Coronary Vascular Disorders
1/19
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
20 Terms
What is coronary atherosclerosis?
Atherosclerosis is the abnormal accumulation of lipid deposits and fibrous tissue within arterial walls and lumen
In coronary atherosclerosis, blockages and narrowing of the coronary vessels reduce blood flow to the myocardium
Cardiovascular disease is the leading cause of death in the United States for men and women of all racial and ethnic groups
Coronary artery disease (CAD) is the most prevalent cardiovascular disease in adults
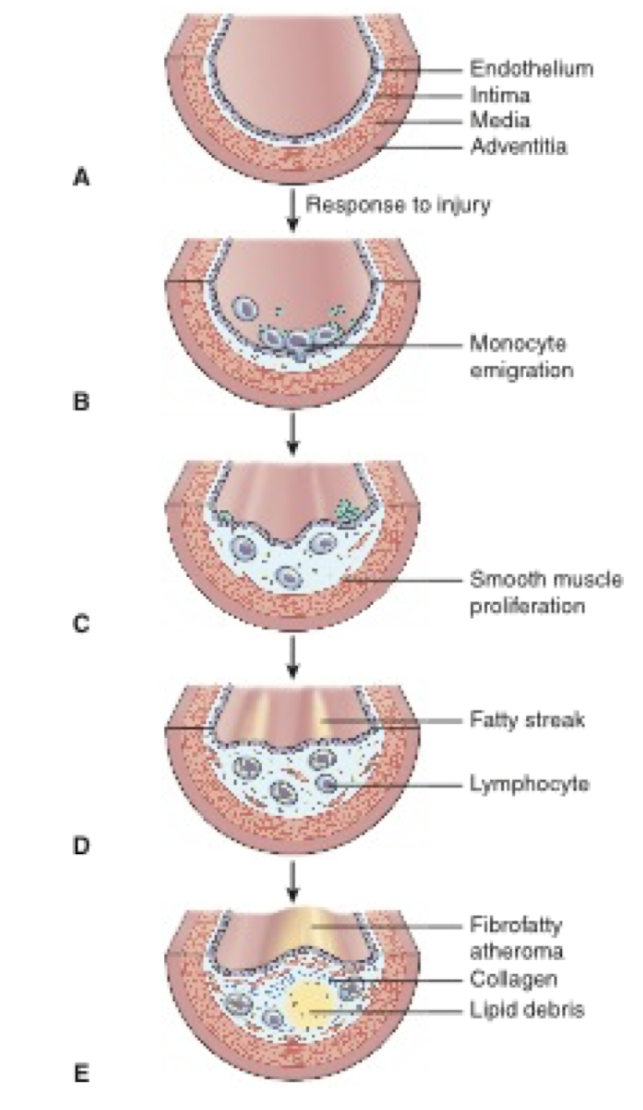
What is the pathophysiology of artherosclerosis?
Atherosclerosis begins as monocytes and lipids enter the intima of an injured vessel.
Smooth muscle cells proliferate within the vessel wall
Contributing to the development of fatty accumulations and atheroma
As the plaque enlarges, the vessel narrows and blood flow decreases
The plaque may rupture and a thrombus might form, obstructing blood flow.
What are the clinical manifestations of artherosclerosis?
Symptoms are caused by myocardial ischemia
Symptoms and complications are related to the location and degree of vessel obstruction
Angina pectoris (most common manifestation)
Other symptoms: epigastric distress, pain that radiates to jaw or left arm, SOB, atypical symptoms in women
Myocardial infarction
Heart failure
Sudden cardiac death
Older people pain sensation is decreased → weakness, fatigue
Women also present differently
What are the four non modifiable and modifiable risk factors of CAD?
Most prevalent type of cardiovascular disease in adults
Four modifiable risk factors cited as major cholesterol abnormalities, tobacco use, HTN, and diabetes
Elevated LDL: primary target for cholesterol-lowering medication
Metabolic syndrome
hs-CRP (high- sensitivity C-reactive protien) → inflamatory marker
How is CAD prevented?
Control cholesterol
Dietary measures
Physical activity
Medications
Cessation of tobacco use
Manage HTN
Control diabetes
What are the cholesterol medications?
Six types of lipid-lowering agents: affect the lipid components somewhat differently
3-Hydroxy-3-methylglutaryl coenzyme A (HMG- CoA) (or statins)
Nicotinic acids
Fibric acids (or fibrates)
Bile acid sequestrants (or resins)
Cholesterol absorption inhibitors
Omega-3 acid-ethyl esters
What are the thereaputic effects and considerations with Statins, Fibrates, Bile acid sequestrants, cholesterol absorption inhibitor, proprotien convertase subtilisin- Kexin Type 9 (PCSK9) Agents?
Statins: lower LDL ("bad") cholesterol in the blood by slowing down its production in the liver
moniter LFTs → give them in evening (more cholesterol to remove)
Drug interactions
Myalgia & arthalgia are sommon adverse effects (Muscle & joint pain)
Myopathy & possible rhabomyolysis are potentially serious s/e (muscle disease- weakness & fatigue, muscle breakdown/destruction)
Fibrates: decreasing your triglycerides and increasing your HDL cholesterol (also decrease lipids)
diarrhea, flatulance, rash, myalgia
Serious adverse effects pancreatitis, hepatotoxicity, and rhabomyolysis
Contraindicated severe kidney & liver disease
Caution with stains bc increase risk of rabdo & heptotaxicity
Bile Acid sequestrants: causes choleterol to be in bile acid and reduce fat absorption, instead is excreted
Adjunct thereapy to statins
S/e constipation, abdominal pain, GI bleeding
can decrease absorption of other drugs, take before meals
Cholesterol absorption inhibitor: inhibit absorption of cholesterol in small intestine
Better absorbed the bile acid sequestrants
used in combincation with statins
S/e abdominal pain, myalgia & arthalgia
Contraindicated in liver disease
PCSK9 Agents: Block PCSK9 protein, allowing more receptors to remove LDL from the blood
Only SQ
S/E: rhinitis, sore throat, flu like symptoms, muscke pain, diarrhea, redness, pain, or bruising at injection site
What is angina pectoris?
A syndrome characterized by episodes or paroxysmal pain or pressure in the anterior chest caused by insufficient coronary blood flow
Physical exertion or emotional stress increases myocardial oxygen demand, and the coronary vessels are unable to supply sufficient blood flow to meet the oxygen demand
What are the types of angina?
Stable angina: predictable and consistent pain that occurs on exertion and is relieved by rest and/or nitroglycerin
Unstable angina (also called preinfarction angina or crescendo angina): symptoms increase in frequency and severity; may not be relieved with rest or nitroglycerin
Intractable or refractory angina: severe incapacitating chest pain
Varient angina (also called Prinzmetal’s angina): pain at rest with reversible ST- segment elevation; thought to be caused by coronary artery vasospasm
Silent ischemia: objective evidence of ischemia (such as electrocardiographic changes with a stress test), but patient reports no pain
Think of MI to rule it out
What are the assessment and findings for angina?
May be described as tightness, choking, or a heavy sensation
Frequently retrosternal and may radiate to neck, jaw, shoulders, back or arms (usually left)
Anxiety frequently accompanies the pain
Other symptoms may occur: dyspnea or shortness of breath, dizziness, nausea, and vomiting
The pain of typical angina subsides with rest or NTG
Unstable angina is characterized by increased frequency and severity and is not relieved by rest and NTG. Requires medical intervention!
What are the genterologic considerations for angina?
Diminished pain transition that occurs with aging may affect presentation of symptoms
“Silent” CAD
Teach older adults to recognize their “chest pain– like” symptoms (i.e., weakness)
Pharmacologic stress testing or cardiac catheterization used to diagnose CAD
Medications should be used cautiously d/t increased risk of adverse reactions!
What are the nursing interventions for patient with angina pectoris?
Treat angina
Reduce anxiety
Prevent pain
Educate patients about self-care
Continuing care
Patient w Angina Pectoris Goals
Immediate and appropriate treatment of angina
Prevention of angina
Reduction of anxiety
Awareness of the disease process
Understanding of prescribed care and adherence to the self-care program
Absence of complications
How is angina pectoris treated?
Treatment seeks to decrease myocardial oxygen demand and increase oxygen supply
Medications (Table 23-2 next slide)
Oxygen
Reduce and control risk factors
Reperfusion therapy may also be done
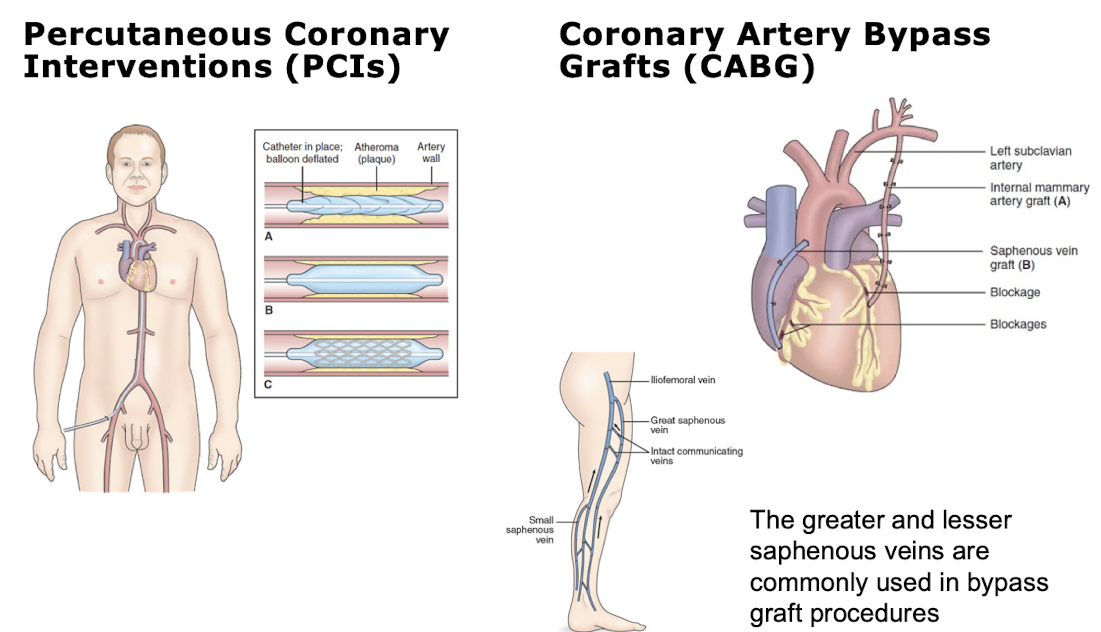
PCI procedures (e.g., percutaneous transluminal coronary angioplasty [PTCA] and intracoronary stents) and CABG
Stable angina meds- What is Nitroglycerin, Beta- andergenic blocking agent, calcium channel blocking agents, Antiplatlet & asprin, heprin, abciximab or eptifibatide side effects/ contraindications, use?
Nitroglycerin: Short & long- term reducation of myocardial oxygen consumtion through selective vasodilation
S/E: dizziness & h/a
Beta-adrenergic blocking agents: Block adrenaline, Reducation of myocardial O2 consumption by blocking beta- adrenergic stimulation of the heart
Contraindication: severe bradycardia ( bpm), cardiogenic shock, low blood pressure, 2nd/3rd-degree heart block (bc slow down conduction which can make matters worse), and severe, unstable heart failure. They should generally be avoided in patients with active asthma or severe COPD due to potential bronchospasm
Calcium channel blocking agents: negative inotropic effect; indicated in pts not responsive to BB, used as treatment for vasospasm
Common drugs used amiodipine & diltazem
Can cause brady, constipation
Antiplatelet and anticoagulant medications: Prevention of thrombus forrmation
Aspirin
Common side effects: mild stomach irritation, heartburn, nausea, and an increased risk of bruising or bleeding
Clopidogrel and ticlopidine- P2Y12 inhibitors
Heparin
SQ vs IV
S&S of bleeding: eccymosis, hematoma, bright red/ tarry stool, hematemesis
Glycoprotein IIb/IIIa agents (abciximab or eptifibatide)
high-risk Acute Coronary Syndrome (ACS) patients undergoing PCI, those with heavy thrombus burden, or as an alternative to P2Y12 inhibitors in patients allergic to them
Heprin check PTT (60-80)
Warfrain PT/INR (2-3)
What is Acute Coronary Syndrome (ACS) and Myocardial Infarction (MI)?
Emergent situation
Characterized by an acute onset of myocardial ischemia that results in myocardial death (i.e., MI) if definitive interventions do not occur promptly
Although the terms coronary occlusion, heart attack, and MI are used synonymously, the preferred term is MI
Unstable angina
NSTEMI
STEMI
How is ischemia, injury, and infarction on ECG?
EKG should be obtained within 10 minutes from the time a patient reports pain or arrives in the ED.
By monitoring serial ECG changes over time, the location, evolution, and resolution of an MI can be identified and monitored.
How is ACS assessed in patient?
Chest pain
Occurs suddenly and continues despite rest and medication
Other S&S: SOB; C/O indigestion; nausea; anxiety; cool, pale skin; increased HR, RR
ECG changes
Elevation in the ST segment in two contiguous leads is a key diagnostic indicator for MI
Lab studies: cardiac enzymes and biomarkers, which include troponin, creatine kinase, myoglobin
What is the nursing intervention for patient for ACS?
Relieve pain and S&S of ischemia
Improve respiratory function
Promote adequate tissue perfusion
Reduce anxiety
Monitor and manage potential complications
Educate patient and family
Provide continuing care
Goals for Pt w ACS:
Relief of pain or ischemic signs (e.g., ST-segment changes) and symptoms
Prevention of myocardial damage
Maintenance of effective respiratory function, adequate tissue perfusion
Reduction of anxiety
Adherence to the self-care program
Early recognition of complications
What is invasive coronary artery procedure?
Percutaneous transluminal coronary angioplasty (PTCA): a balloon-tipped catheter is used to open blocked coronary vessels and resolve ischemia → done in cath lab
Coronary artery stent
Stent: a metal mesh that provides structural support to a vessel at risk of closing
Coronary artery bypass graft (CABG): a surgical procedure in which a blood vessel is grafted to an occluded (at least 50-70%) coronary artery so that blood can flow beyond the occlusion
Cardiac surgery
Cardiopulmonary bypass (extracorporeal circulation)
What is the Nursing Management for Patient Requiring Invasive Cardiac Intervention Invasive Cardiac Intervention?
Assessment of patient
Reduce fear and anxiety
Monitor and manage potential complications
Provide patient education
Maintain cardiac output
Promote adequate gas exchange
Maintain fluid and electrolyte balance
Minimize sensory–perception imbalance
Relieve pain
Maintain adequate tissue perfusion
Maintain body temperature
Promote health and community-based care
PTCA: henmatoma, pedal pulses, vitals, signs of infection, signs of bleeding
If they come out with chest pain it prob means that there is another area that is lacking blood flow