EXAM 4 CHRONIC
1/23
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
24 Terms
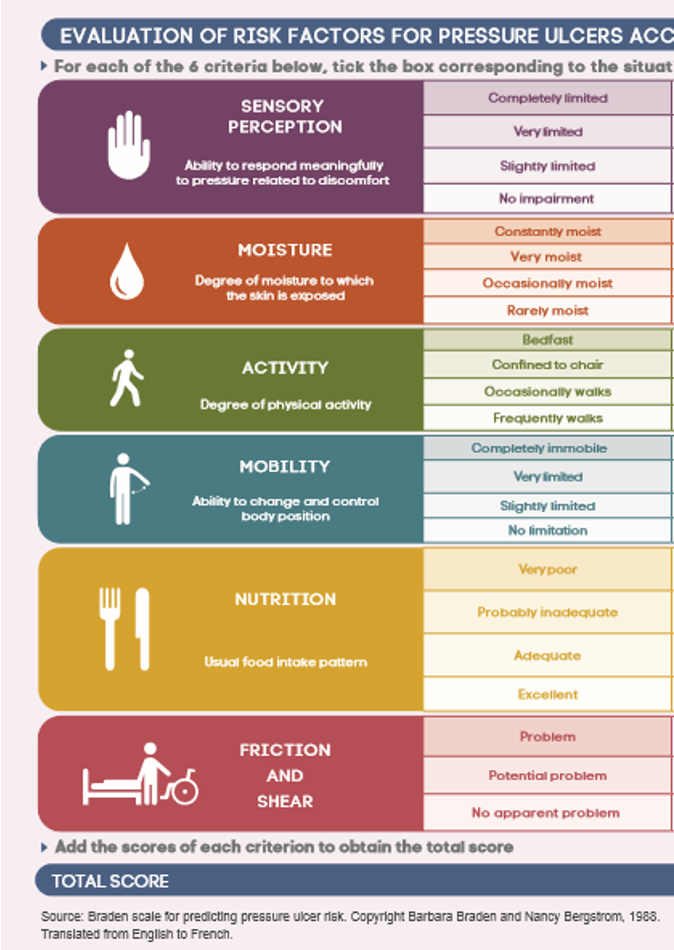
Braden scale
Assess risk for pressure injury:
sensory perception
moisture (ex. due to incontinence)
activity/mobility
nutrition
friction/shear
Score: 6-23
<18 → at risk MUST implement preventative measures
Psoriasis
Immune disorder causing chronic inflamm of skin
skin cell produc. > shedding → epidermal thickness
Signs: occur anywhere → elbows, knees, palms, soles, scalp
thick, raised red patches w/ silvery flaking scales
painful & itchy
Lab: based on signs
elevated CRP & ESR (serum inflamm markers)
Tx: no cure
topicals/ointments (corticosteroid, retinoids), uv light therapy (kills cells), methotrexate
Care:
pt are better in warmer climate → uv kills cells

Skin cancer
Cause: uv radiation
Types:
(#1) basal cell carcinoma → usually tx b/c localized
melanoma → harder to tx
Labs: changes in skin (size, color, sensation)
Tx: chemo, radiation
Care:
limit sun exposure (spf 30, hats/long sleeve)
monthly self exams
Burn injuries types
1) Superficial (sunburn)
affect only epidermal
signs: mild erythema/hypersensitivity
tx: resolves in 24-72 hrs (no meds necess.)
2) superficial partial thickness
affect epidermis & superficial
signs: very painful b/c exposed nerve endings, wet weeping pink blisters, cap refill normal
tx: heals in 1-2 wks
3) deep partial thickness
affect epidermis & extend into deeper portions
signs: appear waxy (no weepy blister), pink/cherry red, vary pain, NO cap refill
4) full thickness
affect epidermis, dermis, subcut tissue, maybe muscle/bone
destroy hair follicles, sweat gland, nerve ending → poor temp control & no pain
tx: skin graft
Burn injuries
Risk: pt age & medical hx
Effects: burn shock & fluid/electrolyte imbalance secondary to massive fluid shifts
fluids/electro leak out of intravascular space into interstitial b/c increased cap perm.
initial: hyerK
late: hypoK & hypoN
Burn injury stages
1) emergent
goal: resolve immediate life threat → baseline eval, airway, fluids, prevent hypothermia, initiate wound care
care: 100% humidified o2, place large bore iv cath (fluid resus), warming measures (ex. blanket)
2) immediate (after resus & stabilize 48-72hr later)
goal: wound healing & closure, optimal nut., prevent infection & pain
care: assess labs (protein, wbc, albumin), wound care, nut. (maybe feeding tube)
3) rehab (may last for years)
goal: rehab & pyschological support
care: community resources, teach pt how to apply pressure garment (prevents hypertrophic scarring)
pt w/ burn may lack sweat gland & skin graft is sensitive to light
increased metabolic rate & caloric need post burn
HIV
Virus that attacks body’s immune system
targets CD4+ lymphocytes → integrate rna into host cell dna through reverse transcriptase
Cause: STI (#1), blood, breast milk
fluid MUST come in contact w/ mucous membrane/injected into bloodstream
Lab: annual screening
viral load & cd4 count to establish baseline
Tx: no cure → proper managment
antiretroviral therapy (ART)
w/o proper tx → AIDS develops
Care:
avoid food that irritate bowel (raw fruit/veg, carbonated)
may need enteral/parenteral nut.
avoid high risk (use condom, reduce partners, no share needles)
hygiene → hand wash, avoid crowds
Stages of HIV
Stage 1: acute
develop 2-4 post exposure → very contagious
hiv rapidly spread → increase viral load → body can still control the virus → CD4 return to normal levels (500 cells/mm3)
signs: temporary flu like symp (fever, chills)
Stage 2: chronic
prolonged → last several decades w/ tx or a decade w/o
low CD4 → 200-499
sign: asymp but STILL contagious
nonspecific sign → resp. tract infection, enlarged lymph
Stage 3: aids
CD4: <200 = aids
HIV tx
Antiretroviral therapy (ART)
interfere w/ ability of hiv to reproduc. & suppress virus
use: confirmed case, pre/post exposure prophylaxis
uses multiple agents & adherence is required
atleast 95% adherence for tx to be effective
eval renal & hepatic
Pneumonia
Inflamm of lung parenchyma from infection
Signs: pleuritic chest pain, cough, fever
Lab: chest x-ray
elevated wbc, crp, positive sputum
starts as resp. alka → later: resp. acid
Tx:
bronchodilator: albuterol or combivent → open airway
antibiotic → broad then specific
Care:
SaO2 >92%
position: good lung down, hob 30
TB
Resp. infection caused by mycobacterium tuberculosis
spread via aerosolized droplet (NOT direct contact) → airborne precaut.
Types:
latent → asymp. & NOT contagious
active → abnormal chest x-ray/sputum
Signs: hemoptysis (coughing blood), weight loss, night sweat
Lab: tuberculin skin test (mantoux test) → assess induration (size/firm)
Tx: 3-9 months
2 phases: intensive → continuation
Asthma
Intermittent, reversible airway obstruction from inflamm → increase mucus, bronchospasm
Signs: wheezing, dyspnea, coughing, increased sputum/RR, tachy
Lab: spirometry, chest x-ray, abg
Tx: anti-inflamm (inhaled corticosteroid), bronchodilator
Care:
maintain o2 >90%
teach action plan, pursed lip, peak flow meter
Laryngeal cancer
Originate from squamous cells that line larynx/hypopharynx/ esophagus entry → slow develop
Risk: (#1) tabacco & alcohol
Signs: change in voice (lower, raspy, >2 wks), persistent sore throat, ear pain
Lab: laryngoscopy, barium swallow
Tx: radiation, chemo, surgery
Care: post op
trach care/suction, pulmonary hygiene (deep breath), nut., emergency equip at bedside
Hypertension
BP that is above normal “silent killer”
Types:
primary (#1) → multifactorial, chronic
secondary → caused by underlying, acute
Signs: increase bp
late → headache, chest pain, sob, vision change
Lab: >2 bp reading at SEPARATE times
Tx: slowly & cautious
start w/ 1-2 med (LOW doses) → diuretic, beta block, ½ dose for older
HTN complications
Hypertensive crisis
hypertensive urgency → bp very high but no sign of organ damage
hypertensive emergency → bp >180/120 + possible damage
Coronary artery disease (CAD)
Obstruct/dysfunc of blood vessels that deliver o2 rich blood to heart muscles → ↓ perfusion of myocardial tissue
Cause: atherosclerosis (harden/narrow of arteries b/c plaque)
Risk: elevated serum lipids
cholesterol >200, trig. >150
Sign: asymp until 40% block → angina
Lab: lipid profile
Tx: surgery (ex. stent)
aspirin (stop aggregate)
nitroglyercin (relief) → every 5 min x3
Care: bleeding precaut.
diet: decrease saturated fat (meat, whole milk), increase complex carb (whole grain)
Peripheral artery disease (PAD)
Narrow/block of vessels that carry blood from heart to upper/lower extremities → deprive o2 → ischemia, necrosis
Cause: atherosclerosis
Signs: intermittent claudication (#1) → muscle pain b/c lactic acid buildup, foot pain worse w/ elevation, coolness, thin shiny skin
Lab: vascular assessment (palp, auscul, inspect), ABI
Tx: meds, angioplasty
Complications: nonhealing ulcers + gangrene → may need amputation
Venous thrombus
Blood clot in vein → potential to break off (thromboembolism)
Signs: Virchow’s triad
stasis, endothelial injury, hyercoag.
Sign: swell, tender, redness, warmth
Lab: duplex ultrasound (confirm), D-dimer (+ test)
Tx: heparin or enoxa. (for active clot only) → transition to long term oral anticoag (warfarin (INR 2-3))
Care: watch out for bleed (bruise, petechiae, hematuria)
Venous insufficiency
Occurs when leg veins do not allow blood flow back to heart → blood flow backward & pools in leg
Sign: “heavy pain”, skin change (brown), varicose vein, venous stasis ulcer (ankles/calves)
twisted, enlarged vein
Tx: surgery
sclerotherapy, vein ligation & stripping
HF
Progressive disease characterized by myocardial cell dyfunc. & muscle weakening
Sign: fatigue, weight gain, tachy
left side: sob, crackles, fatigue, cool/weak
right: JVD, hepatomegaly, ascites, edema
Types:
HFrEF → inability to pump forward “weak pump”
EF <45%
HFpEF → unable to relax & fill “stiff, improper fill”
EF >45% but low CO
Lab: ecg
troponin, BNP/NT-proBNP (released in response to high bp/fluid)
Tx: diuretic, ACE inhibitor (#1), beta block
Cancer
Uncontrolled growth of malignant cells that compromise normal cells
Risk: exposure to carcinogen → cellular mutation
Types:
solid tumor → arise from specific organ (ex. lung)
hematological → from cells (ex. leukemia)
Staging: TNM (tumor size, spread to lymph, metastasis)
Sign: CAUTION
Lab: biopsy
Tx: radiation, chemo, bone marrow transplant
End of life
Pt goals guide treatment
Signs: dyspnea, anorexia, delirium, depression
late → gurgling, terminal bubbling
Care:
suctioning, position (lateral w/ elevated head), antimuscinaric/anticholinergic to dry up secretions
Anemia
Reduction in o2 carrying capacity b/c less rbc or reduction in hemoglobin
Causes: blood loss, inadequate rbc produc, increased rbc destruct., deficiency
Types:
iron defic. (#1) → insuff. hemoglobin to carry o2
sign: hypoxia, pallor, fatigue
lab: low serum ferritin, low H&H
tx: red meat, dark leafy, dried beans, fortified cereal/bread (take w/ vit C)
vit b12 → need for func. of CNS, formation of rbc, dna reg.
sign: cns changes → spinal cord degen, altered mental
lab: b12 assay
tx: animal protein → meat, seafood, egg, dairy
folic acid → need for formation of heme for rbc mature
sign: pallor, tachy, dizzy
lab: cbc
tx: fortification of cereal/grains → supplements for preg.
sickle cell → cause hemoglobin to be sticky → block blood flow → hypoxic
sign: vassooclusion → pain swell
tx: o2 therapy, avoid cold
Polycythemia vera
Disorder of bone marrow → makes blood more viscous (thick) → slow circulation & o2 exchange
increase in volume of rbc BUT still hypoxic
Cause: JAK2 gene
Sign: takes years for symp → sob, headache, risk for clot
Lab: routine blood test
Tx: therapeutic phlebotomy (remove blood)
Care:
hydration (3L/day), elevate legs