Pathopharm II- Female Reproductive system disorders
1/123
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
124 Terms
Dysmenorrhea
Painful menstrual periods
Dysfunctional uterine bleeding (DUB)
AKA: Abnormal uterine bleeding
Premenstrual syndrome (PMS)
Signs and symptoms present before menstruation.
•Physical, emotional, behavior changes prior to menstrual cycle
‒50% of women have mild to moderate PMS
‒Abnormal response to neurotransmitters prior to menstruation
•Treatment with selective serotonin receptor inhibitors (SSRIs) have been helpful to regulate emotional changes.
Menorrhagia
Excessive menstrual blood loss
Menopause
Physiological cessation of ovulation and menstrual cycles Process begins on average age 51 years
Follicular phase
FSH stimulates ovarian follicles to produce estrogen
Days 1–14
FSH- gets everything ready to go.
Ovulation
Positive feedback by estrogen causes surge in FSH/LH
Ovum released from ovary
Day 14
Menstrual cycle involves
Approximately 28 days (may be longer or shorter depending on individual)
Follicular phase, Ovulation, Luteal phase
Estrogen-Stimulates uterine lining growth for implantation
Progesterone-Stabilizes uterine lining for implantation
Fertilization does not occur-Corpus luteum degenerates, Progesterone levels fall, Uterine lining shed
Luteal phase
Corpus luteum forms and produces progesterone
Days 14–28
phase- hope for fertilizations or get bleeding
Menarche
1st episode menstrual bleeding, typically 12-13 years old. 8-9 could indicate precocious puberty or endocrine disorder.
Menses
Menstrual bleeding
Menopause
No menses for a year!
•Permanent cessation of menstrual cycles
•Perimenopause: Gradual decline in ovarian function, time frame leading to menopause.
•Atrophic vaginitis, vasomotor instability
•Low estrogen, high FSH
Thelarche
•Development of breast tissue
•Occurs at about the same time as first menstrual period as part of puberty.
Breast lobules
•Drain into lactiferous duct
•Lactiferous duct empties into nipple surface
Prolactin
Milk formation
Oxytocin
Milk release
Precocious Puberty
under 8 or 9 years old
European American: <8 years
Hispanic/African American: <7.5 years
-Central: Hypothalamus-pituitary involvement
-Peripheral: Ovaries, testes, adrenal glands
Delayed Puberty
By age 13, lack of secondary sex characteristics. Over age 13.
Genetic causes
Constitutional growth delays
Other causes: Chronic illness, eating disorders, strenuous exercise
Infertility
Failure to achieve pregnancy within 12 months (1 year)
•Unprotected intercourse
•Therapeutic donor insemination in females <35 years
Male biggest cause is issue with sperm- amount, if mature
Women biggest cause is structural issues
Polycystic ovarian syndrome (PCOS)
Overproduction of androgens
Ovary does not release ovum
Premature ovarian failure (POF)
Body develops antibodies against ovarian tissue
Endometriosis
Uterine tissue outside the uterus
Fallopian tube damage
Ectopic pregnancy, infection, or inflammation
Cervical obstruction
Inherited malformation of damage to cervix
Uterine fibroids
Disrupt implantation
Amenorrhea
•Absence of menstrual period
•Pregnancy must be ruled out
Tend to be younger, lack of estrogen, progresterone
-Illness, athletes training a lot, signs of eating disorders.
Primary amenorrhea
•Menses does not occur before age 16
•Often congenital, unrecognized until puberty
•Mayer-Rokitansky-Kuster-Hauser syndrome (MRKH)
•Uterus absent and vagina foreshortened, normal ovaries.
Dysmenorrhea
•Painful periods
•75% of 15- to 25-year-olds
•Prostaglandin release (particularly prostaglandin F)
Diagnosis- Rule out pelvic pathologies (infection), or structural issues.
-Indicate Dysmenorrhea- pain that does not go away with medication, pain that interferes with daily life.
Treatment- Oral contraceptives and Anti-prostaglandins
Premenstrual dysphoric disorder (PMDD)
‒More severe form of PMS, interferes with work, school, social activities, and relationships, depressed mood
Menorrhagia
Excessive menstrual bleeding
Menses lasts greater than 7 days
Metrorrhagia
Excessive uterine bleeding
Both at time of normal menstrual period and more frequently- and in between, not really going through cycle.
Oligomenorrhea
Infrequent periods
Prolonged time between periods. Takes longer to get menses cycle, infrequent and irregular
Sexual history (5 Ps)
•Partners- if have multiple or just one
•Practices
•Prevention of STIs
•Past history of STIs
‒Gonorrhea, chlamydia, genital herpes, human papillomavirus, syphilis, and HIV
Pregnancy prevention- oral contraceptives, IUD
Papanicolaou smear (Pap smear)
Cervical cancer cellular changes, annule exam, screen for cervical cancers, Biopsy
Liquid-based cytology (LBC)
Study Cervical cell changes for cancer, HPV
Colposcopy
Visualize cervix, camara to visualize
Culdoscopy
Visualize uterine tubes and ovaries, camara to visualize
Carcinoembryonic antigen 125 (CA-125)
Marker associated with uterine fibroids, endometriosis, ovarian cancer, Tumor markers, blood draw
Hysteroscopy
Visualize interior of uterus, camara to visualize
Laparoscopy
Small surgical incision, view internal organs, camara to visualize
Mammography
Specialized x-ray to visualize breast tissue
Hormone replacement therapy (HRT)
Menopausal symptoms, prevent and slow down.
Weigh risk and benefits, give more estrogen
Excessive estrogen can cause cadiovascular issues, clotting issues and many other issues
What do Fertility drugs do?
Stimulate ovulation
In vitro fertilization (IVF)
Pregnancy, structural issues or want to have own child, healthy sperm, and low sperm count
Dilation and curettage (D & C)
Dilate cervix, surgical removal of lining of uterus, usually with ecptopic pregnancy, not abortions.
Hysterectomy
Surgical removal of uterus
Endometrial ablation
Removal of uterine lining
Cryosurgery
Remove portion of cervix for diagnosis for biopsy
NEVER MIX WITH ESTROGEN with
SMOKING.- vasoconstriction and puts women at higher risk for stroke.
What is Endometritis??
Infection of endometrosis- SOAP BOX
Usually a mixed infection
•Often ascending from vagina
•Gonococcus, Chlamydia trachomatis, Enterococcus
•May occur in conjunction of infection of other tissues
Symptoms= Vaginal bleeding, uterine tenderness, fever, malodorous discharge
Treatment- Antibiotics
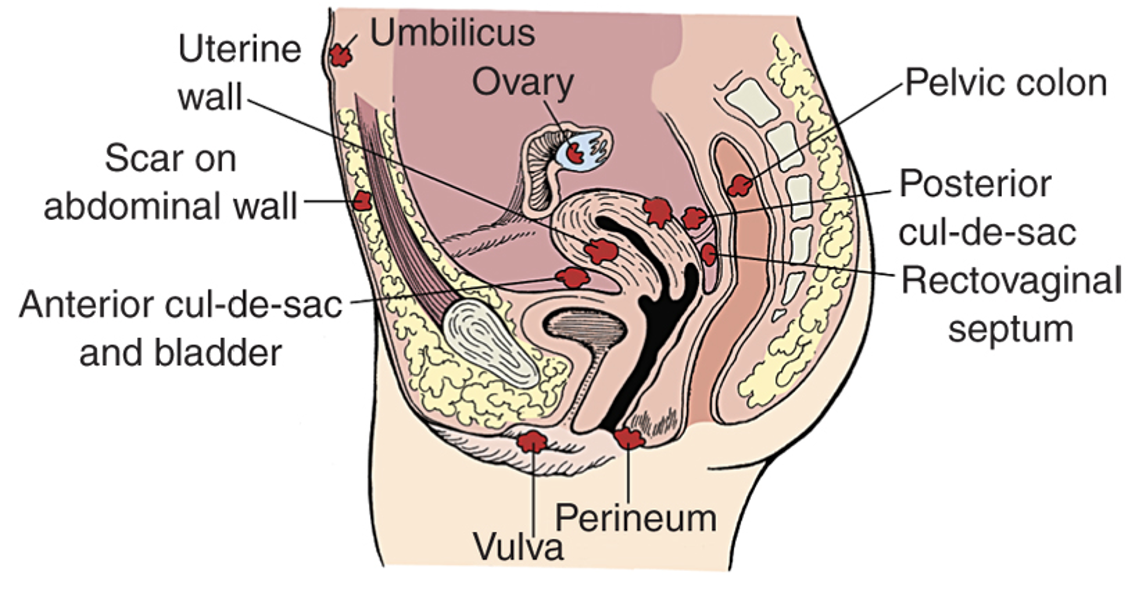
What is Endometriosis?
Endometrial tissue that has been moved.
•Growth of endometrial tissue outside of uterus
•~15% of women
•~80% of women with pelvic pain
•Ovaries, uterine ligaments, pelvic peritoneum,
•Displaced tissue responds to hormonal signals, causing bleeding, pain, infertility
•Biggest problem- infertility, Still responds to hormonal signals and continues to swell and bleed into body cavities.
Adenomyosis
•Endometrial tissue growing inside the muscle layer of the uterus
What are causes of Endometrosis?
Regurgitation/implantation= Endometrial tissue forced up through uterine tubes and into pelvic cavity.
Metaplastic= During embryological development, endometrial tissue appears in abnormal areas, placed wrong.
Vascular or lymphatic= Endometrial tissue metastasized to other areas.
Immunological= Displaced endometrial tissue triggers an autoimmune attack, body attacks it.
Environmental toxicity= Associated with some chemicals (dioxin).
How is Endometriosis diagnosed and treatment?
Definitive diagnosis: Laparoscopy
Treatment
•NSAIDs: First-line- try to control inflammation, Combined oral contraceptives and oral progestins- to regulate period. Progestin-only
•Long-acting GnRH agonists
•GnRH antagonists
•Aromatase inhibitors- prevent excessive estrogen
•Selective progesterone receptor and selective estrogen receptor modulators (SERMs)
•Surgery (not curative)- Remove pieces of tissue, trying to control
Endometrial Polyps
Neoplastic growth, unknown origin
•Usually benign – polyps are benign mucosal tumors.
•Postmenopausal females, vaginal bleeding, highest risk of for malignancy
Diagnosis: 3D color Doppler transvaginal ultrasound, hysteroscopy, biopsy
Treatment= Hysteroscopic surgical polypectomy- to remove polyps
•Hysterectomy recommended with atypical findings
Leiomyomas
Commonly known as fibroid tumors
•75% of women at some point in their lives, May regress at menopause (get better/change in size), Myometrium
•Most asymptomatic, If signs/symptoms present: Bleeding, pain, infertility
Diagnosis: Ultrasound
Treatment: Surgical excision, GnRH
Abnormal Uterine Bleeding
Presents with; Varies, Excessive blood loss, Lack of normal menstruation.
Causes- Vary with age= Adolescents, perimenopausal women: Anovulation, Increasing with age: Structural lesions, malignancies
Anovulatory- Immature hypothalamic–pituitary–ovarian axis.
Ovulatory- Excessive uterine bleeding can occur
Defects in the control mechanisms of menstruation
Abnormal Uterine Bleeding: Assessment and Diagnosis- Treat cause
Rule out pregnancy (b-hCG), Hemodynamic instability and anemia, Identify bleeding source
Blood tests=Complete blood count, Coagulation factors, clotting times, Hormone levels
Determine if following present: Primary ovarian insufficiency, Ovarian tumor, Perimenopause, PCOS.
Rule out: if infrequent, Eating disorders, Certain medications
Testing: Pelvic examination, Cervical cancer screening, Ultrasound, Hysteroscopy, Saline infusion sonohysterography
Abnormal Uterine Bleeding: Treatment
Hemodynamically unstable patients- bleeding out- MEDICAL EMERGENCY
•Uterine tamponade using a Foley catheter or gauze packing
•IV tranexamic acid
Hemodynamically stable
•Hormonal regulation
Surgery
Uterine Prolapse
Protrusion of uterus into vagina- uterus protrudes into vaginal opening.
Multiparous women
Degrees of prolapse
Pessary- Supportive device that is inserted to hold uterus in position- keep uterus in place.
Cause and Treatments for Uterine Prolapse?
Causes: usually age related
•Injury to the levator ani muscle or local nerves
•Pelvic masses, obesity, chronic constipation, connective tissue disorders
•Menopause: Reduced estrogen
Treatments: Kegel exercises- to help gain muscle tone. Native tissue repair without synthetic mesh, Transvaginal hysterectomy, Manchester-Fothergill surgical procedure‒Which is a uterine-preserving technique
Cystocele
Herniation of urinary bladder into vaginal canal. The bladder can have a tear and open into vaginal canal
Rectocele
Herniation of rectum into vaginal canal
Enterocele
Herniation of intestine between uterine ligaments
Herniation treatment
Surgical intervention
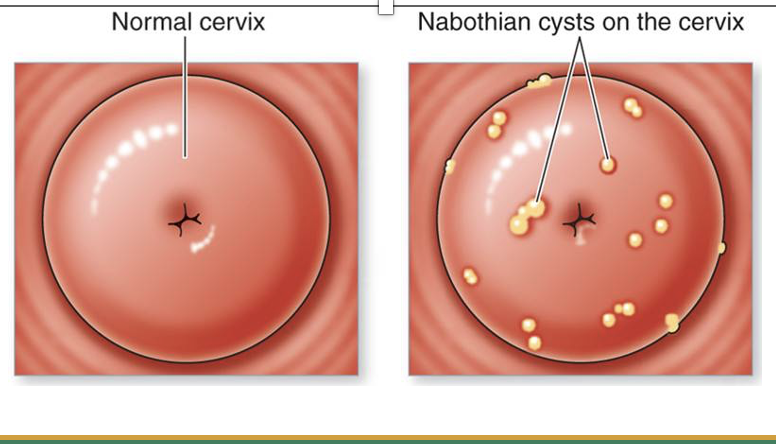
Nabothian cysts
In the Cervix Blockage of mucus-secreting gland in endocervix
•Common, benign, no treatment needed
Cervicitis
•Inflammation of cervix
•Ascending infection from vagina
•Erosion and epithelial cell changes apparent
Cervical polyps
•Usually benign, inflammatory changes of endocervix
•May cause postcoital bleeding, usually after sex
Prevention of Cervical Cancer includes?
High-risk types of human papillomavirus
•hrHPV
•Strains HPV 16 (most carcinogenic) and HPV 18
HPV infections- Different strans, Common
•Most resolve without clinical consequence
Risk factors: Smoking, immunocompromised state, HIV
HPV Vaccination done to Prevent Cervical Cancer are done at?
•2-dose schedule
‒Initiating vaccination at ages 9 to 14 years
•3-dose schedule
‒Initiating at ages 15 to 26 years
Immunocompromised
Vulvodynia
Pain of the vulva
Yeast infection, chemical irritants, infection
Vulvar cancer
Rare
Bleeding, itching, palpable mass, tenderness
Bartholin cyst or abscess
Small spherical structures at entry to vagina
Release secretions, can become infected
Antibiotics
Genitourinary syndrome of menopause (GMS)
AKA: Atrophic vaginitis
Inflammation of vagina after menopause
Caused by low estrogen
Low-dose vaginal estrogen treatment
Vaginitis
•Inflammation of vagina
‒Discharge, burning, itching
‒Pain with urination, sexual intercourse
•Bacterial causes (40% to 45%), vaginal candidiasis (20% to 25%), trichomoniasis (15% to 20%)
•Precise identification of organism is crucial to treatment
•Preventive measures‒Proper hygiene, avoidance of feminine deodorants and douches
Premature Ovarian Insufficiency (POI)
Cessation of ovarian function in women less than 40 years of age |
Genetic, autoimmune |
Irregular menstrual cycles, infertility, hot flashes |
CVD, cognitive decline |
Elevated FSH Other reproductive hormones |
HRT Transdermal or transvaginal estradiol therapy |
Follicular cyst
•Failure to eject ovum during ovulation
•Usually asymptomatic, spontaneous regression
Corpus luteum cyst
Occurs after ovulation
Usually causes symptoms, may rupture
•Pelvic pain, amenorrhea, followed by irregular or heavy bleeding
•Ultrasound confirms diagnosis, Rule out pregnancy, Laparotomy may be necessary to remove cyst
-Very painful, 1st rule out appendencitis, begin. If happen a lot may need to control with contraceptives
Ovarian Torsion
Twisting of ovary |
Obstructed blood flow |
Severe, unilateral pain |
May suspect GI issue (nausea/vomiting) |
Rule out: Ectopic pregnancy |
Ultrasound with color Doppler |
Surgical removal Salvageable detorsion |
Ovarian Teratoma
AKA: Dermoid cyst |
Various embryonic tissues |
Often benign |
Symptomatic with complications |
Blood testes (AFP, CA-125, b-HCG, etc.) |
Imaging studies |
Surgical excision |
Polycystic Ovarian Syndrome (PCOS)
Autosomal dominant genetic disorder
•Women: Puberty to age 30 years
•Most common endocrine disturbance in young women
•Leading cause of infertility in the United States
Anovulation- Follicular cysts, Hypothalamic-pituitary-ovarian axis dysfunction.
Androgen excess, anovulation, hyperinsulinemia
Diagnostic criteria- Different specialty societies have varying criteria
‒Biochemical or clinical hyperandrogenism
‒Ovulatory dysfunction
Evaluate for insulin resistance, T2DM
Treatment of Polycystic Ovarian Syndrome (PCOS)
•Reverse androgen excess
•Stimulate cyclic menstruation
‒Oral contraceptives
•Restoring fertility
•Ameliorate endocrine disturbances
‒Insulin sensitizers
Ectopic Pregnancy
Fertilized ovum implants outside the uterus
•98% occur in fallopian tubes
•Pain, vaginal bleeding, and amenorrhea are present
•Low level hCG (pregnancy hormone)
•Culdocentesis‒Will reveal blood if rupture
•Laparoscopic salpingostomy‒Remove ectopic pregnancy
Salpingectomy required if rupture
Fibrocystic breast disease
•Largely benign
•Female: 35 to 50 years of age
•Granular breast masses‒Prominent in second half of menstrual cycle
•Tenderness, vascular engorgement, and cystic distention‒Dissipates with menses
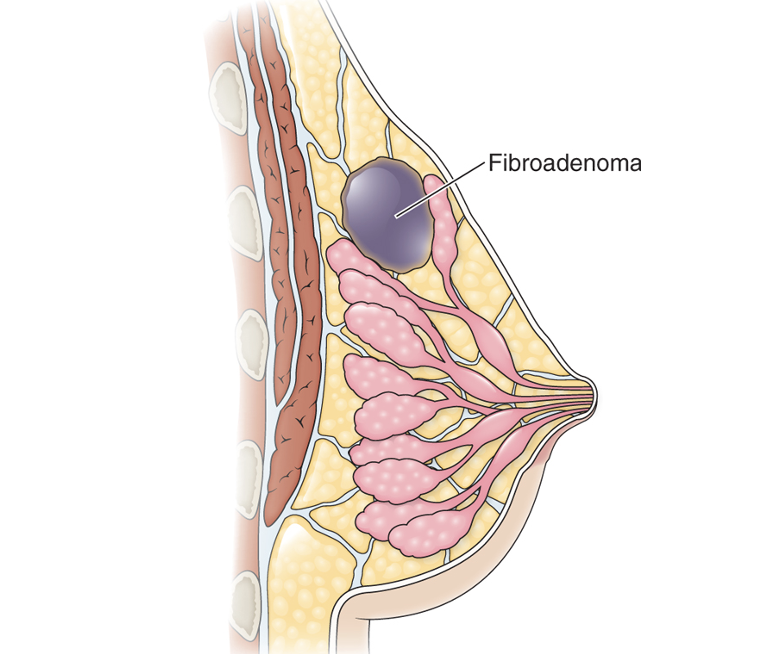
Fibroadenoma
•Benign breast mass
•Female: 25 to 45-year-olds
•Premenopausal women
•May indicate increased risk for breast cancer
•Single, “rubbery” mass
Mastitis
•Inflammation of breast, most commonly occurs with lactation
Galactorrhea
•Secretion of breast milk in non-lactating breast
•May be caused by prolactin-secreting pituitary tumor
Galactography or mammary ductography
Mammary duct ectasia
•Inflammation in subareolar ducts
•Common in postmenopausal women
•Small, calcified mass
Biopsy usually performed
Mammoplasty
Aesthetic surgery of the breast
Mastopexy
Shape of the breast and lifts the breast
Mammoplasty-augmentation or mammoplasty-reduction
Size of breast
Prophylactic Mastectomy: Prevention of Breast Cancer
Mutations in BRCA1 and/or BRCA2 genes
•Risk estimates are extremely heterogeneous
•Multiple strategies
‒Surveillance
‒Chemoprevention
‒Bilateral salpingo-oophorectomy
‒Risk-reducing mastectomy
What is a Gynecological emergency?
Ovarian torsion- May present similarly to appendicitis
Diagnosis of ectopic pregnancy
•Considered whenever a female of reproductive age complains of abdominal or pelvic pain
Therapeutic actions of Estrogens?
•Affect release of FSH and LH, Cause capillary dilation, fluid retention, and protein anabolism and thin the cervical mucus
•Conserve calcium and phosphorus and encourage bone formation. Inhibit ovulation
•Prevent postpartum breast discomfort, Responsible for the proliferation of the endometrial lining
•Absence of or decrease produces signs and symptoms of menopause, Compete with androgens for receptor sites
Systemic effects caused by Estrogens?
positives about estrogen replacement
•Protecting the heart from atherosclerosis
•Retaining calcium in the bones
•Maintaining the secondary female sex characteristics
Indications for Estrogens?
•Hormone replacement therapy (HRT)
•Palliation for discomforts in first few years of menopause
•Treat female hypogonadism and ovarian failure
•Prevent postpartum breast engorgement
•Part of combination contraceptives
•Slow bone loss in osteoporosis
Palliation in certain cancers
Pharmacokinetics for Estrogens?
•Well absorbed through the GI tract
•Undergo extensive hepatic metabolism, excreted in urine
•Cross placenta and enter human milk
•Available in multiple forms
Contraindications for Estrogens?
•Allergies and pregnancy
•Idiopathic vaginal bleeding, breast cancer, and estrogen-dependent cancer, thromboembolic disorders
•Undiagnosed atypical vaginal bleeding, Breast cancer or any estrogen-dependent cancer
•History of thromboembolic disorders, Heavy smoking, Hepatic dysfunction
•Pregnancy, Breast or chestfeeding
Cautions for Estrogens?
•Metabolic bone disease
•Renal insufficiency
•Hepatic impairment
Adverse effects for Estrogens
•GU effects
•Systemic effects
•GI effects