MSK + Rheumatology
1/945
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
946 Terms
infant abnornmalities seen in orthopaedics
spina bifida
proximal femoral focal deficiency
TAR syndrome
thalidomide poisoning
congenital scoliosis
metatarsus adductus
infantile postural scoliosis
plagiocephaly
Talipes-Equino virus
prerequisites of normal gait
stability in stance
clearance in swing
preposition of foot
adequate step length
energy conversation
what is characteristic of a walking gait
single support and double support
what is characteristic of a running gait
double swing
gait cycle
defined from initial contact of one limb to subsequent initial contact of same limb
what is physiological varus and when is it seen up to
bow legs, seen up to 18 months
which immunological process best explains the rheumatoid factor
IgM antibody against the Fc portion of the patient’s own IgG
what is physiological valgus and when is it seen up to
knock knees
between 18 months and 7 years
MSK issues that cause concern in children
bow legs
flat feet
curly toes
late walkers
what is femoral anteversion
femoral neck leans forward with respect to the rest of the femur causing the leg to rotate internally.
Internal rotation of the femur - 40 degrees at birth
seen in school age

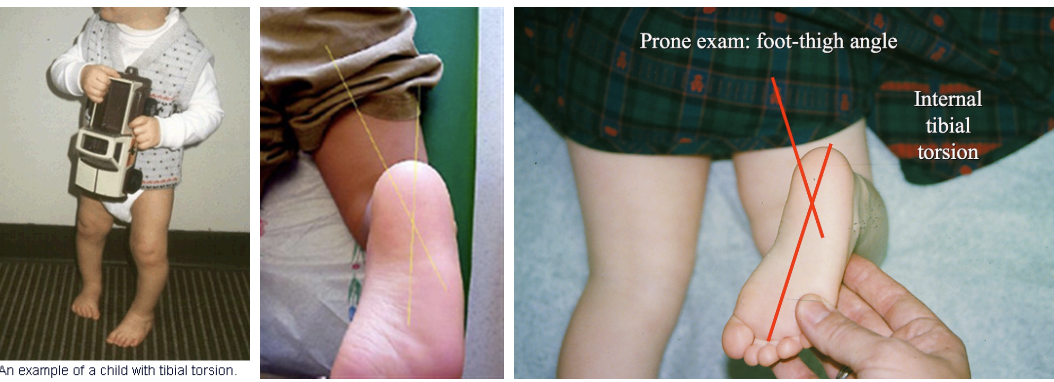
what is internal tibial torsion
internal rotation of the tibia and an in-toeing gait.
thigh foot angle > 10 degrees
seen in infants < 4
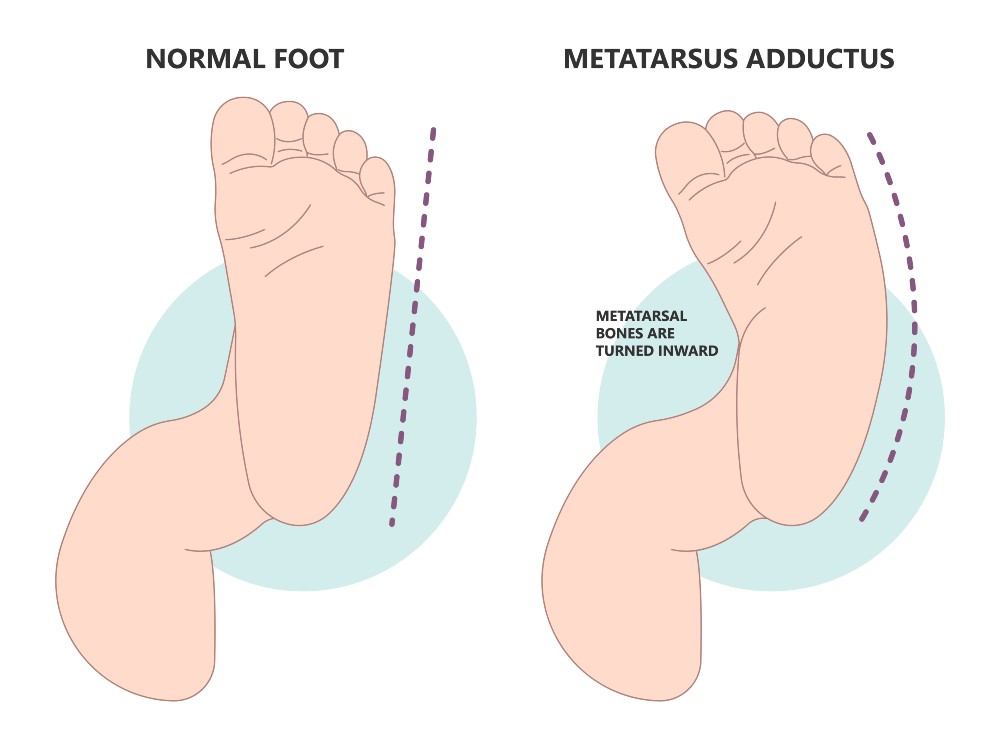
what is metatarsus adductus
the medical term for in-toeing
seen in newborns
treatment is stretches
flexible flat feet
normal at birth due to fat foot pad and lax ligaments diminishes with age
- no benefit of insoles
how to examine a child with an intoed gait
Assess the Thigh-Foot Angle: This helps identify Internal Tibial Torsion.
Assess Femoral Anteversion: This is a developmental norm where the femur is rotated; 80% of children reach a normal degree of rotation by age 16.
Check Foot Flexibility: For metatarsus adductus, if the foot is flexible, splintage is not required.
Note Progression: Clinicians should know that intoeing does not improve in children with neuromuscular disease
what is cadence
number of steps taken per unit of time and is the rate at which a person walks expressed in steps per minute
100-115
how much is your eye moving during normal gait cycle
16 frames per second
velocity
distance/time
-mean velocity (m/min) = step length (m) x cadence (steps/min)
stride length vs stride period and step length
step length = right initial contact to left initial contact
stride length = the distance from right heel contact to the following right heel contact.
stride period/cycle time = the period of time in seconds from initial contact of one foot to the following initial contact of the same foot.
what is comfortable walking speed
80 m/min
minimum energy consumption per unit distance
what is curly toes
3rd or 4th tie have tight flexor tendons - mostly a cosmetic issue
mean walking age
12 months
when would a child be referred to paediatric orthopaedics
5 S's
- symptoms
- symmetry - lack of
— stiffness
- syndromes
- systemic illness
bone or joint pain that is worse at night is what until proven otherwise?
considered infection or tumour
which of the following are characteristic of walking in old age:
a - up to ¼ loss of joint range by 65 y/o
b - decreased cadence
c - reduced step length
d - reduced ankle plantarflexion
e - impaired balance
a - up to ¼ loss of joint range by 65 y/o
c - reduce step length
d - reduced ankle plantarflexion
e - impaired balance
cadence does not change
what is spastic diplegic
form of spastic Cerebral Palsy that primarily affects movement in the legs. It causes muscle stiffness, tightness, and jerky movements
what is polymyalgia rheumatics
SUDDEN onset inflammatory condition that causes pain and stiffness in shoulders, pelvic girdle and neck
presentation of PMR
relatively rapid onset but symptoms need to be present for at least 2 weeks to consider PMR diagnosis
- pain and stiffness in shoulder (elbow and upper arm too), pelvic girdle and neck
characteristics of stiffness and pain in PMR
worse with movement
interferes with sleep
takes at least 45 mins to ease in morning
difficulty in daily activities e.g. getting dressed
associated features of PMR
systemic symptoms - weight loss, fatigue, low grade fever
muscle tenderness
carpal tunnel syndrome
peripheral oedema
diagnosis of polymyalgia rheumatica
•Compatible history
•Age > 50
•ESR/plasma viscosity high
•Dramatic steroid response
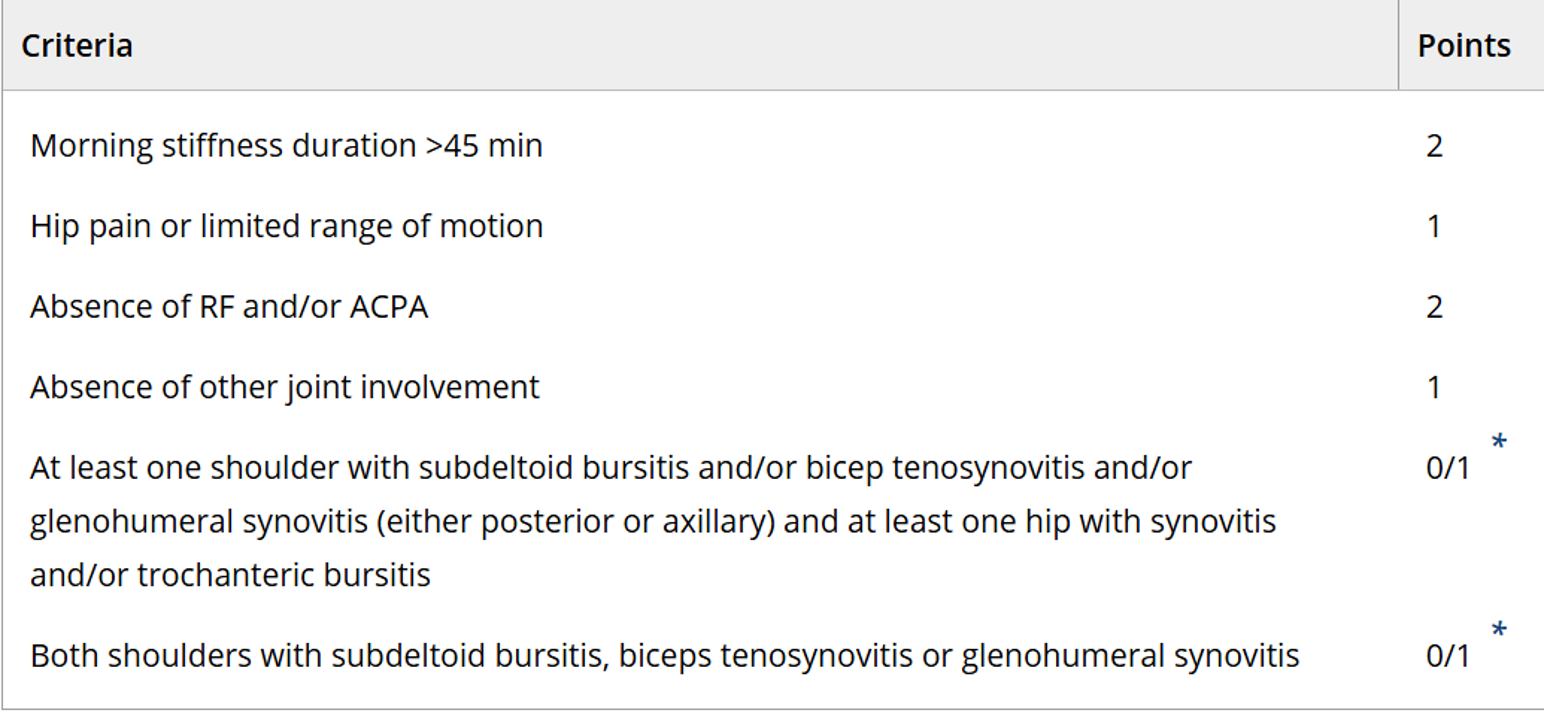
EULAR/ACR classification criteria for polymyalgia rheumatica
Morning stiffness duration >45 min: 2 points.
Hip pain or limited range of motion: 1 point.
Absence of Rheumatoid Factor (RF) or Anti-citrullinated protein antibodies (ACPA): 2 points.
Absence of peripheral joint pain (other joint involvement): 1 point
imagine for PMR
•Ultrasound
•MRI
•CT PET
–Subacromial subdeltoid bursitis
–Long head biceps tendinitis
investigations for mimics of polymyalgia rheumatic
•Myalgic onset Inflammatory joint disease – CCP ab
•Inflammatory muscle disease – CK (normal in PMR)
•Hypo/ hyperthyroidism - TFTs
•Bilateral shoulder capsulitis - imaging
•Fibromyalgia
•Check bone profile and vitamin D – important for muscle strength
important to rule out in PMR
giant cell arteritis (temporal arteritis)
Underlying malignancy
e.g., multiple myeloma (immunoglobulins), lung cancer
what blood tests need to be done before initiating steroid therapy
FBC
U&Es
LFTs
calcium
serum protein electrophoresis for myeloma
TSH
CK for myosotis
RF for RA
urine dipstick
additional investigations that are commonly done with PMR
ANA for SLE
anti-CCP for RA
CXR
urine bence jones protein for myeloma
treatment of PMR
prednisolone
- 15mg daily initially - follow up after 1 week
how long does steroid treatment for PMR usually last
1-2 years - reducing regime
- 15mg until symptoms controlled
- 12.5mg for 3 weeks
- 10mg for 4-6 weeks
- reducing by 1mg every 4-8 weeks
steroid sparing treatment for refractory Polymyalgia rheumatica
•Cs DMARDs
–Methotrexate
–(Azathioprine)
•bDMARDs
•Activated dendritic cells – CD4+ T cells – IL6 (and macrophage activation)
–Tocilizumab (Jak inhibitors)
additional management for patients on long term steroids - don't STOP mnemonic
don't - steroid dependence occurs after 3 weeks and suddenly stopping causes ADRENAL CRISIS
S = sick day rule - steroid dose increase if patient becomes unwell
T = treatment card - patient should carry steroid treatment card to alert others they are on steroids incase of emergency
O = osteoporosis - biphosphonates and calcium and vitamin D for prevention
P = PPI considered e.g. omeprazole
50% of patients with giant cell arthritis may have…
so what will you ask them
polymalgia rheumatica
if they have headache, vision changes, jaw pain
crystal deposition disease are characterised by
deposition of mineralised material within joints and peri-articular tissue
crystal deposition diseases commonly seen in practice
•Monosodium urate - gout
•Calcium pyrophosphate dihydrate (CPPD) - Pseudogout
•Basic calcium phosphate hydroxy-apatite (BCP) – calcific periarthritis/tendonitis
complete deficiency of HGPRT leads to
Lesch-Nyhan syndrome
X chromosome-linked recessive genetic disorder
intellectual disability
aggressive and impulsive behaviour
self harm
gout
renal disease
-lack of recycling of purines
what causes over production of uric acid
malignancy
severe exfoliative psoriasis
drugs
ethanol
cytotoxic drugs
HGPRT deficiency
inborn errors of metabolism
causes of hyperuricaemia that can lead to gout
High purine diet (red meat, seafood)
renal impairment
hypertension
hypothyroid
alcohol
drugs
low does aspirin
diuretic
ciclosporin
exercise, starvation, dehydration
lead poisoning
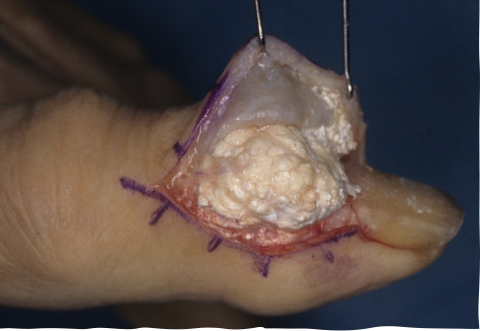
what is tophus-tophi
massive accumulations of uric acid
gold standard investigation for mono-arthritic joint
synovial fluid aspiration and analysis
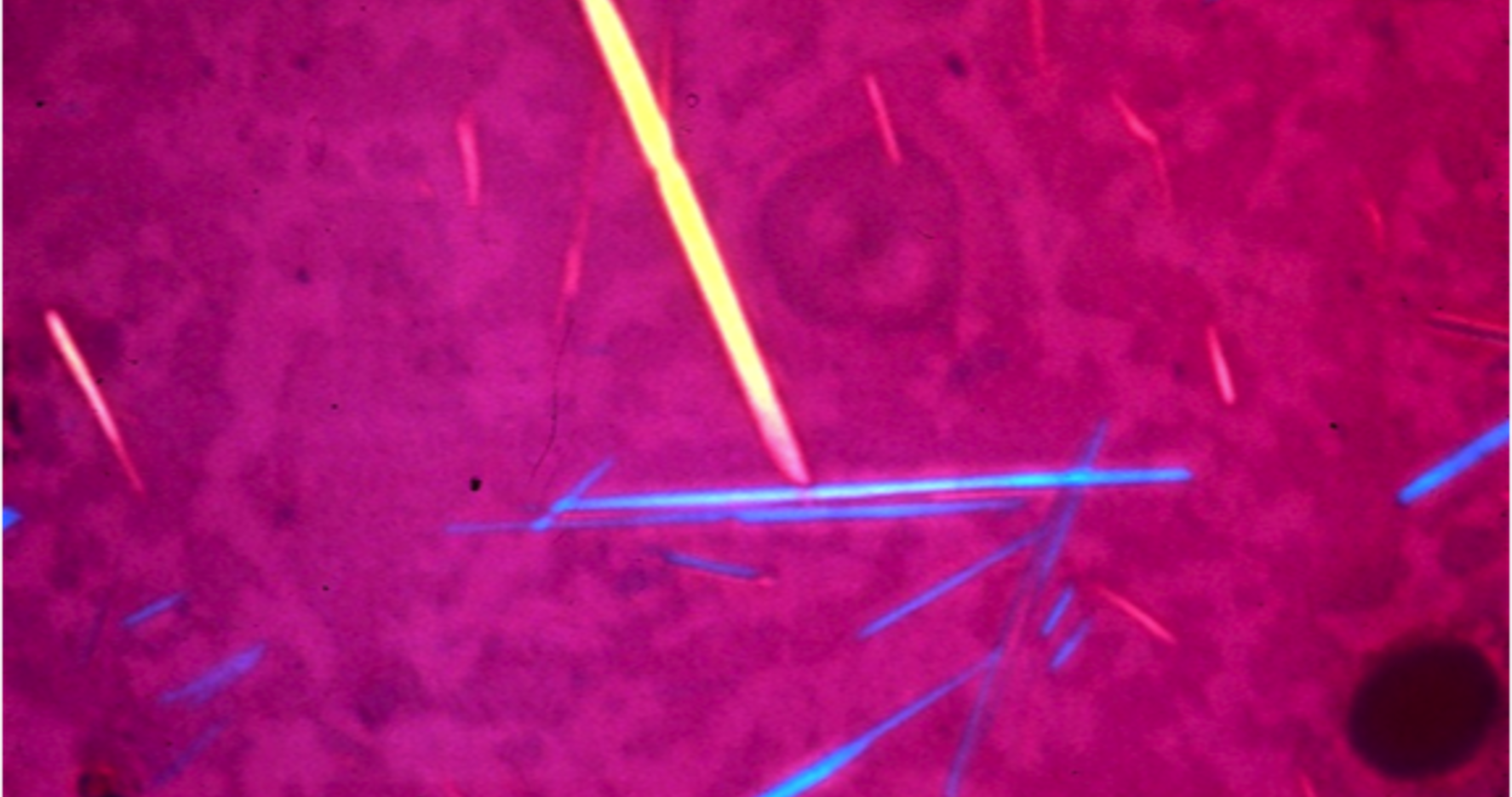
name and description of gout crystals
monosodium urate
needle-shaped crystals
management of acute flare of gout
NSAIDs
colchicine
steroids - intraarticular injection, IM injection, oral
long term management of gout - 1st attack not treated unless
–Single attack of polyarticular gout
–Tophaceous gout
–Urate calculi
–Renal insufficiency
long term management of gout - treat if 2nd attack within..
1 year
•Prophylactically prior to treating certain malignancies
do you treat asymptomatic hyperuricaemia?
NO
just monitor until a flare
in recurrent gout flares, what is your uric acid target
300-360
drugs that lower uric acid
xanthine oxidase inhibitor - allopurinol, febuxostat
uricosuric agents - probenecid, benzbromarone
IL-1 inhibitor - canakinumab
paradoxical flare in gout
an acute attack that occurs shortly after starting urate-lowering therapy (ULT) like allopurinol. Although the medication is meant to prevent flares, the rapid reduction of uric acid causes existing, solid tophi crystals to dissolve and release, triggering intense inflammation. This requires co-prescription of preventive medicine e.g., colchicine or NSAIDs
rules for lowering uric acid levels
Wait until the acute attack has settled before attempting to reduce the urate level
Use prophylactic NSAIDs or low dose colchicine/steroids until urate level normal - Prophylactic treatment for at least one month after last dose adjustment has been made.
Adjust allopurinol dose according to renal function
most common part of body affected by pseudogout and gout
pseudogout - knee
toe - gout
pseudogout affects who mainly
elderly females
pseudogouut triggers
trauma
intercurrent illness
causes of pseudogout
idiopathic
familial
metabolic
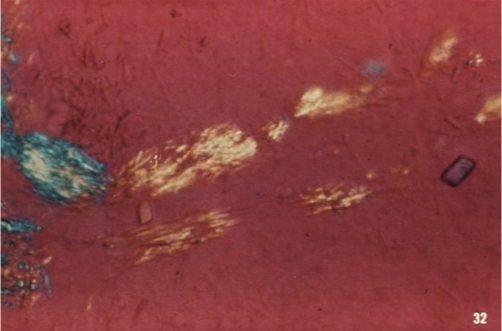
pseudogout
form of arthritis triggered by deposits of calcium crystals (calcium pyrophosphate dihydrate) in the joints.
erratic flare
rhomboid shaped crystals
pyrophosphate crystals
management of pseudogout
NSAIDs
intra-articular steroids
*no preventative therapies
chondrocalcinosis
deposition of calcium pyrophosphate crystals in joint cartilage

what is SLE
multisystem autoimmune disorder related to antibody-mediated cellular attack and deposition of antigen-antibody complexes
aetiology of SLE
genetics - polygenic mode of inheritance
hormones
environment - UV, drugs, infection
pathogenesis of SLE
immune response against endogenous nuclear antigens - break in immunological tolerance
immune complex formation
tissue injury
- type 3 hypersensitivity
symptoms of SLE
- any 4 for diagnosis
malar rash (butterfly rash)
discoid rash (raised, scarring, permanent marks, alopecia)
photosensitivity
oral ulcers
arthritis (2 joints at least)
serositis (pleurisy or pericarditis)
renal (significant proteinuria or cellular casts in urine)
neurological (unexplained seizures or psychosis)
haematological (low WCC, platelets, lymphocytes and haemolytic anaemia)
immunological (anti ds-DNA, Sm, cardiolipin, lupus anticoagulant, low complement)
ANA
lupus nephritis - SLE kidney - classs I-VI
I - minimal mesangial
II - mesangial proliferative
III - focal
IV - diffuse
V - membranous
VI - advanced sclerosing
when to consider SLE
woman of childbearing age with: -
- constitutional symptoms of fever, weight loss, malaise and severe fatigue
- skin rash and/or stomatitis
- arthritis
- pleuritic chest pain
- renal disease
- cytopenia
what autoantibodies are seen in SLE
ANA
anti ds-DNA
anti-Sm
anti-Ro - neonatal lupus
anti-phospholipid antibodies
anti-cardiolipin, lupus anticoagulant
what is systemic sclerosis
Rare disorder characterized by diffuse fibrosis and of skin and internal organs. Caused by immune damage to endothelial cells which causes inflammation followed by fibrosis.
aetiology of systemic sclerosis
environment - silica, solvents, viral infections
genetics
pathogenesis of systemic sclerosis
vascular damage
immune system activation and inflammation
fibrosis
which scleroderma has better prognosis
localised scleroderma
-patches of thick sclerosed skin (morphia)
-linear scleroderma - bands of fibrous tissue
subsets of systemic sclerosis
limited - anti-centromere antibodies, pulmonary HTN and GI
diffuse - anti Scl70 antibodies, pulmonary fibrosis, renal crisis and small bowel bacterial overgrowth
limited cutaneous slceroderma - CREST
C - calcinosis: Calcium deposits forming under the skin
R - raynaud’s Phenomenon: Blood vessels in fingers/toes spasm, turning them white or blue in response to cold or stress.
E - esophageal Dysfunction: Acid reflux and difficulty swallowing due to muscle dysfunction.
S - sclerodactyly: Skin thickening and tightening on the fingers, making them stiff.
T - telangiectasia: Small red spots (dilated blood vessels) on the face, hands, chest
how does Sjrogens syndrome present
dry eyes and mouth
salivary gland biopsy
parotid enlargement
systemic upset
- fatigue, fever, myalgia, arthralgia, dry skin
what antibodies are associated with Sjrogens syndrome
anti-Ro and anti-La
complications of sjrogens syndrome
uLymphoma
uNeuropathy
uCutaneous vasculitis
uInterstitial lung disease
uRenal tubular acidosis
what are the autoimmune myositis'
polymyositis and dermatomyositis
myositis
what is there an increased risk of in polymyositis and dermatomyositis
increased risk of malignancy
so always screen for cancer
how does myositis present
muscle weakness - symmetrical and proximal
raised creatinine kinase
EMG, MRI and muscle biopsy
interstitial lung disease - anti Jo1 antibodies
cutaneous - Gotrons papules, Heliotrope rash
what are the overlap syndromes
mixed connective tissue disease
Raynauds
soft tissue swelling/sclerodactylyl
myositis
arthralgia
what are vasculitides
Group of vascular disorders that cause inflammatory injury.
classification criteria for GCA
any 3 of: -
- age of onset >50
- new headache
- temporal artery tenderness/ reduced pulsation
- ESR >50
- abnormal temporal biopsy
investigations for giant cell arteritis
temporal artery biopsy
ultrasound doppler - within 5 days
CT angio, MR angio
FDG PET - aortic involvement
complications of GCA
irreversible visual loss
aortic aneurysm
arterial stenosis and limb ischaemia
stroke
treatment of GCA
prednisolone 40-60mg per day - gradually tapered + PPI and bone protection
-steroid sparing medication used to reduce long-term steroid dependence
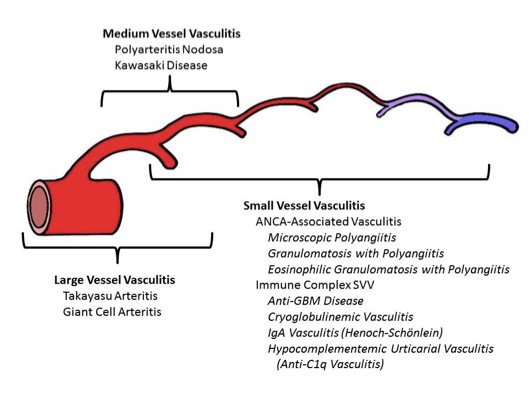
what are the types of ANCA associated vasculitis
granulomatosis with polyangitis
microscopic polyangitis
eosinophilic granulomatosis with polyangitis
what is granulomatosis with polyangitis
necrotising granulomatosis inflammation
usually involving upper and lower respiratory tract
hearing loss, sinusitis and haemoptysis
what antibodies are involved with granulomatosis with polyangitis
cANCA, anti-PR3 antibodies
what glomerulonephritis is associated with granulomatosis with polyangitis
necrotising glomerulonephritis
what is microscopic polyangitis
necrotising vasculitis with few or no immune deposits, mainly affecting small vessels
granulomatous inflammation is absent
-renal and pulmonary involvement
antibodies associated with microscopic polyangitis
pANCA, anti-MPO antibodies
what is eosinophilic granulomatosis with polyangitis
eosinophil rich necrotising granulomatosis inflammation often involving respiratory tract
late onset asthma, nasal polyps, eosinophilia
- small to mediums vessels
neurological involvement
cardiac and GI involvement
presentation of eosinophilic granulomatosis with polyangitis
late onset asthma
nasal polyps
eosinophilia
necrotising vasculitis
neuro involvement
cardiac and GI give poor prognosis
MPO antibodies +ve
treatment options for foot and ankle conditions
analgesia
shoe wear modification and activity modification
weight loss
physio
orthotics
surgery - last resort
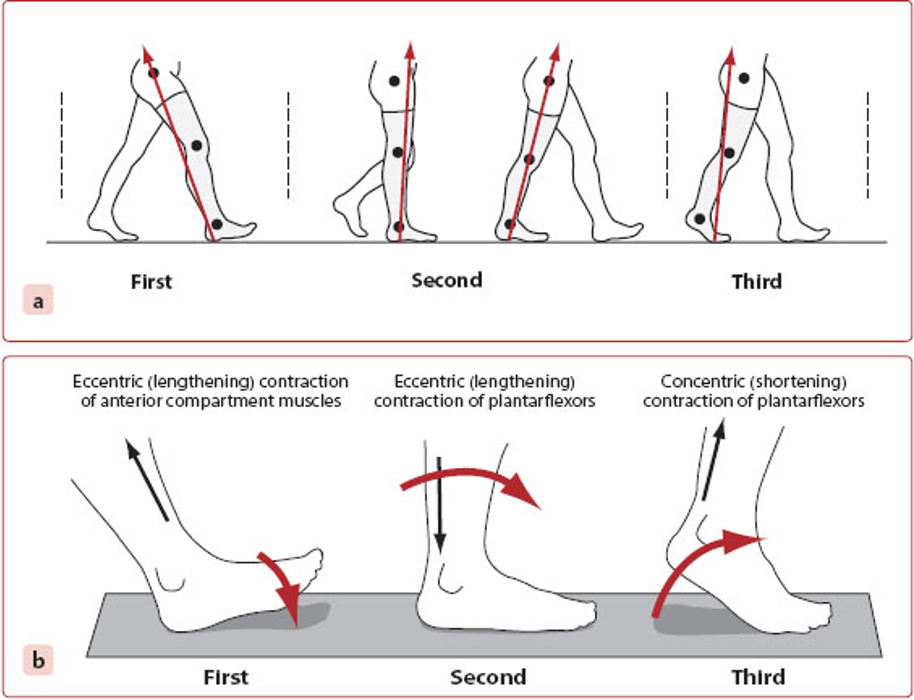
first, second and third of gait
first - eccentric (lengthening) contraction of anterior compartment muscles
second - eccentric (lengthening) contraction of plantar flexors
third - concentric (shortening) contraction of plantarflexors