blood gas transport and regulation
1/21
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
22 Terms
why do we need O2 3
O2 in bloodstream diffuses to mitochondria of all cells where it is needed for the production of ATP via oxidative phosphorylation
ATP is energy currency, no storage so is needed in continuous supply
Catabolism of macromolecules yields FADH + NADH which are oxidised by protein complexes in the mitochondria inner membrane
what 2 things do redox reactions produce
E,E
Electrons
They are transported along the protein complexes until they react with O2 and H+ in the matrix to generate H2O
Without O2 as the final electron acceptor, electron flow would stop
Energy
Redox reaction generates a small amount of energy allowing H+ to be pumped into the mitochondria inter-membrane space
The H+ gradient created across the inner membrane, powers ATP synthase -> generates large amts of ATP
alveolar partial pressure
pCO2, O2, air
how much O2 is dissolved in plasma
pO2 - 100mmHg
pCO2 - 40mmHg
pAir - 760mmHg
15mL O2/min (henry’s law/ dissolved O2 in plasma = alveolar pO2xO2 solubility) - insufficient to meet body’s needs
protein bound O2
how much O2 is transported bound to Hb
what is the graph shape of O2-Hb dissociation curve, why
what is in each Hb molecule 4×2
what is the role of Hb 2
what are the two conformations T,R (what is the affinity for O2 in each)
98%
The sigmoidal shape of the oxygen-haemoglobin dissociation curve is due to cooperative binding of O2 to Hb
Each Hb molecule contains:
4 globin proteins: 2 alpha and beta chains
4 hemes: a Fe2+ ion bound to a porphyrin ring
Roles:
Reversible O2, CO2 transport in the blood, buffering agent
2 conformations:
Tensed (T) state has LOW affinity for O2
Relaxed (R) state has high affinity for O2
light absorbance of Hb
what is the difference between Hb and Hb-O2 light absorbance
why is this useful clinically
what conditions would affect readings
how does skin tone affect this
Hb-O2 and Hb absorb red and infrared light differently, this is compared to a standard curve
oximetry, finds clinical signs of hypoxaemia, determines spO2
CO poisoning, abnormal Hb, sickle cell
darker skinned people might have overestimated oxygen saturation
why is the Hb-O2 dissociation curve SIGMOIDAL
what state is Hb in at low pO2
what is the affinity for oxygen
as pO2 rises, what happens to the probability for O2 to bind to Hb
what happens to Hb when O2 binds
what does disrupting salt bridges do to the subunits
what does this mean for the oxygen binding sites
what happens to the Hb form and affinity as pO2 rises
what happens when Hb is saturated
T (tense) state, low affinity for O2
probability for O2 to bind Hb increases
O2 binds to a subunit and causes a conformational change in the SU
conformational change causes it to pull on non-covalent salt bridges, linking all the subunits together and change to the R (relaxed) form
O2 binding sites are more exposed and increases the affinity of Hb
T state to R state and affinity increases
max affinity for O2 but all O2 binding sites are saturated, no more O2 can bind to Hb
respiring tissues
how do they get O2 from Hb
in low pO2, Hb has a low affinity for O2
this triggers it to unload its O2
respiring tissues have low pO2 and high CO2
the bohr effect
what conditions facilitate unloading of O2 3
how does this happen
what does this effect allow
how does this appear on a graph
increase in temperature, increase in pCO2 level, reduction in pH
CO2 and H+ react with Hb causing a decrease in Hb affinity for O2
allows for increased delivery of O2 in metabolically active tissues
right side shift in Hb-O2 dissociation curve
where does CO2 come from in our bodies
what does RQ tell us, what is it
by-product of macromolecule catabolism in mitochondria, diffuses out the cell and into the blood
ratio of O2 consumed and CO2 released = respiratory quotient
tells us which macromolecule is being used as a metabolic source
what are the 3 forms CO2 can be transported as in the body + %
D, B, CC
10%
dissolved CO2
70%
bicarbonate
20%
carboamino compound
CO2 as bicarbonate
what enzyme catalyses conversion of CO2 into carbonic acid H2CO3
what happens to carbonic acid (turns into ion)
what does this ion bind to
what happens at the lungs
what is the chloride shift
carbonic anhydrase
H+ ion
binds to Hb to buffer the process
reverse: H+ dissociates and combines with bicarbonate to make carbonic acid → h2o+co2
exchange of bicarbonate HCO3- and Cl- across RBC (co2 can diffuse but hco3- needs a protein to leave and exchanged cl-, helps remain charge)
carbamino compounds
how are they formed
what is the haldene effect
why does it happen 2
CO2 combined with Hb
describes the ability of deoxygenated Hb to carry more CO2 than oxy-Hb
deoxy-Hb forms carbamino complexes more ready with CO2 (this is how it can carry CO2)
it is a better buffer than O2-Hb, of H+ ions
in the lungs
the blood has a high amount of what dissolved 2
what binds to Hb in the alveoli
what does this reduce the affinity of
CA (enzyme) works to do what
dissolved bicarbonate HCO3-, H+, CO2
O2 binds to Hb
reduced affinity for Hb for H+ and CO2 so they unbind
carbonic anhydrase helps remove co2 from lungs
respiratory centres of the brain
what type of innervation is responsible
how is rhythmic activation of resp. skeletal muscles activated
what 2 inputs modulate ventilation
where are the neurons in the respiratory centre in the brain
DRG
VRG
somatic motor
intrinsic periodic AP firing by neurons in the brainstem (central pattern generator)
sensory and voluntary
medulla
dorsal respiratory group neurons are active during normal inspiration
ventral respiratory group neurons are active during forced in/expiration
factors modulating ventilation
emotions
where in the brain does it act through
sensory inputs
3 examples
voluntary behaviour
what part of brain is involved
emotions
emotional stimuli acts through hypothalamus
sensory input
pain, temp acts through hypothalamus
voluntary behaviour
cerebral cortex
what are the two types of chemoreceptors
central and peripheral
central chemoreceptors
what are they
where are they located
why can they only respond to CO2
where is carbonic anhydrase and what does it do
how does reduced pH of CSF directly activate central chemoreceptors
specialised cells that monitor arterial blood gases (PaO2 and PaCO2) and pH levels
In the medulla oblongata
dissolved CO2 penetrates the blood-brain-barrier (while H+ and HCO3- cannot)
in CSF, catalyses the formation of HCO3- and H+ (from CO2 and H2O)
the H+ made in the reaction stimulates AP firing of chemosensitive neurons
peripheral chemoreceptors
what are carotid bodies
location, which CN
what are aortic bodies
location, which CN
what is the metabolic rate and blood flow like for peripheral chemoreceptors
CAROTID BODIES:
Located at the bifurcation of each common carotid artery
Afferent fibres of glossopharyngeal nerve CN IX
AORTIC BODIES:
Located on the underside of the aortic arch
Afferent fibres of the vagus nerve CN X
Peripheral chemoreceptors have high metabolic rate and high arterial blood flow
They are complex structures made of glomus cells, arterioles sinusoids, afferent and efferent neurons
peripheral chemoreceptors
what do they mainly sense (condition of blood)
what increases sensitivity of carotid bodies
what do glomus cells detect
how
They mainly sense hypoxaemia, a decrease in blood pO2
a decrease in pH and increase in pco2
Glomus cells detect changes in PaO2
Receptor activates and closes K+ membrane channels
Depolarisation
VG Ca2+ channels -> ca2+ influx -> exocytosis of NT
Sensory neurons activated -> AP
what are short term compensations for a drop in pO2 or rise in pCO2
firing of AP
ventilation
heart rate
cardiac output
Fall in Pao2/ rise in pco2
Increased firing of chemoreceptors
Increased ventilation, increase o2 (decreases arterial pco2 and increase lung stretch)
Inhibition of cardio-inhibitory centre in medulla -> tachycardia -> increase cardiac output
long term adaptations of low O2/ high CO2
erythrocyte production
what detects hypoxaemia
what hormone is produced
what is a result
O2 unloading
what does low pO2 stimulate in RBC
what does 2,3-DPG bind to and do
what unloading is increased
Increased erythrocytes production
Hypoxaemia is detected by fibroblast-like cells in the renal cortex
Activation of hypoxia inducible factor HIF
Increased transcription erythropoietin EPO
EPO stimulates erythrocytes production in bone marrow
Increases O2 carrying capacity of blood
But, can increase blood viscosity and risk of thrombus
Enhanced O2 unloading at the tissues
Low pO2 stimulates glycolysis in erythrocytes and ^ production of 2,3 DPG
2,3-DPG binds to Hb and lowers Hb affinity for O2 (right shift in Hb-O2 dissociation curve)
Increased O2 offloading
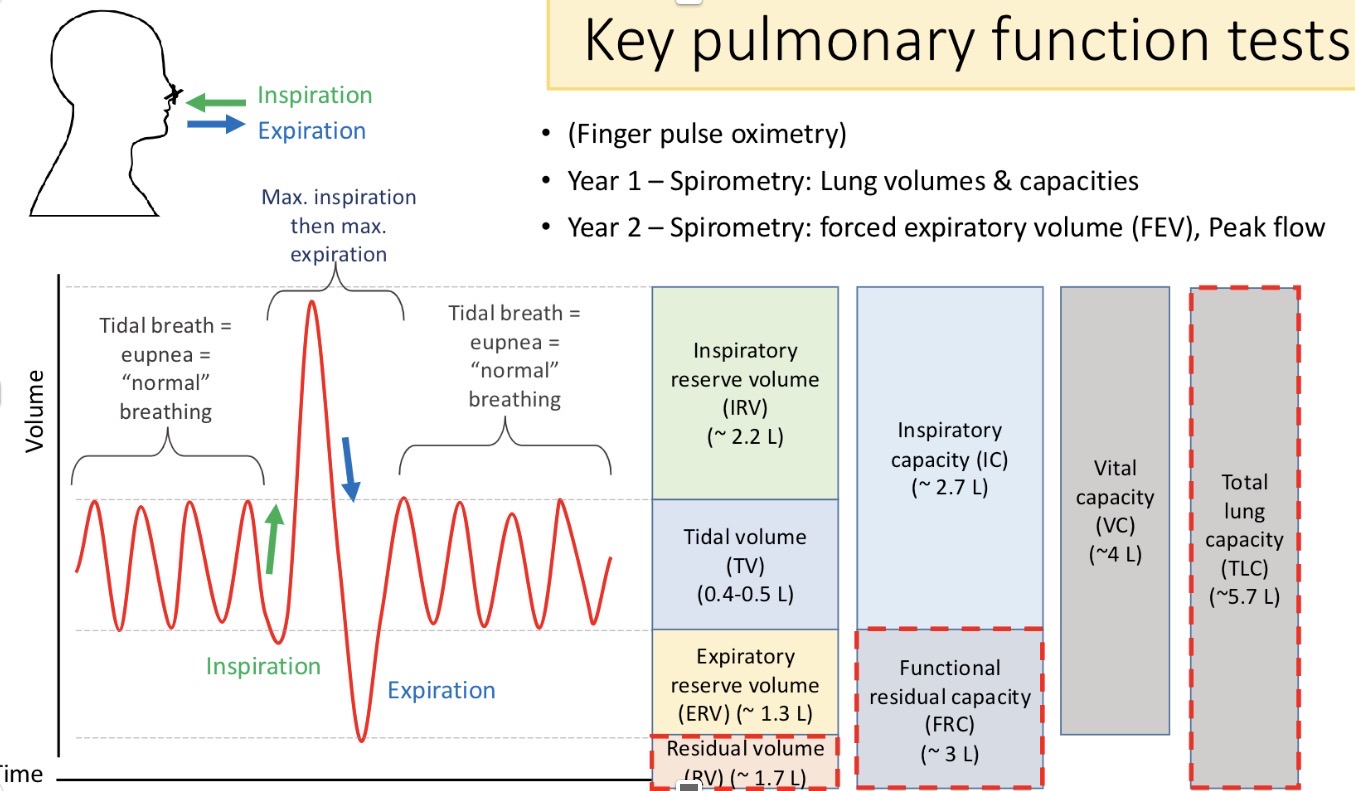
name:
inspiratory reserve volume
tidal volume
inspiratory capacity
vital capacity
expiratory reserve volume
total lung capacity
functional residual capacity
residual volume