BOARD REVIEW PERIO
1/189
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
190 Terms
Gingiva
This provides a tissue seal around the tooth, and protects underlying structures.
stratified squamous epithelium
Gingival epithelium is a type of specialized ——————— ——————— epithelium.
Gingival margin
coronal boundary of the gingiva near the crown of the tooth
Biological width
The distance from the alveolar crest to the junctional epithelium. This includes the JE and connective tissue attachment to the tooth surface.
2mm
A least — mm of vertical space is needed for a resto to be successfully placed. If a resto is too close to the alveolar bone, it invades the biological width, and damage will occur to the periodontium.
Free gingiva
This is the unattached gingiva near the gingival margin.
Free gingival groove
Slight depression that separates the free (unattached) and attached gingiva. May not be visible in some patients. Not measured on the palate. Corresponds to the depth of the sulcus.
Attached gingiva
This is the portion of gingiva between the free gingival groove and the mucogingival junction. The tissue is connected to the cementum (of the root) and the periosteum of the alveolar bone. This is where oral pigmentation usually occurs if it is present. Generally widest in the facial aspect of max anteriors (3.5-4.5mm) and narrowest in the facial aspect of the mandibular premolars (1.8mm).
Mucogingival Junction (MGJ)
The apical boundary where the attached gingiva (coral pink and keratinized) meets the alveolar mucosa (red, smooth, shiny, and non-keratinized).
Gingival sulcus (pocket)
space between the lining of the free gingiva and the tooth surface where the probe is inserted.
Sulcular epithelium
This is the lining of the free gingival sulcus, the surface that faces the tooth/root. Extends from the crest of the gingival margin to JE. Consists of non-keratinized epithelium. The permeability of the non-keratinized tissue allows gingival crevicular fluid (GCF) to flow into the sulcus. GCF is always present but increases in disease.
Collagen
The fibres of the gingiva are composed mainly of ——————— and elastic fibres.
Transeptal
Fibres that run from the cementum of one tooth, over the alveolar crest, to the cementum of the adjacent tooth are called this. These fibres connect adjacent teeth to one another.
Alveogingival
Fibres that run from the alveolar crest to the gingiva are called:
These fibres attach gingiva to bone.
Dentogingival
These are the fibres that attach the gingiva to the tooth. They run from the cementum to the gingiva.
Periostogingival
These fibres run from the periosteum to the gingiva. They attach the gingiva to the bone.
Circular
These fibres encircle the tooth like a ring. They support the free gingiva.
Intergingival
—————————— fibres form a mesiodistal connection between teeth. These fibres, along with intercircular fibres, link adjecent teeth in the dental arch.
Interpapillary
These fibres are in papillae, they are coronal to transseptal fibres. They support the papillary gingiva.
Periodontal ligament (PDL)
This connects the tooth (cementum) to the alveolar bone of the tooth socket. It has 5 components; supportive, sensory, nutritive, formative, and resorptive. Has a rich supply of nerves and blood vessels. Fibroblasts are the most prominent cell. Sharpey's fibers are at the ends of the ————————- ——————— fibres embedded in the cementum and alveolar bone. Teeth that are accidentally exfoliated can be reimplemented into the socket of the damage to this is minimal. The fibre bundles of this are: alveolar crest fibre group, horizontal fibre group, oblique fibre group, apical fibre group, interradicular fibre group.
Alveolar crest fibre group
This is one of the 5 PDL fibre bundles: runs diagonally in a downward direction from the cementum to the alveolar crest. Their function is to resist horizontal movement of the tooth.
Horizontal fibre group
This is one of the 5 PDL fibre bundles: runs horizontally from cementum to the bone apical to the alveolar crest fibres. Its function is to resist horizontal pressure.
Oblique fibre group
This is one of the 5 PDL fibre bundles: runs diagonally in a downward direction from bone to cementum. Its function is to resist vertical pressure. This is the largest and most significant group of fibre bundles in the periodontal ligament.
Apical fibre group
This is one of the 5 PDL fibre bundles: extends from the apex of the tooth to bone. Its function is to resist large forces that pull the tooth out of the socket.
Interradicular fiber group.
This is one of the 5 PDL fibre bundles: extends from cementum in furcation area to interradicular septum of alveolar bone. Its function is to stabilize the tooth in its socket. These fibres are only present in multirooted teeth.
Cementum
This is the thin layer of mineralized tissue made of hydroxyapatite crystals (calcium phosphate) that covers the root of the tooth. Light yellow in colour. This is the area where the PDL connects the tooth to the bone. Resilient to pressure allows bone resorption without root resorption. Trauma and infection may thicken this layer of the tooth. Receives nutrients from the PDL. Contains no blood vessels or nerves. In most cases, ——————— overlaps with enamel. Less frequently, the ——————— meets the enamel. In more rare cases, there is a gap between the ——————— and enamel. The Sharpey's fibres at the ends of the PDL fibres are embedded into the ——————— and alveolar bone.
Supportive, sensory, nutritive, formative, resorpitive.
What are the 5 functions of the PDL?
Alveolar bone
This is the overall bone that surrounds the teeth. Dependent on the presence of teeth. If teeth are lost, bone resorbs, and the patient will lose their ——————— ridge dimensions.
Alveolar bone proper/cribriform plate
This is a part of the alveolar bone. A thin later of bone that lines the tooth socket around the root. Radiographically known as the lamina dura.
Alveolus
This is a part of the alveolar bone. Hole in the bone that contains the root. The lining of the ——————— is the cribriform plate.
Cortical bone
This is a part of the alveolar bone. Layer of compact hard bone. Composes the outside wall of the facial and lingual sides (will not show on radiographs). Thicker in the mandible than in the maxilla.
cancellous bone (spongy bone)
This is a part of the alveolar bone. Porous bone that fills the anterior portion of the alveolar process. Contains many holes and allows the blood vessels and nerves to travel.
Alveolar crest
This is a part of the alveolar bone. The most coronal portion of the alveolar process. In health, located 2mm apical to the CEJ. It is the first type of bone to be destroyed when an infection is present.
Periosteum
This is a part of the alveolar bone. This is the layer of connective soft tissue covering the bone. The bone is constantly being remodelled.
Osteoblasts (osteoblasts=build bone)
These are the cells that make bone.
Osteoclasts (osteoclasts=crash down bone)
These are the cells that resorb bone.
Pathogenesis
The sequence of events in the development of a disease.
Gingivitis
What stage of gingival/periodontal disease is this? Colour: red/erythmatous (bc blood flow increases). If this stage of disease persists, the blood vessels may become contests, and gingiva can appear bluish/purple. Consistency: edematous (swollen) or fibrotic (when this stage of disease is chronic). Bleeding: bleeding upon gentle probing. Margin: usually rolled, loses knife-edged adaptation to tooth. Interdental papillae: bulbous and swollen. Sulcus: 4mm+ PDs due to swelling. There is no apical migration of the JE. Alveolar bone: no changes, infection has not progressed into the alveolar bone. Can be acute or chronic. Can be plaque-induced or non plaque-induced.
4-14 days
Gingivitis can be observed clinically — to —— days after plaque accumulates in the gingival sulcus.
Collagen
The body may attempt to repair the tissue by forming new ——————— fibres, which gives the gingiva its fibrotic (leathery) appearance. Excess ——————— fibres mask the redness and make the tissue appear healthier than it actually is.
Periodontitis
What stage of gingival/periodontal disease is this? Defined by a loss of clinical attachment due to destruction of the periodontium. Clinical appearance of gingival tissues is not a reliable indicator of presence, severity, or extent. Colour: dark bluish-purplish or red. Can also appear light pink in chronic —————————— bc of the production of new collagen fibres. Therefore, the appearance of the tissues is not a reliable indicator. Consistency: edematous tissue (spongy tissue), or smooth with a shiny appearance. In chronic conditions, the tissue is usually fibrotic (leathery). Gingival margin: swollen or fibrotic. Interdental papillae: blunted and may not fill embrasure space. Bleeding: bleeding upon gentle probing and/or suppuration. Pocket: 4mm+ due to inflammation and apical migration of the JE. Marked by the apical migration of the junctional epithelium. Tooth mobility may be present. Can be generalized or localized.
Periodontitis GRADING
This is determined after it has been established that periodontitis is present (generalized or localized). It aims to indicate the rate of periodontitis progression, responsiveness to therapy, and potential impact on systemic health.
grade B
What GRADE of periodontitis? There has been less than 2mm of radiographic bone loss over 5 years, when the % of bone loss is divided by age, it is equal to 0.25-1.0, the destruction is commensurate with biofilm deposits. Grade modifiers for this grade: <10 cigarettes per day, HbA1c <7.0% in patients with diabetes. Moderate rate of progression
Grade A
What GRADE of periodontitis? There has been no loss RBL over 5 years, % of bone loss divided by age = <0.25, heavy biofilm deposits with low levels of destruction. Grade modifiers: non-smoker, normglycemic/no diagnosis of diabetes. Slow rate of progression
Grade C
What GRADE of periodontitis? 2 mm or more RBL over 5 years, % of bone loss divided by age is >1.0, destruction exceeds expectations given biofilm deposits,; specific clinical patterns suggestive of periods of rapid progression and/or early onset of disease.. grade modifiers: 10 or more cigarettes a day, HbA1c of 7 or more in patients with diabetes. Rapid rate of progression.
If a patient has diabetes and periodontitis, they are automatically put in grade B or above.
Necrotizing periodontal disease
———————— periodontal diseases are strongly associated with impairment of the host immune system: chronically, severely compromised patients, (e.g., HIV/AIDS patients, children suffering from severe malnourishment, extreme living conditions, or severe infections). And temporarily and/or moderately compromised patients (e.g., smokers or psycho-socially stressed adult patients).
Necrotizing gingivitis
This is an acute inflammatory process of the gingival tissues characterized by presence of: necrosis/ulcer of the interdental papillae, gingival bleeding, pain, other signs/symptoms include halitosis, pseudomembranes, regional lymphadenopathy, fever, and sialorrhea (in children).
Necrotizing periodontitis
Inflammatory process of the periodontium characterized by the presence of: necrosis/ulcer of the interdental papillae, spontaneous gingival bleeding, halitosis (fetid odour), pain, rapid bone loss, other signs/symptoms associated with this condition may include pseudomembrane formation, lymphadenopathy, fever, and malaise.
Necrotizing stomatitis
This is a severe inflammatory condition of the periodontium and the oral cavity. I which the soft tissue necrosis extends beyond the gingiva and destruction may occur through the alveolar mucosa, tongue, cheek, and palate. Typically occurs in severely systemically compromised patients. Atypical cases have also been reported, in which this may develop without prior appearance of necrotizing gingivitis/periodontitis lesions.
Down Syndrome
Patients with this syndrome have a higher prevalence of severity of periodontal disease than individuals without it. And the periodontal attachment loss starts in adolescence. Intrinsic abnormalities of the immune system may predispose these individuals to infections.
Papillon-Lefèvre syndrome
This systemic disorder causes hyperkeratosis of the palms of hands and soles of the feet and severe periodontal destruction. Includes severe gingival inflammation, early onset, and rapidly progressive alveolar bone loss; early loss of the primary and permanent teeth.
Congenital neutropenia
This condition involves the presense of neutropenia at or around the time of birth aANC less than 1500. Severe periodontitis is common; higher risk for tooth loss; oral ulcers.
Systemic lupus erythematousus (SLE), diabetes, HIV infection, arthritis, cytotoxic chemotherapeutics
These other 5 systemic conditions can cause periodontitis and/or exacerbate periodontitis symptoms:
Oral Squamous Cell Carcinoma (oral SCC)
This type of oral cancer causes localized swelling or ulceration of the gingiva, typically in the mandibular molar region.
Odontogenic tumours
This type of tumour found in/around the oral cavity cause early lesions such as: mandibular or maxillary localized swelling and tooth displacement and late features similar to localized periodontitis
Giant cell granuloma (GCG)
Peripheral —.—.—. causes expanding epulis-like gingival swelling, occasional loss of periodontal supporting tissue; and Central —.—.—. Causes loss of deep periodontal supporting tissue, which may expand toward marginal periodontal tissue.
Occlusal trauma
This is a term used to describe injury resulting in tissue changes, within the attachment apparatus, including the PDL, supporting alveolar bone, and cementum as a result of occlusal forces.
Primary occlusal trauma
This is a type of occlusal trauma resulting in tissue changes from excessive occlusal forces applied to a tooth or teeth with normal periodontal support.
Secondary occlusal trauma
This is a type of occlusal trauma resulting in tissue changes from normal or excessive occlusal forces applied to a tooth or teeth with reduced periodontal support.
Bruxism
This is a type of occlusal trauma. This or tooth grinding is a habit of grinding, clenching, or clamping teeth.
Peri-implant health
Clinically, this is the state of an implants supporting structure characterized by an absence of visual signs of inflammation and bleeding on probing. Can exist around implants with normal or reduced bone support. It is not possible to define a rage of probing depths comparable with this peri-implant state.
Peri-implant mucositis
Clinically, this is the state of an implants supporting structures characterized by bleeding on probing and visual signs of inflammation. While there is strong evidence that this peri-implant state is caused. By plaque, there is very limited evidence for non-plaque induced ———— ——————— ————————. Can be reversed with measures aimed at eliminating the plaque.
Peri-implantitis
This state of the implant supporting structures is defined as a plaque-associated pathologic condition occurring in the tissue around dental implants, characterized by inflammation in the peri-implant mucosa and subsequent progressive loss of supporting bone. Associated with poor plaque control and with patients with a history of severe periodontitis. Onset of this state of implant supporting structures may occur early following implant placement as indicated by radiographic data. Seems to progress in a non-linear and accelerating pattern.
Plaque-biofilm
Periodontal diseases can be affected by numerous factors. ————— ————— and the bacteria associated with it are the main causes of periodontal disease. Gram-negative, motile, anaerobic, rod-shaped bacteria are associated with periodontitis. The presence of bacteria alone is not sufficient to cause periodontal disease. Previous theories focused on species that were thought to be the major etiologic agents of periodontal disease (red and orange complex).
Host response
Body's response to bacteria is important in the disease process. Loe and coworker study examined Sri Lankan tea workers over 20 years. Despite the same level of dental care, the subjects did not have the same amount of periodontal disease. This study emphasizes the importance of the ———— ———————. The ———— ——————— theory is that an individual's body response dictates the disease initiation and progression.
Local factors
These factors do not initiate periodontal diseases but contribute plaque retention. Ex: poorly contoured resto, calc, furcation, tooth decay or cavity (holes), irregular tooth morphology such as grooves or concavities.
Risk factors
Tobacco use, genetics, educational level, socioeconomic status, parafunctional habits, mouth breathing, occlusal trauma, impingement on the biological width, furcations, calc, restorations, pits, caries, obesity, poor nutrition, age, stress, and systemic diseases are all ———— ————— for periodontal disease.
Tobacco
This is one of the most significant risk factors for periodontal disease. Inhibition of collagen production and slow healing after therapy is seen in patients who use this. Gingival can appear healthy due to impaired vascularization (diseased gingiva usually looks dark and swollen due to increased vascularization).
Genetics
This is a risk factor for periodontal disease. Despite aggressive oral care habits, some patients are more likely to develop periodontal diseases because of this. Ex: patients with Down syndrome are often develop severe periodontitis.
Educational level/socioeconomic status
This is a risk factor for periodontal disease. Patient with lower education levels and socioeconomic status are more likely to have perio disease.
Parafunctional habits
This is a risk factor for periodontal disease. Clenching, grinding, tongue thrusting, and other habits exert excessive stress on the periodontium and weaken it.
Impingement on the biological width
This is a risk factor for periodontal disease. This is when a restoration is placed too close to the crystal bone and can destroy the periodontium.
Obesity/poor nutrition
This is a risk factor for periodontal disease. Lack of nutrients can compromise the body's immune system and make it harder for the body to preserve oral tissues. Vitamin C is important for wound healing and collagen production. Protein is important for the repair process.
Age
This is a risk factor for periodontal disease. Elderly patients have the highest rates of periodontal disease. It is important to remember that ——— itself does not cause periodontal disease. Factors related to it such as lack of dexterity, soft diet, medication use, and duration of disease process can contribute to the disease.
Phenytoin (Dilantin), cyclosporine (Sanimmune), and nifedipine (Procardia)
Gingival enlargement can be caused by these 3 medications:
Diabetes
This systemic disease increases the level of glucose present in the gingival crevicular fluid that serves as nutrition for bacteria. Patients can be affected by: delayed wound healing, increased risk for infections including candidiasis and periodontal disease., diminished sensation, burning mouth, parotid gland enlargement.
Bulbous
This is when the papilla is enlarged and bulges out of the interproximal space.
Blunted
This is when the papilla is flat and does not fill the interproximal space.
Cratered
This is when the papilla has a concave depression, described as "scooped out".
Papillary
——————— gingivitis is when only the interdental papilla are inflamed.
Marginal
——————— gingivitis is when the gingival margin is inflamed.
Localized
This is when the disease affects 30% or less of all sites.
Diffuse
——————— gingivitis is when the gingival margin, papilla, and attached gingiva are all inflamed.
Recurrent disease
This is when new signs of destructions reappear after periodontal therapy caused by inadequate professional or self care.
Refractory disease
This is when there is destruction despite appropriate professional care and self-care.
Class I
This class of embrasure is characterized by the interdental papilla filling the space. The best interdental cleaning aid is traditional dental floss.
Class III
This class of embrasure is characterized by the interdental papilla being missing. The best interdental cleaning aids are tufted dental floss, interdental brush, wooden interdental cleaners, end tuft brushes, or toothpicks.
Class II
This class of embrasure is characterized by the interdental papilla not filling the entire space. The best interdental cleaning aids are tufted dental floss, interdental brushes, wooden interdental cleaners, or toothpicks.
Gingival margin to mucogingival junction minus the Probing depth
How to measure attached gingiva width.
Pseudopocket
This is caused by gingival inflammation without loss of attachment. This is also called a "gingival pocket" instead of a periodontal pocket, as a periodontal pocket involves apical movement of the junctional epithelial attachment.
Horizontal
A suprabony pocket is when the base of the pocket is above (coronal) the alveolar crest. It is created by what type of bone loss?
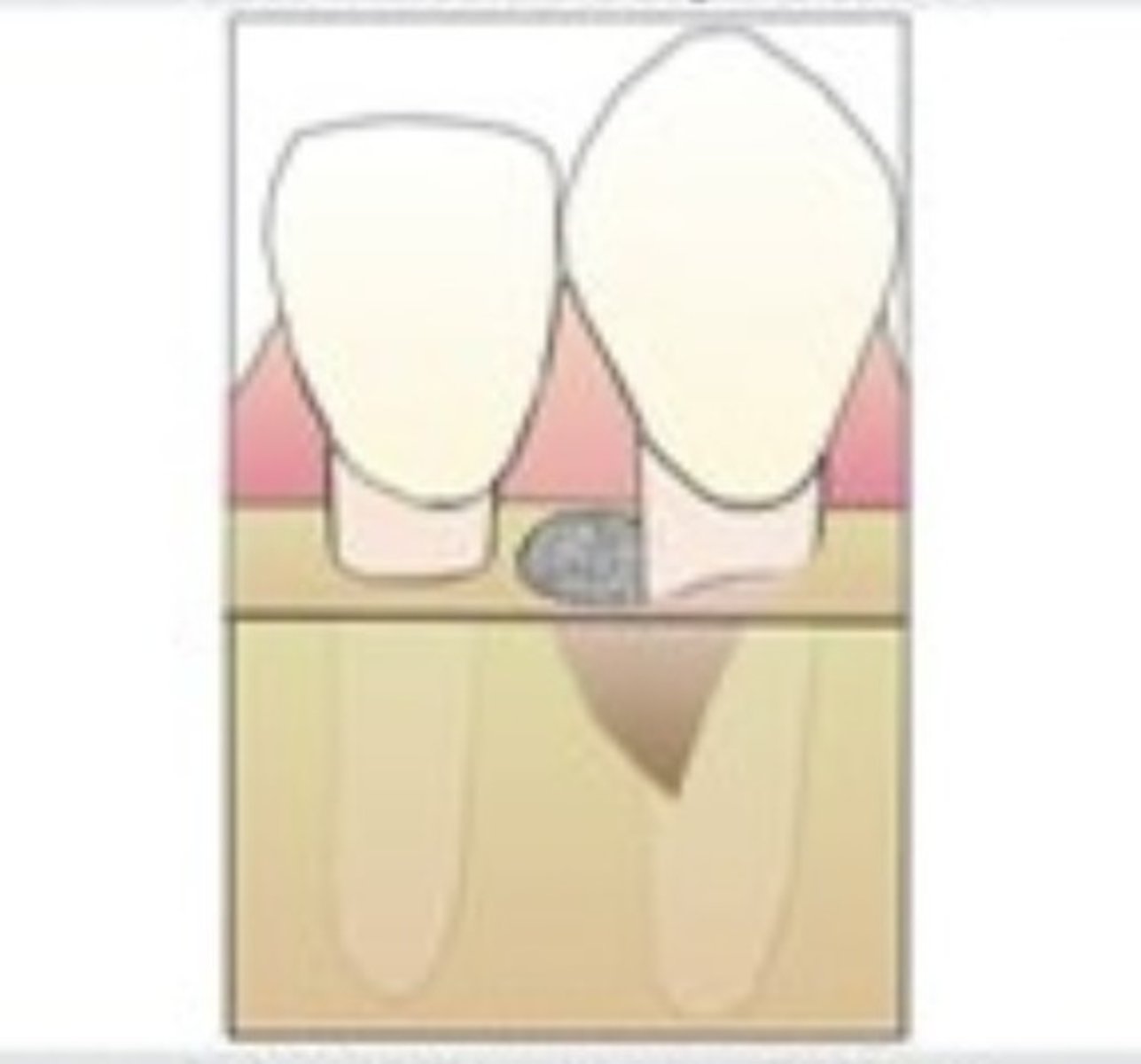
Infrabony pocket
This is when the base of the pocket is below the alveolar crest. Created by vertical bone loss.
Three-wall defect, two-wall defect, one-wall defect.
An infrabony pocket can be exhibited in 3 forms:
Three-wall defect
This is a form of Infrabony pocket. When it is bordered by 3 osseous surfaces and 1 tooth surface. Has the best prognosis among the three bone defects.
Two-walled defect
This is a form of Infrabony pocket. When it is bordered by 2 osseous surfaces and 2 tooth surfaces.
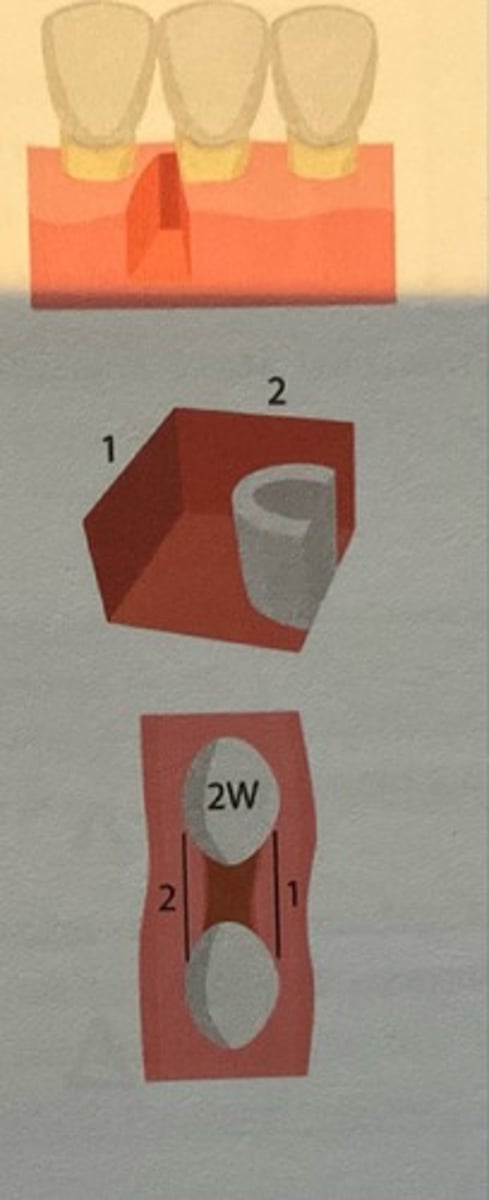
One-walled defect
This is a form of Infrabony pocket. When it is bordered by 1 osseous defect and 3 tooth surfaces.
Less than 1mm
According to the miller classification system of tooth mobility, class I tooth mobility involves facial-lingual horizontal displacement of how much?
1-2mm
According to the miller classification system of tooth mobility, class II tooth mobility involves facial-lingual horizontal displacement of how much?
More than 2mm horizontal and any depression into socket
According to the miller classification system of tooth mobility, class III tooth mobility involves facial-lingual horizontal displacement of how much and vertical displacement.