Therapeutic Agents for Common Mucosal Diseases
1/38
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
39 Terms
What are the two most common types of oral non-microbial mucositis?
Aphthous Stomatitis
Lichen Planus

What is Lichen Planus?
White lacy patches or sores in the mouth
Three types
Reticular → lacy white lines
Erosive → ulcers/erosions with reticular pattern
Plaque → solid white patches
Commonly found on buccal mucosa

What is aphthous stomatitis?
Canker sores
Classic findings are pain greater than expected for lesion size
Occurs on non-keratinized mucosa → buccal vestibule, ventral tongue, floor of mouth
What are baseline activities that are essential for therapeutic success in the mucosa?
Avoid common intra-oral irritants
Maintain salivary pellicle
Maintain saliva production
Manage microbes
What drugs commonly cause non-microbial mucositis?
ACE-I
Beta blockers
Diuretics
Allopurinol → for gout
AEDs → carbamazepine
Statin drugs → for hyperlipidemia
Oral hypoglycemic drugs → ex; glimepiride
Precipitating factors for non-microbial mucositis?
Genetics, Systemic diseases, Microelement deficiencies, Stress, Estrogen shifts, Medications, Minor oral trauma, Toothbrushing, Dental treatment, Orthodontic bands, Popcorn, Sharp/hard devices or Foods
What topical chemicals can contribute to non-microbial mucositis?
Pyrophosphates / Polyphosphates
Flavoring agents
Cocamidopropylamine → CAPB
Sodium lauryl sulfate → SLS
How do aphthous stomatitis and lichen planus differ?
Aphthous stomatitis → painful recurrent ulcers/canker sores
Lichen planus → chronic inflammatory condition with white lacy lesions (reticular), plaques, or erosive ulcerations; commonly on buccal mucosa
What is the treatment of non-microbial mucositis?
Topical corticosteroids
Triamcinolone rise → cornerstone therapy but must be compounded
Dexamethasone solution → commercially available
Neither are “cures” → palliative care
Dexamethasone 0.5mg/5ml oral solution?
Available in 500ml bottle
Half the potency of triamcinolone
Covered by insurance → reasonable initial choice
Dexamethasone 0.5mg/5ml oral solution counseling points?
Must be held in mouth for 1-2 minutes
DO NOT Swallow → can cause adrenal suppression → 3 weeks
Triamcinolone acetonide rinse?
Compounded suspension → $$$
Disped as 240ml
Never should be flavored
Triamcinolone acetonide rinse counseling points?
Rinse 5 mL for 1 minute up to 4 times daily PRN
Spit out after rinsing (do not swallow)
Avoid food or drink for 30 minutes after use
Triamcinolone + antifungal suspensions?
Combination of triamcinolone with an antifungal to help prevent/treat Candida overgrowth during steroid therapy
Nystatin suspension → less consistent Candida coverage; contains high sucrose
Amphotericin B suspension → better activity against Candida krusei and Candida glabrata
How are topical corticosteroid ointments used for oral lesions?
High potency → Clobetasol 0.05%, Fluocinonide 0.05%
Apply thin film to dentures/medication trays
Hold ~30 minutes, then rinse mouth
When are corticosteroid ointments used in mucositis?
For localized, non-microbial inflammatory mucositis
When lesions are persistent, painful, or not responding to basic care
Used to reduce inflammation directly at specific lesion sites
What are the most common types of oral microbial mucositis?
Candidosis
Herpes simplex virus → HSV
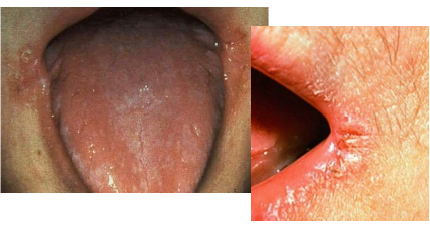
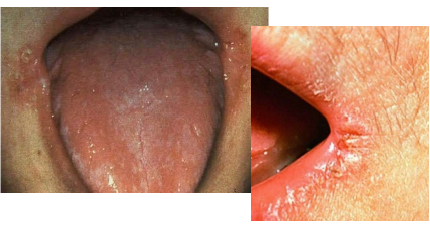
Angular cheilitis?
Infected painful, red, cracked sores at one or both corners of the mouth
Usually Candida, sometimes mixed with Staph bacteria
Common in denture wearers
Linked to dry mouth and loss of vertical face height (mouth “collapses”)
How is angular cheilitis treated?
Ketoconazole 2% cream
Apply → 2–3 times daily to corners of mouth
Can be used with dentures as a delivery method
Sometimes compounded with high-potency steroids
Off-label use → not officially approved for intraoral use
How are clotrimazole and miconazole used for angular cheilitis?
Clotrimazole 1% or Miconazole 2% cream
Apply to affected area (OTC or Rx)
Treats Candida-related infection
Also used for other superficial fungal skin infections
Why is nystatin + triamcinolone cream not recommended for angular cheilitis?
Poor antifungal effectiveness for Candida
Steroid can worsen infection by suppressing immune response
Not recommended for routine use
When is fluconazole used for angular cheilitis?
Used for more severe or resistant Candida infections
Oral systemic therapy
Significant drug interactions → CYP3A4 inhibition
Use short course → 7–14 days depending on severity
What is Herpes Simplex Virus?
Most common cause of oral and ocular herpes
HSV-1 → causes most oral disease (HSV-2 can also cause ~20%)
Very common
Primary infection often occurs in childhood and may be asymptomatic
What are the different types of oral herpes simplex?
Primary herpes gingivostomatitis → First infection
Recurrent intraoral herpes → Reactivation inside the mouth, localized ulcers (often hard palate/gingiva)
Herpes labialis → cold sores, reactivation on the lip
What is the course of herpes labialis?
Prodrome → pain, itching, burning, tingling for 6 hours
Vesicle formation erythematous base, may merge
Ulcers/crust → develop within 72–96 hrs
Pain → worst early, then improves over 4–5 days
Healing → fully resolves in 8–10 days
What is the abortive therapy of choice for herpes labialis?
Valacyclovir → 1000 mg
Take 2 tablets at first sign → tingle/buzz
Then 2 tablets 12 hours later
Most effective if started within 6–8 hours of prodrome
Maintain good hydration
Supply of 16 tablets = about 4 treatment episodes
What are some possible reactivation triggers for herpes labialis?
Dental procedures if lip trauma
Physical or emotional stress
Fever, upper respiratory infections
Menstruation
Immunosuppression → due to drugs, disease or idiopathic
When are treatments for herpes labialis most effective?
Most effective if started within 48 hours of prodrome
Little benefit once lesions fully develop
Supportive options → ice applied frequently (about every 20 min)
Corticosteroids may reduce inflammation but are controversial
How are HSV infections different in immunosuppressed patients?
Harder to treat than in healthy patients
Require higher doses and longer treatment duration
Often need suppressive/prophylactic antivirals to prevent spread to organs/CNS
Lesions near the nose can signal eye involvement → ophthalmic emergency
How is topicals for herpes labialis?
Rx → Penciclovir 1% cream
OTC → Docosanol 10% cream
Apply thin film every 2 hours at onset of prodrome
Valacyclovir for primary HSV?
1g BID x 10 days
Valacyclovir for recurrent HSV?
2g BID once a day
FDA approved regimen
Acyclovir for primary HSV?
400mg TID x 10 days
Must remain hydrated to avoid renal problems
Acyclovir for recurrent HSV?
400 mg TID x 5 days
Must remain hydrated to avoid renal problems
What are HSV prophylaxis options and when are they used?
Used for frequent recurrences (≥6 episodes/year) or predictable triggers (e.g., sun exposure)
Acyclovir 400 mg BID (also 400 mg BID for 7 days before sun exposure)
Valacyclovir 500 mg daily (increase to 1 g daily if ≥9 episodes/year)
Therapy options for dry lips?
Chapped lips → moisturizer → Hydrous lanolin 3-4x a day
Lip balm → use when in sun 1-2x, put on after lanolin
How to treat angular cheilitis + staph?
Ketoconazole 2% cream and Bactroban 2% ointment in 1:1 ratio
Apply to lip first thing morning and last at night
After application → wait 30min before any other lip treatments
Do not use other steroids without further consultation
What are 3 topical and 1 systemic drug options for oral mucosal candidiasis?
Topical →
Ketoconazole
Clotrimazole
Miconazole
Systemic →
Fluconazole
Fluconazole dosing for angular cheilitis?
200 mg day 1
Then 100 mg daily for 7–14 days