Special Tests
1/116
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
117 Terms
Yergason's test
- integrity of transverse ligament
(+) long head of bicep tendon will pop out of groove. tenderness in bicipital groove alone without dislocation may indicate bicipital paratenonitis / tendinosis
Speed's test
- bicep tendinosis / tendinopathy
(+): pain long head of bicep tendon / increase tenderness in bicipital groove

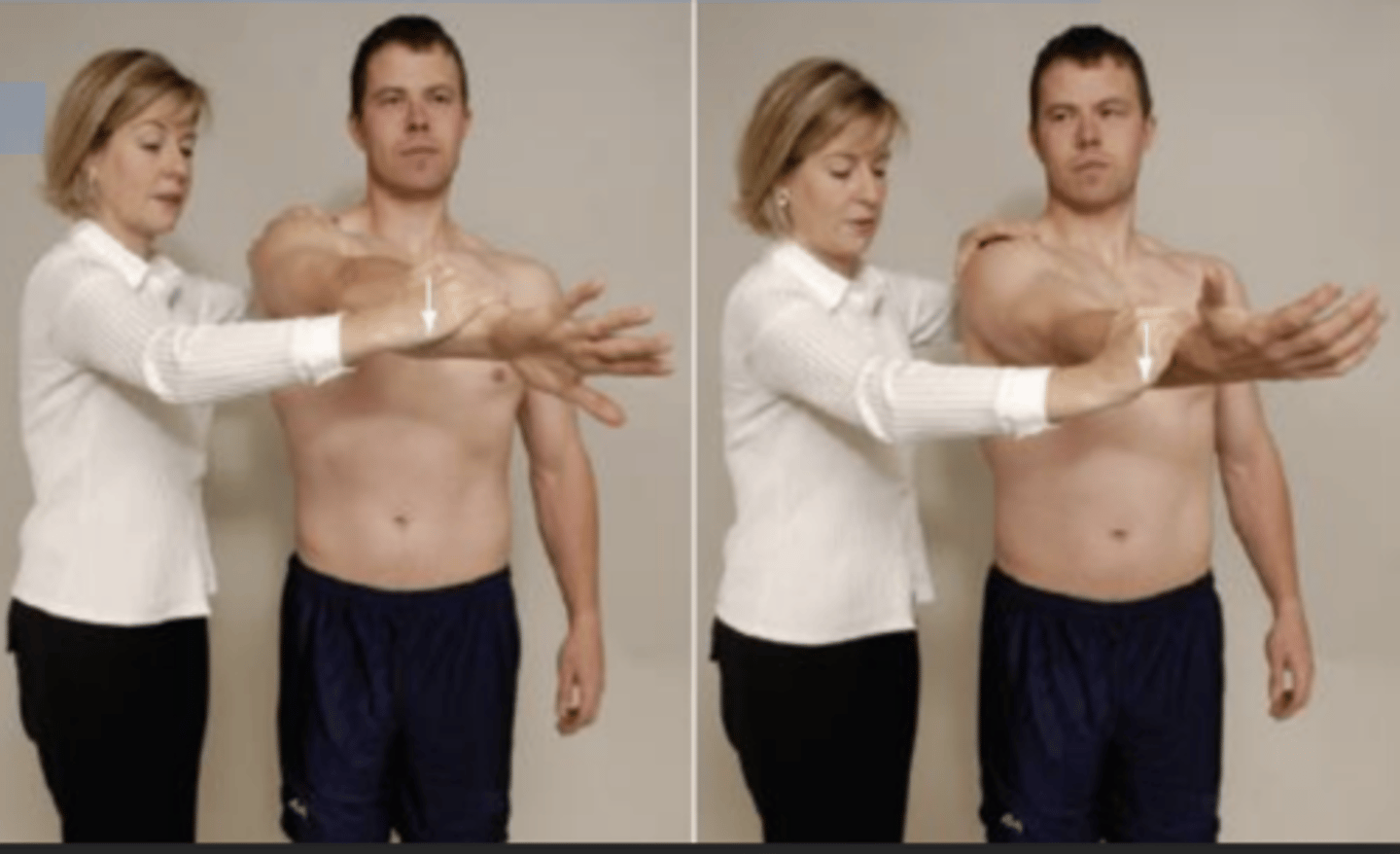
Neer's Impingement test
- impingement of supraspinatus and bicep tendon
(+): reproduces symptoms of pain in shoulder

Empty Can / Jobe test
- tear or impingement of supraspinatus tendon or suprascapular nerve neuropathy
(+): reproduces pain in supraspinatus tendon or weakness in empty can position

Drop Arm Test (Codman's Test)
- tear / full rupture of rotator cuff
(+): if pt is unable to return the arm to side slowly or has severe pain when attempt to do so
Posterior Internal impingement test
- impingement between rotator cuff and greater tuberosity or posterior glenoid and labrum
(+): reproduction of pain in posterior shoulder during test

Hawkins- Kennedy Test
- subacromial impingement
(+): pain indicates positive test for supraspinatus paratenonitis / tendinosis or secondary impingement

Yocum Test
- modification of Hawkins Kennedy test (subacromial impingement)
- pt's hand is placed on opp shoulder & examiner elevates the elbow
- pain indicates a (+) test

Horn Blower's Sign (Patte test)
- to detect RC tears involving teres minor
- description: pt sitting or standing. pt's arm is supported at 90 degrees of abduction in the scapular plane, with the elbow flexed to 90 degrees. pt is then asked to rotate the forearm externally against the resistance of PT hand.
(+): pt is unable ER shoulder in test position, the hornblower's sign is said to be present
Active compression test of O'Brien
- SLAP (type 2) or superior labral lesions
(+): If pain on the joint line or painful clicking is produced inside the shoulder (not over the acromioclavicular joint) in the first part of the test and eliminated or decreased in the second part, the test is considered positive for labral abnormalities.
Bicep Load Test
- integrity of superior labrum
(+): apprehension remains the same or shoulder becomes more painful + SLAP lesion
- apprehension decrease or pt feel more comfortable (negative for SLAP lesion)

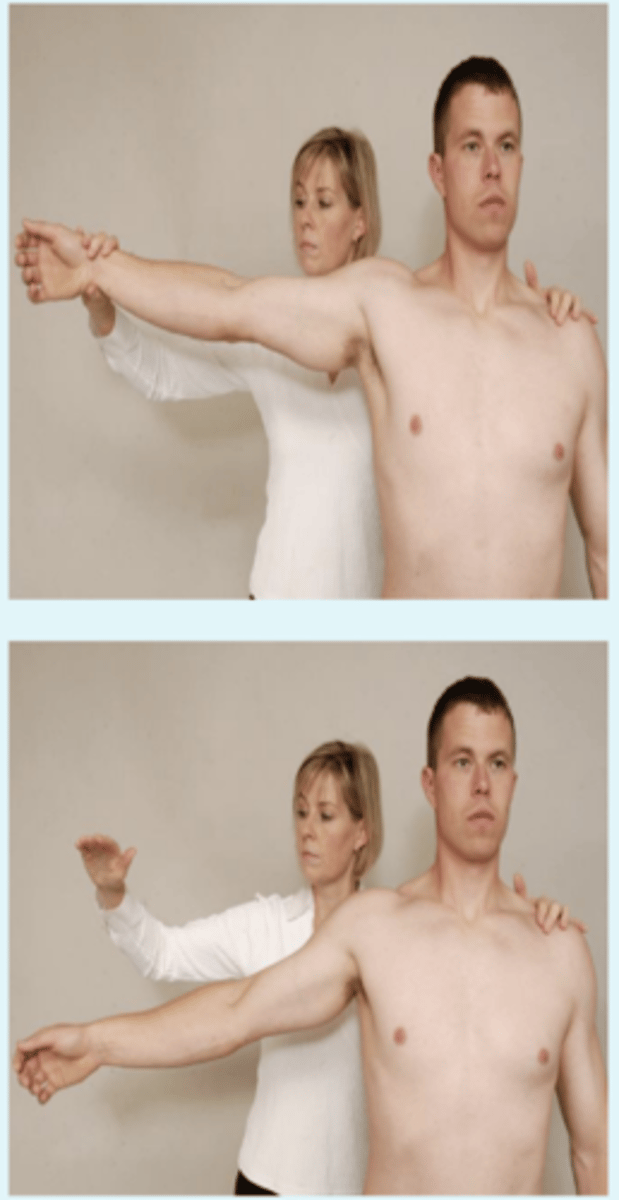
Lateral Rotation Lag sign ( Spring Back test); ER lag sign
- test teres minor and infraspinatus
(+): pt can't hold position and hand springs back anteriorly toward midline, indicates infra and teres minor can't hold position due to weakness or pain

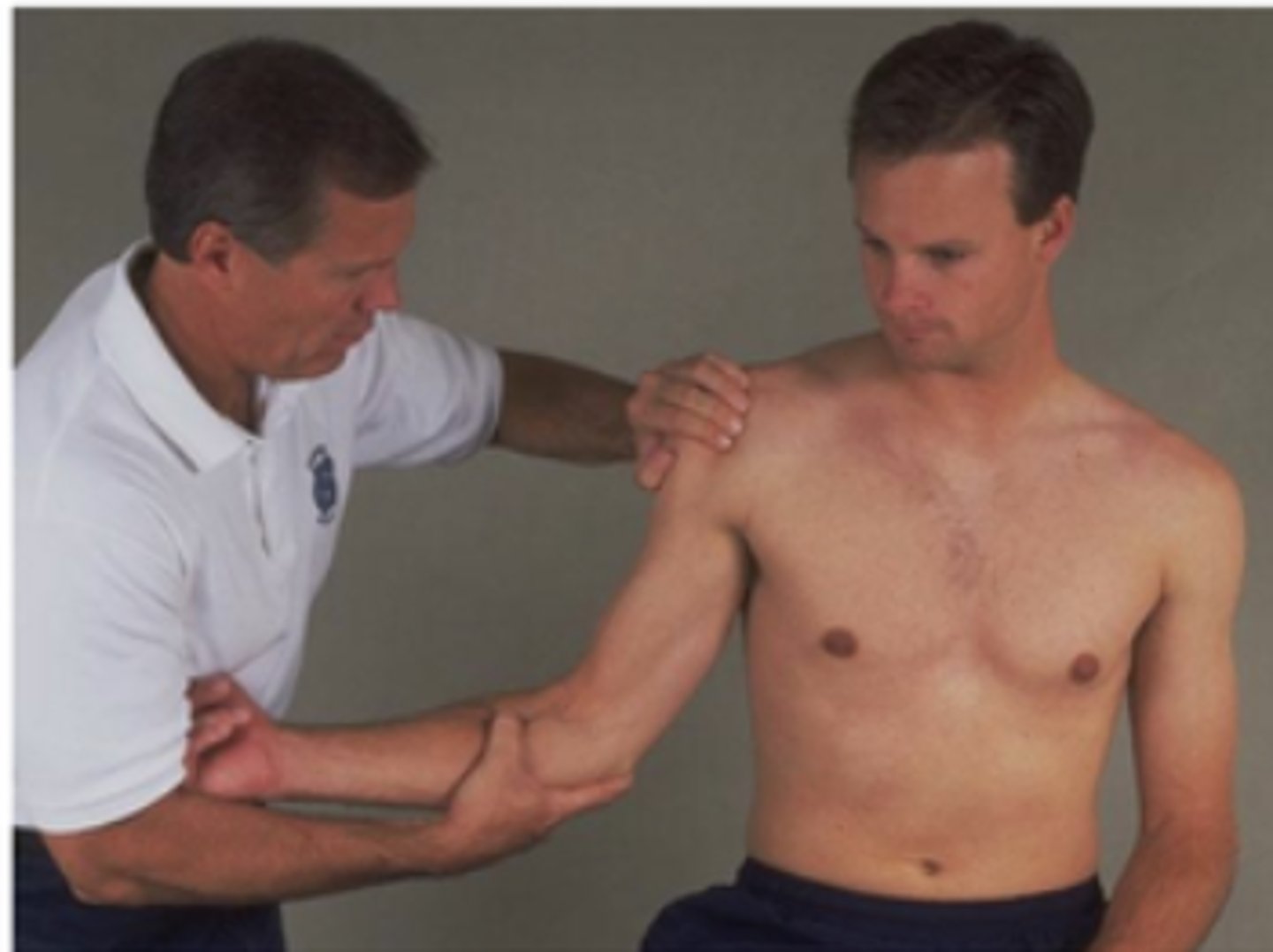
Abdominal Compression Test ( belly-press or Napoleon Test)
- checks the subscapularis
(+): pt unable to maintain pressure on PT hand while moving elbow forward or posteriorly flexes the wrist or extends the shoulder = tear of subscapularis muscle

Lift Off Sign (gerber's test)
- to detect a lesion of subscapularis
- description: pt places the dorsum of the hand on his back pocket of against the mid-lumbar spine (great subscapularis activity is shown with the second position) the pt then lifts the hand away from the back
(+): inability to do so indicates lesion of subscapularis muscle
Jerk Test
- to test recurrent posterior instability
description: pt sits with the arm medially rotated and forward flexed to 90 degrees. PT grasps the pt's elbow and axially loads the humerus in a proximally direction. while maintaining the axial loading, the PT moves the arm horizontally across the body
(+): production of a sudden jerk or clunk as the humeral head slides off (subluxes) back of the glenoid
- when arm is returned to original 90 degrees abduction, a second jerk maybe felt as head reduces

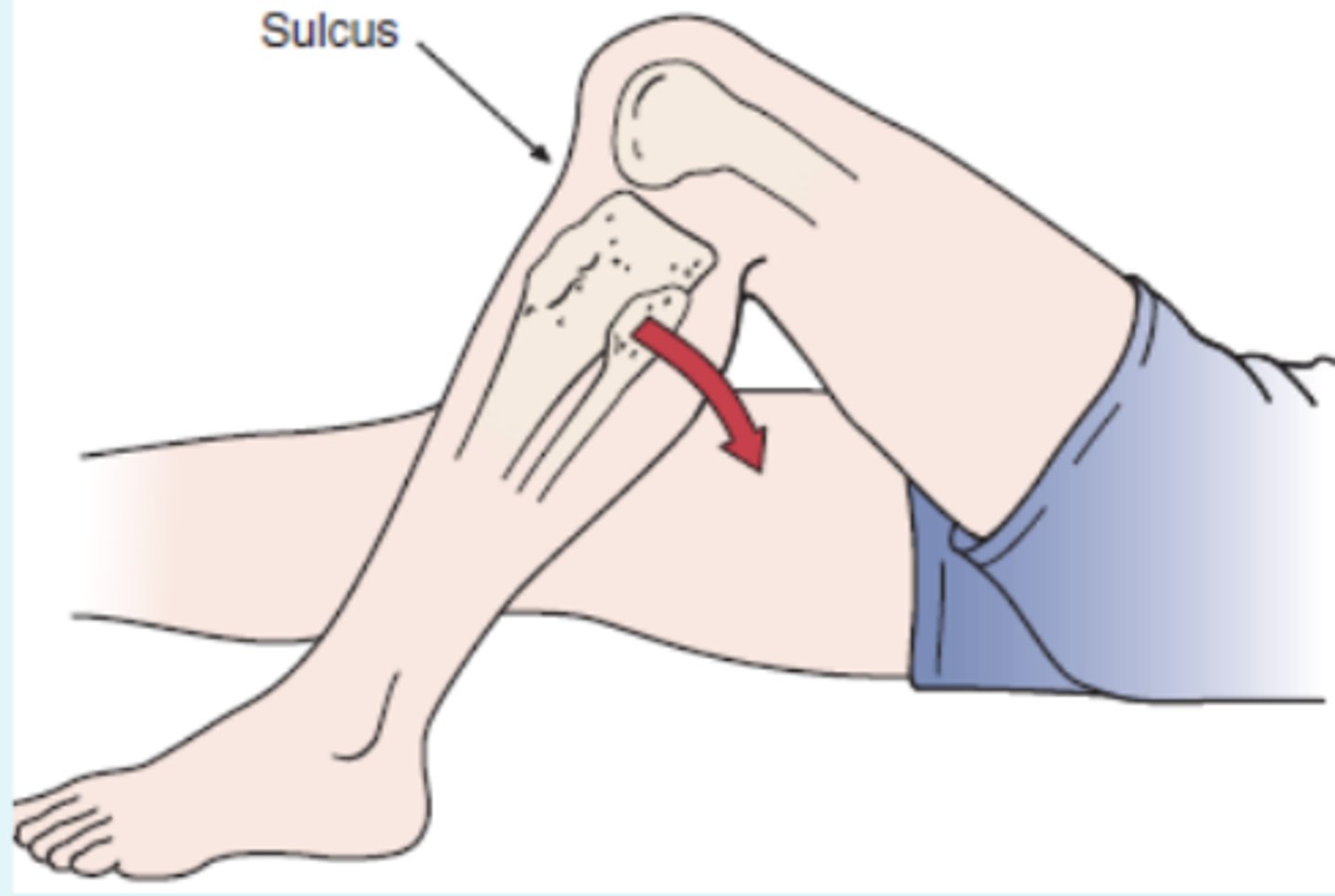
Sulcus Sign
- test for inferior glenohumeral instability
description: pt stands with the arm by the side and shoulder muscles relaxed. the PT grasps the pt's forearm below the elbow and pulls the arm distally.
(+): presence of sulcus sign indicates inferior instability of glenohumeral laxity

Pectoralis Major Contracture test
- identify tightness of pec major
- description: pt lies supine and clasps the hands together behind the head. the arms are then lowered until the elbows touch the table
(+): elbows do not reach table, and indicates a tight pec major muscle

Halstead Maneuver
- pathology of structures that pass through thoracic inlet
description: PT finds radial pulse and applies downward traction on the test extremity while the pt's neck is hyperextended and head is rotated to the opposite side.
(+): Absence or disappearance of a radial pulse indicates a positive test for thoracic outlet syndrome.

Clunk test
- glenoid labrum tear
- description: pt supine, with shoulder in full abduction. push humeral head anteriorly, while rotating humerus externally
(+): audible clunk is heard while performing test

Anterior Apprehension / Crank test
- identify past anterior dislocation of shoulder
- description: pt supine, PT abducts the arm to 90 degrees and laterally rotates the pt's shoulder slowly. by placing a hand under the glenohumeral joint to act as a fulcrum, the apprehension test becomes the fulcrum test.
(+): pt doesn't allow or doesn't like to move shoulder in that direction to simulate anterior dislocation

Posterior Apprehension Sign
- identify past history of posterior shoulder dislocation
- description: pt supine/sitting. PT elevates the pt's shoulder in the plane of the scapula to 90 degrees while stabilizing the scapula with the other hand, then - applies a posterior force on the pt's elbow. while applying the axial load, the examiner horizontally adducts and medially rotate the arm
(+): pt doesn't allow or does not like to move shoulder in that direction to simulate posterior dislocation

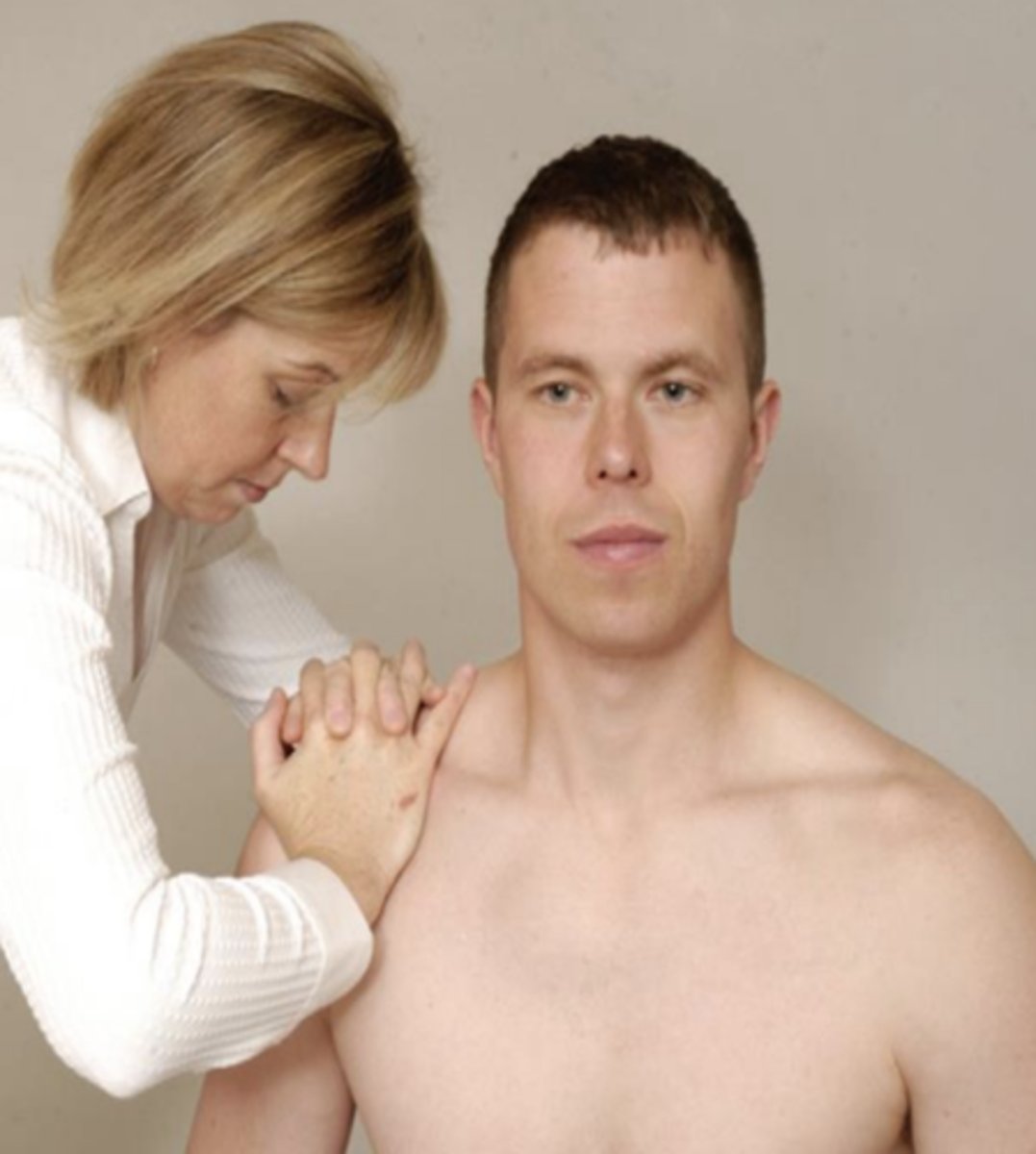
Acromioclavicular shear test
- identifies dysfunction of AC jt (arthritis or separation)
(+): reproduce pain in AC jt
Adson's Test
- identify pathology of structures that pass through the thoracic inlet:
- description: PT locates radial pulse. the pt's head is rotated to face the test shoulder. pt then extends the head while the examiner laterally rotates and extends the pt's shoulder. pt is instructed to take a deep breath and hold it
(+): disappearance of radial pulse

Costoclavicular Syndrome Test (Military Brace Test)
- thoracic outlet syndrome
- description: PT palpates radial pulse and then draws the pt's shoulder down and back.
(+): absence of the pulse and implies possible thoracic outlet syndrome (costoclavicular syndrome). This test is particularly effective in patients who complain of symptoms while wearing a backpack or heavy coat.

WRIGHT (Hyperabduction) test
- thoracic outlet syndrome
description: pt sitting, locate radial pulse of extremity being tested. move shoulder into max abduction and external rotation. taking a deep breath and rotating head opposite to test site may accentuate symptoms
(+): neurological / vascular symptoms (disappearance of pulse) will be reproduced

Roos Test
- thoracic outlet syndrome
(+): pt unable to keep arms in starting position for 3 minutes, or suffers ischemic pain, heaviness or profound weakness of the arm, or numbness and tingling of the hand during the minutes, the test is considered positive for thoracic outlet syndrome on the affected side.

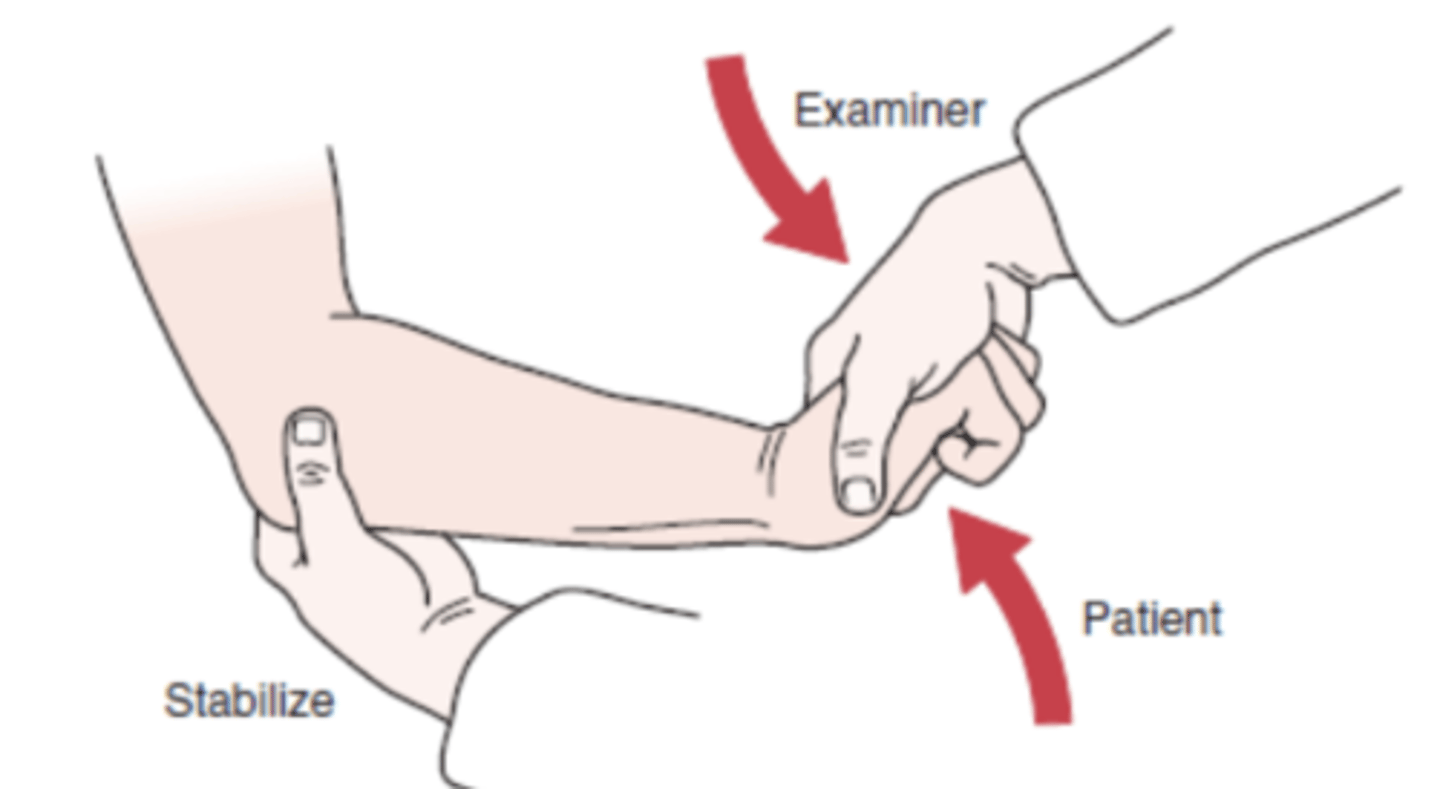
Ligament Instability test (elbow)
- ligament laxity or restriction (valgus = UCL, varus = radial)
(+): primary finding is laxity but pain can be present

Lateral Epicondylitis Test (Cozen's test)
- lateral epicondylopathy
- extensor carpi radialis brevis
- description: pt is sitting with elbow 90 degrees flexion then asked to actively make a fist, pronate the forearm, and radially deviate and extend the wrist while the examiner resists the motion.
(+): sudden severe pain in area of lateral epicondyle of humerus
Mill's test
- lateral epicondylopathy
- extensor carpi radialis brevis
- description: while palpating lateral epicondyle, examiner passively pronates the pt's forearm, flexes the wrist fully and extends the elbow.
(+): pain over lateral epicondyle of humerus
Maudsley's test
- lateral epicondylopathy
- puts stress on extensor digitorum
- procedure: Patient sitting with arm on table Pt fixates forearm while palpating the lateral epicondyle with thumb. Patient then pronates arm and palm in table. Patient then extends 3rd digit distal to proximal interphalangeal joint against resistance
(+): pain over lateral epicondyle of humerus
Elbow flexion test
- cubital tunnel syndrome
procedure:
- The patient is asked to fully flex the elbow with extension of the wrist and shoulder girdle abduction (90°) and depression and to hold this position for 3 to 5 minutes. Symptoms should develop in less than 5 seconds
(+): tingling or paresthesia in the ulnar nerve distribution of forearm and hand

Medial Epicondylitis test
- golfer's elbow test
- medial epicondylopathy
- description: while the PT palpates the pt's medial epicondyle, the pt's forearm is passively supinated and examiner extends the elbow and wrist
(+): pain over medial epicondyle of the humerus

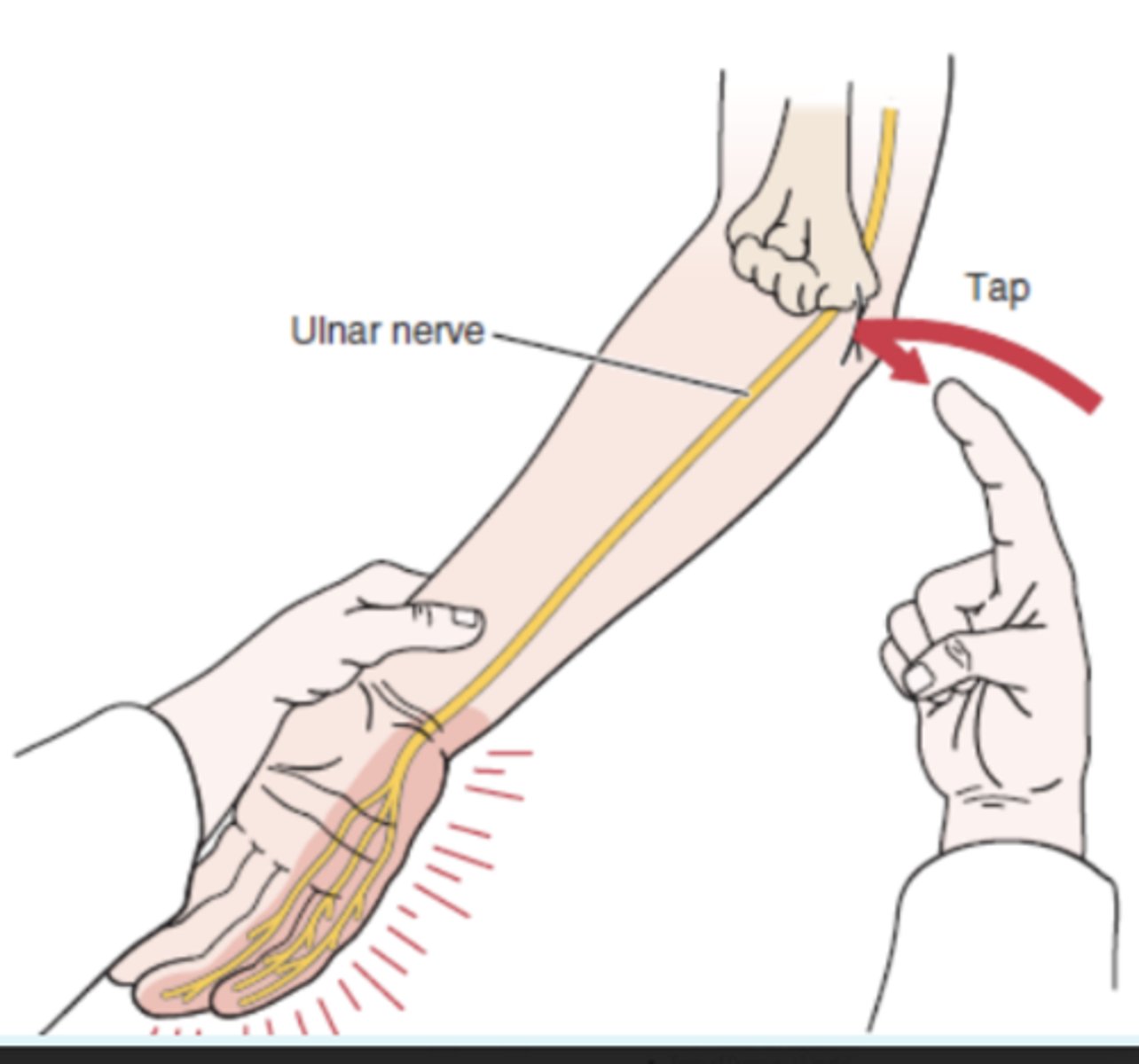
Tinel's Sign (elbow)
- dysfunction of ulnar nerve at olecranon
(+): tingling sensation in ulnar distribution of forearm and hand distal to point of compression. The test indicates the point of regeneration of the sensory fibers of a nerve. The most distal point at which the patient feels the abnormal sensation represents the limit of nerve regeneration.
Pronator Teres syndrome test
- median nerve entrapment within pronator teres
- procedure: elbow flexed to 90 degrees, PT strongly resists pronation as the elbow is extended
(+): tingling or paresthesia in median nerve distribution in forearm and hand

Bunnel - Littler Test (intrinsic plus test)
- identifies tightness in structures surrounding the MCP joint
- description: the MCP joint is held slightly extended while the PT moves the proximal interphalangeal joint into flexion, if possible
(+): test is positive (which indicated by inability to flex the proximal interphalangeal joint), there is a tight intrinsic muscle or contracture of the joint capsule. if the metacarpophalangeal joints are slightly flexed, the proximal interphalangeal joint flexes fully if the intrinsic muscle are tight, but it does not flex fully if the capsule is tight. the pt remains passive during the test.

Tight Retinacular Test
- identify tightness around PIP joint
- description: the proximal interphalangeal joint is held in a neutral position while the distal interphalangeal joint is flexed by the examiner. if the distal interphalangeal joint does not flex, the retinacular (collateral) ligaments or proximal interphalangeal capsule is tight. if the proximal interphalangeal joint is flexed and the distal interphalangeal joint flexes easily, the retinacular ligaments are tight and the capsule is normal.
Ligament Instability Test (hand)
- identify ligament instability, medial or lateral
- description: fingers are stabilized and supported. varus or valgus stress applied to the joint (proximal or distal interphalangeal) to test the integrity of the collateral ligaments
result: the results are compared for laxity with those of the uninvolved hand, which is tested first

Finkelstein's test
- De Quervain's disease (paratenonitis in the thumb)
- muscle bellies of extensor pollicis brevis and abductor pollicis longus
- description: pt makes a fist with the thumb inside the fingers. the PT stabilizes forearm and deviates the wrist toward the ulnar side.
(+): pain over abductor pollicis longus and extensor pollicis brevis tendons at the wrist and is indicative of a paratenonitis of these two tendons.
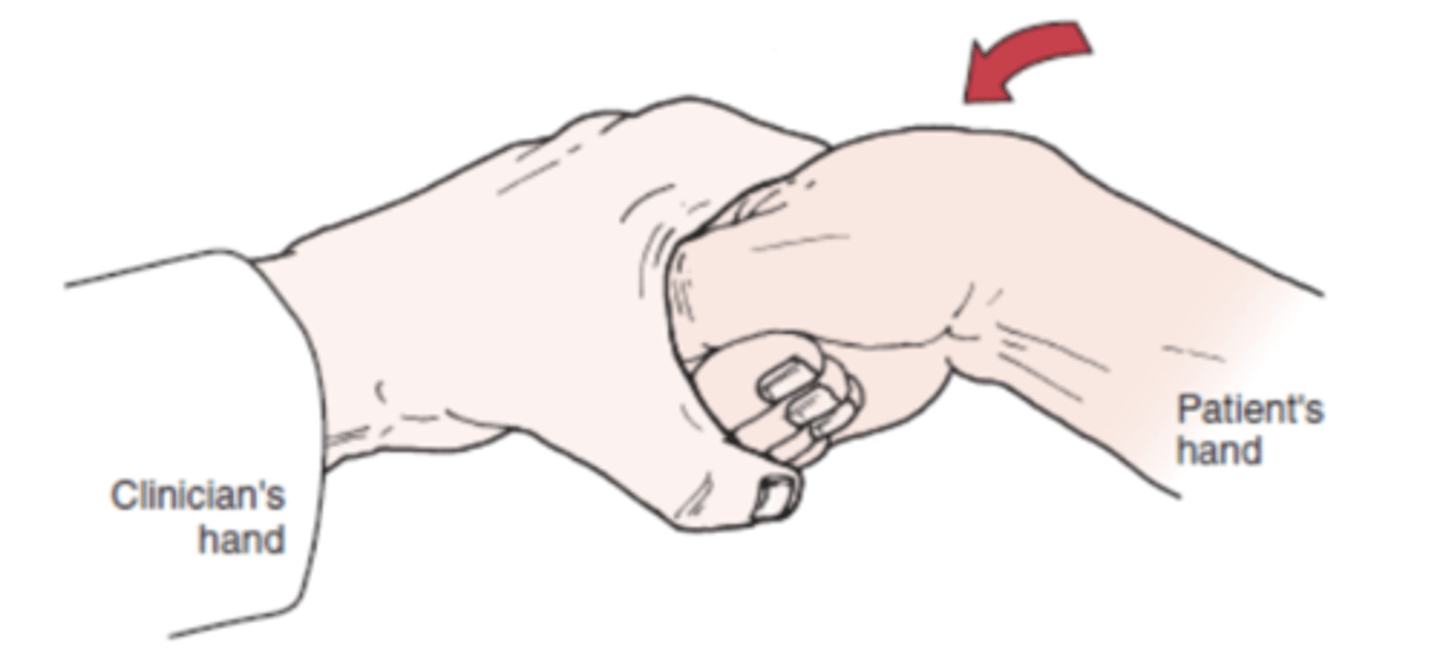
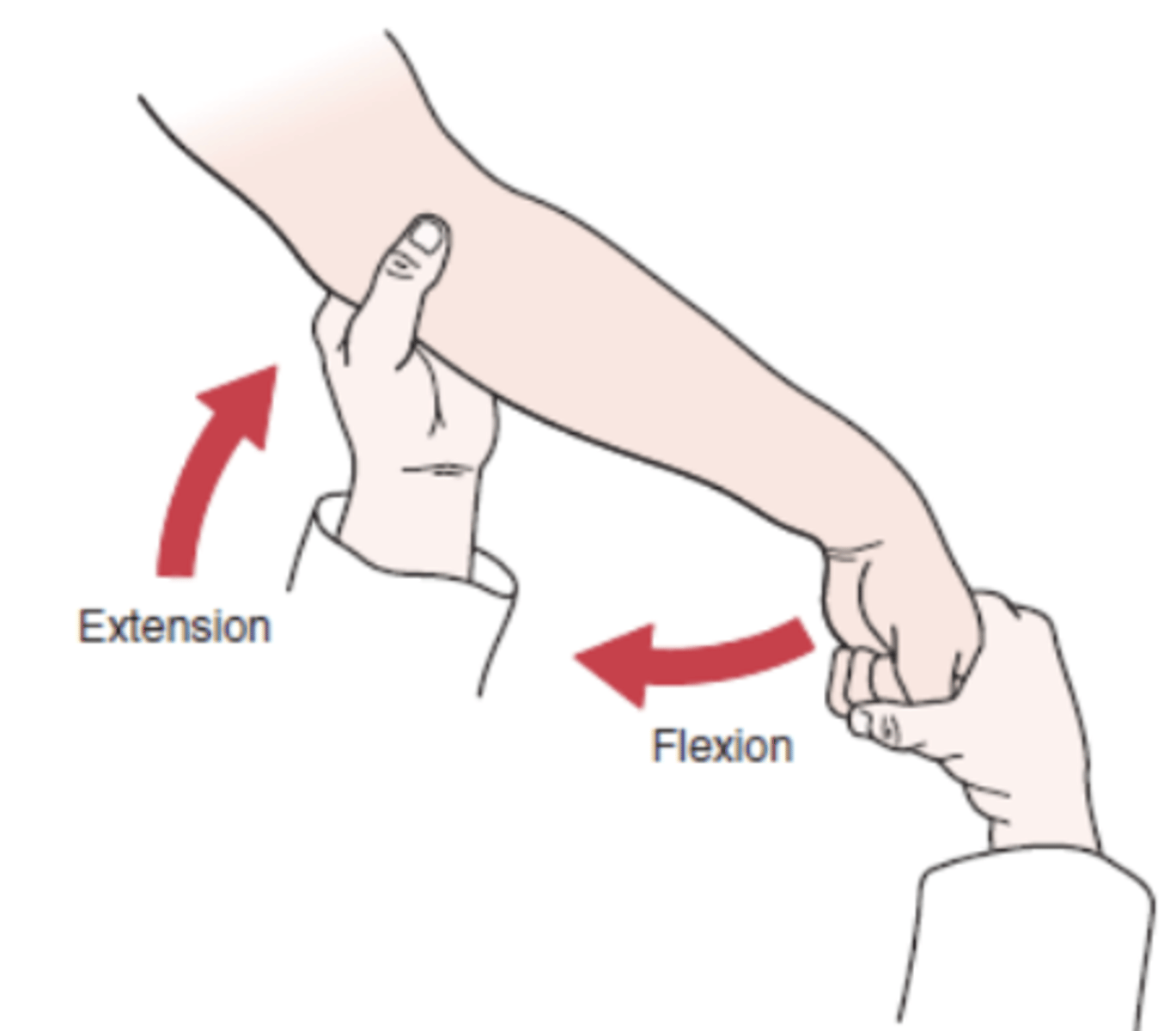
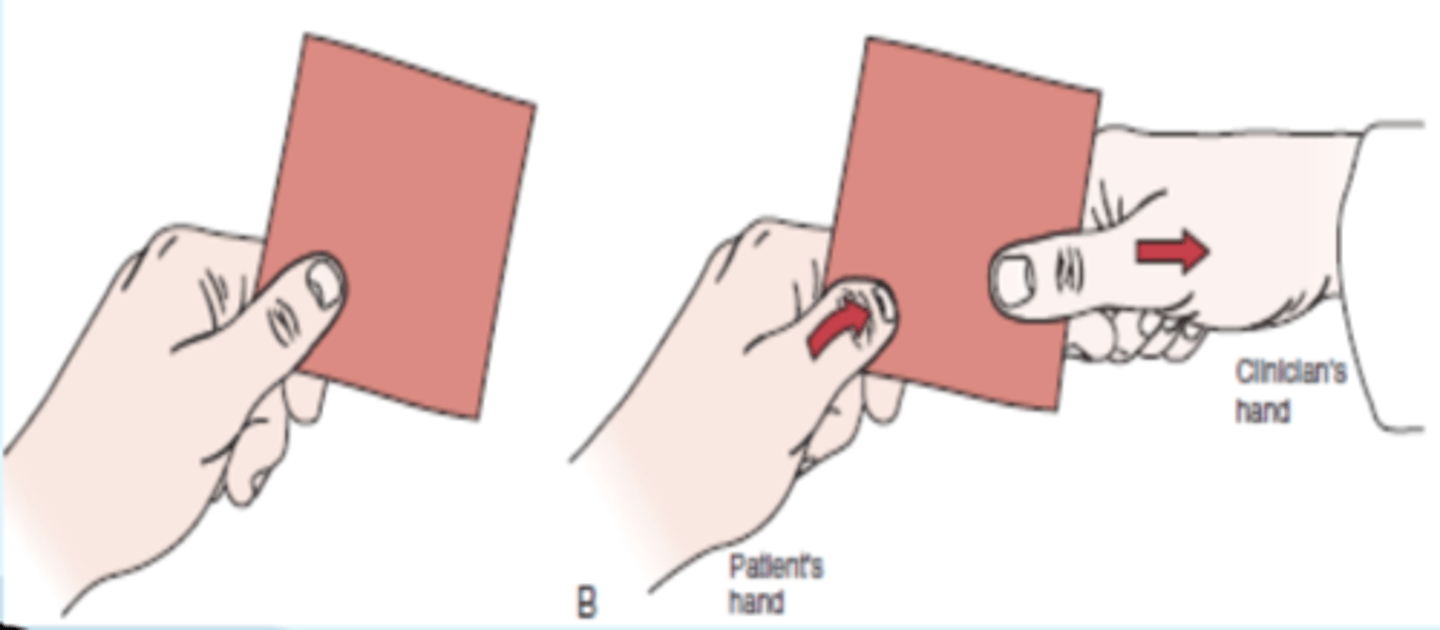
Froment's sign
- ulnar nerve dysfunction
(+): When the examiner attempts to pull away the paper, the terminal phalanx of the thumb flexes because of paralysis of the adductor pollicis muscle, indicating a positive test.
- If, at the same time, the metacarpophalangeal joint of the thumb hyperextends, the hyperextension is noted as a positive Jeanne's sign. Both tests, if positive, are indicative of ulnar nerve paralysis
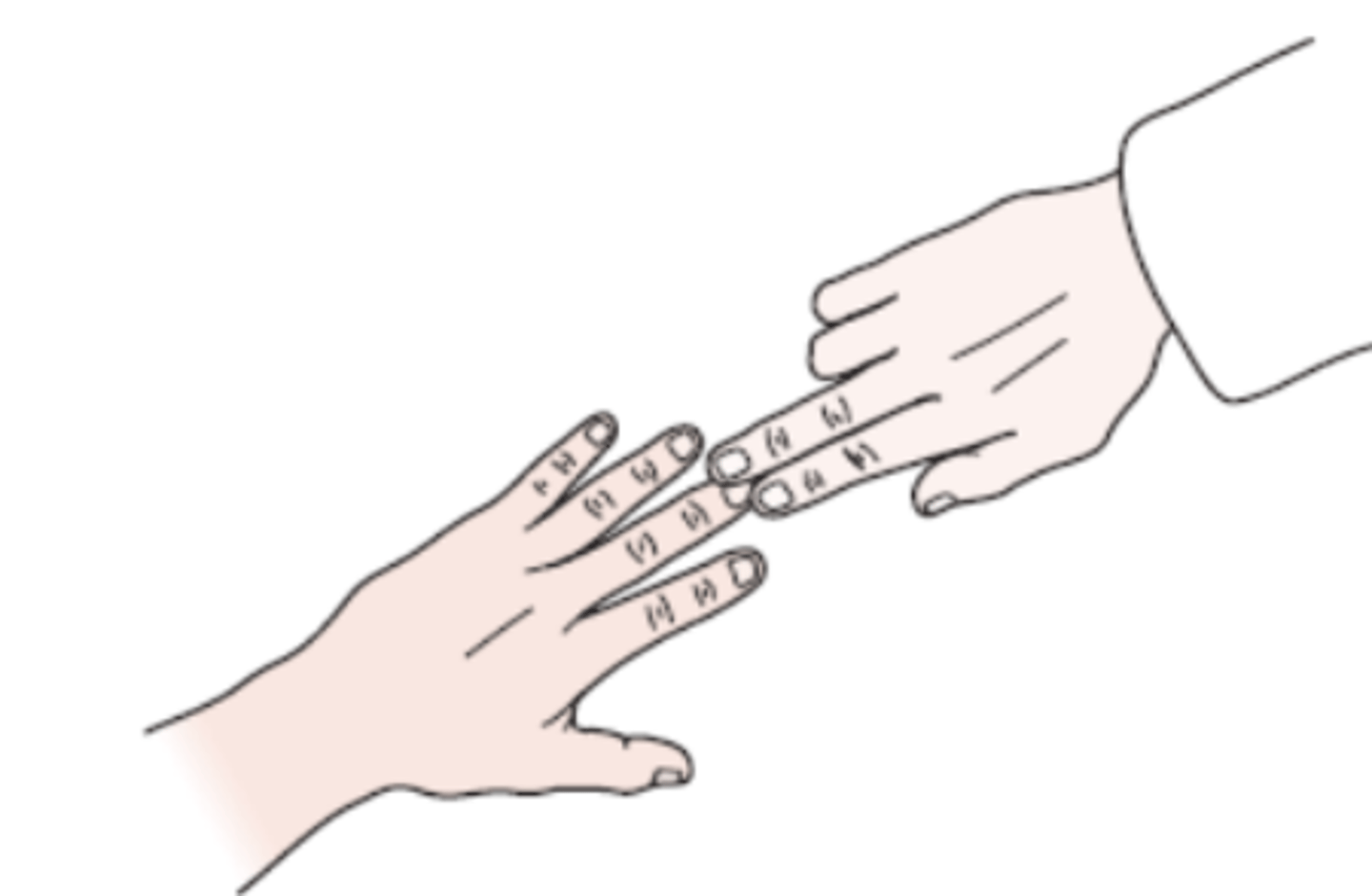
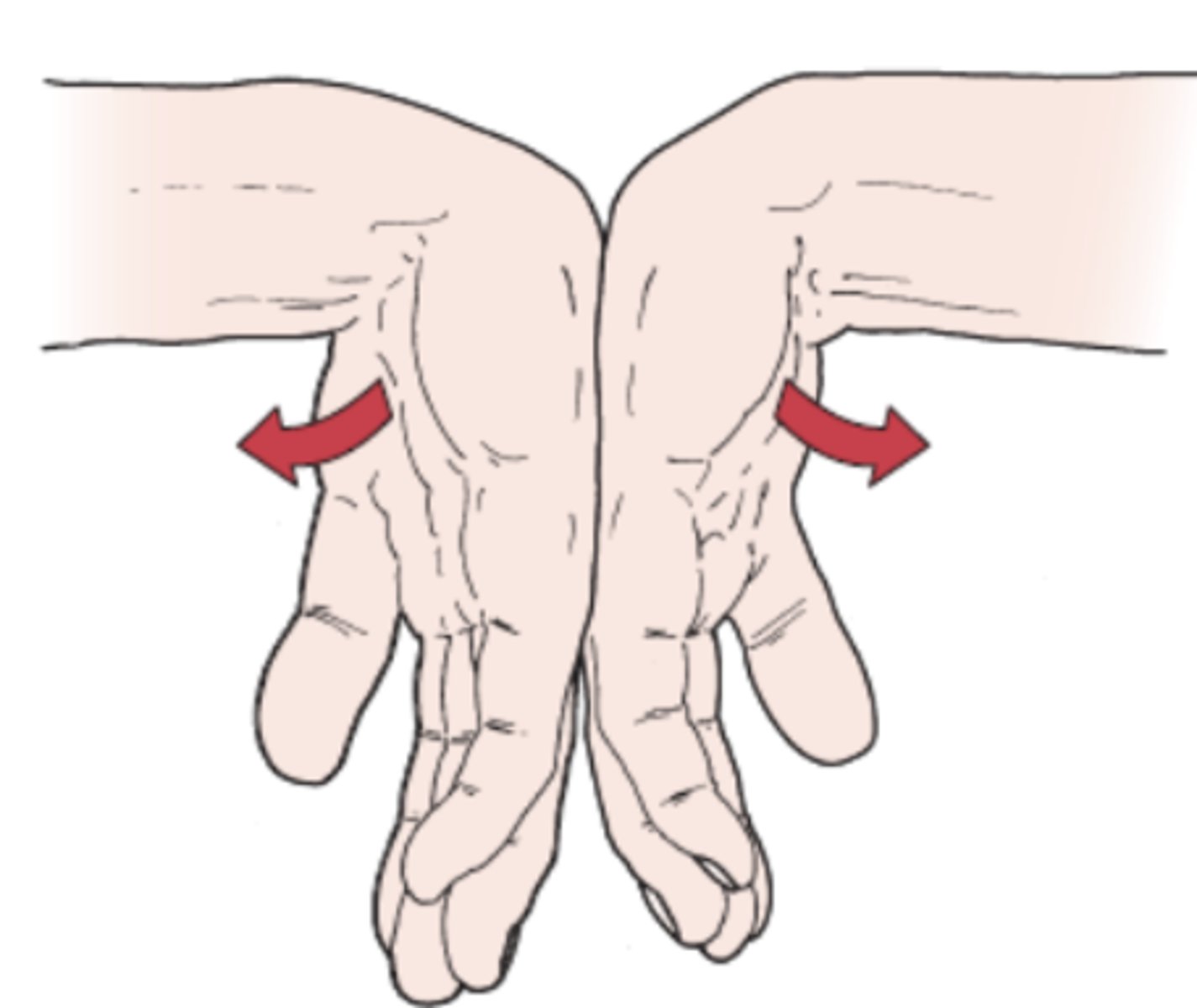
Wartenberg's Sign
- ulnar nerve neuropathy
- palmar interossei paralysis = results in small finger being more abducted relative to unaffected side, due to unopposed pull of extensor digiti minimi and extensor digitorum
(+): inability to squeeze little fingers to the remainder of the hand indicates a positive test for ulnar neuropathy

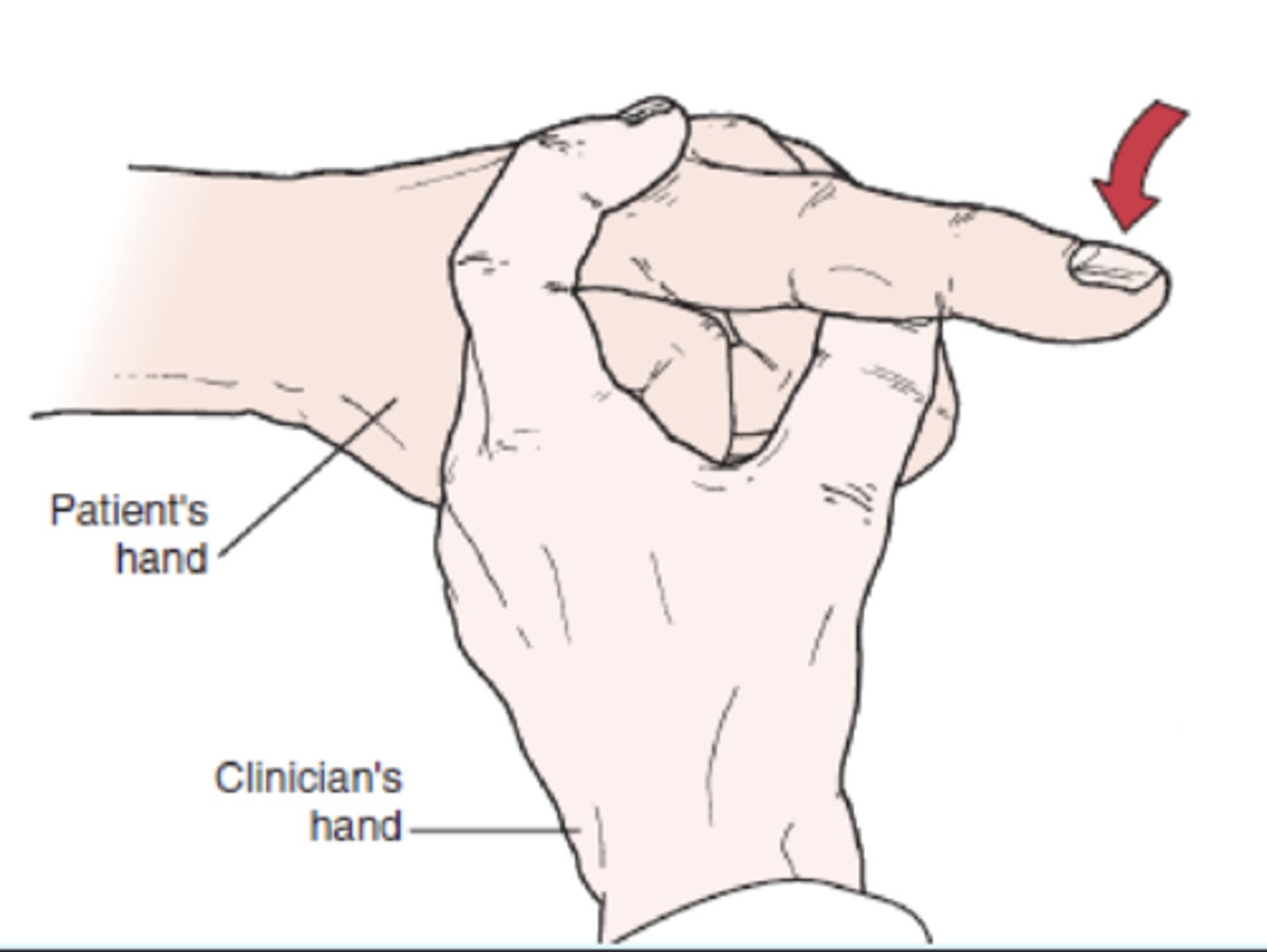
Hoffman's Sign
- UMN dysfunction
- description: PT holds the pt's middle finger and briskly flicks the distal phalanx
(+): if interphalangeal joint of thumb of the same hand flexes/adducts. Fingers may also flex

Thumb Grind Test
- identify degenerative joint disease in the metacarpophalangeal or metacarpotrapezial joint
- The examiner holds the patient's hand with one hand and grasps the patient's thumb below the metacarpophalangeal joint with the other hand. The examiner then applies axial compression and rotation to the metacarpophalangeal
joint
(+): If pain is elicited, the test is positive and indicative of degenerative joint disease in the metacarpophalangeal or metacarpotrapezial joint

Murphy's Sign (wrist)
- lunate dislocate
- The patient is asked to make a fist. If the head of the third metacarpal is level with the second and fourth metacarpals, the sign is positive and indicative of a lunate dislocation. Normally, the third metacarpal would project beyond (or further distally) the second and fourth metacarpals.

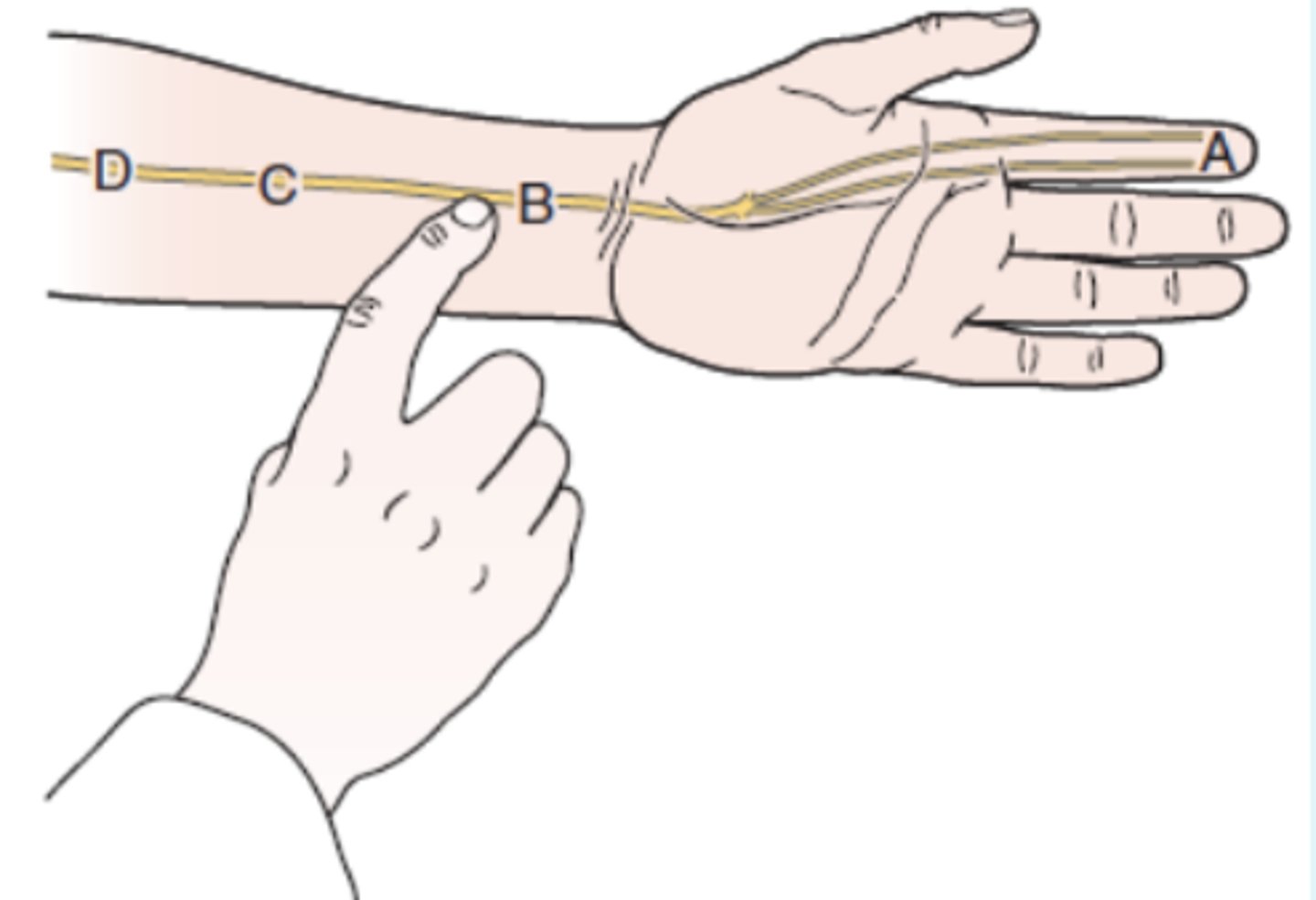
Tinel's Sign (wrist)
- carpal tunnel compression of median nerve
(+): tingling or paresthesia into thumb, index finger, and middle and lateral half of the ring finger
Phalen's Test
- carpal tunnel compression of median nerve
description: PT flexes the pt's wrist maximally and holds this position for 1 minute by pushing the pt's wrist together.
(+): production of pt's symptoms indicates positive test for carpal tunnel syndrome.
- The test may also involve flexing the wrist 60° before applying the pressure and whether symptoms are relieved when the examiner lets go. The wrist flexion is felt to make the test more sensitive
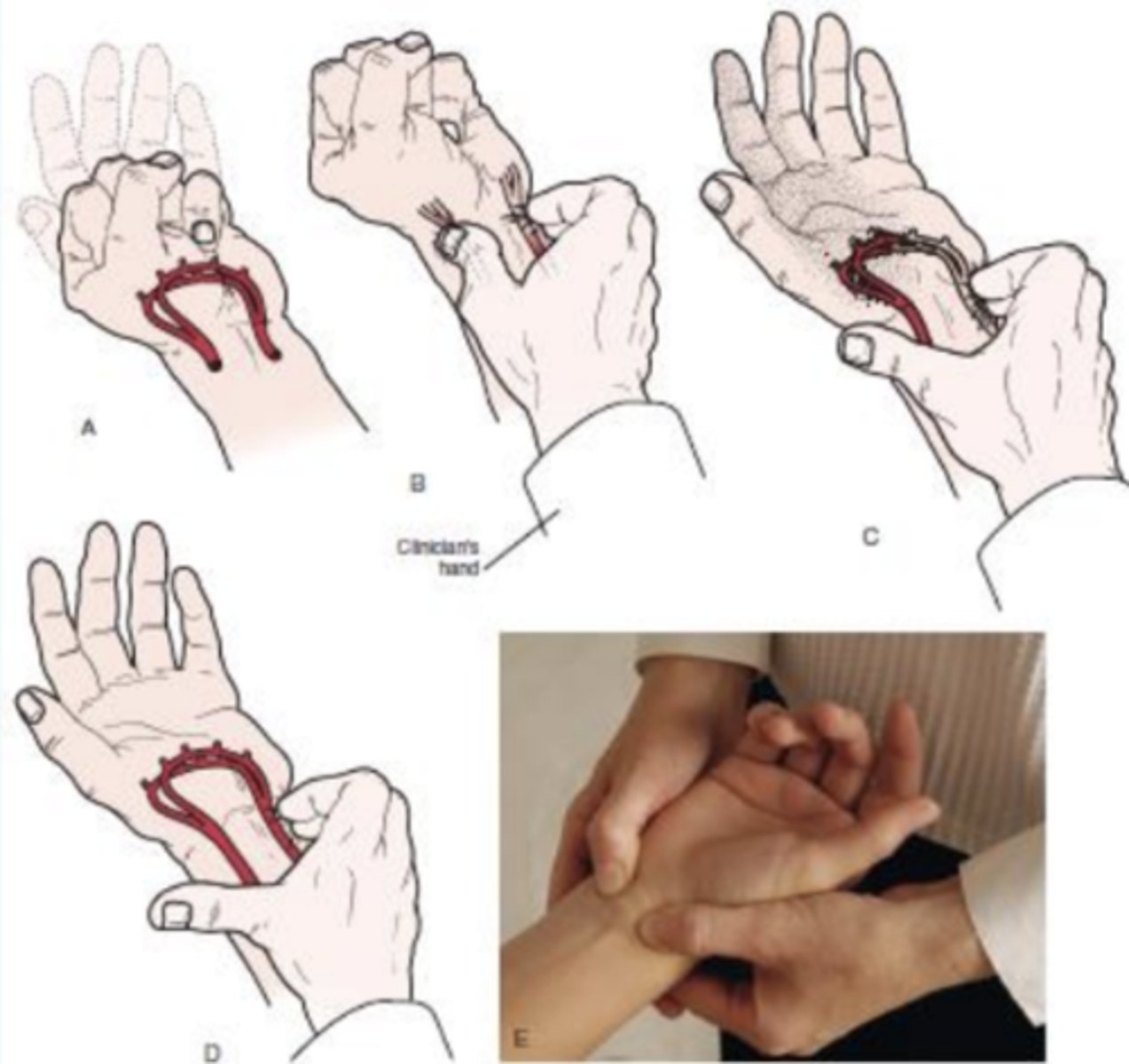
Allen's Test
- identify vascular compromise
- The patient is asked to open and close the hand several times as quickly as possible and then squeeze the hand tightly. The examiner's thumb and index finger are placed over the radial and ulnar arteries, compressing them. The patient then opens the hand while pressure is maintained over the arteries. One artery is tested by releasing the pressure over that artery to see if the hand flushes. The other artery is then tested in a similar fashion.
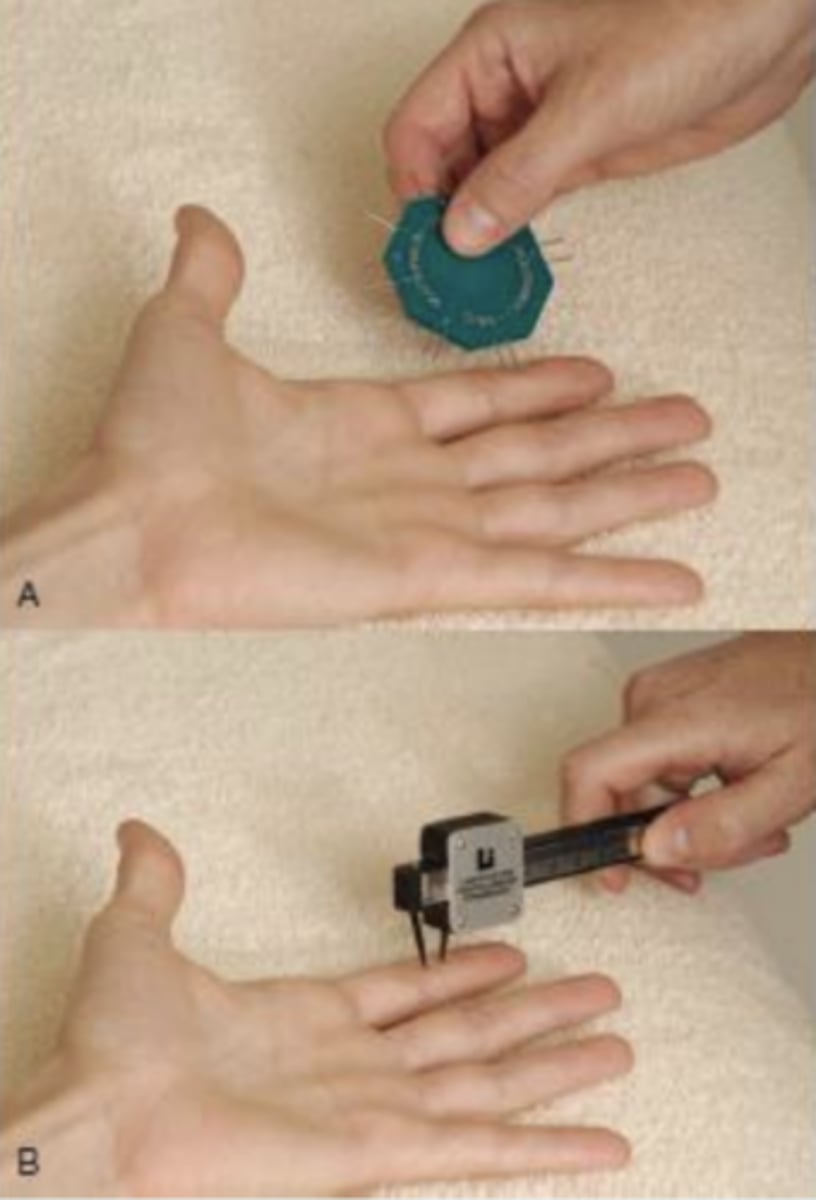
Two Point Discrimination Test
- identify level of sensory innervation in hand
description: PT uses paper clip, two point discriminator or calipers to simultaneously apply pressure on two adjacent points in a longitudinal direction - or perpendicular to the long axis of the finger; the PT moves proximal to distal in an attempt to find the minimal distance at which the pt can distinguish between two stimuli
- only fingertips need to be test.
normal discrimination distance recognition is less than 6 mm.
FABER Test (patrick's test)
hip dysfunction (mobility restriction)
(+): A positive test is indicated by the test leg's knee remaining above the opposite straight leg. Positive the test indicates that the hip joint may be affected, that there may be iliopsoas spasm, or that the sacroiliac joint may be affected.
groin pain reproduction during the test indicates iliopsoas pathology, psoas impingement or anterior capsule involvement
posterolateral pain is suggestive of ischiotrochanteric impingement

WHAT (wrist hyperflexion abduction of thumb) Test
- rule out De Quervain's tenosynovisitis
- stresses Abductor Pollicis longus and extensor pollicis brevis
- patient's wrist fully flexed with thumb in full abduction and full extension. Examiner applies force into adduction and flexion while the patient resists.
(+): reproduction of pain

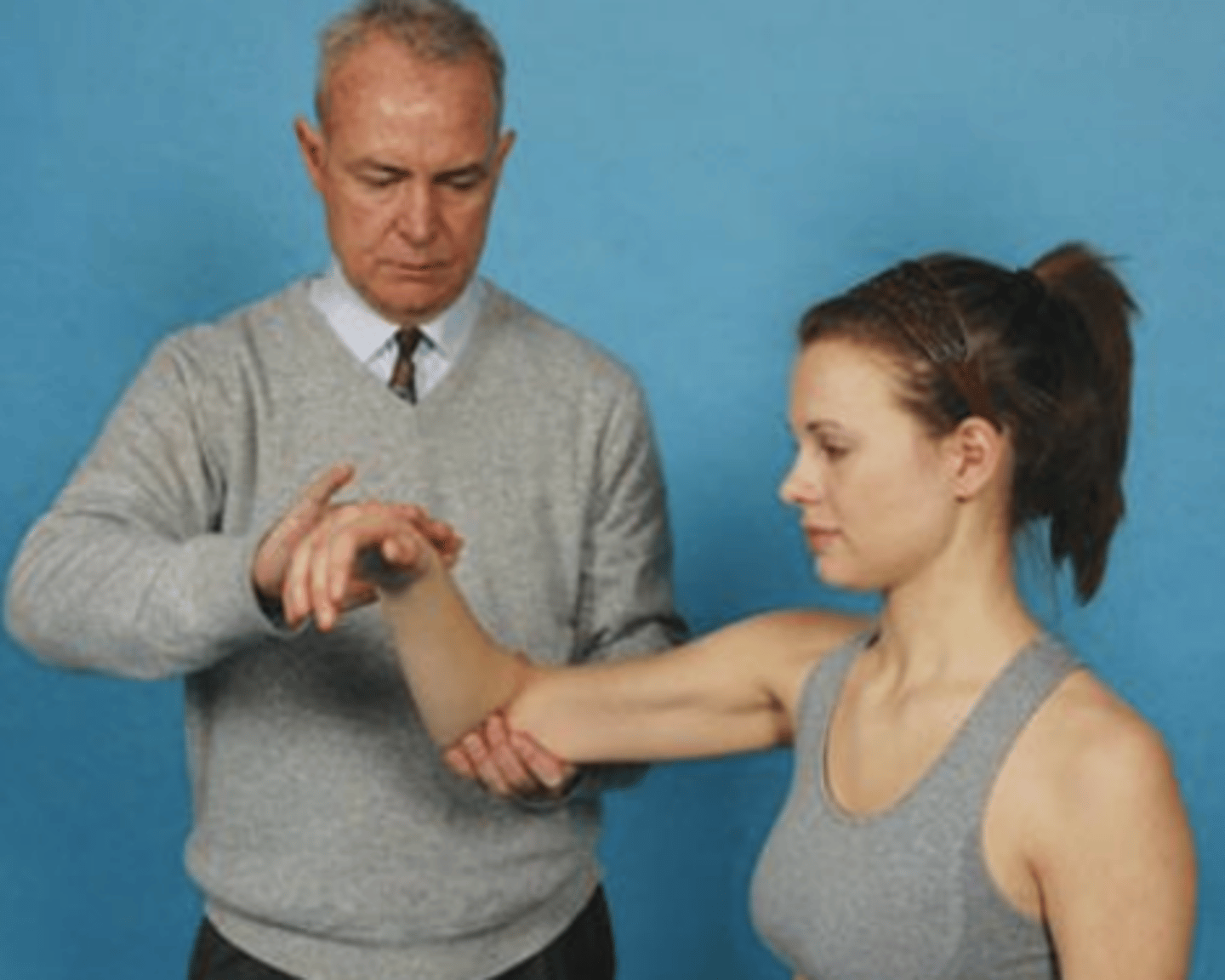
Watson's Test
- scaphoid-lunate instability
procedure:
- Patient in sitting with elbow resting on treatment table Pt then fixates the patient's radius with one hand and give pressure into dorsal direction on the palmar prominence of the scaphoid with his thumb With the other hand, examiner grasps patient's metacarpals from the ulnar side to control the wrist Examiner bring the wrist from maximal ulnar deviation and slight extension into maximal radial deviation and slight flexion and releases the pressure of the thumb on scaphoid
(+): Scaphoid shifts back ventrally upon the release of the thumb and produces a painful "thunk" sound. Or reproduces the patient familiar wrist pain on the dorsal side

Scour Test
- DJD of hip joint
description: pt lies supine, the PT flexes and adducts the pt's hip so that the hip faces the pt's opposite shoulder and resistance to the movement is felt.
(+): reproduce pain or refer pain to knee

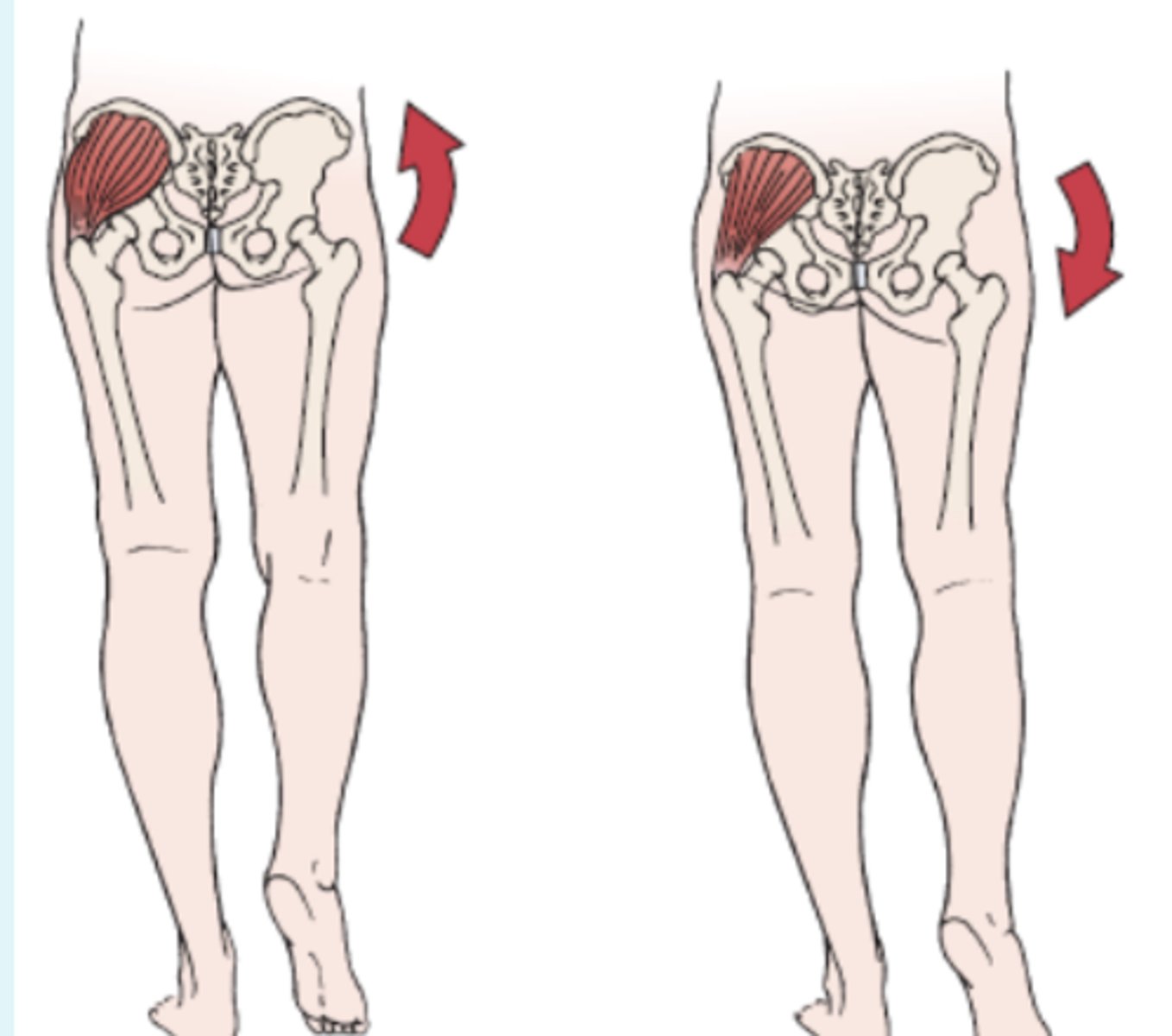
Trendelenburg Sign
- identify weakness of Gluteus Medius or unstable hip joint
- The patient is asked to stand on one lower limb. Normally, the pelvis on the opposite side should rise; this finding indicates a negative test
(+): If the pelvis on the opposite side (non-stance side) drops when the patient
stands on the affected leg, a positive test is indicated.
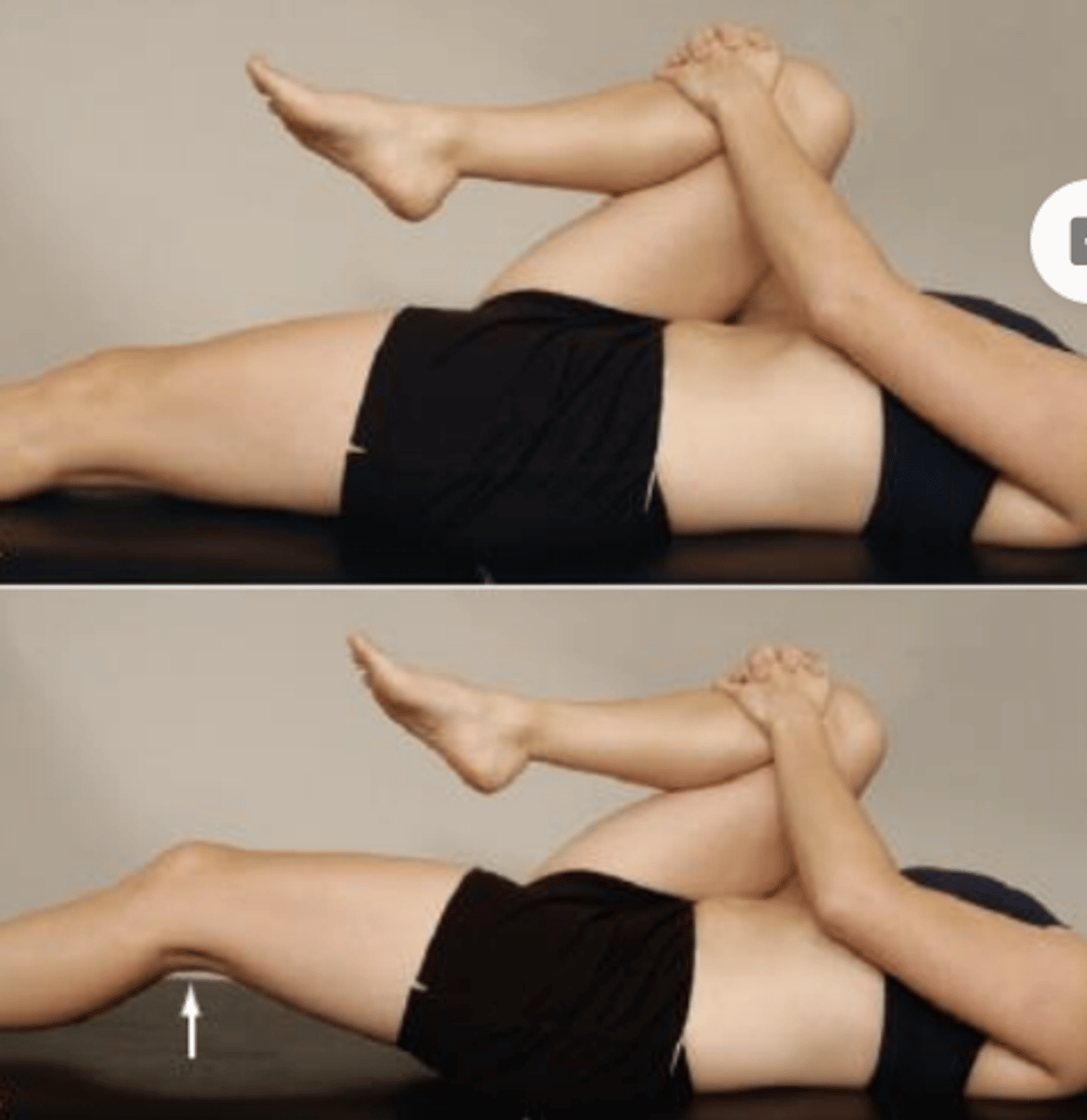
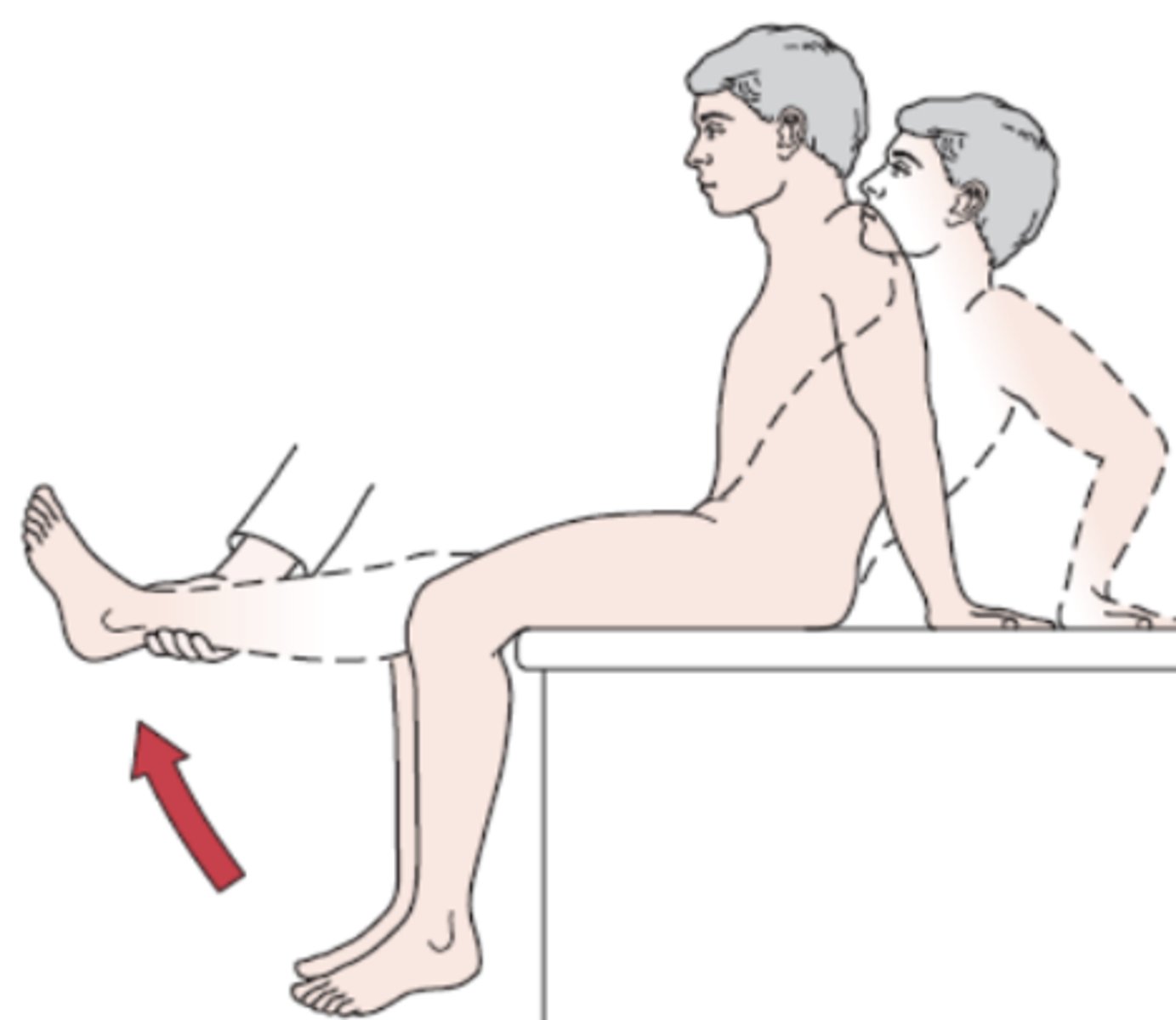
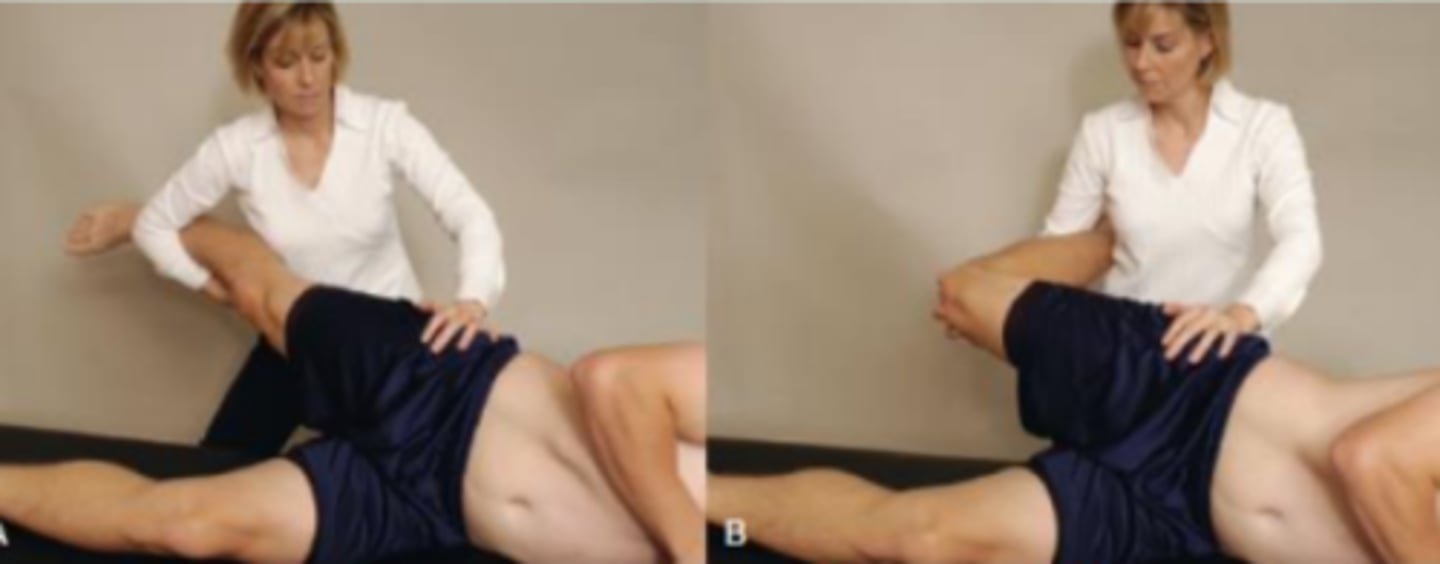
Thomas Test
- tightness of hip flexors
Procedure:
- The patient lies supine while the examiner checks for excessive lordosis, which is usually present with tight hip flexors. The examiner flexes one of the patient's hips, bringing the knee to the chest to flatten out the lumbar spine and to stabilize the pelvis. The patient holds the flexed hip against the chest.
(+): If there is no flexion contracture, the hip being tested (the straight leg) remains on the examining table. If a contracture is present, the patient's straight leg rises off the table and a muscle stretch end feel will be felt
***The Thomas test screens for hip flexor tightness. The iliopsoas is a one-joint hip flexor; when it is tight, the test-side thigh cannot reach the table and rises into hip flexion. Because the knee remains at 90° of flexion, the rectus femoris (a two-joint muscle that flexes the hip and extends the knee) is of adequate length. The combination of thigh lift-off with the knee staying at 90° localizes the restriction to a one-joint hip flexor, the iliopsoas. B. A two-joint hip flexor (rectus femoris): tightness here would additionally pull the knee into extension; since the knee remains at 90
Ober's Test
- tightness of TFL / IT band
(+): leg remains abducted and does not fall to table

Ely's Test
- tightness of rectus femoris
(+): on flexion of knee, pt's hip on same side spontaneously flexes, indicated tight rectus femoris

90-90 Hamstring Test
- hamstring tightness
(+): if knee is unable to reach 10 degrees from neutral position, lacking 10 degree of extension

Tripod Sign
- tightness of hamstrings
Procedure:
- The patient is seated with both knees flexed to 90° over the edge of the examining table. The examiner then passively extends one knee. If the hamstring muscles on that side are tight, the patient extends the trunk to relieve the tension in the hamstring muscles. The leg is returned to its starting position, and the other leg is tested and compared with the first side. Extension of the spine is indicative of a positive test.
(+): extension of spine
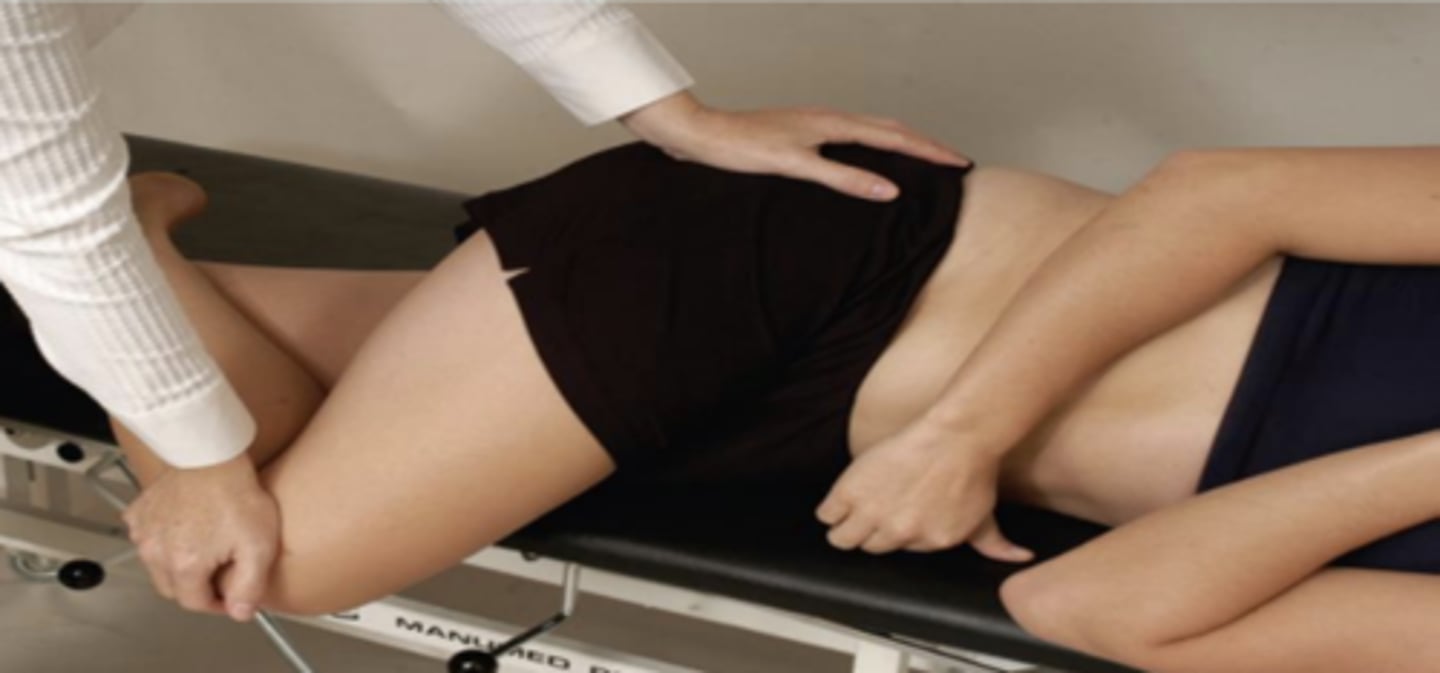
Piriformis Test
- piriformis syndrome
Procedure:
- The patient is in the side lying position with the test leg uppermost. The patient flexes the test hip to 60° with the knee flexed. The examiner stabilizes the hip with one hand and applies a downward pressure to the knee
(+): If the piriformis muscle is tight, pain is elicited in the muscle. If the piriformis muscle is pinching the sciatic nerve, pain results in the buttock and sciatica may be experienced by the patient
Leg Length Test
- true leg length discrepancy
Procedure:
- True leg length is measured by placing the patient in a supine position with the ASISs level and the patient’s lower limbs perpendicular to the line joining the ASISs. Using a flexible tape measure, the examiner obtains the distance from the ASIS to the medial or lateral malleolus on the same side. The measurement is repeated on the other side, and the results are compared.
(+): a difference of 1 to 1.3 cm (0.5 to 1 inch) is considered normal

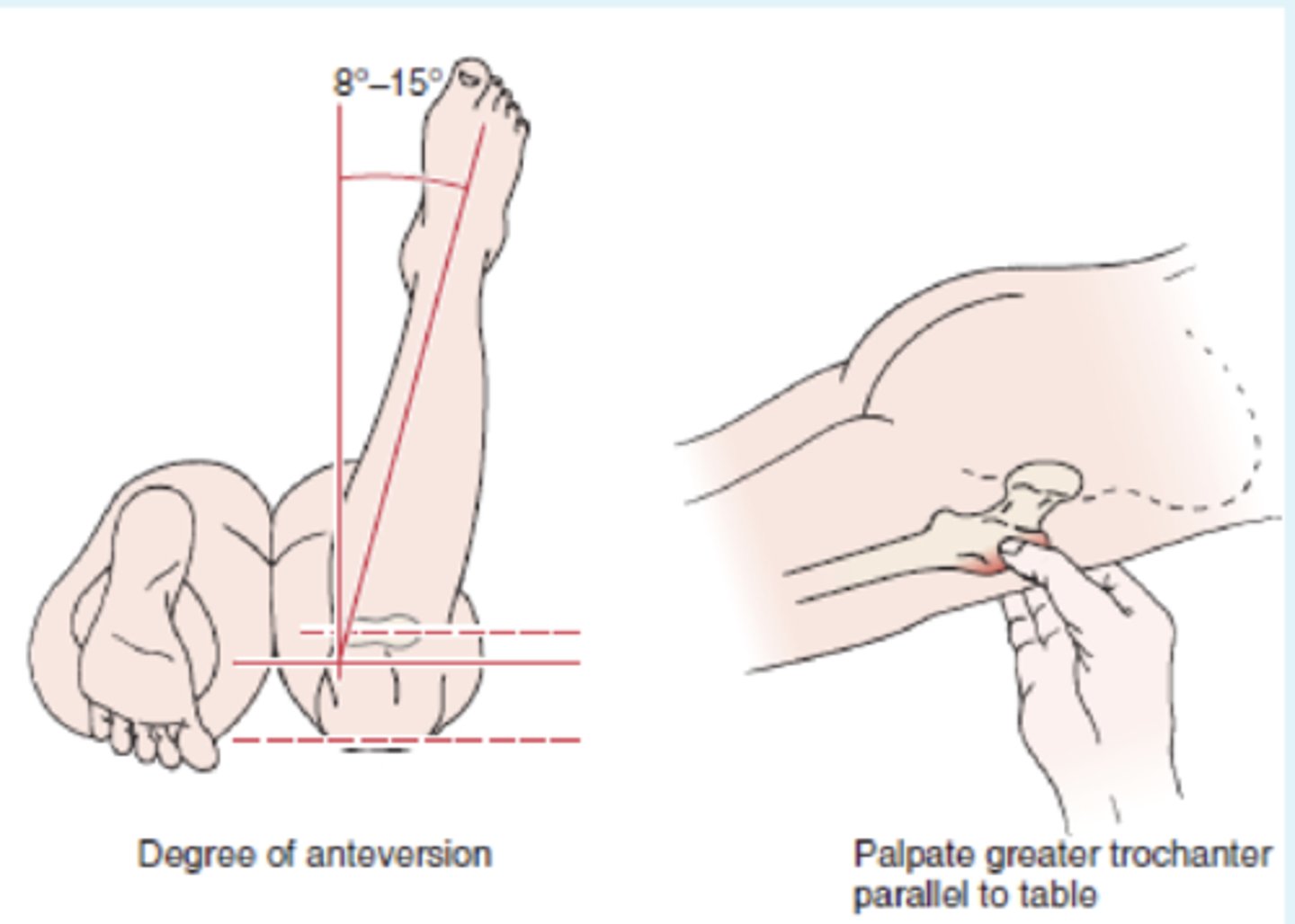
Craig's Test
- identify abnormal femoral anteversion
Procedure:
- The patient lies prone with the knee flexed to 90°. The examiner palpates the posterior aspect of the greater trochanter of the femur. The hip is then passively rotated medially and laterally until the greater trochanter is parallel with the examining table or reaches its most lateral position.
(+): degree of anteversion can be estimated based on the angle of lower leg with the vertical
Normal: 8-15 degrees of IR
Anteversion: angle > 15 degrees; pigeon toed or in-toeing & increase IR
Retroversion: angle < 8 degrees; out-toeing & increased ER
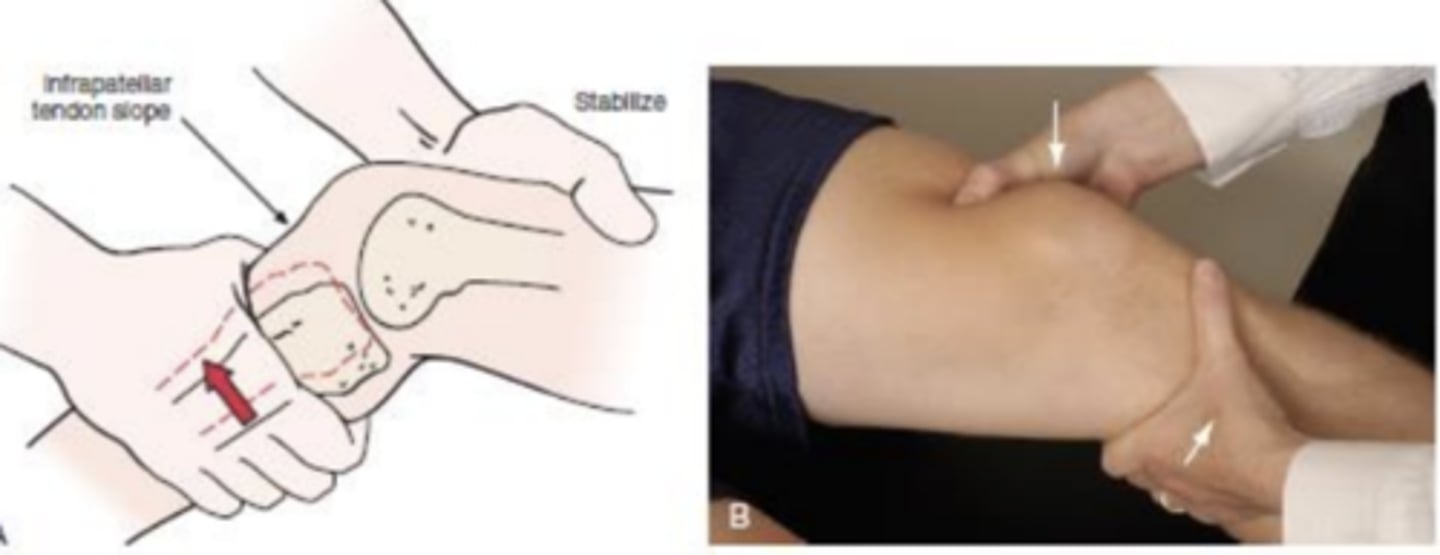
Lachman's test
- ACL
(+): mushy or soft end feel when tibia is moved forward on femur (increased anterior translation with medial rotation of the tibia) and disappearance of the infrapatellar tendon slope
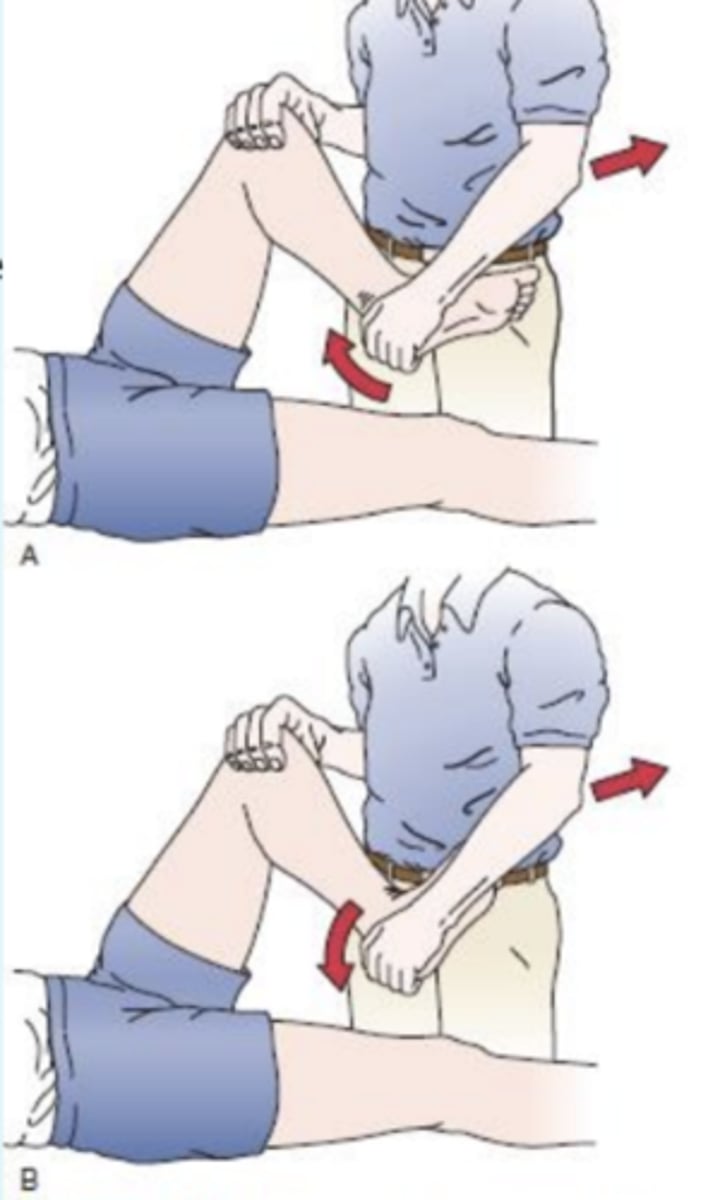
Pivot Shift Test
- ACL
Procedure:
There are two main types of clinical tests to determine the presence of the pivot shift:
1. Reduction test. The clinician stabilizes the patient's lower leg and flexes the knee to 90 degrees with one hand while using the palm of the other hand to medially rotate the tibia, effectively subluxing the lateral tibial plateau. A sudden reduction of the anteriorly subluxed lateral tibial plateau is seen as the pivot shift
2. Subluxation test. This test is effectively the reverse of the reduction test. The test begins with patient's knees flexed. PT internally rotates the patient's tibias with one hand and applies a valgus stress to knee joint with the other hand. The clinician slowly extends the knee, maintaining rotation of the tibia. As the patient's knee reaches full extension, the tibial plateau will be felt to relocate.

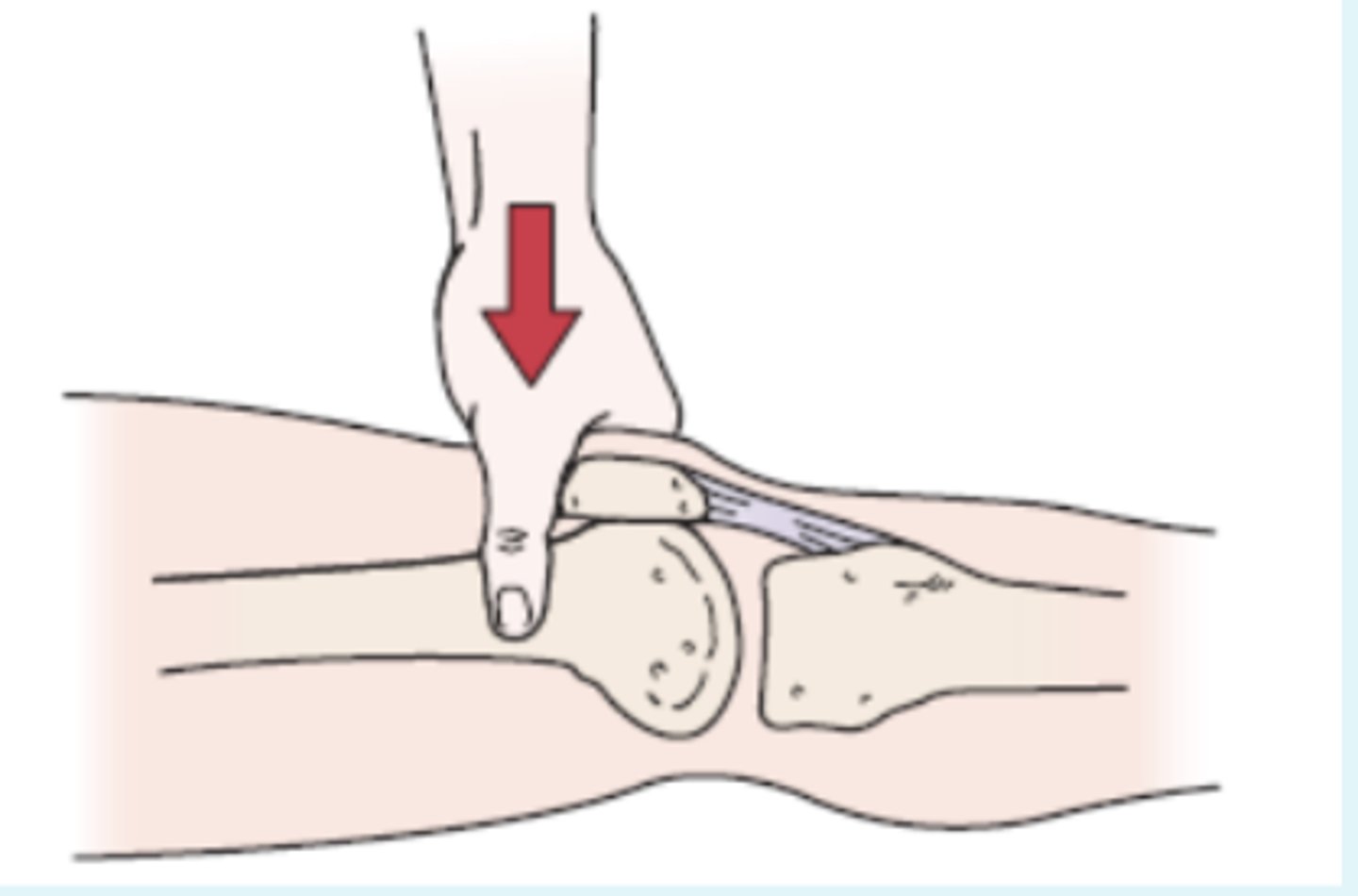
Posterior Sag test
- PCL
- pt lies supine with hip flexed to 45 and knee flexed to 90
(+): tibia drops back or sags back on femur because of gravity if PCL is torn
Slocum Test
- assess both anteromedial and anterolateral rotary instabilities
Procedure:
- The patient's knee is flexed to 80° or 90°, and the hip is flexed to 45°. The foot is first placed in 30° medial rotation. The examiner then sits on the patient's forefoot to hold the foot in position and draws the tibia forward; if the test is positive, movement occurs primarily on the lateral side of the knee. This movement is excessive relative to the unaffected side and indicates ALRI.
In the second part of the test, the foot is placed in 15° of lateral rotation, and the tibia is drawn forward by the examiner. If the test is positive, the movement occurs primarily on the medial side of the knee. This movement is excessive relative to the unaffected side and indicates anteromedial rotary instability
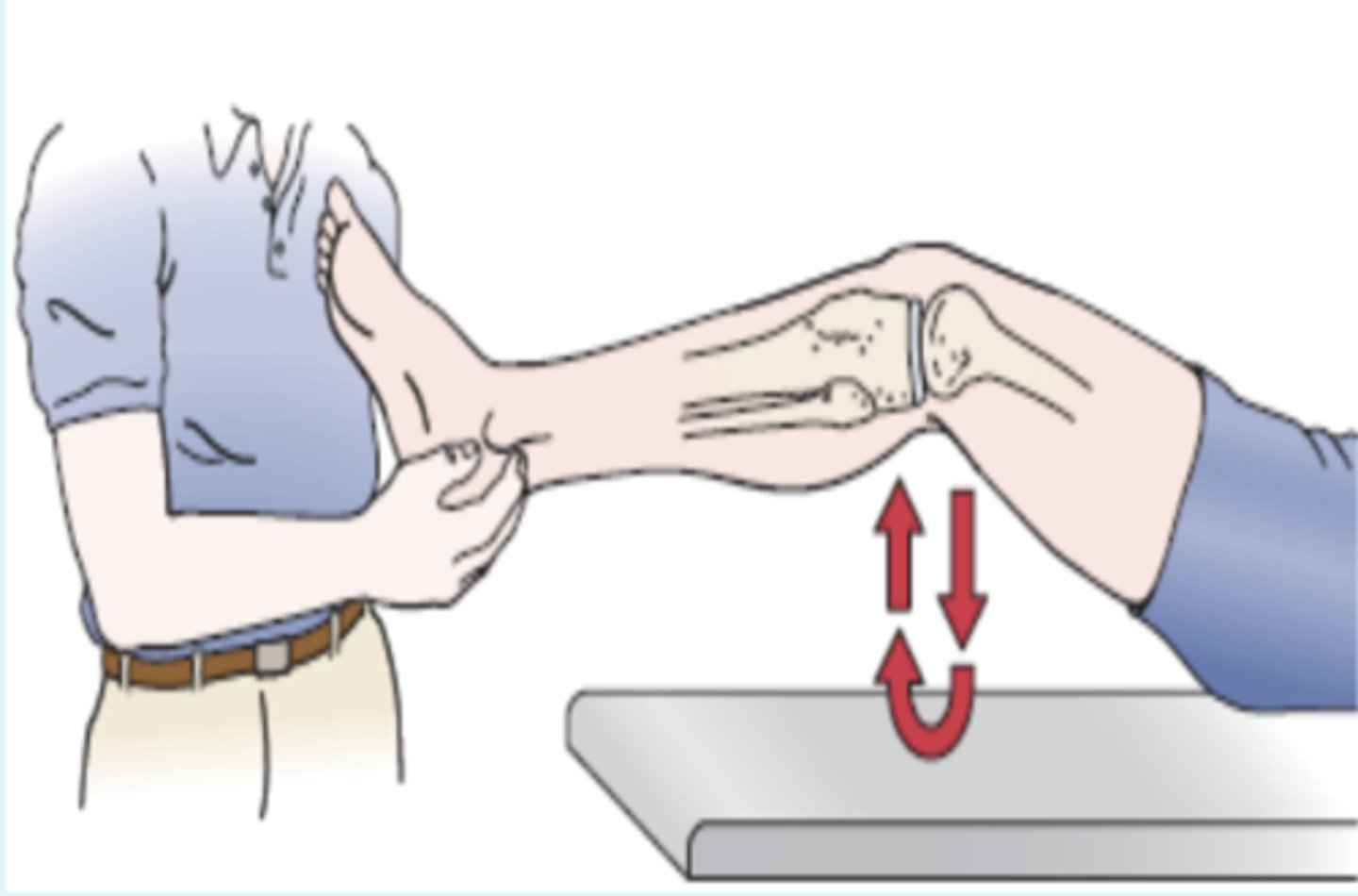
Posterior Drawer Test
- PCL
(+): excess posterior glide

Reverse Lachmans Test
- PCL
Procedure:
- The patient lies prone with the knee flexed to 30°, and the examiner grasps the tibia with one hand while fixing the femur with the other hand. The examiner then pulls the tibia up (posteriorly), noting the amount of movement and the quality of the end feel.

McMurray's Test
- meniscal tears
description: pt lies in supine with knee completely flexed (heel to the buttock). the PT then medially rotates the tibia and extends the knee.
(+): if there is a loose fragment of lateral meniscus, this action causes a snap or click, with pain
test medial meniscus with same procedure except rotate tibia into lateral rotation =
Apley's Test (knee)
- helps differentiate between meniscal tears and ligamentous lesion
Procedure:
- The patient lies in the prone position with the knee flexed to 90°. The patient's thigh is then anchored to the examining table with the examiner's knee. The examiner medially and laterally rotates the tibia, combined first with distraction, while noting any restriction, excessive movement, or discomfort. Then the process is repeated using compression instead of distraction
(+): If rotation plus distraction = ligamentous.
Rotation plus compression = meniscus injury.
Bounce Home Test
- meniscal
Procedure:
- The patient lies in the supine position, and the heel of the patient's foot is cupped in the examiner's hand. The patient's knee is completely flexed, and the knee is passively allowed to extend. If extension is not complete or has a rubbery end feel ("springy block"), there is something blocking full extension.
(+): most likely cause of block is a torn meniscus
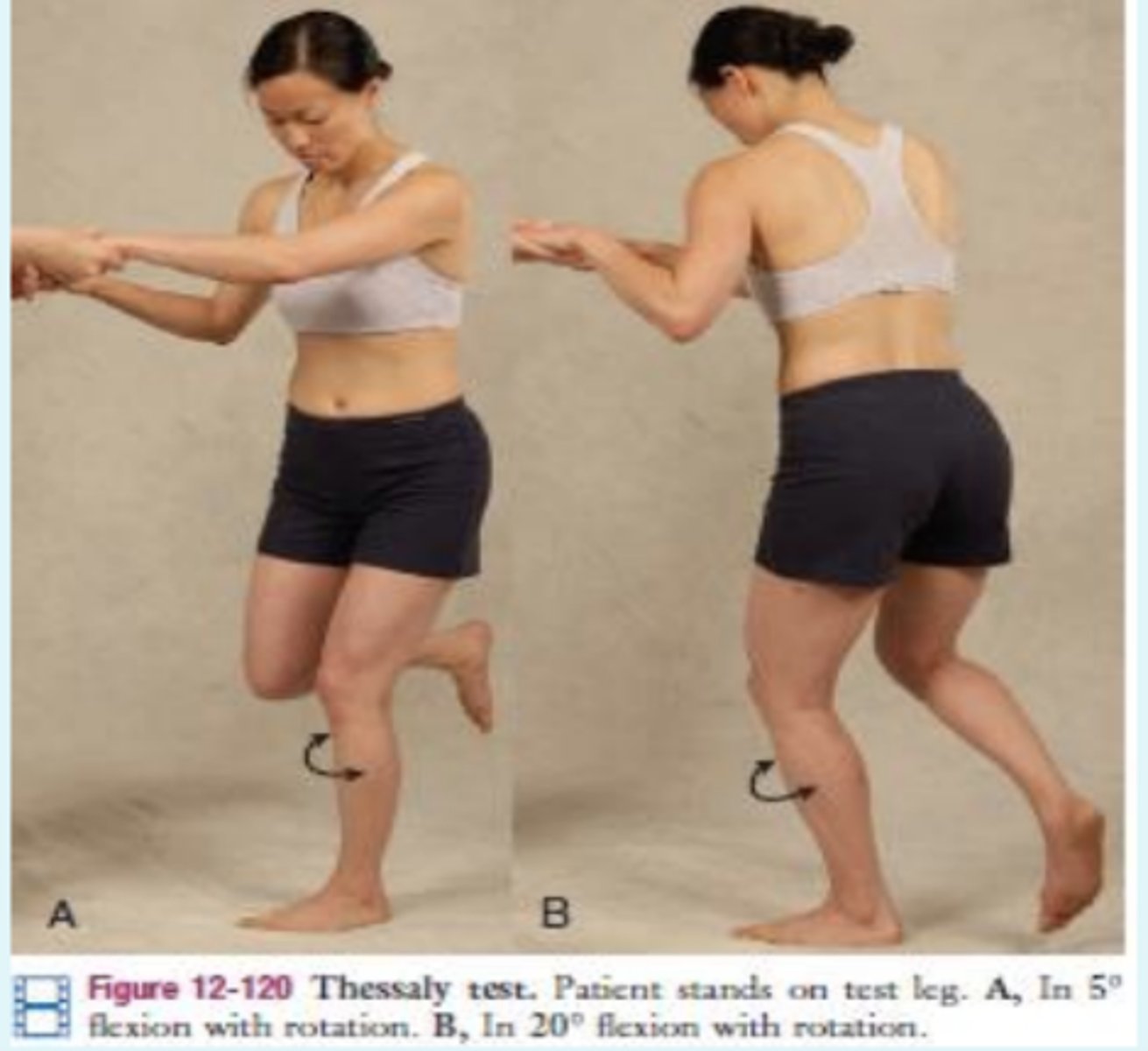
Thessaly Test
- meniscal
(+): pt experiences medial or lateral joint line discomfort. also sense of locking or catching the knee
Hughston's Plica Test
- identify dysfunction of plica
Procedure:
- The patient lies in the supine position, and the examiner flexes the knee and medially rotates the tibia with one arm and hand while pressing the patella medially with the heel of the other hand and palpating the medial femoral condyle with the fingers of the same hand
(+): The patient's knee is passively flexed and extended while the examiner feels for "popping" of the plica band under the fingers. The popping indicates a positive test.
Patellar Apprehension Test
- past history of patella dysfunction
(+): pt doesn't allow the patella to move in lateral direction

Clarke's Sign
- patellofemoral dysfunction
procedure:
- The examiner presses down slightly proximal to the base of the patella with the web of the hand as the patient lies relaxed with the knee extended. The patient is then asked to contract the quadriceps muscles while the examiner pushes down.
(+): If the patient can complete and maintain the contraction without pain, the test is considered negative. If the test causes retropatellar pain and the patient cannot hold a contraction, the test is considered positive.
Ballotable Patella Test
- indicates infrapatellar effusion
procedure:
- pt's knee extended or flexed to discomfort, PT applies a slight tap or pressure over patella
(+): floating of the patella should be felt. this is sometimes called the dancing patella sign

Fluctuation Test
- knee joint effusion
procedure:
- The examiner places the palm of one hand over the suprapatellar pouch and the palm of the other hand anterior to the joint with the thumb and index finger just beyond the margins of the patella
(+): By pressing down with one hand and then the other, the examiner may feel the synovial fluid fluctuate under the hands and move from one hand to the other, indicating significant effusion
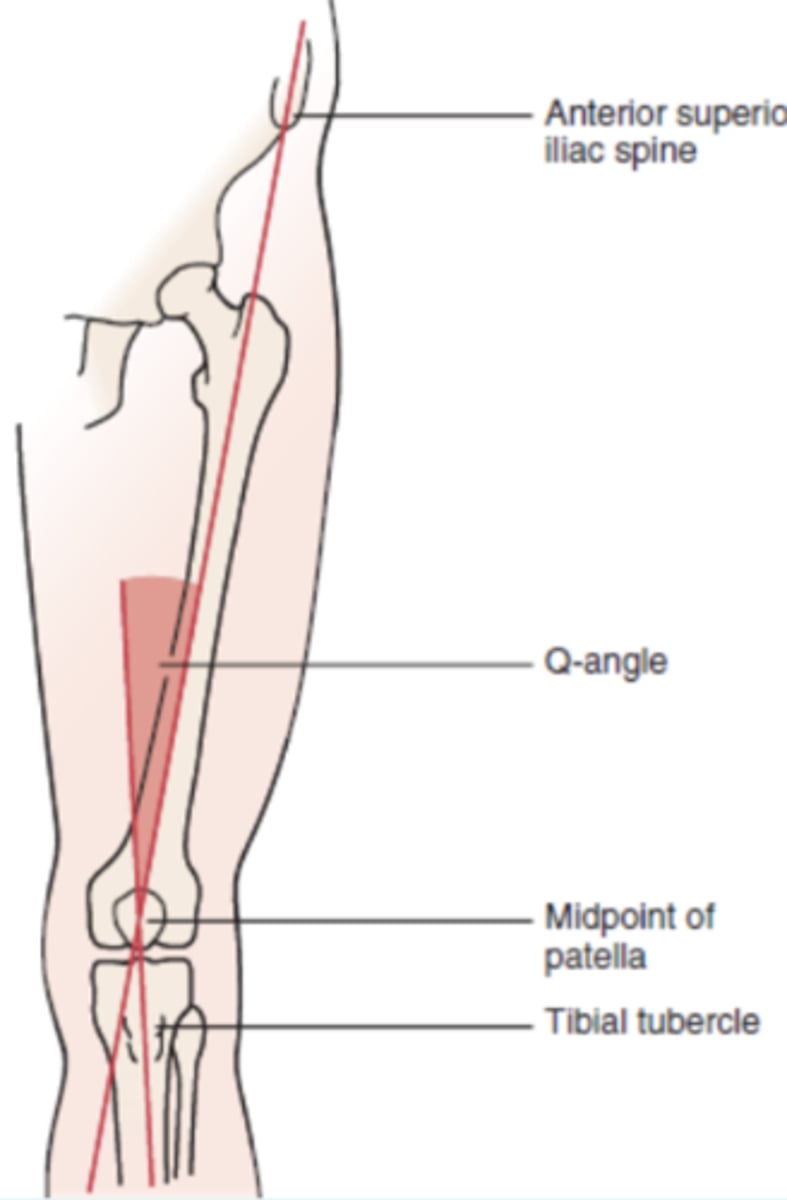
Q angle
- normative values for men at 13 deg and women at 18 deg
- high angle causes quads to pulls on patella / leads to poor tracking-predisposition for pain
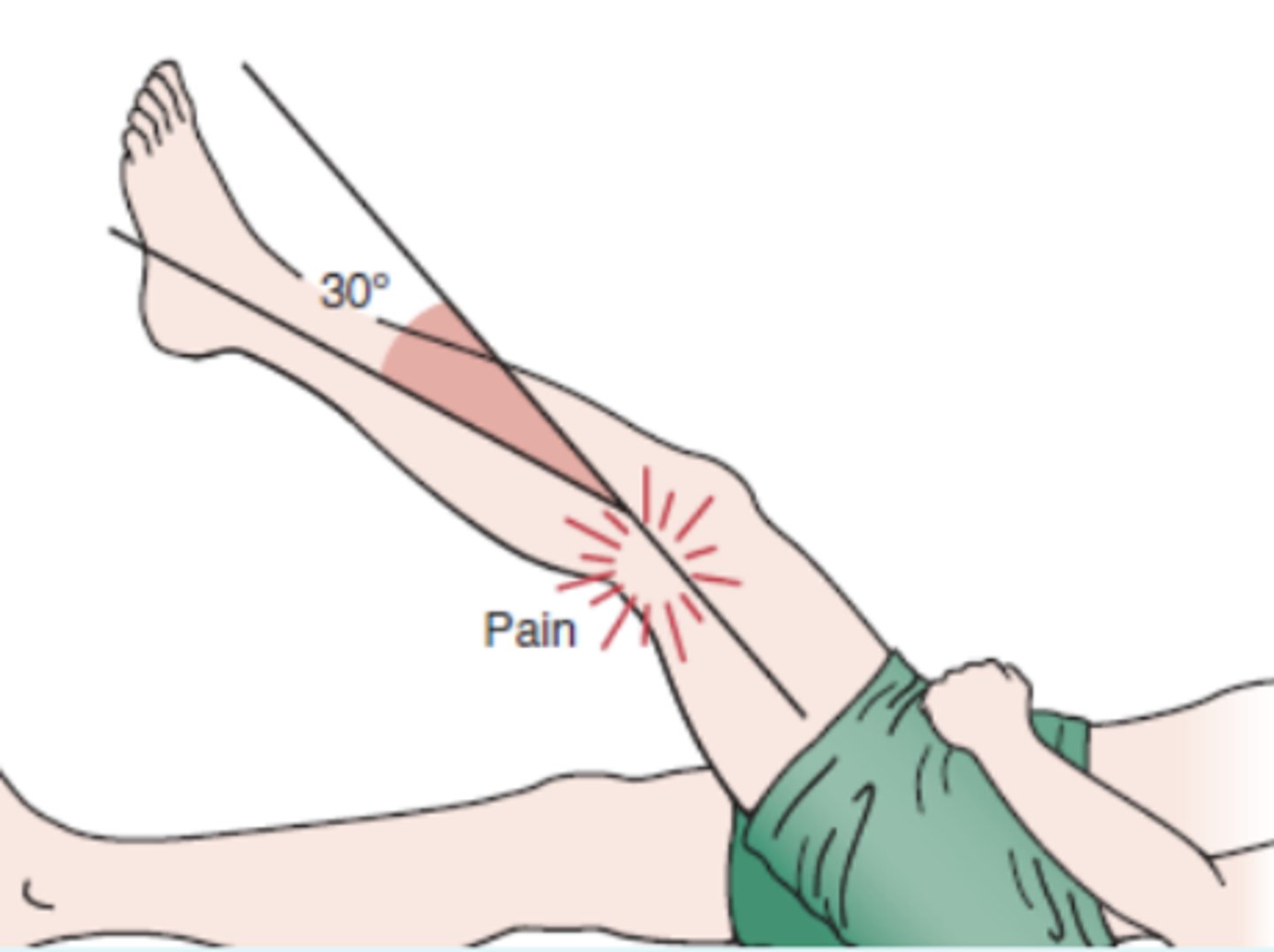
Noble compression test
- distal IT band friction syndrome
procedure:
- The patient lies in the supine position, and the examiner flexes the patient's knee to 90°, accompanied by hip flexion. Pressure is then applied to the lateral femoral epicondyle, or 1 to 2 cm (0.4 to 0.8 inch) proximal to it, with the thumb. While the pressure is maintained, the patient's knee is passively extended
(+): At approximately 30° of flexion (0° being straight leg), the patient experiences severe pain over the lateral femoral condyle
Tinel's Sign (knee)
- dysfunction of common fibular nerve posterior to fibular head
(+): reproduces tingling sensation or paresthesia in leg

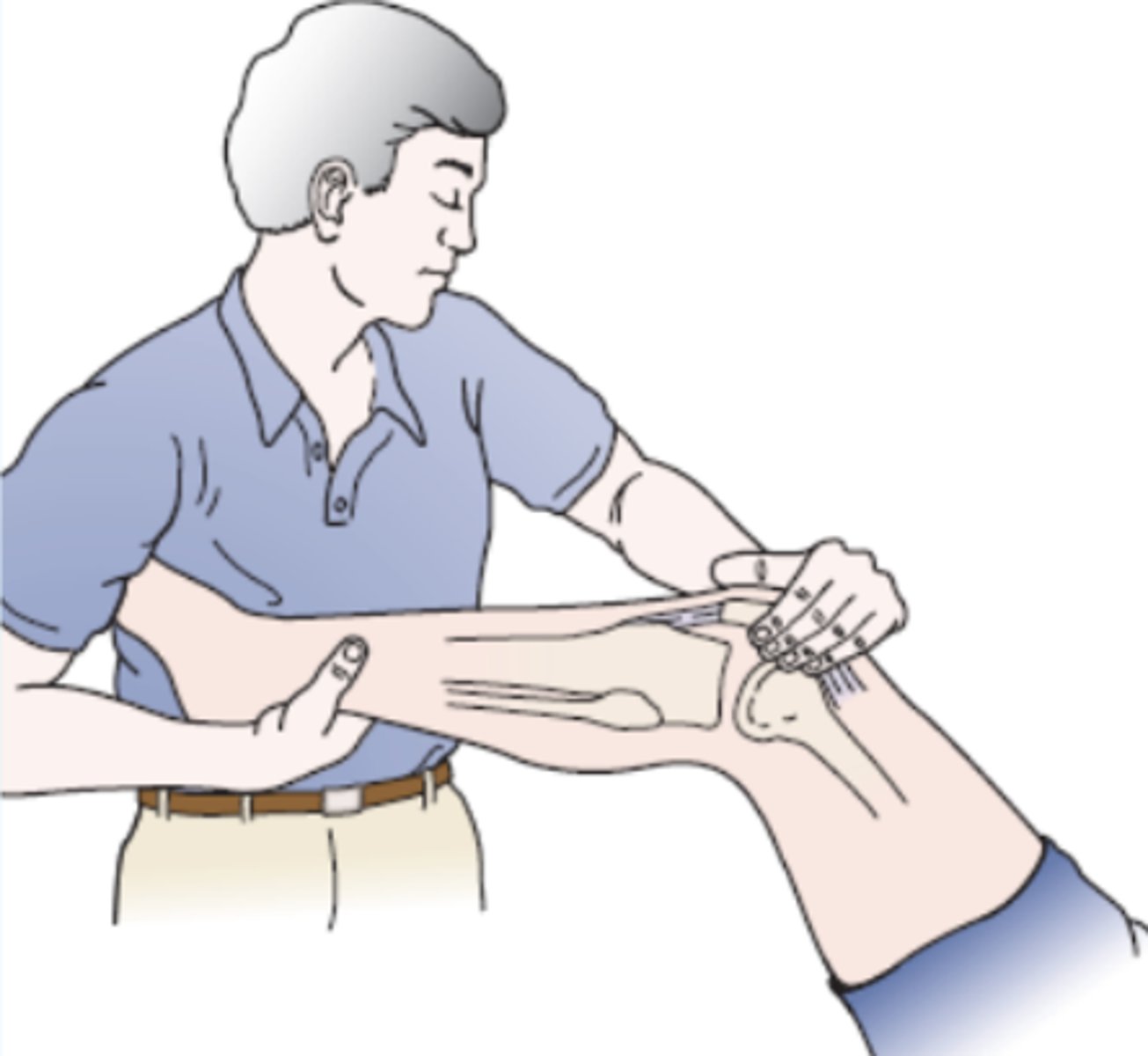
Anterior Drawer Test (ankle)
- anterior talofibular ligament
(+): talus has excessive anterior glide / pain is noted

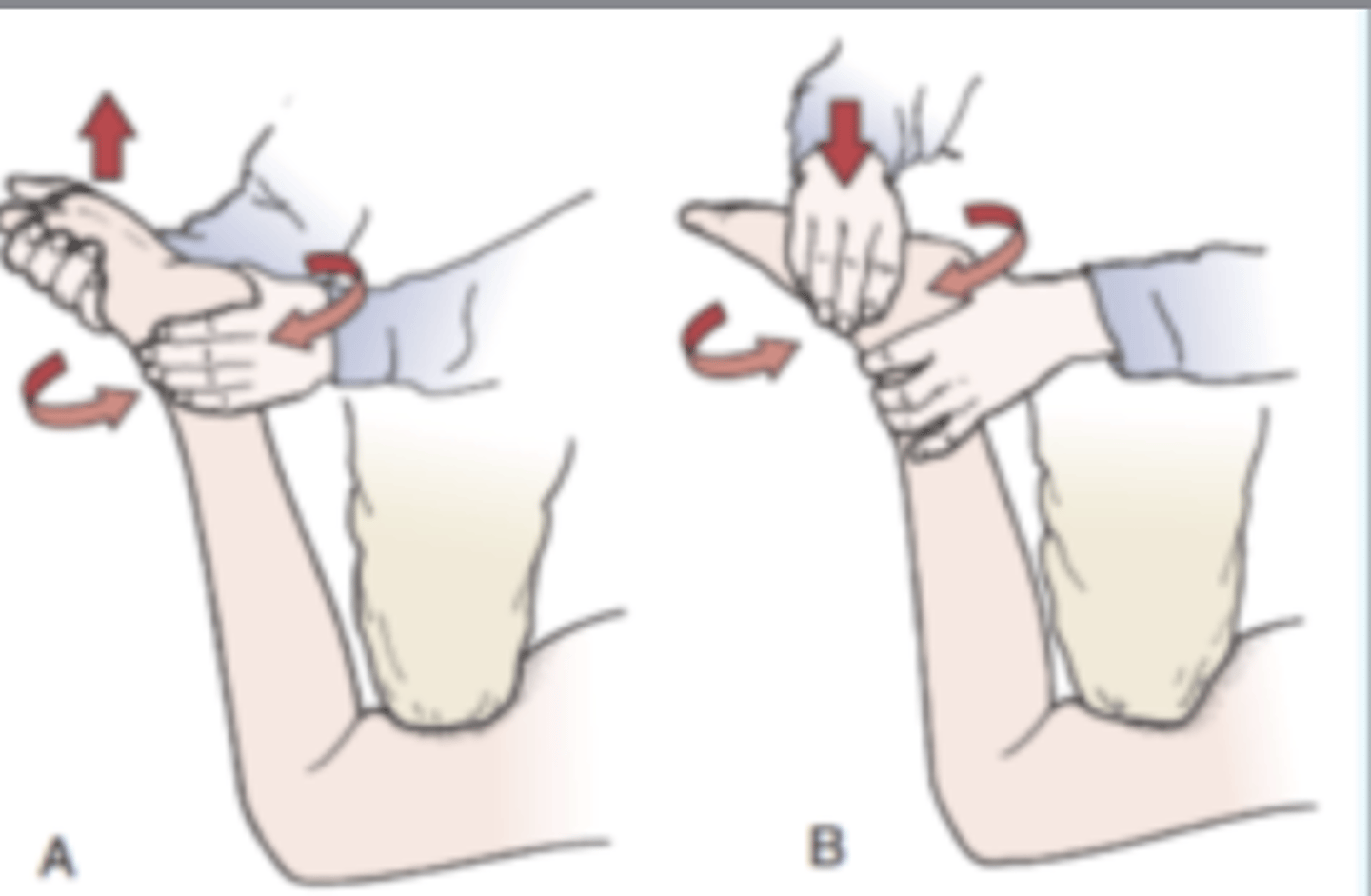
Talar Tilt Test
- instability calcaneofibular ligament
(+): inversion tests the calcaneofibular ligament and eversion stressed the deltoid ligament

External Rotation Stress Test (kleiger's test)
- syndesmosis injury and tear of deltoid ligament
(+): syndesmosis (high ankle) injury is pain is produced over anterior or posterior tibiofibular ligaments and interosseous membrane
- pain is present medially, PT feel talus displace from medial malleolus = deltoid ligament tear

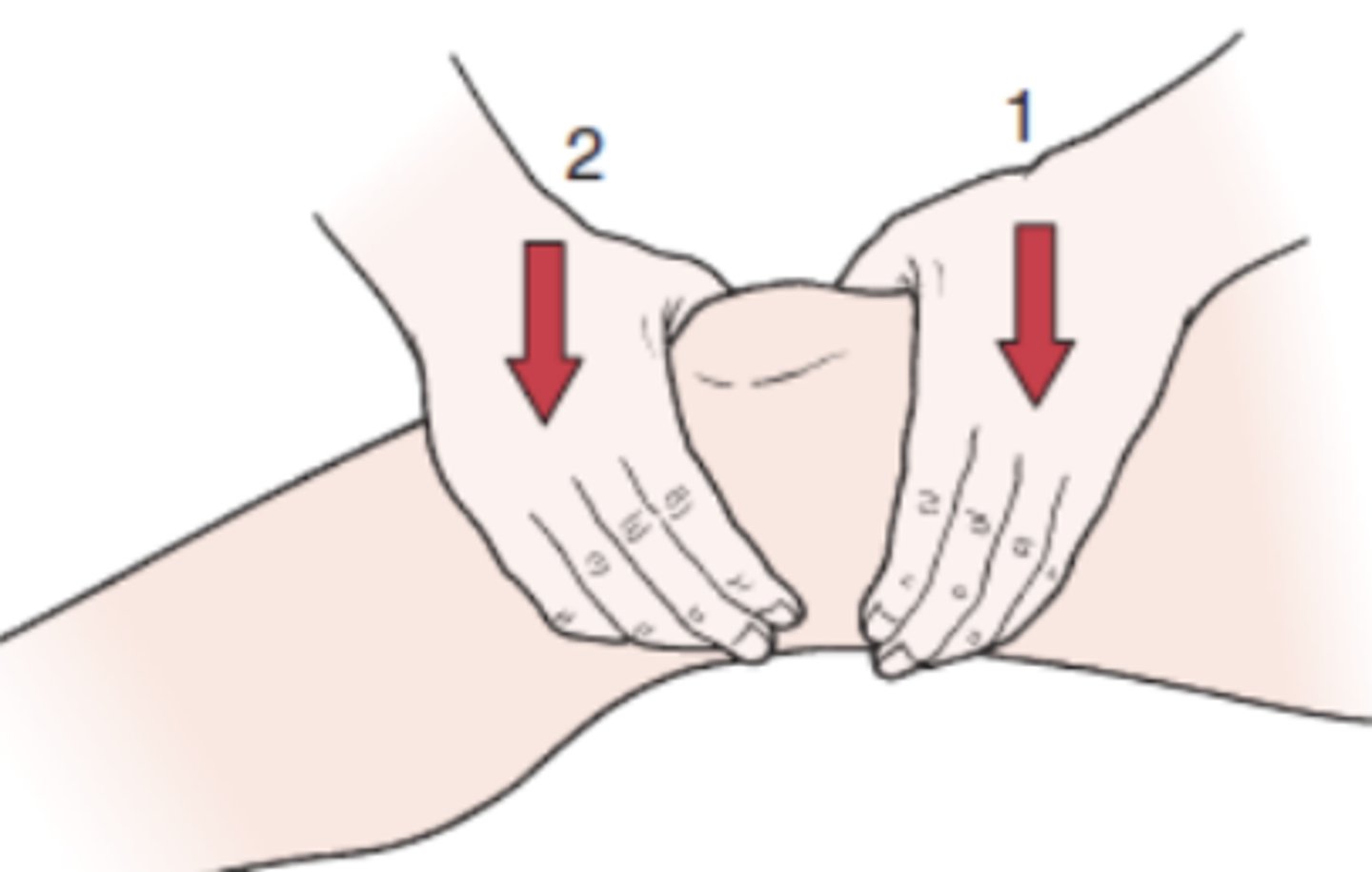
Squeeze Test
syndesmosis integrity
(+): pain in lower leg = syndesmosis injury (rule out fracture, contusion, and compartment syndrome)
A syndesmosis injury of the leg, or "high ankle sprain," is damage to the ligaments connecting the tibia and fibula bones just above the ankle joint. Unlike common ankle sprains, it involves tearing the connective tissue, causing high-ankle pain, swelling, and instability, usually resulting from forceful external rotation of a planted foot.

Thompson's Test
- achilles tendon
(+): absence of PF when muscle is squeeze = ruptured achilles tendon (3rd degree); ThomPson test, Pump the calf to assess achilles

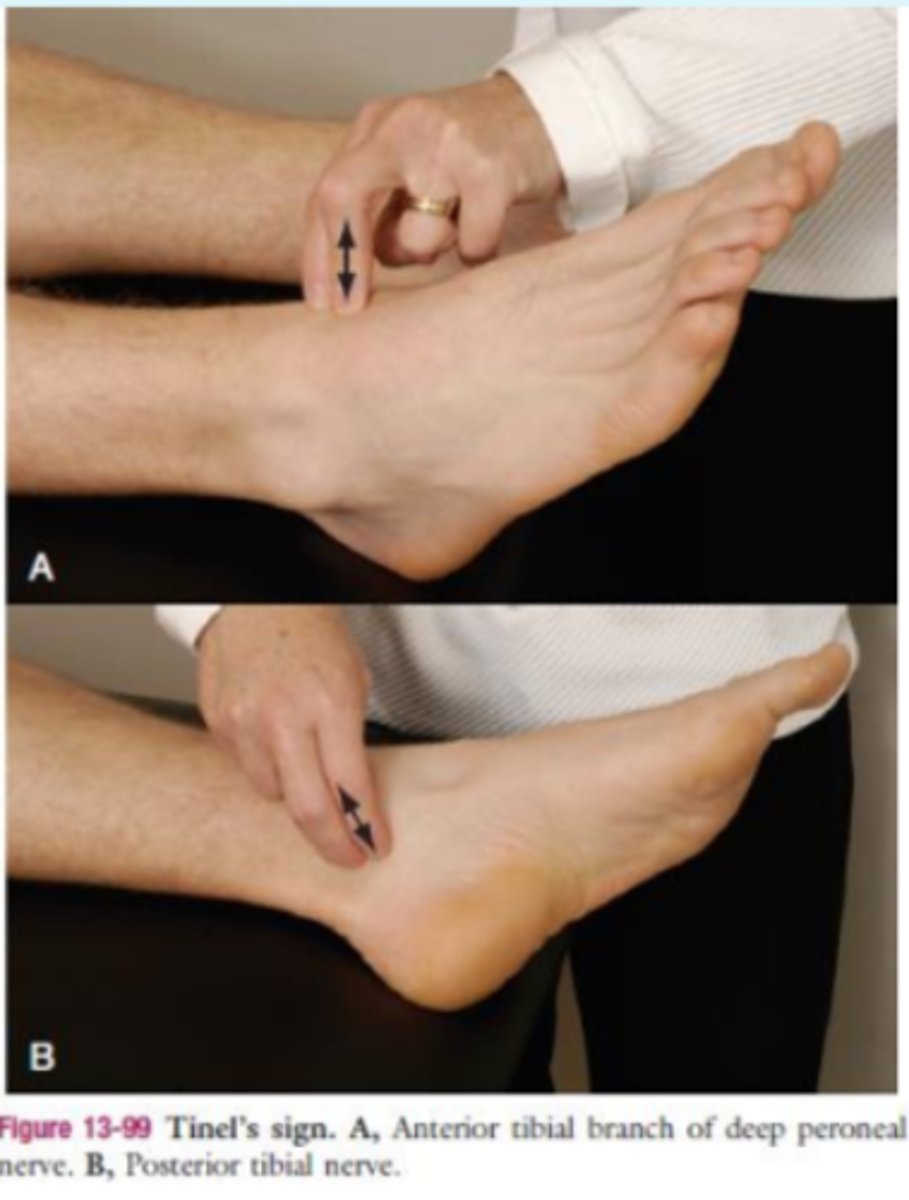
Tinel's Sign (ankle)
- dysfunction of posterior tibial nerve
(+): tingling or paresthesia felt distally
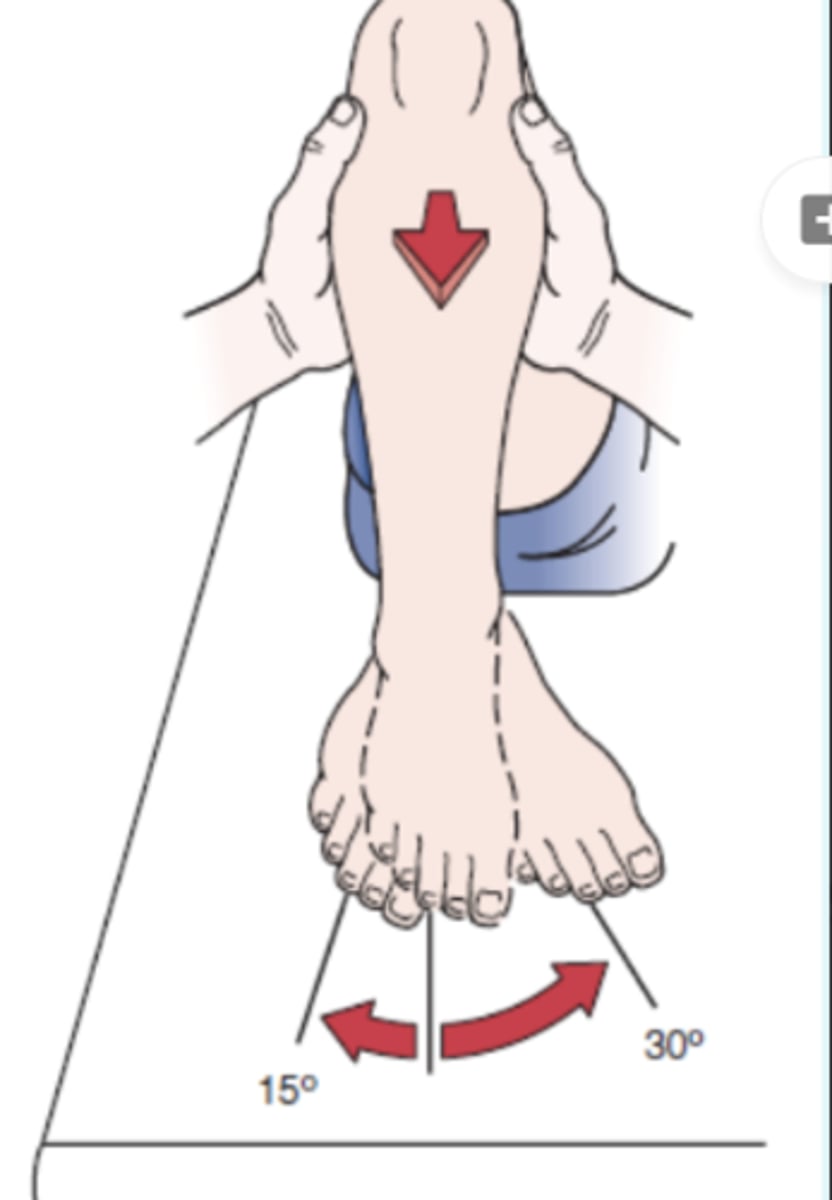
Morton's Test
- stress fracture or neuroma in forefoot
description: pt supine. PT grasps the foot around the metatarsal heads and squeeze the heads together.
(+): pain is positive sign for stress fracture or neuroma.

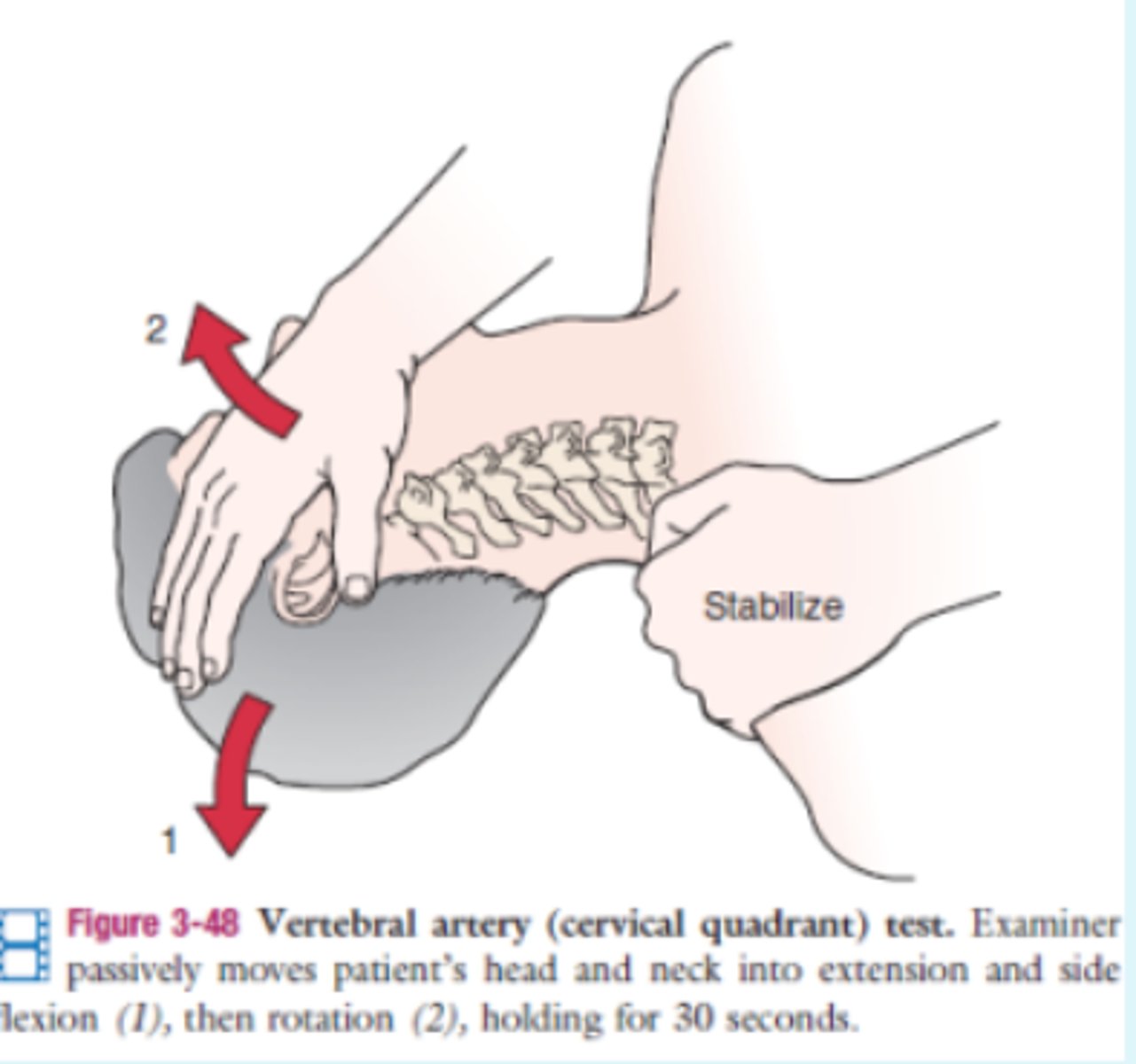
Vertebral Artery Test
- vertebrobasilar vascular
(+): symptoms if the opposite artery is affected
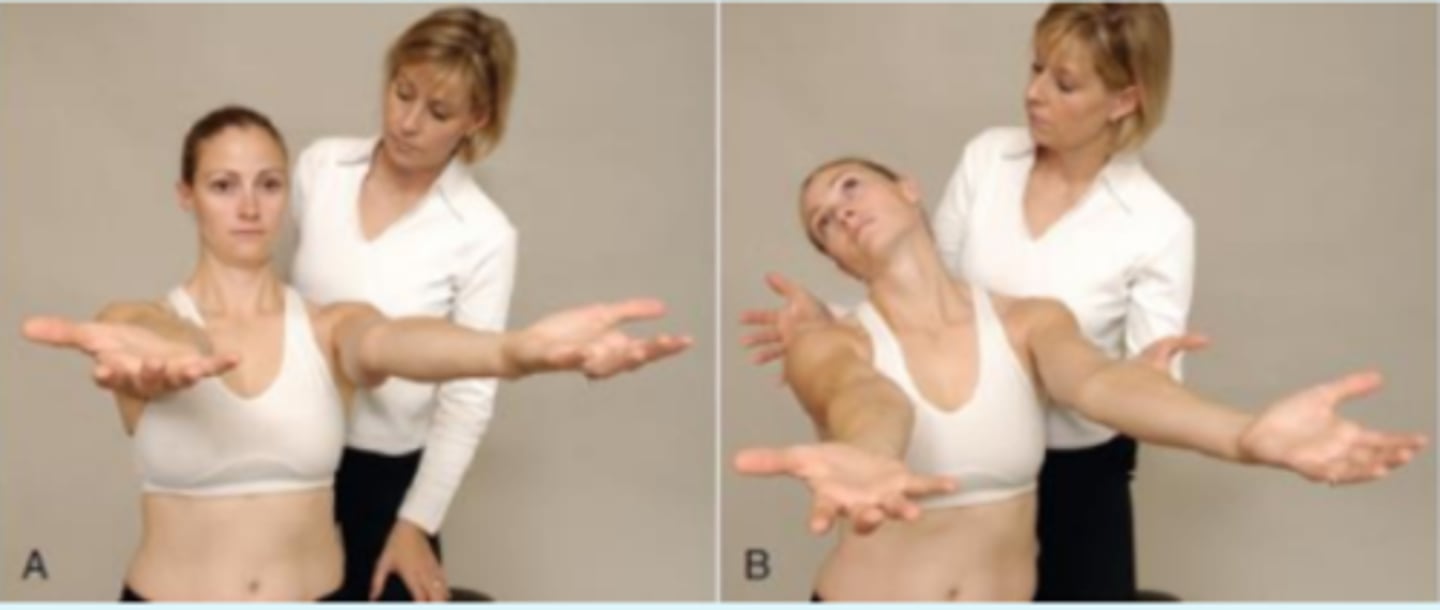
Hautant's Test
- differentiate dizziness or vertigo caused by articular problems for that caused by vascular problems
Procedure:
- The patient sits and forward flexes both arms to 90°.The eyes are then closed. The examiner watches for any loss of arm position. If the arms move, the cause is nonvascular.
(+): The patient is then asked to rotate, or extend and rotate, the neck; this position is held while the eyes are again closed. If wavering of the arms occurs, the dysfunction is caused by vascular impairment to the brain. Each position should be held for 10 to 30 seconds
Transverse Ligament Stress Test
- transverse ligament
procedure:
- The patient lies supine with head supported on the table. Glide C1 anterior. Should be firm end feel. The position is held for 10 to 20 seconds to see whether symptoms occur, indicating a positive test
(+): Positive symptoms include soft end feel; muscle spasm; dizziness; nausea; paresthesia of the lip, face, or limb; nystagmus; or a lump sensation in the throat.

Sharp Purser Test
- subluxation of atlas on the axis
procedure:
- The examiner places one hand over the patient's forehead while the thumb of the other hand is placed over the spinous process of the axis to stabilize it. The patient is asked to slowly flex the head; while this is occurring, the examiner presses backward with the palm.
(+): A positive test is indicated if the examiner feels the head slide backward during the movement. The slide backward indicates that the subluxation of the atlas has been reduced, and the slide may be accompanied by a "clunk."
MEDICAL EMERGENCY

Anterior Shear Test (cervical)
- integrity of ligaments and capsular tissues
procedure:
- The patient lies supine with the head in neutral, resting on the bed. The examiner applies an anteriorly directed force through the posterior arch of C1 or the spinous processes of C2 to T1 or bilaterally through the lamina of each vertebral body. In each case, the normal end feel is tissue stretch with an abrupt stop
(+): Positive signs, especially when the upper cervical spine is tested, include nystagmus, pupil changes, dizziness, soft end feel, nausea, facial or lip paresthesia, and a lump sensation in the throat

Spurling's Test
- compression of cervical nerve root
(+): dermatome distribution pain and altered sensation
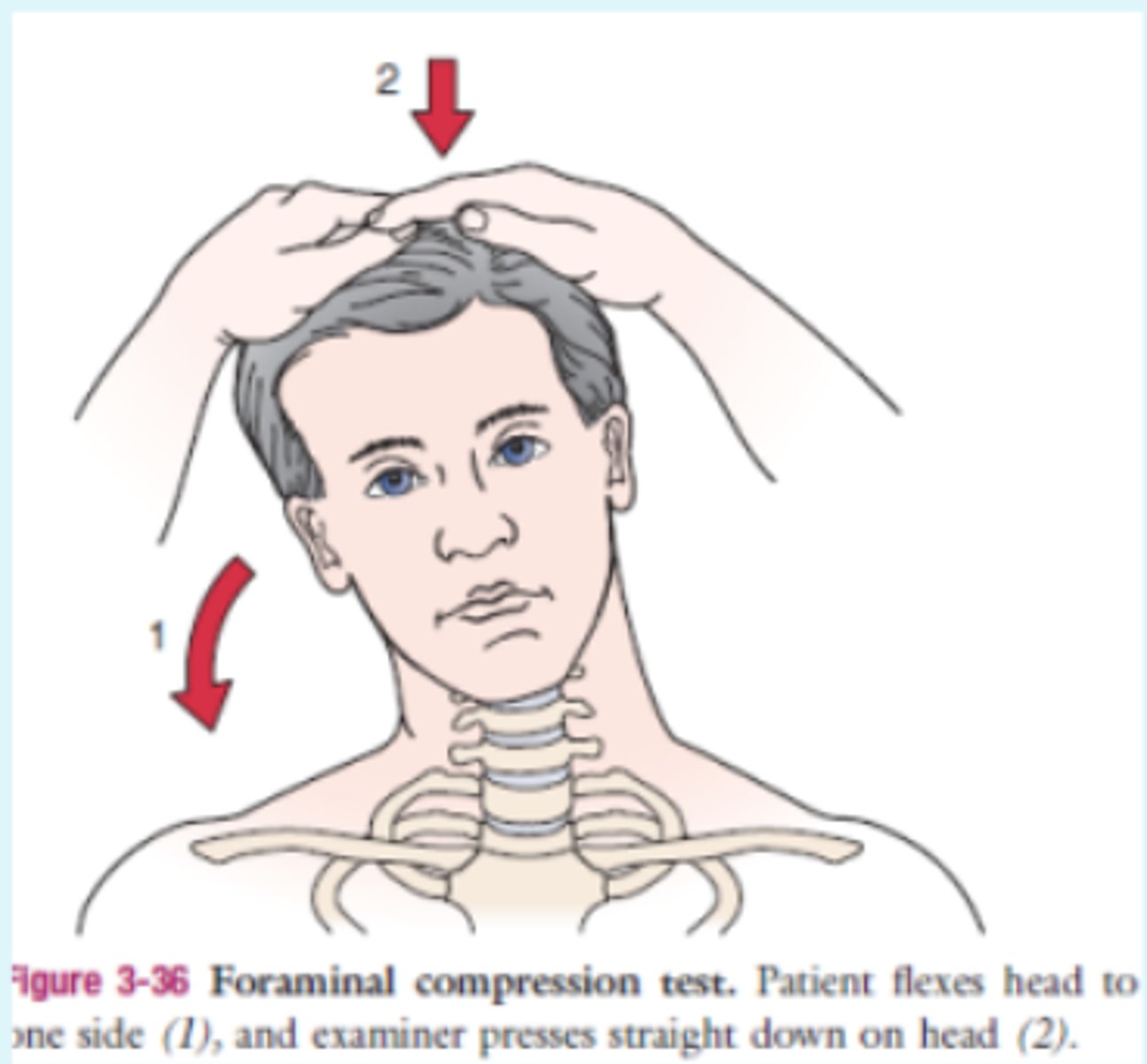
Maximum Cervical Compression Test
- compression of neural structures at intervertebral foramen or face joint dysfunction
(+): The patient side flexes the head and then rotates it to the same side. The test is repeated to the other side. A positive test is indicated if pain radiates into the arm. If the head is taken into extension (as well as side flexion and rotation) and compression is applied, the intervertebral foramina close maximally to the side of movement and symptoms are accentuated. Pain on the concave side indicates nerve root or facet joint pathology, whereas pain on the convex side indicates muscle strain

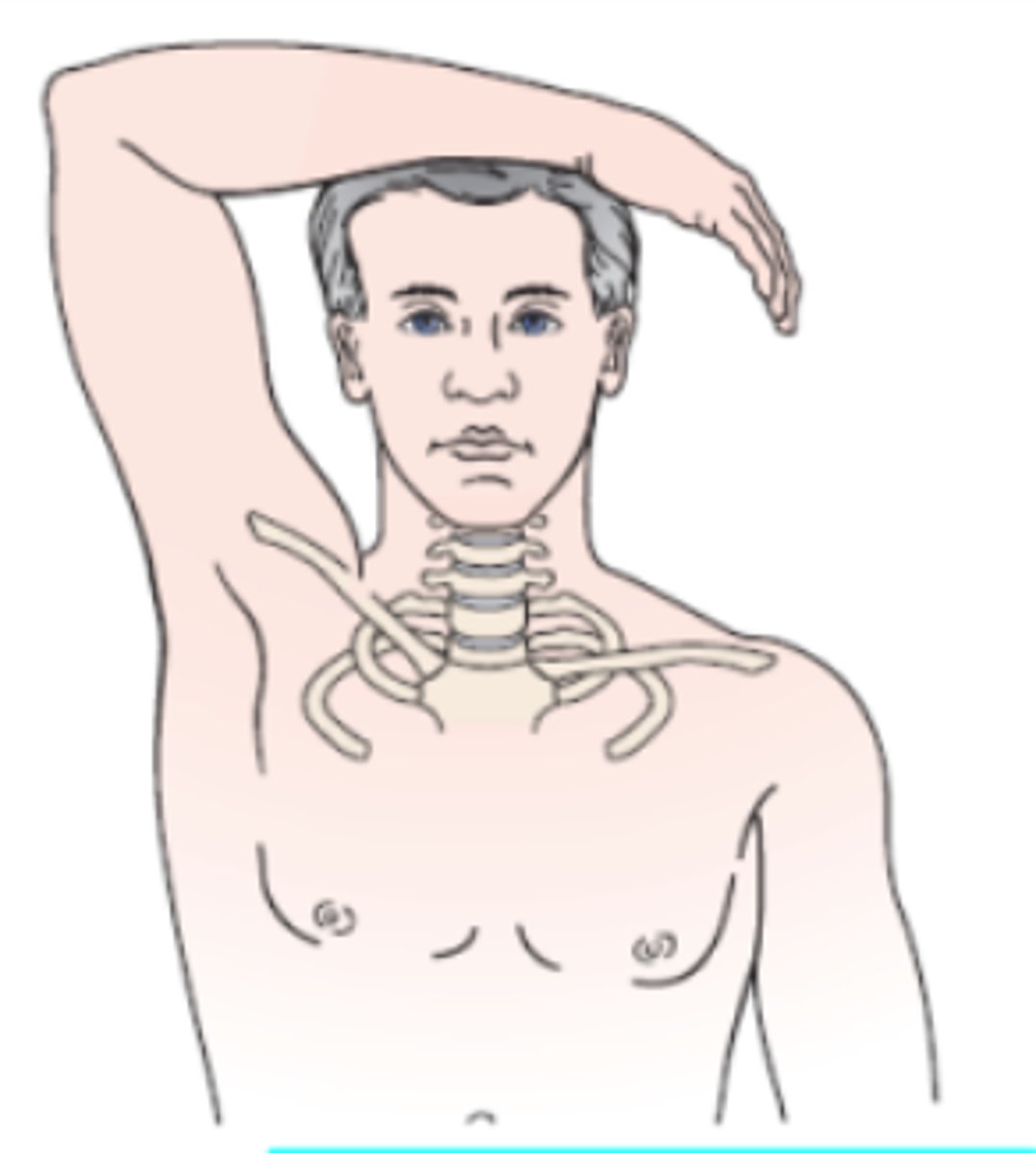
Shoulder Abduction Test (bakody's sign)
- radicular symptoms (C4/ C5)
(+): A decrease in or relief of symptoms indicates a cervical extradural compression problem, such as a herniated disc, epidural vein compression, or nerve root compression, usually in the C4-C5 or C5-C6 area.
Lhermitte Sign
- dysfunction of spinal cord and UMN
(+): A positive test occurs if there is a sharp, electric shock-like pain down the
spine and into the upper or lower limbs; it indicates dural or meningeal irritation in the spine or possible cervical myelopathy.

Lasegue’s test
AKA: SLR
(+): reproduction of n/t when foot DF or neck flexed
Femoral Nerve Traction test
- femoral nerve; sidelying slump test
procedure:
- The patient lies on the unaffected side with the unaffected limb flexed slightly at the hip and knee. The examiner grasps the patient's affected or painful limb and extends the knee while gently extending the hip approximately 15°. The patient's knee is then flexed on the affected side; this movement further stretches the femoral nerve
(+): pain anterior thigh
Babinski Test
- UMN
procedure:
- pointed object along plantar aspect of pt's foot
(+): extension of big toe and abduction of other toes

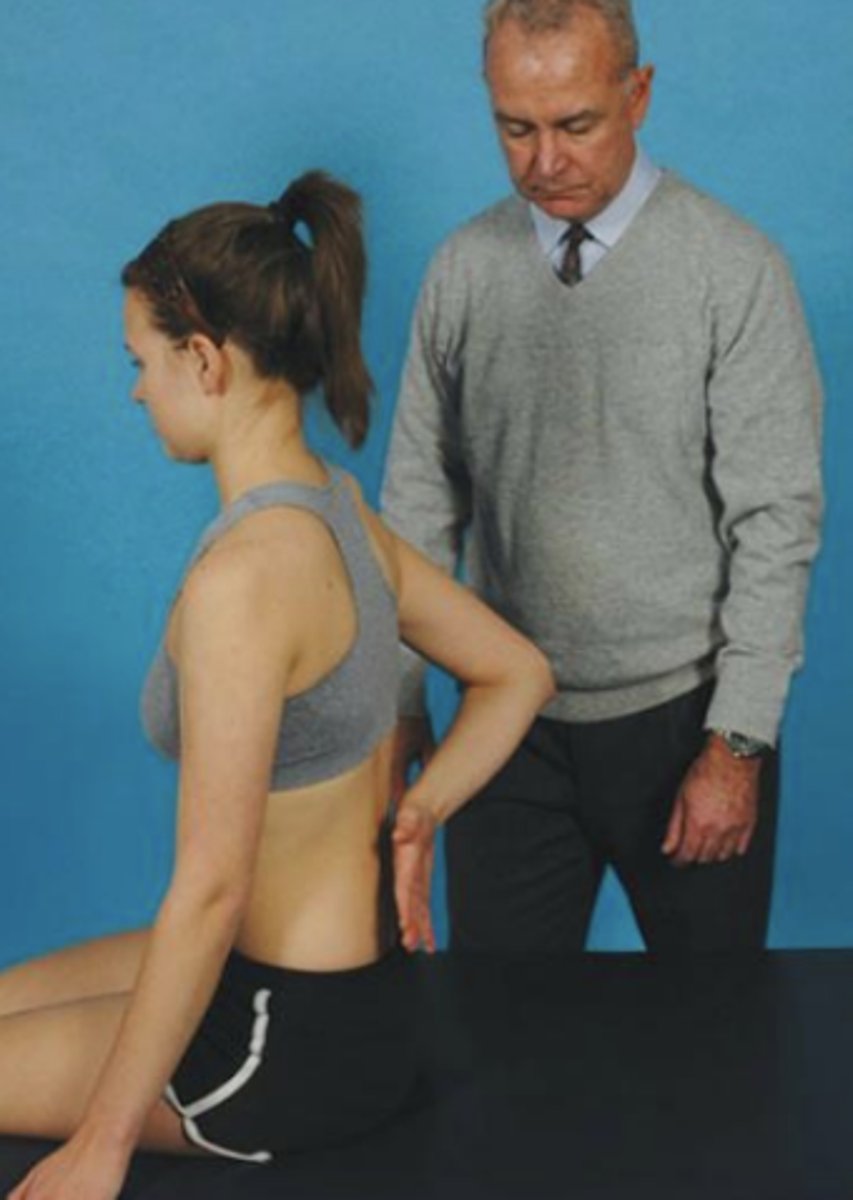
Stork Standing Test
- spondylolisthesis
procedure:
- The patient stands on one leg and extends the spine while balancing on the leg. The test is repeated with the patient standing on the opposite leg.
(+): A positive test is indicated by pain in the back and is associated with a pars interarticularis stress fracture (spondylolisthesis). If the stress fracture is unilateral, standing on the ipsilateral leg causes more pain.

Mckenzie's slide glide test
Differentiates between scoliotic curve versus neurological dysfunction
procedure:
- The patient stands with the examiner standing to one side. The examiner grasps the patient's pelvis with both hands and places a shoulder against the patient's lower thorax. Using the shoulder as a block, the examiner pulls the pelvis toward the examiner's body. The position is held for 10 to 15 seconds, and then the test is repeated on the opposite side.
(+): A positive test is indicated by increased neurological symptoms on the affected side.

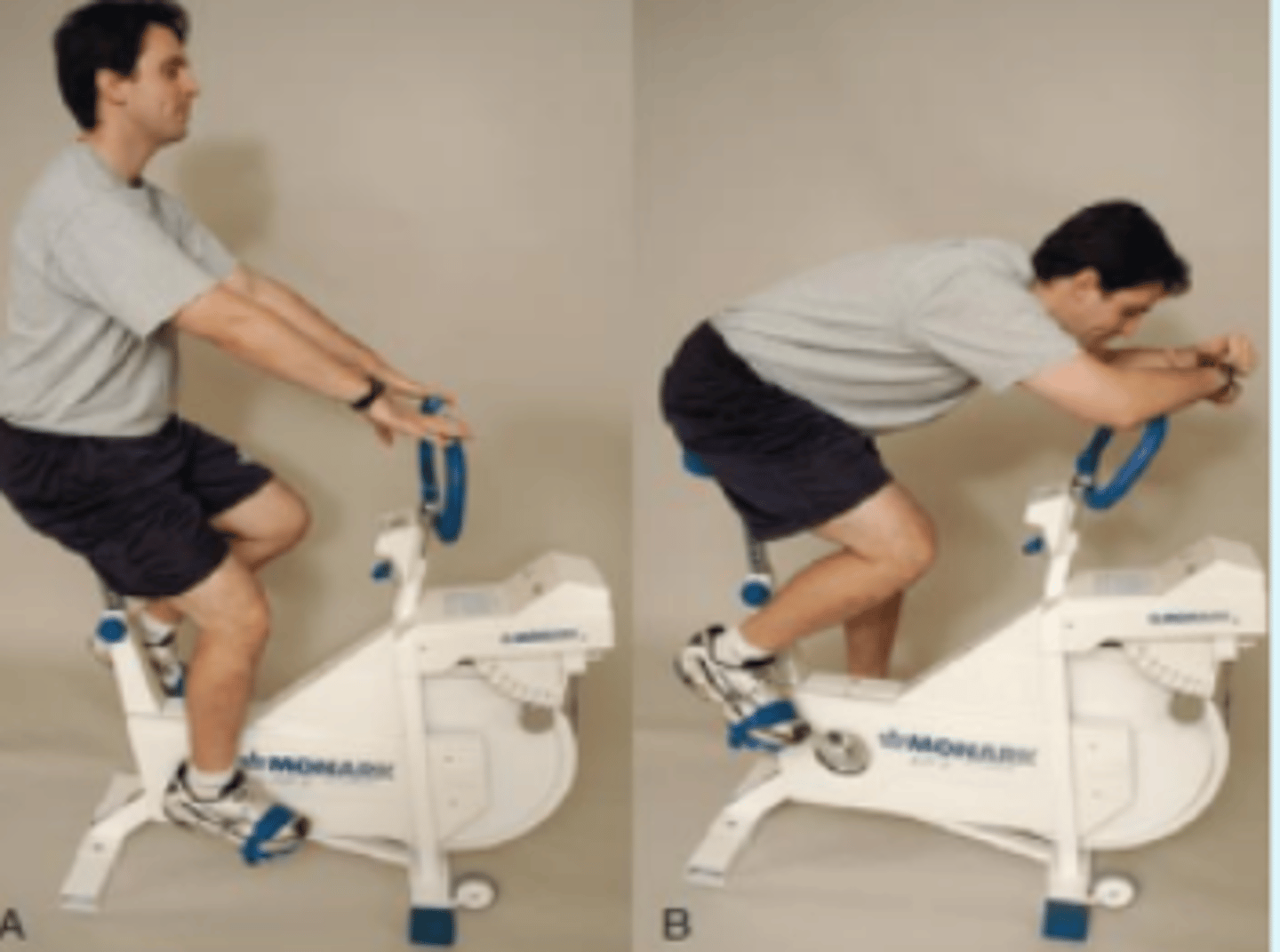
Bicycle (Van Gelderen Test)
- intermittent claudication and spinal stenosis
- The patient is seated on an exercise bicycle and is asked to pedal against resistance. The patient starts pedaling while leaning backward to accentuate
the lumbar lordosis. If pain into the buttock and posterior thigh occurs, followed by tingling in the affected lower extremity, the first part of the test is positive. The patient is then asked to lean forward while continuing to pedal. If the pain subsides over a short period of time, the second part of the test is positive; if the patient sits upright again, the pain returns. A patient with intermittent claudication of the lower extremities typically experiences an increase in symptoms with continued exercise, regardless of the position of the spine.