Dental disease
1/34
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
35 Terms
what can we advise owners to prevent plaque build up?
brush teeth = gold standard
dental diet
regular dental cleaning/polishing
chewing toys
reduce treats
how does osteoclast formation occur?
cytokines trigger stem cells to be attracted to the gingiva → differentiation into osteoclasts
why is osteoclastogenesis is important in periodontal disease?
causes bone resorption and this weakens teeth → increased chances of damage and ideal environment for infection
what are the stages of periodontal disease?
0-4
what is stage 0 periodontal disease?
healthy periodontal tissue, no issues present, no disease
what is stage 1 periodontal disease?
gingivitis only and no attachment loss
what is stage 2 periodontal disease?
gingivitis is present with ,25% alveolar attachment loss
may be early radiographic signs of periodontitis and attachment loss
what is stage 3 periodontal disease?
gingivitis + 20-50% alveolar attachment loss
increased probing depth or radiographic determination of the loss of attachment
stage 2 furcation involvement in multirooted teeth
what is stage 4 periodontal disease?
gingivitis + >50% attachment loss
measured by increased probing depth/radiographic evidence or stage 3 furcation involvement
what is gingivitis generally caused by?
dental plaque accumulation - indicates poor oral hygiene - not for certain that there’s assosicated disease
what are two types of periodontitis?
active - loss of attachment + gingivitis
quiescent - loss of attachment but no inflammation/severe inflammation
key clinical signs of periodontal disease?
halitosis
plaque and calculus
gingivitis
gingival recession
periodontal pocketing
bone loss
furcation exposure
mobile teeth and loss of teeth
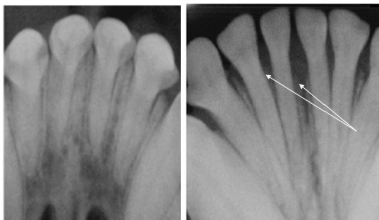
Compare the right radiograph to the left
right radiograph = alveolar bone resorption
due to periodontal disease
what is FORL?
feline odontoclastic resorptive lesions
what is the aetiology of FORL?
loss of outer, protective blast-cell layer of root
persistant stimulus → root absorption-repair pattern
what are potential causes of FORL
inflammation due to periodontal disease
abfraction - microfracture due to mechanical loading causing bacterial resorption
commercial pet food
vit D levels
what is the pathophysiology of FORL?
abnormal teeth remodelling by odontoclasts starting in cementum
type 1 lesions affecting cervical region, type 2 affecting apical root
cementum and dentine resorbed → enamel resorption and lacunae develop int he crown
weakened teeth → increased fracture risk
what are the 3 types of lesion in FORL?
inflammatory - apple core lesions radiographically
replacement resorption → periodontal ligament loss → ‘ghost roots’ on radiograph
type 1 and 2 lesions simultaneously
what areas are most commonly affected by FORL?
notably lower third premolars
canines
upper fourth premolars
sites of poor hygiene and inflammation
with FORL, is only one side of the mouth affected?
no, it’s bilaterally symmetrical
how do we diagnose FORL?
oral examination
radiography
what are our differentials for FORL?
periodontal disease
dental cavities
gingival hyperplasia
traumatic fracture
How do we treat FORL?
extraction of all teeth with any stages present
coronal amputation for advanced stage 2/3 with ghost roots radiographically
what do we need to do post op for FORL?
post op check at 1 and 3 weeks
routine dental and oral checks every 3 months