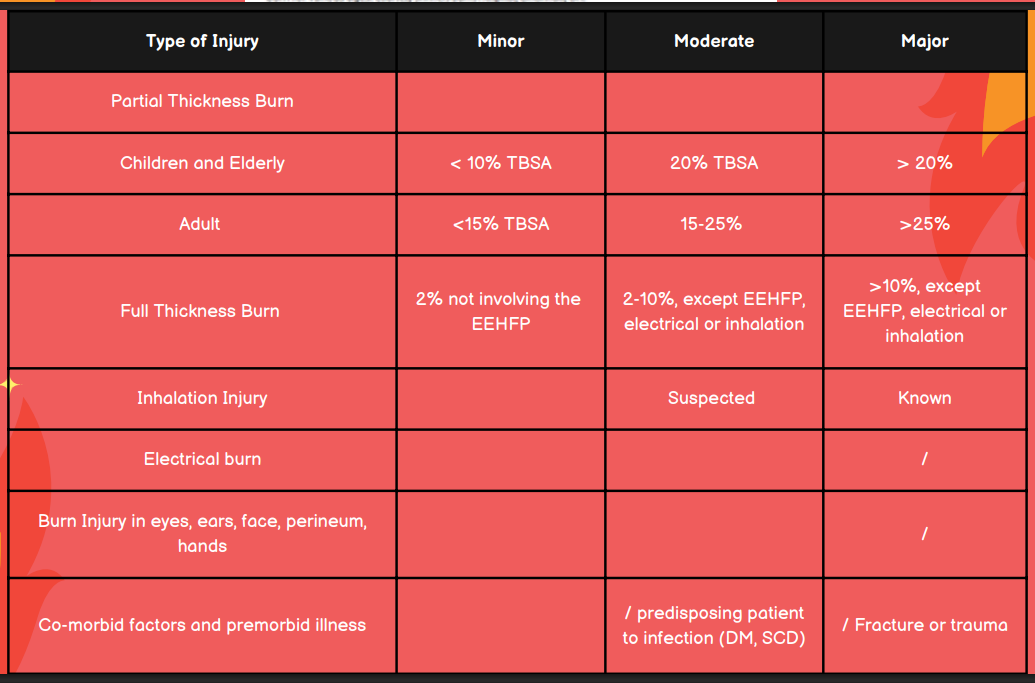
Is the burn injury minor, moderate, or major in a patient with burns in the eyes, ears, face, perineum, or hands?
Major