NTRN201 Final (Energy - Life Cycle Nutrition)
1/131
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
132 Terms
risk of obesity
increase risk of chronic disease - cancer, heart/kidney disease, diabetes
adipokines
hormones made in adipose tissue, regulate inflammation
inflammation leads to
heart disease, insulin resistance, etc.
can someone with obesity be healthy
maybe - lower bp without meds, smaller waistline, etc could protect organscan
adiposity
body fat
risks for underweight
increased risk of death, less storage for times of undernutrition
weight tells abt composition - T/F
false
body composition evaluates:
total body fat, location of body fat, weight related medical problems
BMI - body mass index
weight for height standardization
who does BMI apply to
men and women
BMI equation

BMI: underweight, healthy, overweight, obese ranges
under: <18.5, healthy: 18.5 to <25, over: 25 to <30, obese: >30
BMI doesn’t apply to
children, teens, older ppl, pregnant/lactating women
good amt of body fat
men: 8% to 24%, women: 21% to 35%
why women need more body fat
needed for reproductive functions
measuring body fat
consider body weight and volume, with underwater weighing, air displacement, skinfold thickness, bioelectrical impedance, dual energy x-ray absorptiometry (DXA)
most accurate method of measuring body fat fontent
dual energy x-ray absorptiometry (DXA), releases some radiation through body to measure body fat/bone density
upper body (android) obesity related to:
heart disease, high bp, T2D
android obesity seen in
males (high blood testosterone), high glycemic diets, high alcohol intake, smokers
measuring android obesity
>40 inch waist males, >35 inch waist females
female hormones - estrogen and progesterone - lead to fat storage in ___ body
lower: small belly, large buttocks and thighs
how does menopause affect women
estrogen levels fall, belly fat distribution in women
chance for children with no obese parents becoming obese
10%
chance for children with 1 obese parent becoming obese
40%
chance for children with 2 obese parents becoming obese
80%
weight gain in twins
similar even when raised apart
percent of weight differences accounted for by genes
40%-70%
can inherit a metabolism that uses energy more efficiently or stores fat more readily T/F
true
set point theory
genetically predetermined body weight or fat content thats regulated by body
REGULATION: reduce E intake, thyroid hormone less secreted, slows metabolism
when weight lost, body more efficient at storing fat
similarities among family memebrs in body weight due to
due to learned behaviors, friends/couples could behave similarly toward food
gene pool hasn’t changed much over 50 years BUT
obesity increased a lot
genes and environment both affect body weight and composition regardless of genetic predisposition T/F
true
energy balance
relationship between energy intake and energy expenditure
energy equilibrium
When calories consumed matches the amount of energy expended
positive energy balance
Energy intake exceeds energy expenditure and results in weight gain
negative energy balance
Energy intake is less than energy expenditure and weight loss occurs
when do u want positive energy balance
pregnancy, infancy, childhood, adolescence
TIMES OF GROWTH
when do u want negative energy balance
when body fat exceeds healthy levels in ADULTS
if not during times of growth, can impair normal growth pattern
does aging cause weight gain
no
measure calories
bomb calorimeter
calculate using grams per macronutrient
why does body use energy
basal metabolism
physical activity
digestion, absorption, processing of ingested nutrients
form of energy output - minor
thermogenesis → during fidgeting or shivering
basal metabolism
min. amt of E used to keep someone resting/alive in warm/quiet envt
heart beating, respiration, organ activity
60-70% of total expenditure
resting metabolism
person not fasting or rested
number of calories burned per unit of time - measurement of BMR/RMR
women - 0.9 kcal/kg per hour
men - 1.0 kcal/kg per hour
increase basal metabolism
greater muscles mass
larger body surface
male
body temp
high secretion of thyroid hormone
nervous system activity
growth stages
caffeine/tobacco use
recent exercise
decrease basal metabolism
low secretion of thyroid hormone
restricted calorie intake
less body surface area/muscle mass
aging after 30 yrs
big cause of obesity in america
inactivity → drive instead of walk, elevator instead of stairs
physical activity increases energy expenditure by _% above basal needs
25-40%
thermic effect of food - TEF
energy to digest, absorb, transport, metabolize food
increases w larger meals
what percent of energy consumed is thermic effect of food
5-10%
TEF changed by food composition T/F?
TRUE
protein rich - 20-30% (most energy to store)
carbs - 5-10%
fats - 0-5% (easiest to store)
alcohol - 20%
thermogenesis
heat production
small contribution to total E expenditure
when body uses E for non-voluntary physical activity →fidgeting, shivering, maintaining muscle tone, holding body upright
how to measure energy used by body
direct or indirect calorimetry
energy used can be estimated based on
height
weight
physical activity
age
direct calorimetry
estimate E expenditure measuring amt of heat released by body
60% of E used leaves as heat
person goes into chamber, change in water temp determines energy used
indirect calorimetry
collect exhaled air → measure amt of O consumed and CO2 produced
estimated energy requirements (EERs)
estimate energy needs based on:
weight
height
gender
age
physical activity level
moderate restriction is recommended
during fast, nervous system/brain needs glucose for energy
glycogen used first
then ketosis → breaks down fat into ketone bodies to fuel brain
ketosis
break down fat into ketone bodies, some amino acids yield ketone bodies
intermittent fasting
helpful fasting, controlled and time restricted
harmful fasting
severe restriction
muscle breakdown, nutrient deficiency
breakdown protein
protein → amino acids
excess converted to glucose/fat
breakdown fat
fat→ glycerol/fatty acids
excess stored as body fat
breakdown carbs
carbs → monosaccharides
excess converted to glycogen/fat
breakdown alcohol
used for fuel or converted to fat
ghrelin
hunger
stomach and hypothalamus
appetite
can occur without hunger
leptin
satiety
stomach, small intestine, brain
regulates frequency of meals
hunger
physiological drive to find/eat food
controlled by organs, hormones, nervous system
appetite
psychological drive to eat
controlled by society, time of day, mood, memories, sight
hypothalamus
site of regulation for satiation
communicates w endocrine and nervous system
internal cues of blood glucose lvls, hormone secretions, sympathetic NS
fulfilling hunger/appetite leads to
satiety
can hunger bc of lack of appetite T/F
true
don’t like the food being served
or opposite, dessert on full stomach
internal signals stimulate satiety center, we
stop eating
internal signals stimulate feeding center, we
eat more
satiety
elicity by sensory aspects, knowledge that food’s been eaten, chewing, expansion of stomach/intestines, low energy dense food increase it, effects of digestion/absorption/metabolism
process of satiety
hormones during digestion turns off hunger
cholecystokinin
glucagon-like peptide-1 (GLP-1)
short term satiety
decrease ghrelin → short term satiety
long term satiety
body composition and amt of body fat
adipose tissue secretes leptin to reduce food intake and decrease body fat
signals to eat
after eating, macronutrient [ ] decrease, body uses stored energy
satiety decreases
cortisol and ghrelin stimulate appetite
satiety vs satiation
perception of fullness that lingers after a meal
perception of fullness that builds during a meal
brown adipose tissue (BAT)
type of body fat that burns calories to generate heat when you’re cold
outside the body theories for obesity
availability/larger portions of food
dopamine when eating
screen time/sedentary jobs lower physical activity
food deserts/forests (availability of food)
percent of people following commercial diet programs that succeed
5%
how much weight regained within 3 to 5 years of weight loss
1/3 of the weight
method thats routinely successful against obesity
surgery
weight cycling
gaining and losing weight in a cycle
negatives of weight cycling
increased upper body fat
less self esteem
decline HDL cholesterol
decline immune system function
weight loss
energy intake less than energy needs (still give nutrients for health)
avg limited energy intake
women - 1200 kcal/day
men - 1800 kcal/day
low energy density approaches (low fat, high fiber) more successful long term T/F
true
steady weight loss amt of energy spent
100 to 300 kcal per day above normal activity
resistance exercises
increase lean body tissue and metabolic rate
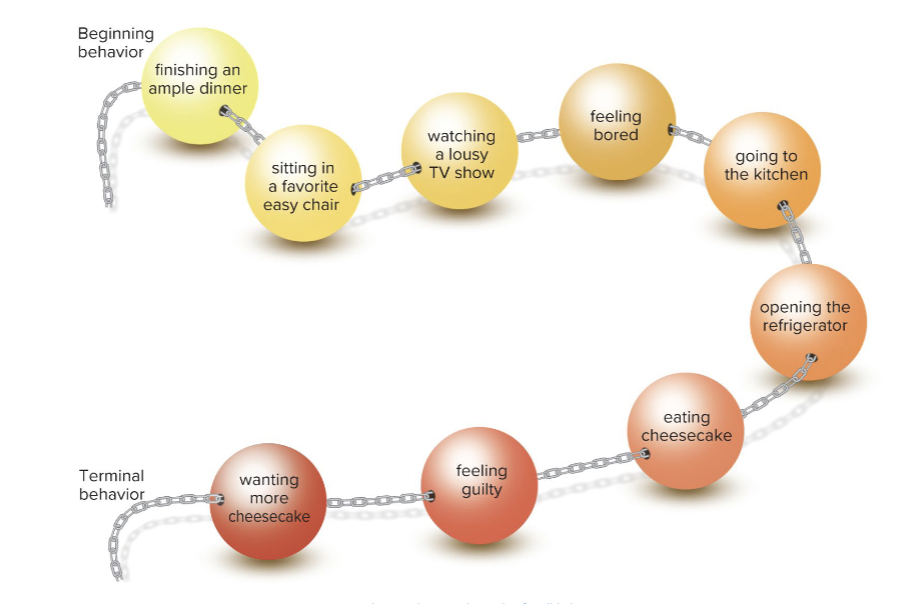
chain breaking
separate behaviors that occur together
stimulus control
alter environment to minimize stimuli for eating
cognitive restructuring
change frame of mind regarding eating
contingency management
prepare for situations that may trigger overeating
self-monitoring
track food eaten when, why, how you feel, physical activities, body weight
behavior chain