week3: labor and delivery
1/101
Earn XP
Description and Tags
what labor is supposed to look like
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
102 Terms
List the physiologic changes before labor
backache, loss of weight 1-3.3lb, lightening energy burst, cervical ripening
What distinguishes true labor from false labor?
cervical dilation and effacement
First stage(early) of labor facts
0-5cm, frequency is 2-30 min, duration is 30-40 seconds
First stage of labor patient observation
scant amount of brownish discharge, pale pink mucous. talkative and calm and can walk and talk through contractions. can be apprehensive
First stage of labor (active phase)
6- 10 cm, contractions are stronger, frequency is 1.5-5 min→2-3 min, duration is 40-90 seconds
dilation and effacement→ complete dilation, will feel the urge to pushf
first stage of labor in active phase patient observation
anxiety and restlessness increase as contractions become stronger, N/V, will need to have a bowel movement but this is just the baby moving
When are we in 2nd stage of labor?
in full dilation until the birth of baby
third stage of labor
placental separation and expulsion
schultze presentation
the shiny surface of the placenta comes first
Duncan presentation
the dull surface of the placenta comes first
Fourth stage is also called
recovery phase
Spontaneous rupture (SROM)
naturally rupturing of the membranes
Amniotomy (AROM)
artificial rupture of membranes
how long does labor usually begin after the rupture of membranes?
within 24 hours
what will happen to mom if membranes ruptured but its been past 24 hours before birth of baby??
infection
what is an immediate assessment for the nurse following the rupture if membranes
assess for FHR for abrupt decelerations to rule out umbilical cord prolapse
Assessment of the amniotic fluid
watery, clear, slightly yellow tinge, volume is 700-100mL, with nitrazine paper confirming as a deep blue color with a PH of 6.5-7.5
list the 5 P’s
passenger, passageway, powers, position, psychological
What consist of the P (Passager)
consist of the baby’s head, presentation, lie, attitude, and position affecting baby’s ability to navigate the birth canal, also placenta
facts about the size of the baby’s head
sutues (the skinny flexeble part) and Fontanels (the fatter part of the flexeble head) molding can occur during labor and it resumes normal shape after 3 days after birth
facts about the baby presentation
how is the baby positioned for birth, cephalic, breech, or shoulder. presenting part refers to the part of the baby closest to the internal part of cervix
facts about the lie
how the baby is positioned either transverse or parallel. if a baby is transverse mom requires a C-section. if baby is a breech then its also recommended for a C-section
facts about attitude
fetal flexion is when chin is flexed into chest and extremities is flexed into torso,
fetal extension is when chin extended away from chest and extremities are extended
facts about fetal position
tells healthcare workers how baby is positioned, first letter is the side of moms pelvis, second letter is the presenting part of baby, third letter is references the part of the moms pelvis
facts about the station
a measurement in fetal decent in cm.
station 0 is at the level of ischial spines
-stations are above the ischial spines
+stations are under the ischia spines
2nd P passage way facts
the birth canal composed of bony pevlis, cervix, pelvic floor, vagina, and introitus
Powers (primary)
Uterine contractions cause effacement and dialationp
powers (secondary)
the involuntary urge to push and voluntary bearing down that helps push baby out
the mom position facts
mom should engage in frequent position changes during labor to increase comfort, relieve fatigue and promote circulation. gravit aids in fetal descent(uptight, sitting, kneeling, and squatting).
dr. may be slightly restrictive b/c we need to monitor baby
Leopold maneuvers
externally positioning the baby
tocotransducer (toco)
measures contractions
When is group B steptococcus screened
36-38 weeks. if positive we are doing IV antibiotics
Nursing actions during Intrapartum
Assess om VS, and check Mom’s temo every 2 hours
assess FHR
assess uterine contractions characteristics; frequency, duration, intensity, resting tone of uterine contractions
Why are we checking for maternal temperature
checks for infection if her temperature is above 100.5
What goes into a vaginal examination (SVE)?
effacement, cervical dilation, descent of the fetus in station, fetal position, membranes are intact or ruptured
Post procedure Nursing assessments
maternal VS, fundus, Lochia, Perineum, Urinary output, maternal/newborn baby-friendly activates
During the 4th stage what are AAP and ACOG recomendations for vital signs for mom?
BP and Pulse- every 15 min for first two hours after birth
temp every 4 hours for the first 8 hours after birth then every 8 hours
assess fundus and lochia every 15 min for first hour
why should we massage the uterine fundus or admin oxytocic during post procedure?
to maintain uterine tone and prevent hemorrhage
First stage of labor the source of pain
internal visceral pain felt as back and leg pain
coming from dilation, effacement, and stretching of cervix, contractions
second stage of labor the source of pain
somatic pain that occurs with fetal descent and expulsion
coming from pressure and distention from the vagina and perineum(burning, splitting, and tearing), pressure and pulling of the pelvic structures, and lacerations of soft tissues like the cervix, vagina and perineum)
third stage of labor the source of pain
with expulsion of placenta, is mostly visceral pain. pressure and pulling of pelvic structures
fourth stage of labor source of pain
distention and stretching of vagina and perineum during the second stage, splitting, burning, and tearing sensations
what is the main use of nonpahrmalogical pain
to reduce anxiety, fear, and tension
gate-control theory of pain
sensory nerve pathways allowing a limited number of sensations to travel at any given time.
cognitive interventions of nonpharmacological pain management
childbirth education, Lamaze, doulas
assessing for hyperventilation, lightheadedness, and tingling of fingers
sensory stimuli strategies interventions of nonpharmacological pain management
aromatherapy, breathing techniques, imagery, music, focal points, subdued lighting
Cutaneous Stimulation strategies
back rubs and massage, walking, rocking, application of heat or cold, frequent maternal position changes
Cutaneous Stimulation strategies: Efflurage
gentle circular motions in the abdomen in rhythm with breathing during contraction
Cutaneous Stimulation strategies: Sacral counterpressure
pressure applied using the heel of the hand or fist against the sacral area to counteract pain in the lower back
Cutaneous Stimulation strategies: Hydrotherapy
pool or shower that can increase maternal endorphin levels
pharmacological pain management: Analgesia Sedatives (barbiturates)
using during the early or latent phase
pharmacological pain management: Opioid Analgesics
given during early part of active labor
pharmacological pain management: regional blocks, Pudendal
transvaginal injection of local anesthetic in perineal area
pharmacological pain management: regional blocks, Epidural
administered during labor
pharmacological pain management: regional blocks, Spinal
used for cesarean
What does admin of nitrous oxide most benefit maternal for?
reduces the perception of pain
Epidural Catheter placement
local anesthetic, bupivacaine, or analgesic injected into epidural space at lv 4th and 5th of vertebrae.
it will remove pain but not pressure sensations. the medication can be continuous or intermittent or patient-controlled (PCEA)
Epidural Adverse effects
Maternal hypotension, fetal bradycardia, fever, itching, inability to feel the urge to void, urinary retention, loss of bearing down reflex, prolonged labor
Epidural nursing actions
admin IV bolus →aids with hypotension
make position and have steady for correct placement
tilt or remain side-lying to avoid supine hypotension
monitor maternal BP, HR, RR, O2
assess FHR continuously
maintain IV and have O2 and suction available → for their N/V
assessing for ortho hypotension → preparing to admin IV vasopressor(ephedrine) positioning laterally, IV fluids, initiate O2
side rails, (SCD), insert a foley catheter, and coach in pushing
Spinal Anesthesia: Adverse effects
Maternal hypotension, fetal bradycardia, loss of bearing down reflex, potential headache from leakage of cerebrospinal fluid at puncture site, there is a higher incidence of uterine atony following birth → bc pain is blocked
Spinal Anesthesia: nursing actions
Assess maternal VS every 10 min
maternal hypotension → manage by IV fluid bolus as prescribed, positioning patient laterally, increasing the rate of fluid IV, initiate O2
assess uterine contractions, lv of anesthesia, FHR patterns, raise side rails
General anesthesia: nursing actions
use as a last option
M mom VS/ M FHR patterns, mom should have nothing by mouth, ensure IV infusion in place. Apply SCD, premedicate mom with oral antacid to nutralize somatch acid contents. admin histamine 2 recepor antagonist (famotidine) to decrease gastric acid production
admin metoclopramide to increase gastric emptying, place wedge on hips to displace uterus. maintain an airway
Leopold Maneuvers
external palpations of maternal uterus through abdominal wall to determine fetal lie , attitude, and resenting part, degree of descent
guidelines for listening to fhr during latent phase (<4cm)
hourlygu
guidelines for listening to FHR during latent phase(4-5cm)
every 15-30 min
guidelines for listening to FHR during active phase
every 15-30 min for active
guidelines for listening to FHR during the second stage
every 5-15 min
indications for an EFM
determines active labor
rupture of membranes
preceding and subsequent to ambulation
prior or following admin of change in med analgesia
at speak action of anesthesia following vaginal examination
following expulsion of an enema
after urinary catheterization
abnormal or excessive uterine contractions
what is a normal fetal heart rate?
110-160bpm
diagnostic measures to determine tacky or bradycardia
FHR being above or below expected range for 10 min or longer
Non-reassuring FHR are associated with___ and include the following
hypoxia,
fetal brady, tacky, absence of FHR variability, late decelerations, variable decelerations
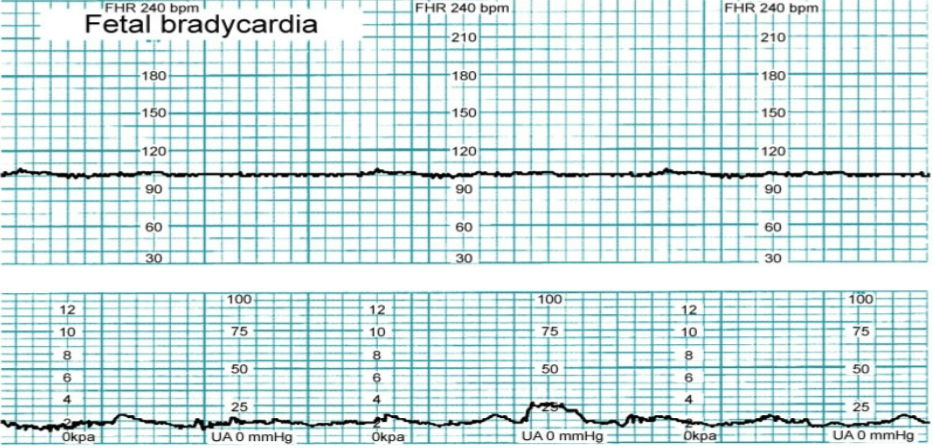
complications or causes for feal bradycardia
Uteroplacental insufficiency, umbilical cord prolapse, maternal hypotension, prolonged umbilical cord compression, fetal congenital heart block, anesthetic medications, viral infection, maternal hypoglycemia, fetal heart failure, maternal hypothermia
Nursing interventions for FHR bradycardia
discontinue oxytocin, assist mom to side-lying position, admin O2 at 10 L/min via non-rebreather face mask, insert an IV catheter and admin fluids, admin a tocolytic med. Notify provider → if your interventions did not stabilize mom and baby
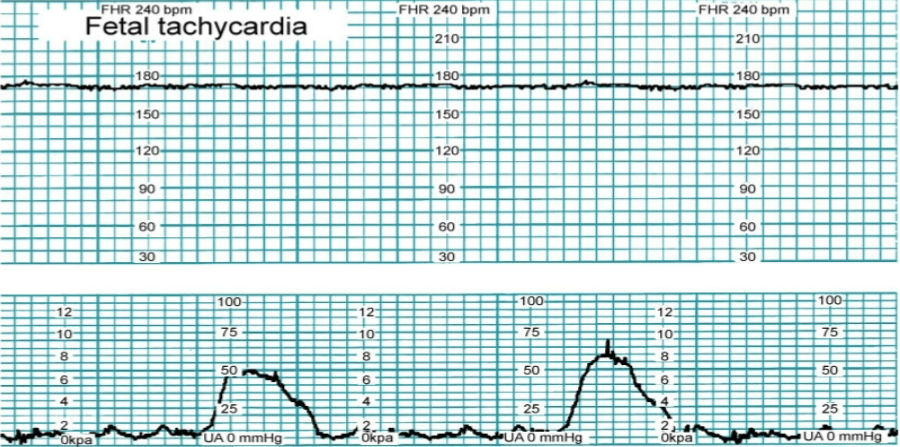
complications or causes of FHR tachycardia
Maternal infection, intrauterine infection, fetal anemia, fetal dysrhythmias, maternal use of cocaine, caffeine, or methamphetamines, maternal dehydration, maternal or fetal infection, maternal fever(>100.5), maternal hyperthyroidism
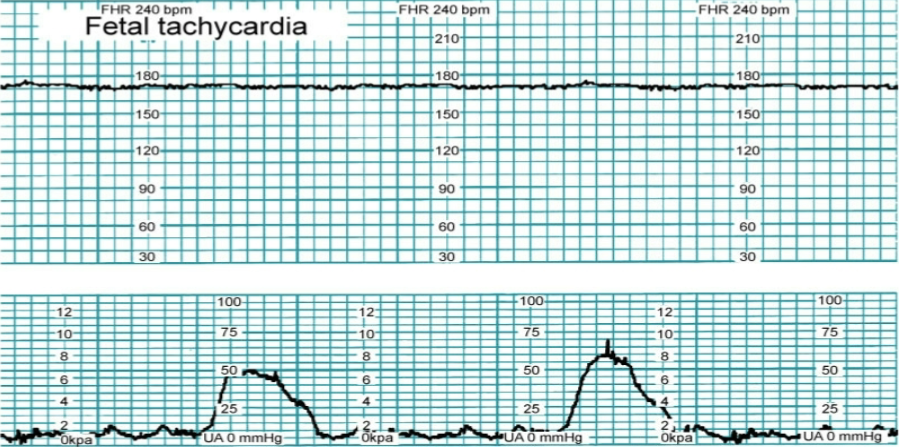
nursing interventions for FHR tachycardia
admin prescribed antipyretics for maternal fever if present, admin o2 by mask at 10L/min non-rebreather face mask. admin IV fluid bolus
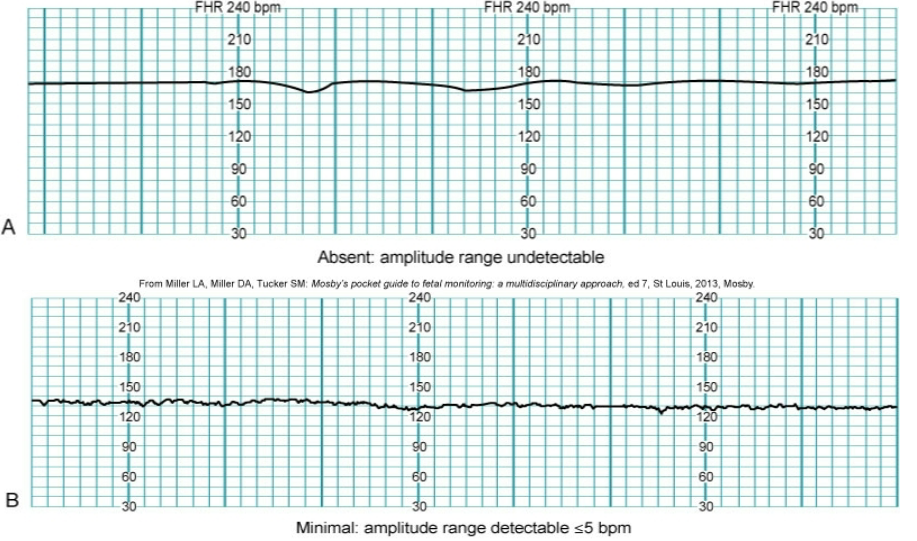
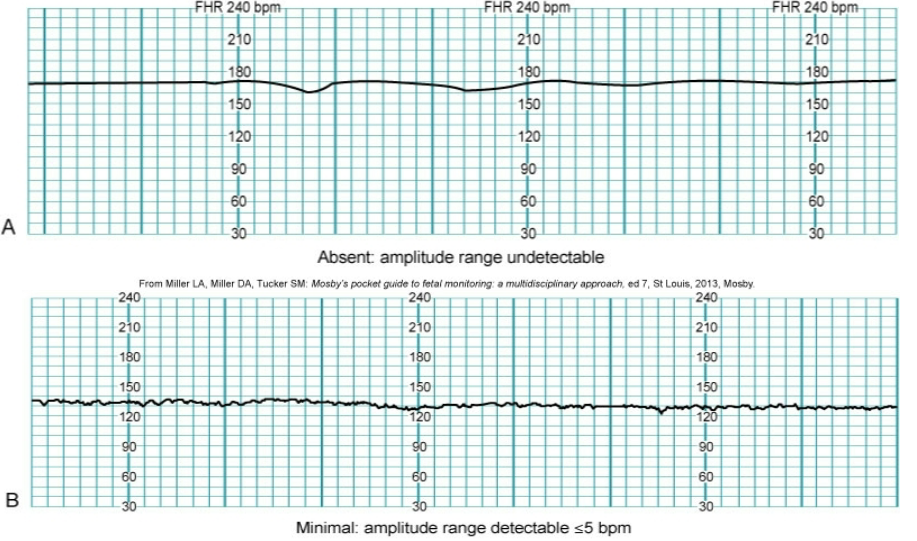
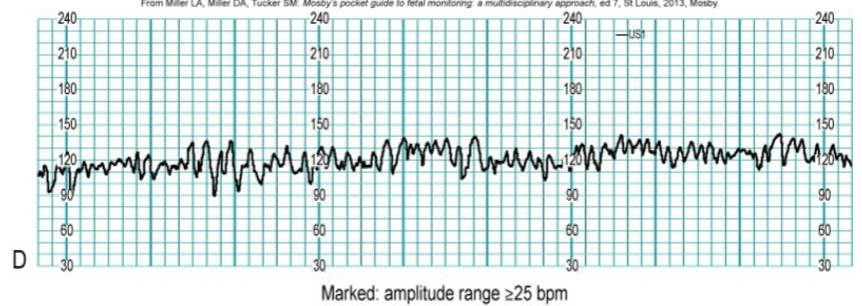
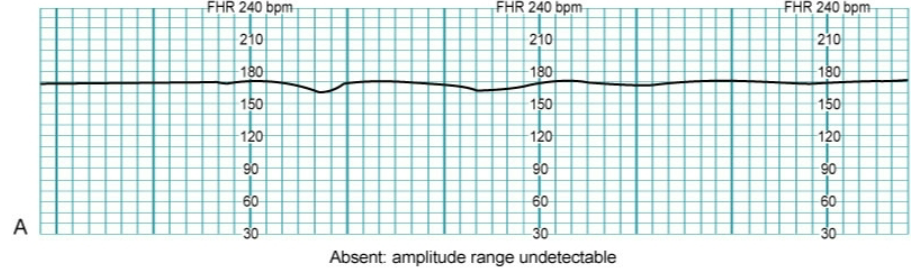
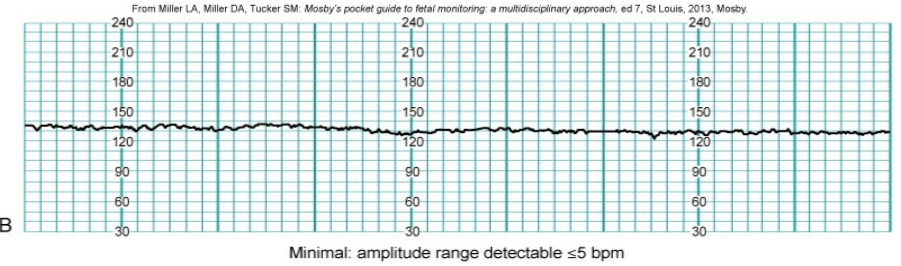
FHR variability
fluctuations in FHR baseline
causes that decrease or loss of FHR variability
med that depress the CNS (barbiturates, mag sulf, gen anesthesia, fetal hypoxemia and metabolic acidemia, fetal sleep cycle(this loss does not last longer than 30 min), congenital abnormalities
nursing interventions for FHR that has loss of variability
stimulate fetal scalp. Assist provider with application of scalp electrode. place client in left- lateral position
moderate variability
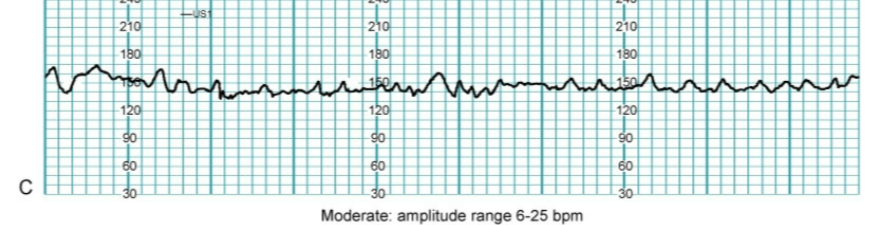
marked variability
absent or non-reasuring variability
minimal variability
accelerations in FHR
FHR patterns: Accelerations
healthy fetal/ placental exchange
indicates a reactive nonstress test.
variable deceleraction of FHR
slowing of FHR of 15 bpm or more below baseline for at least 15 seconds
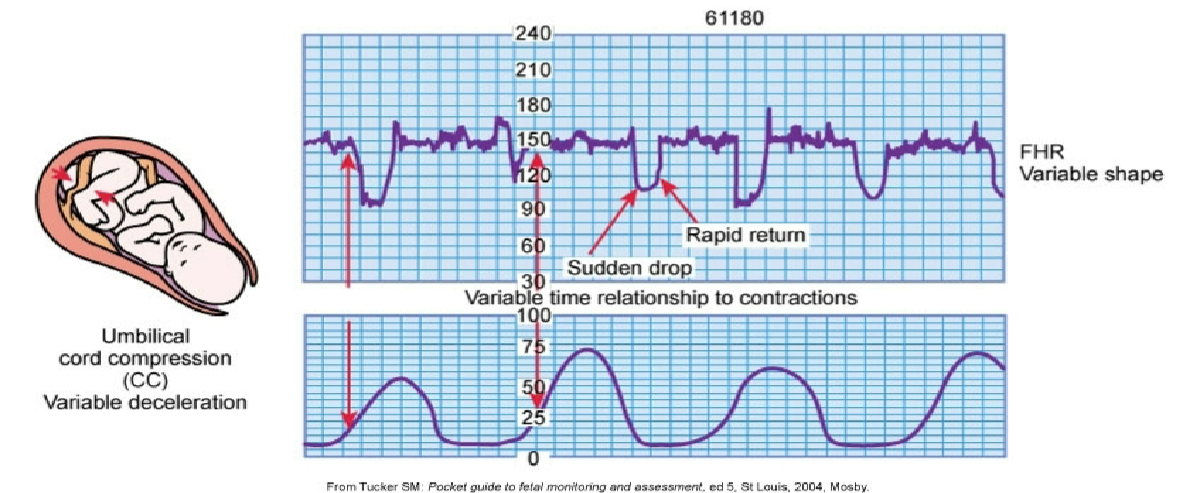
causes or the complications that cause deceleration of FHR
umbilical cord prolapse, short cord, prolapse cord, knot in cord, nuchal cord(around the fetal neck)
nursing interventions if variable decelerations are found in FHR
reposition the client from side to side or knee-chest
discontinue o2
admin oxygen by mask at 10-15L/min via non-rebreather face mask
perform or assist with a vaginal examination
Assist with an amnioinfusion if prescribed
early deceleration of FHR
slowing of FHR at the start of a contraction and returns to baseline at the end of contraction
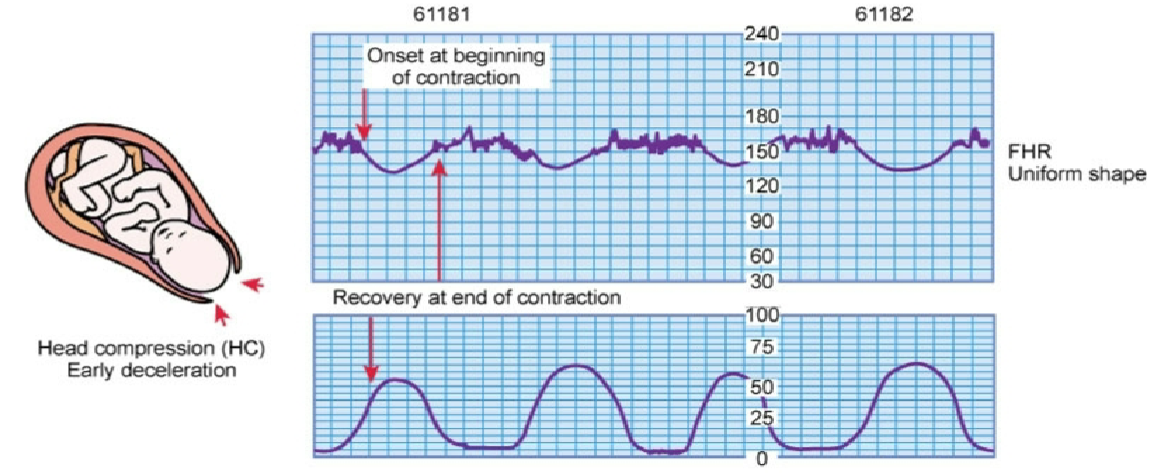
cause or complications that cause early deceleration of FHR
compression of the fetal head resulting from: Uterine contractions, vaginal exam, fundal pressure, placement of internal monitoring
no intervention required, normal labor
Late deceleration of FHR
slowing of the FHR that returns well after contraction has ended
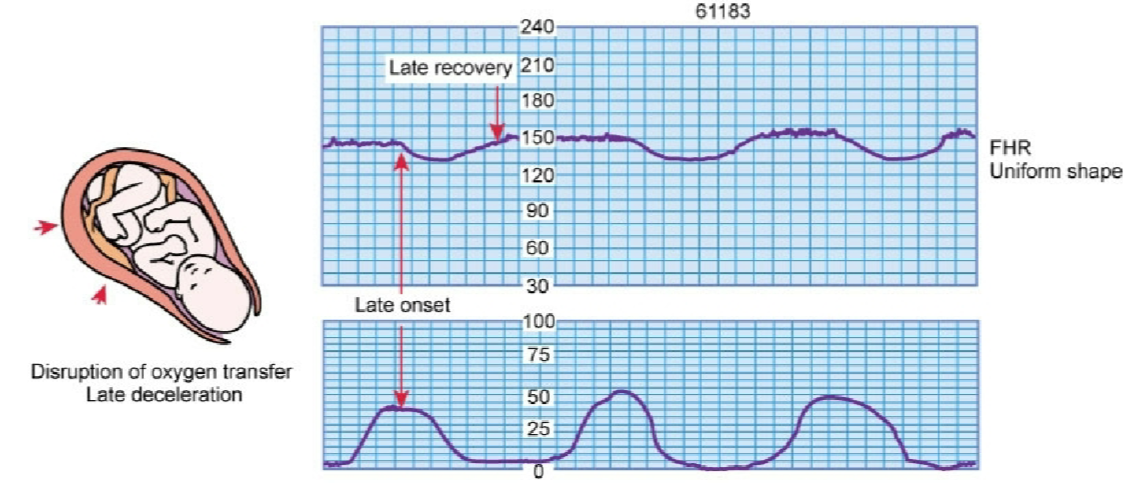
cause or complication that cause late deceleration of FHR
Uteroplacental insufficiency,
maternal hypotension, placenta previa, abruptio placentae, uterine tachysystole with oxytocin,
preeclampsia
late or post term pregnancy
maternal diabetes mellitus
Nursing interventions for late decelerations of FHR
Place the client in a side-lying position
Insert an IV catheter if not in place and increase rate of IV fluid admin
discontinue oxytocin if being infused
admin oxygen mask at 10-15L/min via nonrebreather face mask
elevate the clients legs
notify provider
prepare for assisted vaginal birth or C-section
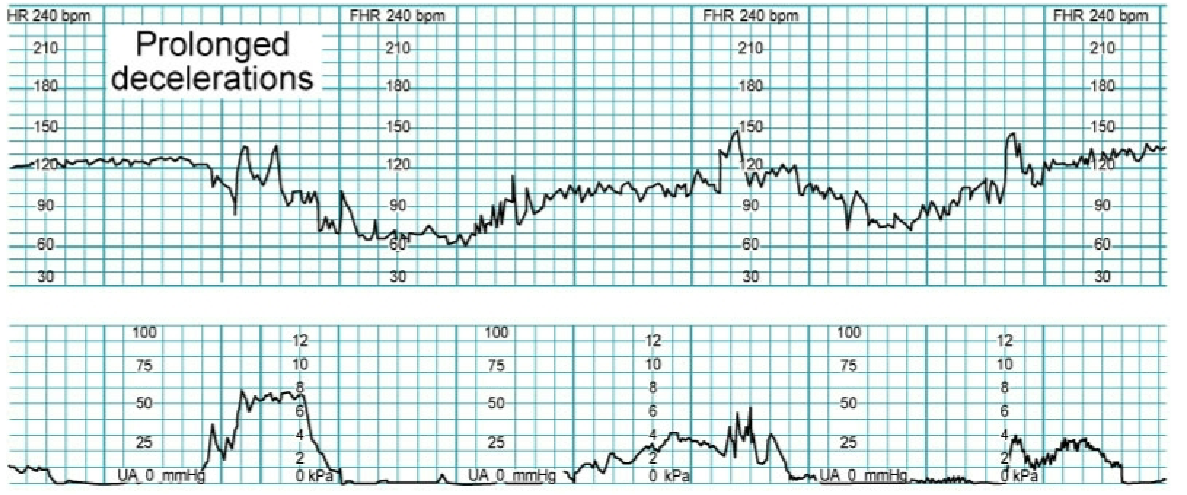
prolonged deceleration
advantage of a continuous internal fetal monitoring
early detection of abnormal FHR patterns
accurate assessment of FHR variability
accurate measurement of uterine contraction intensity
Allows greater maternal freedom of movement because tracing s not affected by fetal activity, or maternal positions
disadvantages of continuous internal fetal monitoring
membranes need to have ruptured to use internal monitoring
cervix must be dilated to a min of 2 to 3 cm
presenting part must have descended to place electrode
potential risk of injury to fetus if it is not placed properly
a provider, nurse practitioner/midwife, or specially trained RN must preform this procedure
risk of infection to client and fetus
Category l
‘A perfect baby”
baseline in FHR is 110-160/min
baseline FHR variability is moderate
Accelerations: present or absent
early decelerations": present or absent
variable or late decelerations: absent
Category ll
baseline rate: tacky or brady cardia
variability: minimal, absent, or marked variability
decelerations: prolonged FHR deceleration ≥2min but <10min/ late deceleration with moderate variability/ variable deceleration with minimal or moderal baseline variability
accelerations: absent
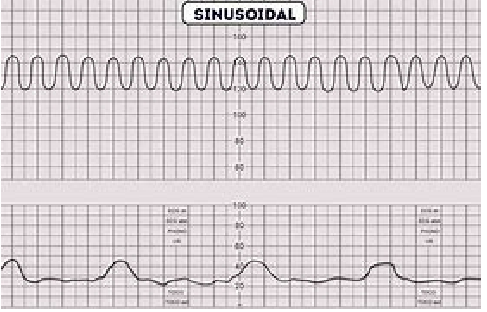
Category lll
“Abnormal must deliver”
sinusoidal pattern
absent baseline FHR with recurrent variable or late decelerations, bradycardia
Tachysystole
uterine contractions more than 5 min of contractions in 10 min averaged over a 30 min window
FHR pattern VEAL mnemonic
V (variable deceleration)
E (early deceleration)
A (acceleration)
L (late deceleration)