osmoregulation in kidney
1/14
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
15 Terms
what are the 2 functions of the kidney?
remove urea from blood (ultrafiltration + selective reabsorption), osmoregulation
why is osmoregulation important?
if blood too dilute, tissue cells absorb water by osmosis and lyse. also high BP causes capillary damage
if blood too concentrate, water drawn out of tissue cells by osmosis, slows cell metabolism. BP too low, heart can’t pump blood into tissues
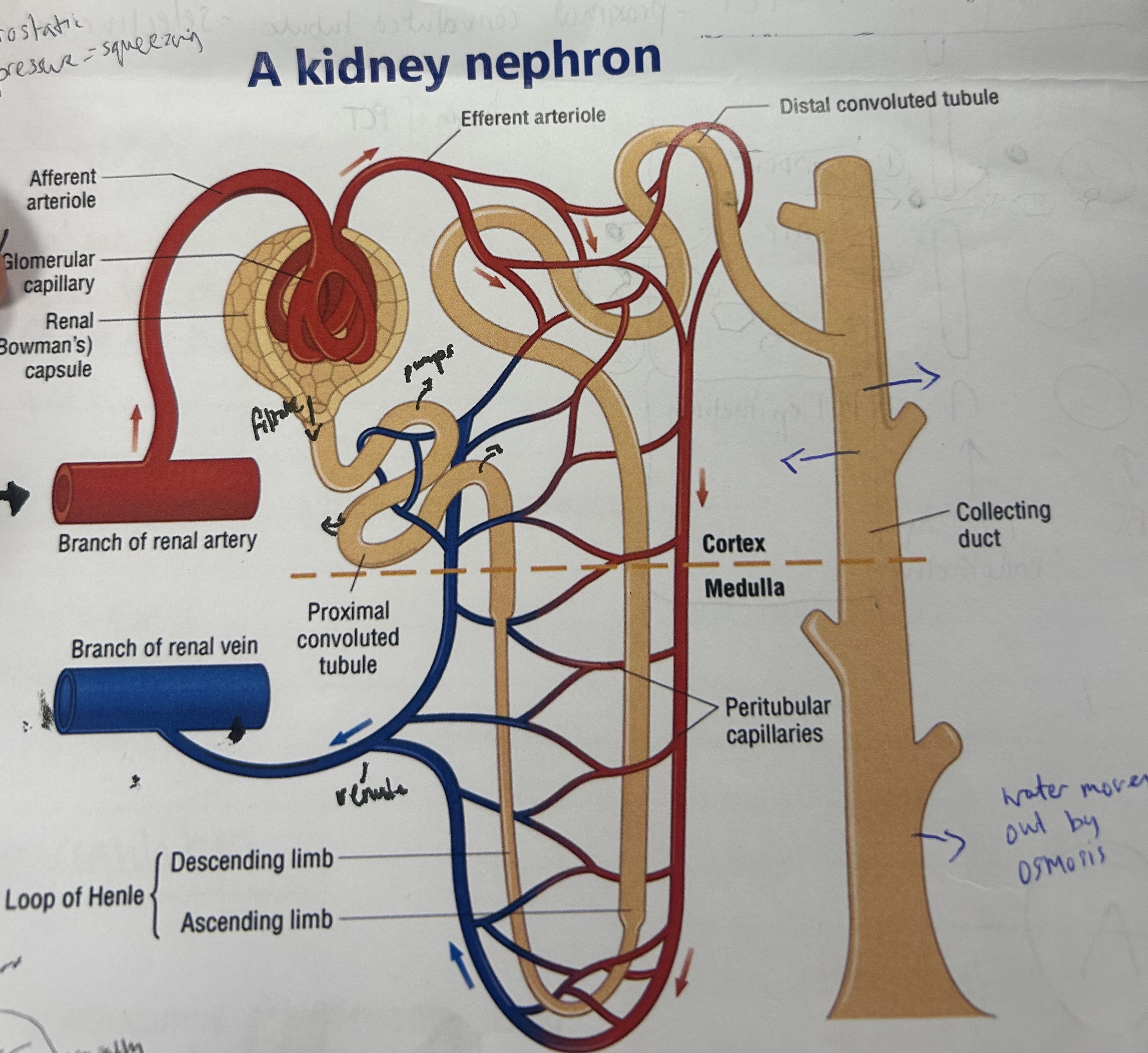
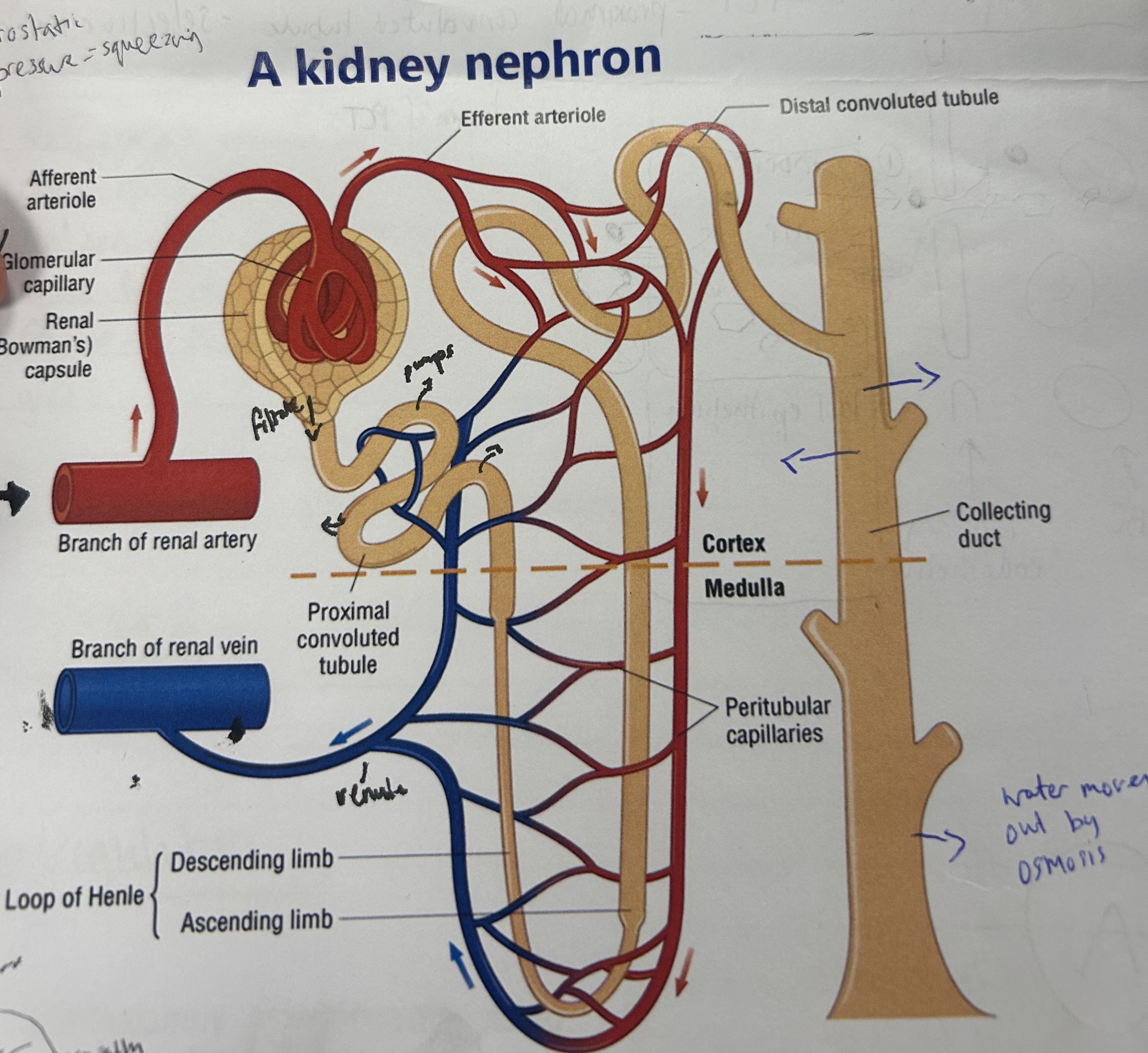
what creates the blood pressure required for ultrafiltration?
affluent arteriole wider than effluent arteriole causes bottle neck and therefore high BP
which substances are in the filtrate forced out of the blood by ultrafiltration?
water, urea, mineral ions, amino acids, glucose
what are the 2 parts of the filtration of urea? (1st function of kidney)
ultrafiltration, selective reabsorption
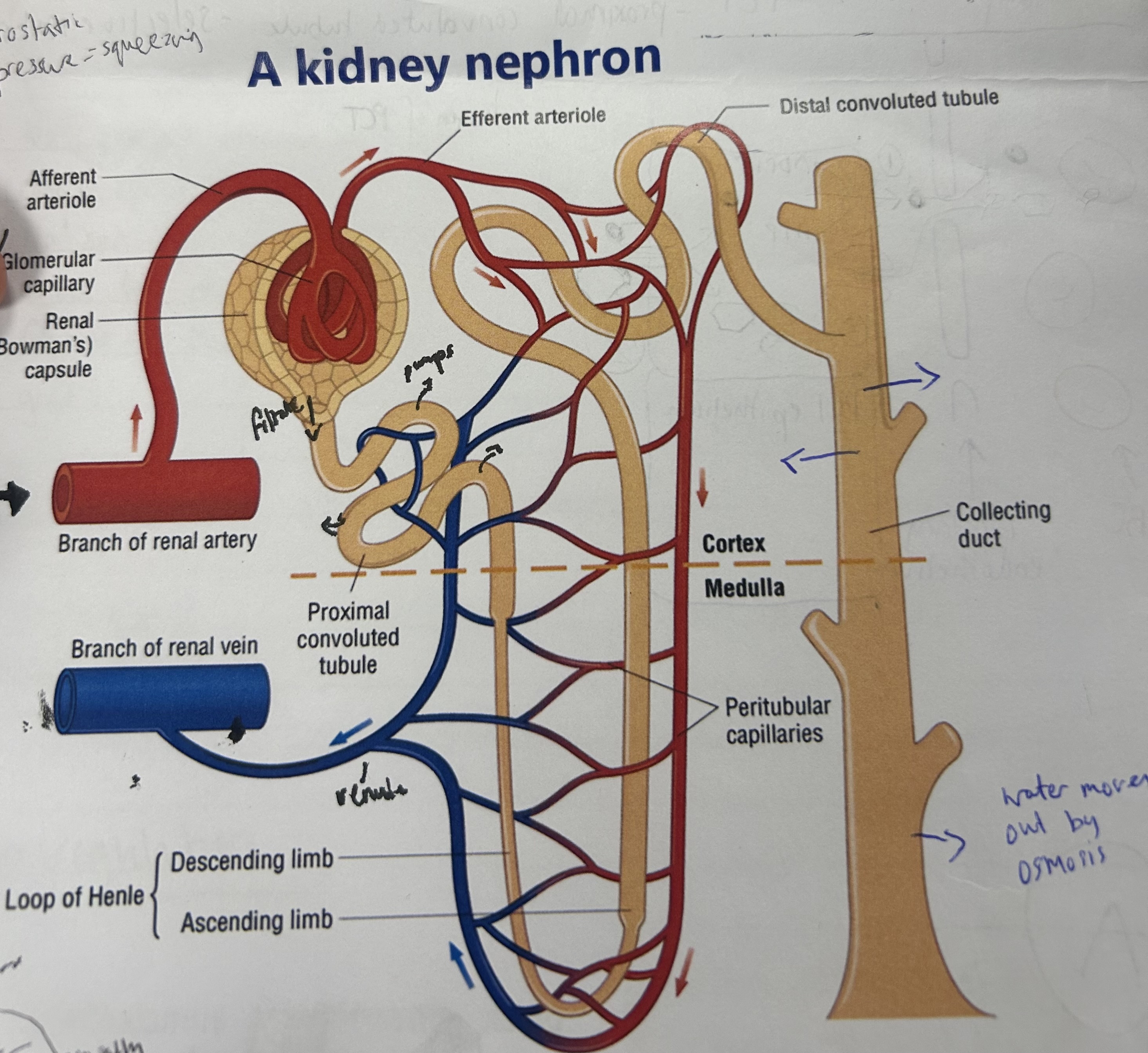
explain the process of ultrafiltration (1st stage of removing urea from blood)
blood enters through afferent arteriole, splits into smaller capillaries in glomerulus
causes high hydrostatic pressure of blood
water and small molecules incl glucose/mineral ions forced out of capillaries for glomeruls filtrate
large protein/blood cells too big to fit through gaps in capillary endothelium, so stay in blood
blood leaves via efferent arteriole
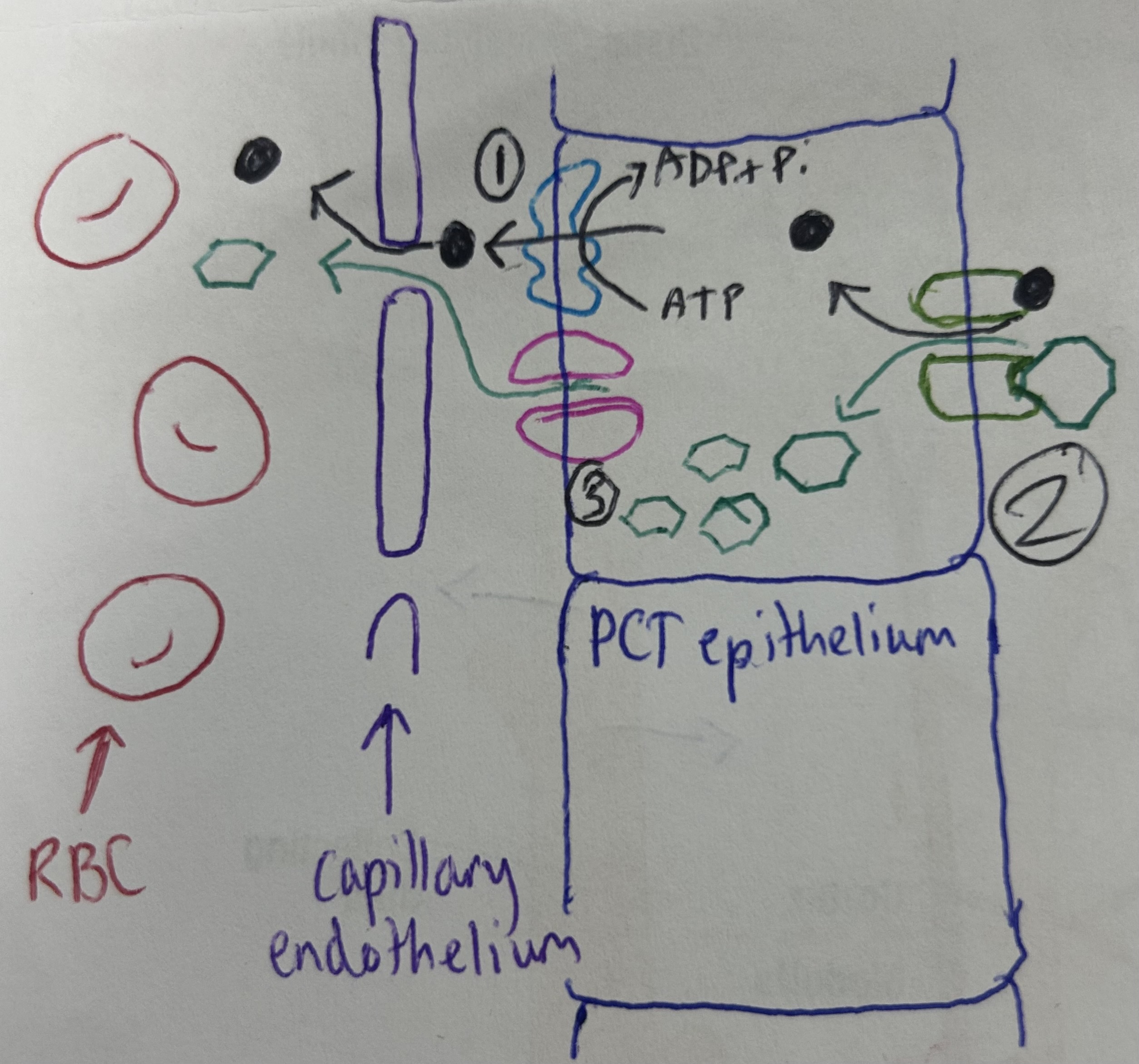
explain selective reabsorption (2nd part of filtration of urea), AKA cotransport in the PCT
Na+ pumped out of PCT epithelial cell by active transport, reduces Na+ conc in epithelial cell
Na+ and glucose/amino acids bind to cotransport carrier protein, which opens, allowing them into cell down Na+ conc grad
Glucose conc builds up in epithelial cell and diffuses out into blood down conc grad
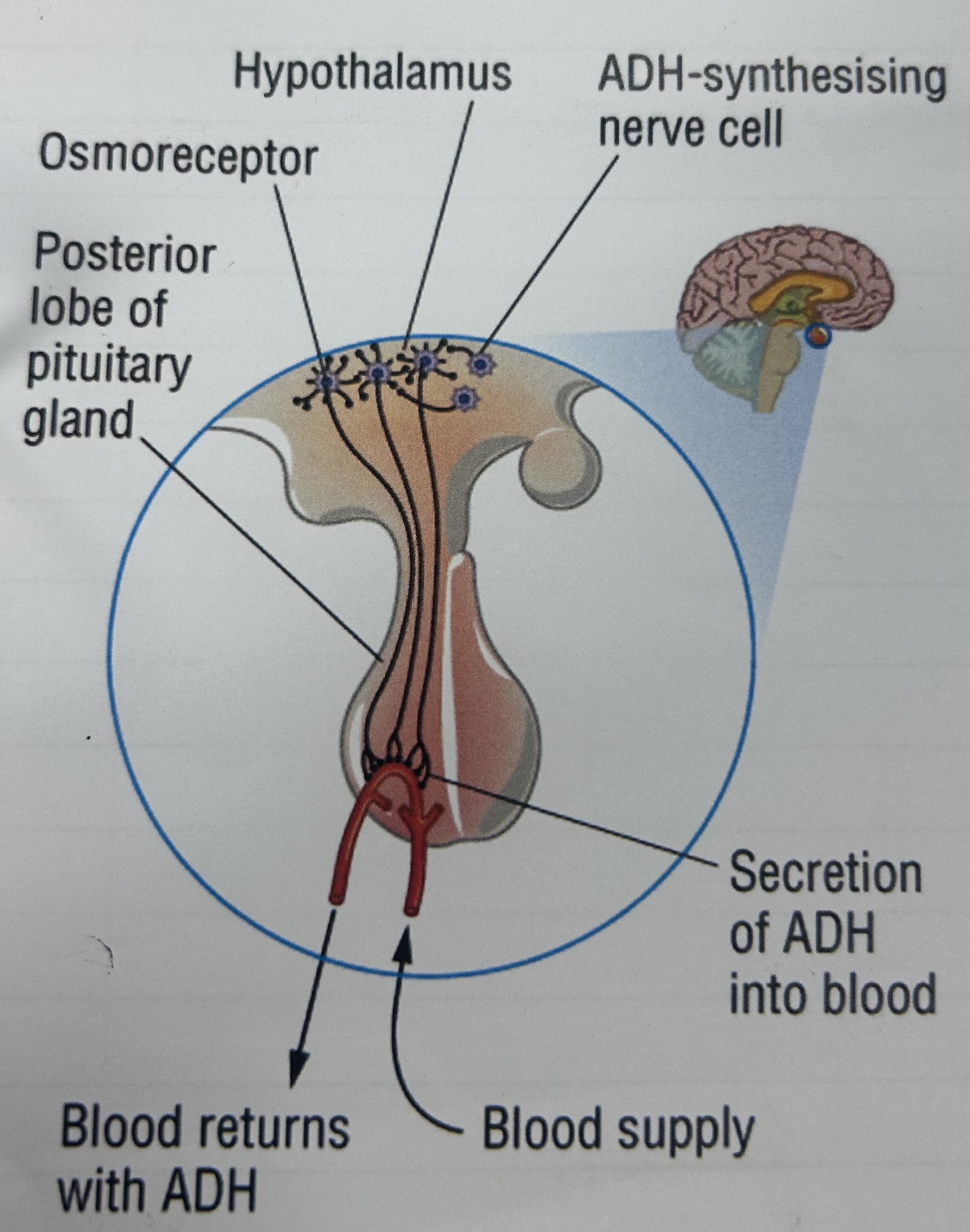
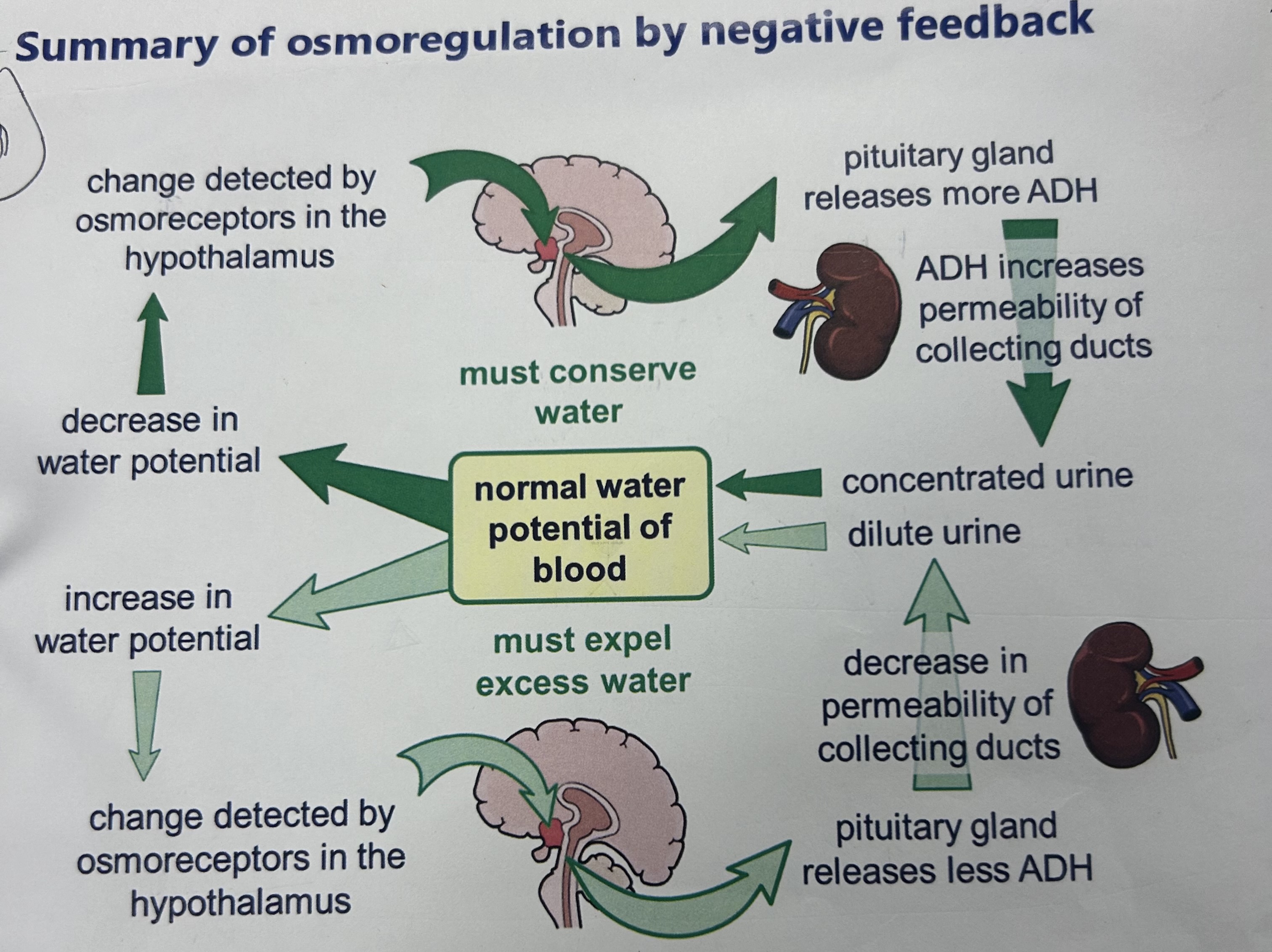
the water potential of blood is constantly measured by what?
osmoreceptors in hypothalamus
if dehydrated, how does the blood water potential return to normal?
low water conc in blood detected by osmoreceptors in hypothalamus
pituitary gland releases ADH
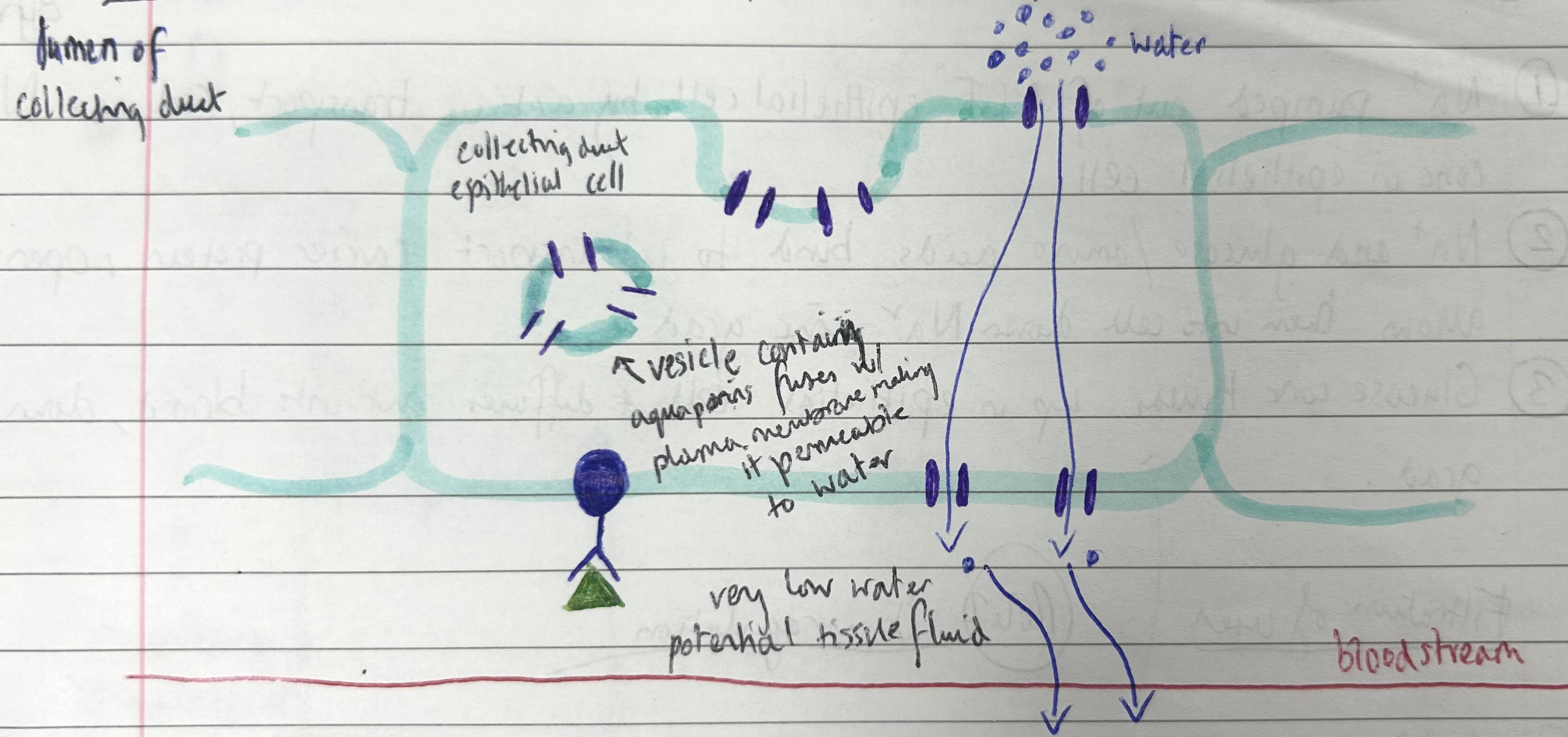
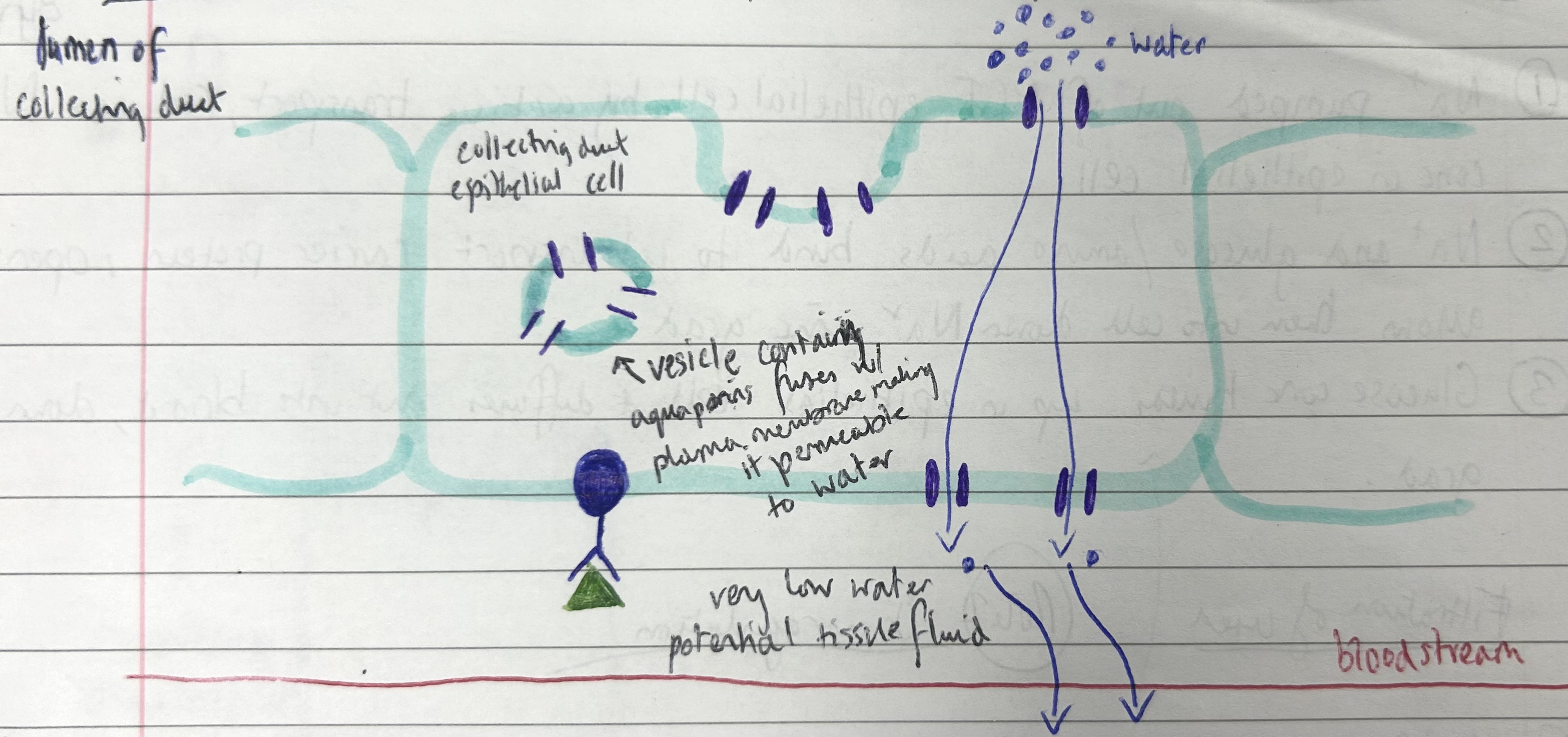
collecting duct epithelial cells detect ADH, aquaporin vesicles move towards and fuse w plasma membrane
makes collecting duct walls permeable to water, water osmoses from CD lumen through epithelium to tissue fluid (due to low WP in tissue fluid) and into blood
small amounts of concentrated urine produced
increases blood water conc to normal
if overhydrated, how does the blood water potential return to normal?
high water conc in blood detected by hypothalamus
pituitary gland releases less ADH
aquaporins remain in vesicles in collecting duct epithelial cells, so collecting duct less permeable to water
water remains in collecting duct, large quantities of dilute urine produced
reduces water conc in blood to normal
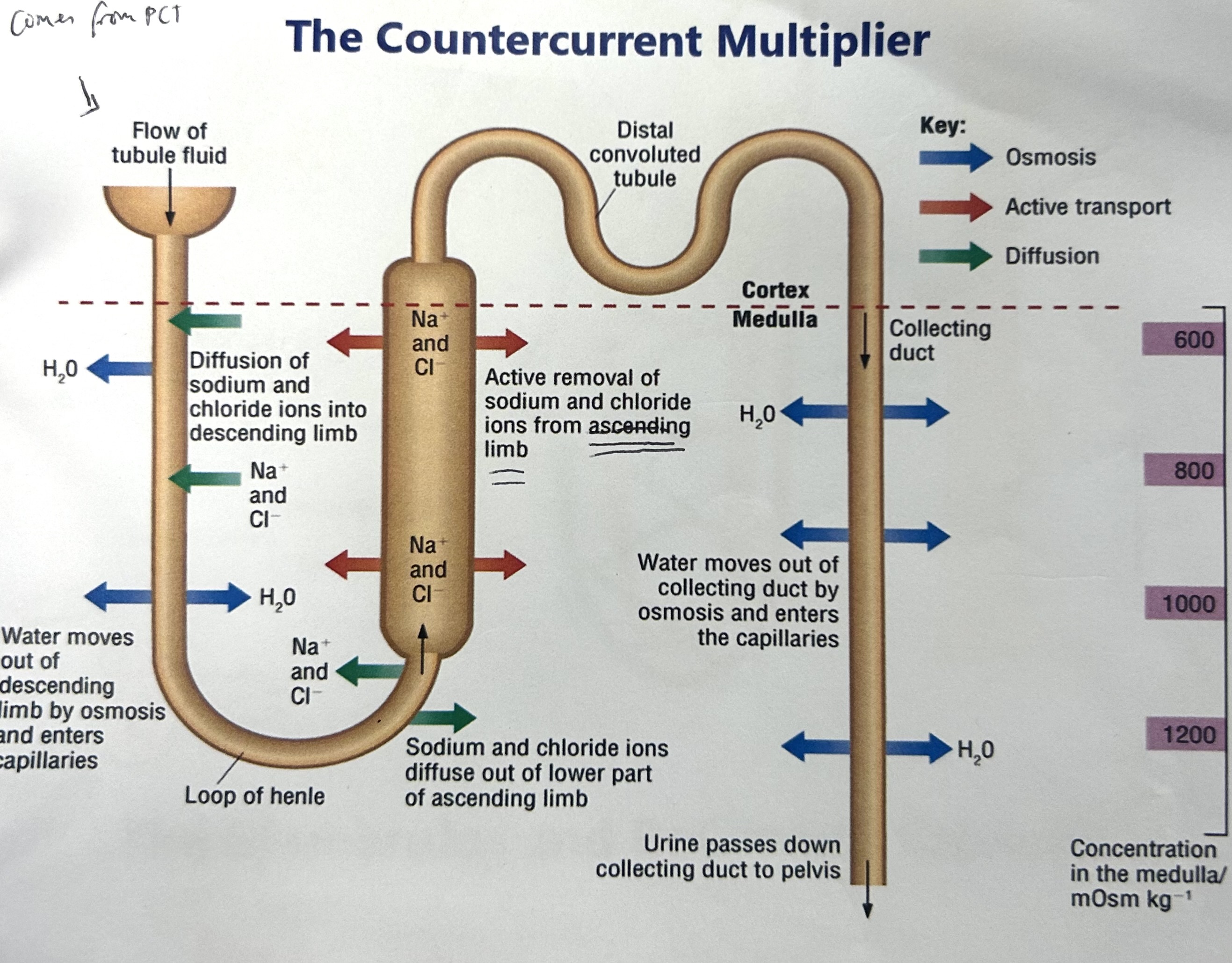
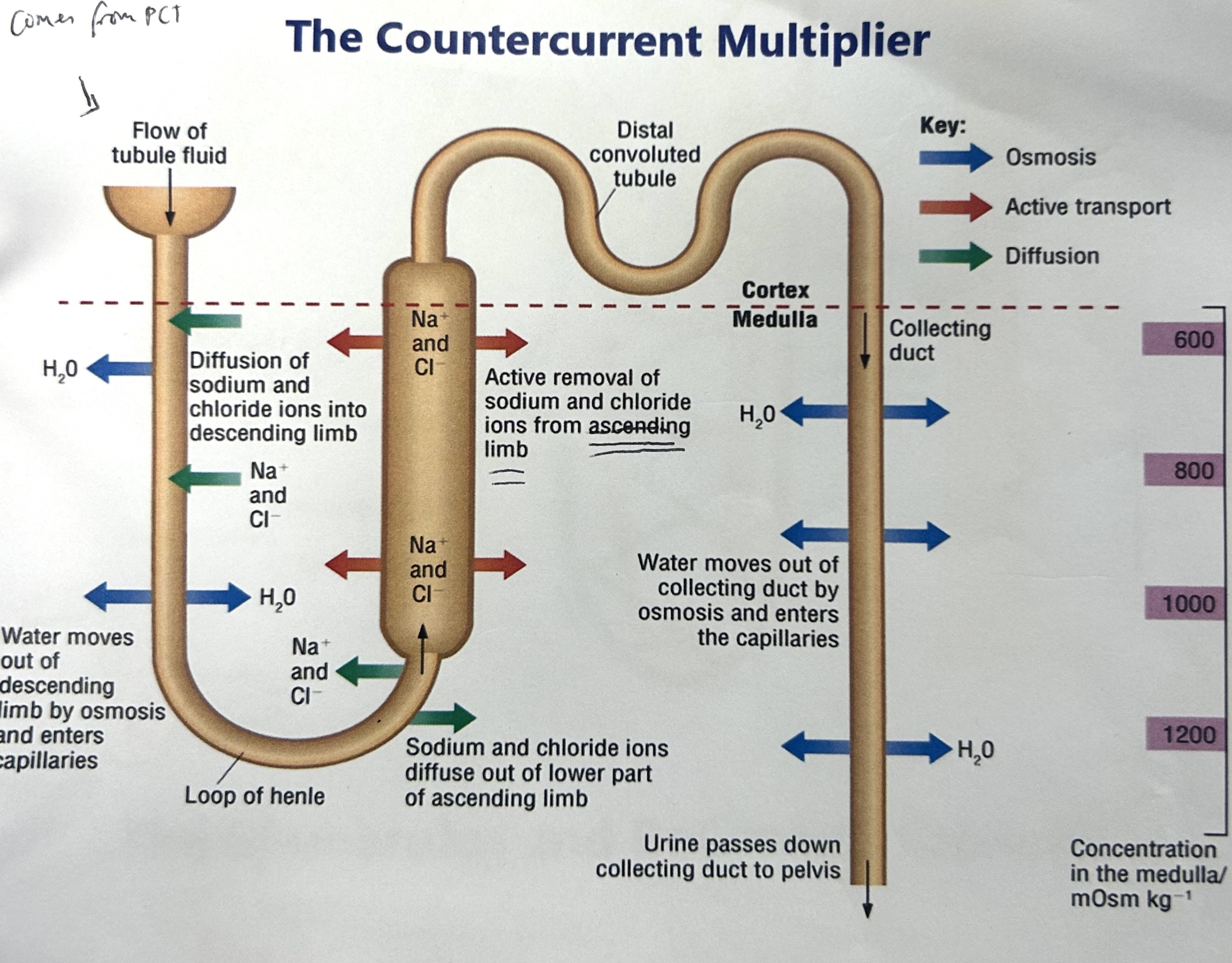
explain how the countercurrent multiplier works (osmoregulation- how salt is controlled)
Na+ pumped out of ascending limb of loop of henle by active transport
Na+ conc higher at start of ascending limb, decreases as go up, more active transport at the start
The Na+ that was actively transported out of ascending limb diffuses back into descending limb
This active transport and diffusion causes Na+ ions to be concentrated in lower regions of medulla, creates salt gradient for water reabsorption in collecting duct
what would be the result if there was a problem with the ascending / descending limb
no salt concentration down, lose water as no lower water potential the further down the medulla
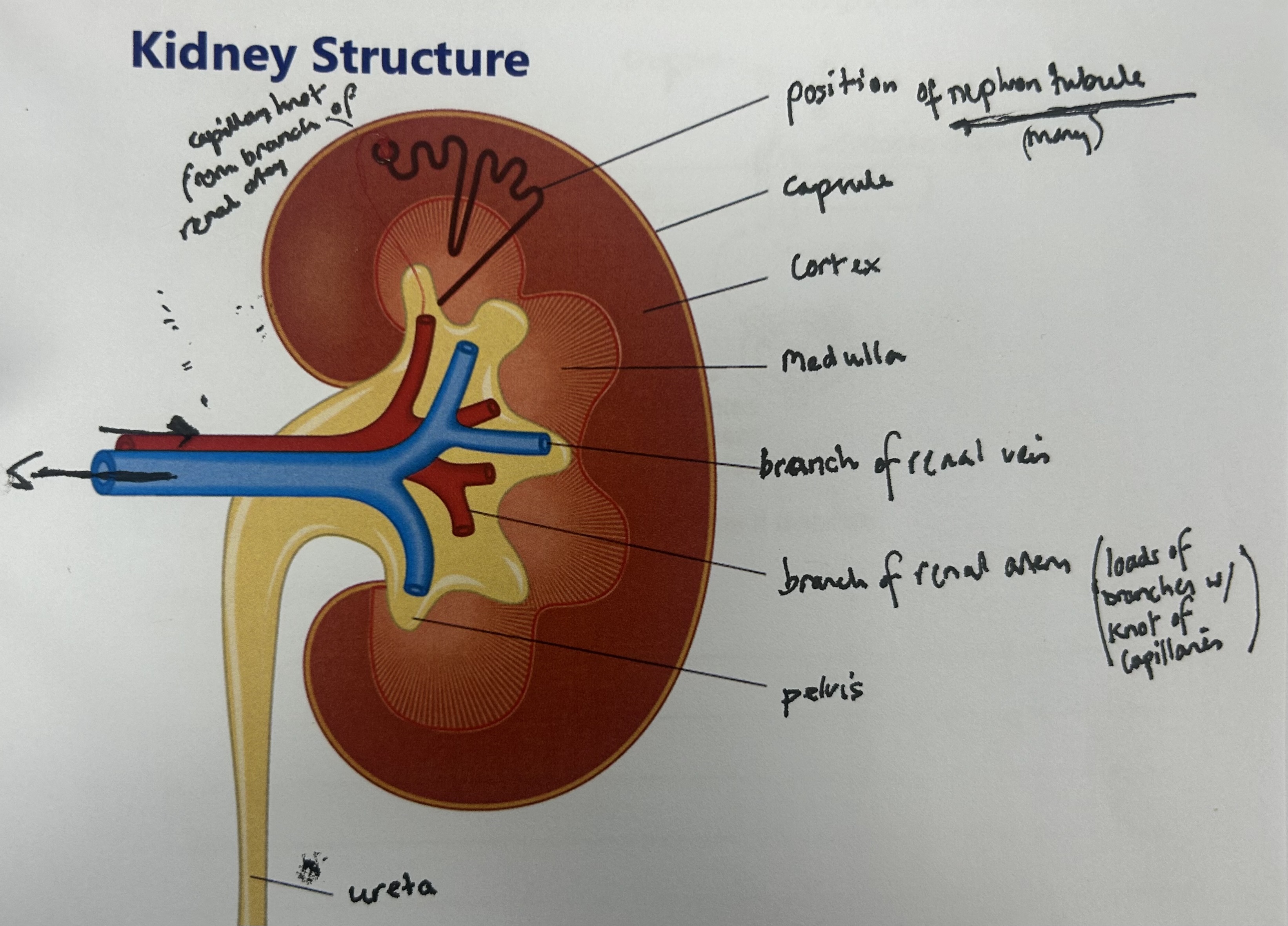
what does the renal artery do?
carries oxygenated blood from heart to kidneys
what does the renal vein do?
carries deoxygenated filtered blood from kidneys to heart
2 adaptation of PCT
microvilli- large SA for reabsorption
lots of mitochondria- provide energy for active transport