Lectuer 43: Fungal and Opportunistic Respiratory Infection
1/111
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
112 Terms
Pathogenic
Pathogenic or Opportunistic?
• Blastomyces dermatitidis
• Coccidioides immitis
• Histoplasma capsulatum
Opportunistic
Pathogenic or Opportunistic?
• Cryptococcus neoformans
• Candida albicans
• Aspergillus spp.
• Pneumocystis jirovecii
Opportunistic
Pathogenic or Opportunistic?
• Rhizomucor
• Mycobacterium avium complex
• Mycobacterium kansasii
• Cytomegalovirus
Opportunistic Infection
Infections that are more frequent or more severe in immunocompromised patients
Endemic Mycoses
• Fungal infections with pathogens found in specific areas
• Can cause disease in immunocompetent patients
Blastomycosis, Coccidioidomycosis,
Histoplasmosis
endemic mycoses in US
Paracoccidioidomycosis
endemic mycoses in Central and South America
Talaromycosis
endemic mycoses in Southeast Asia
-Acute self-limited pneumonia
-Chronic Disease
-Disseminated infection
3 basic forms of disease due to fungi
Blastomyces dermatitidis
• Thermally dimorphic fungus: white mold at 25°C, brown yeast at 37°C
• Thick refractile cell wall, single broad based budding
Blastomyces dermatitidis
• Endemic in Ohio and Mississippi River valleys, Great Lakes area, and SE U.S.
• Isolated from soil containing decaying vegetation
• Transmitted by inhaling conidia
Blastomycosis
Acute pneumonia:
• Looks like viral or bacterial pneumonia
• Cough becomes productive as illness progresses
• Fever, SOB, weight loss, night sweats
Chronic pneumonia:
• Looks like tuberculosis or carcinoma
• Diagnosis is delayed
• Fever, productive cough, hemoptysis, chest pain, weight loss
Blastomycosis
Blastomycosis

Blastomycosis
Skin:
• Verrucous lesion with irregular borders
• Ulcerative lesions with well-demarcated
borders
• Subcutaneous nodules
Osteomyelitis:
• Soft tissue swelling or chronic sinus drainage
• Little to no bone pain
Blastomycosis
• Inhaled conidia are phagocytized
• Thick cell wall of yeast form is difficult to phagocytize
• Giant cells and epithelioid granulomas form (pyogranulomatous inflammatory response)
• Glycoprotein BAD-1 facilitates binding to macrophages, allowing dissemination
Blastomycosis
• Sabouraud dextrose agar @ 25-30°C, takes 1-4 weeks
• Conidia found singly at tips of conidiophores; resemble lollipops
• Presumptive diagnosis made by visualization of yeast in a clinical specimen
• KOH wet mount or H&E staining
• May use PAS or Gomori Methenamine Silver stain
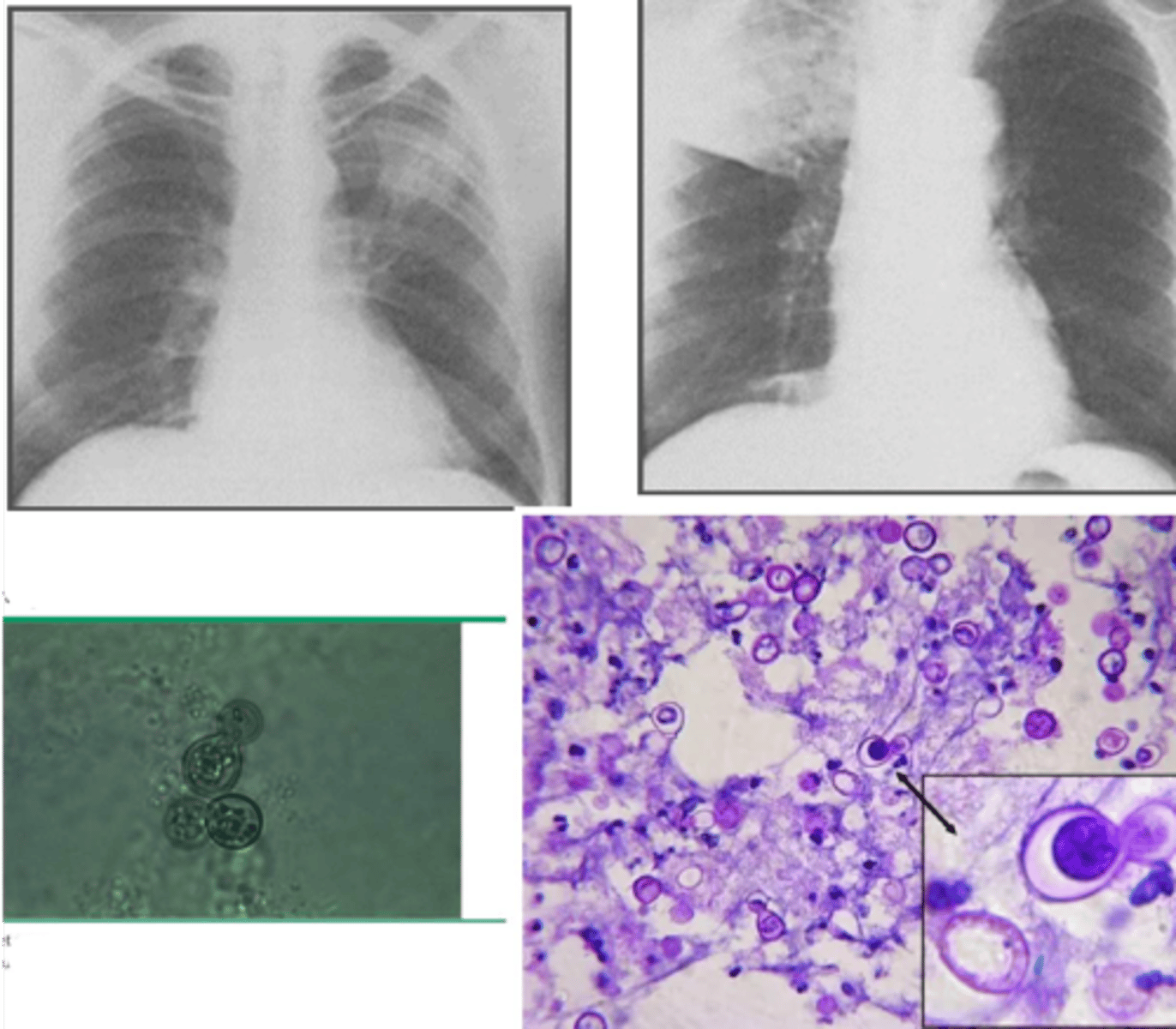
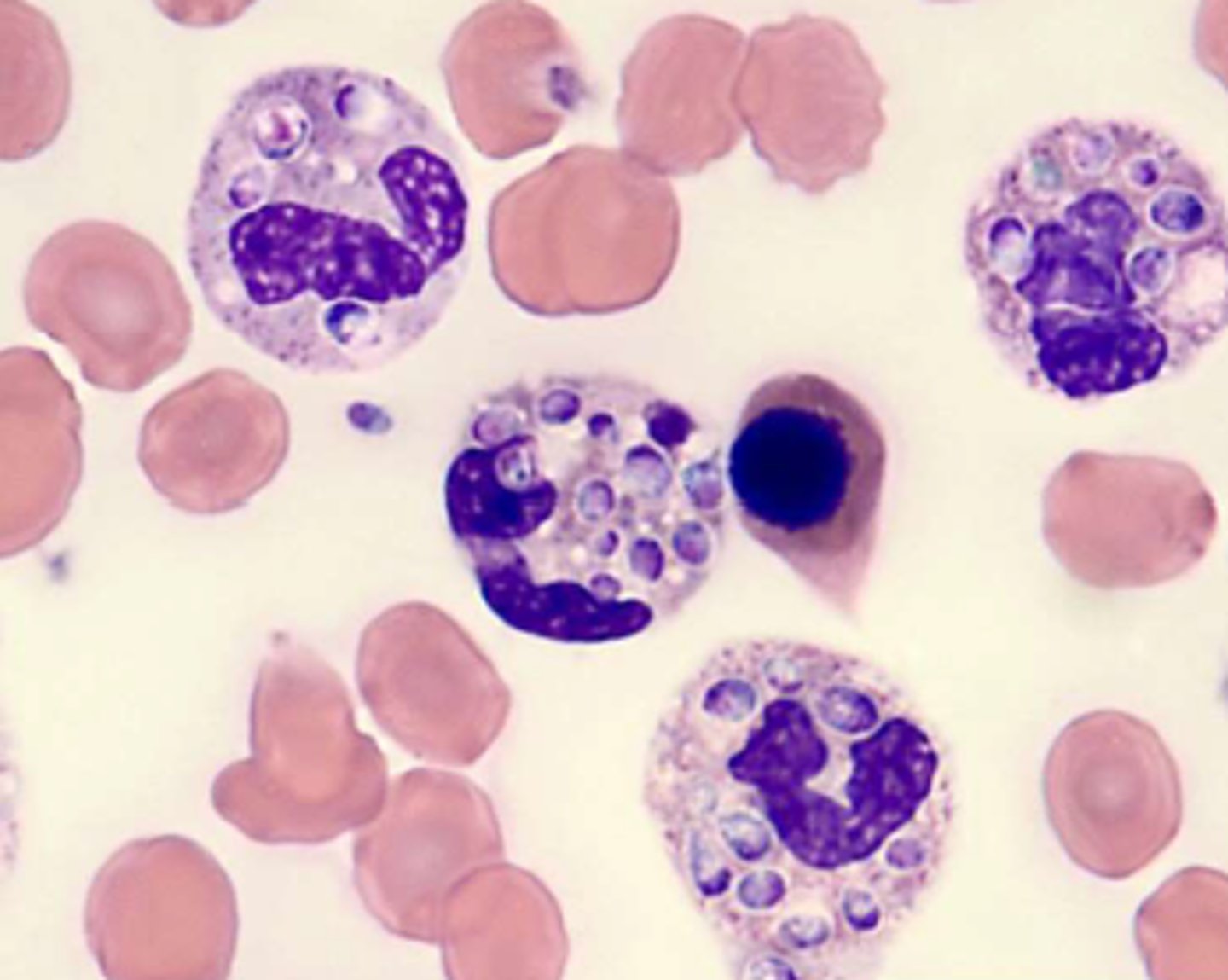
Histoplasmosis
aka Darling Disease
Histoplasma capsulatum
• Thermally dimorphic fungus (mold in soil, yeast at body temp)
• Ovoid yeast with narrow based budding
• Survives inside macrophages
Histoplasma capsulatum
• Most common cause for hospitalization among endemic mycoses
• Most common in midwestern and SE U.S., along Ohio and Mississippi River valleys
• Concentrated in soil contaminated with bird/bat droppings
• Transmitted by inhaling spores from soil
Histoplasma capsulatum
Acute Pulmonary Histoplasmosis
• Looks like community-acquired pneumonia
• Radiographs may show focal infiltrates and mediastinal/hilar lymphadenopathy
• Fever, chills, headache, myalgia, cough, substernal chest pain
• Illness is usually self limited
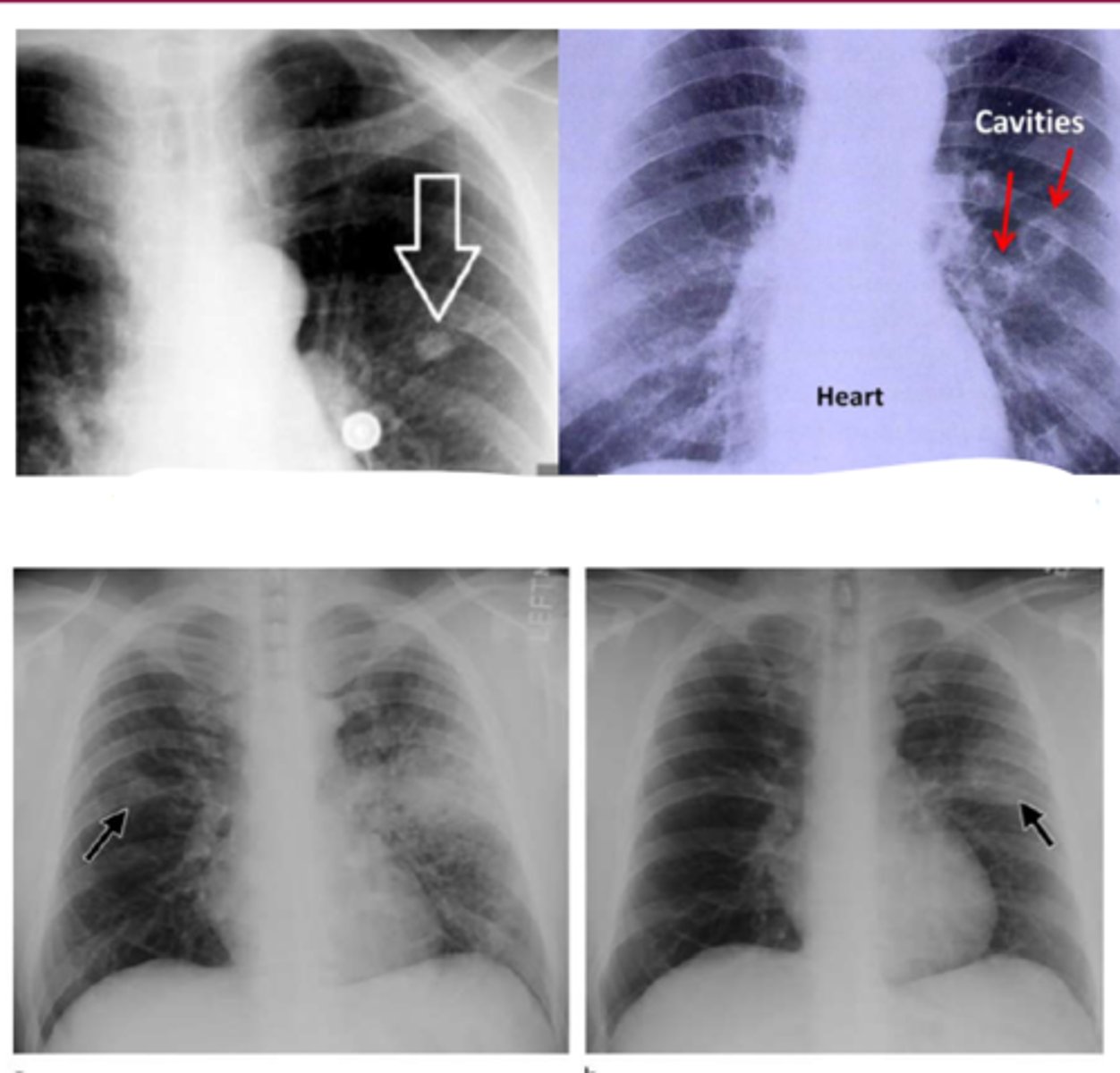
Chronic Cavitary Histoplasmosis
• Seen in older patients with pre-existing lung disease
• Productive cough, dyspnea, chest pain, fatigue, fever, sweats
• Looks like reactivated TB: fibrotic apical infiltrates with cavitation
Disseminated Histoplasmosis
-Histoplasmosis in immunocompromised patients
-fatal if not treated
Acute Histolasmosis
• Fever, fatigue, hepatosplenomegaly, pancytopenia
• Possibly diarrhea and dyspnea
• Severely immunocompromised patients may present with shock and organ failure
Chronic Histoplasmosis
• Pancytopenia, hepatosplenomegaly, oropharyngeal or GI lesions
• May also include skin, brain, and/or adrenal glands
Histoplasmosis
• Macrophages ingest but don't kill fungi; infected macrophages spread fungi
• Cell-mediated immunity is vital for clearing infection
• TNF, IFN-γ, IL-12
Histoplasmosis
-Culture is better in chronic disease, but it's really slow
• Histopathology shows granulomas
• Microscopy can show yeast in specimens
• Detect antigen in serum, urine, or BALF
• Cross reacts with Blastomyces, other fungi
• Serology has limitations
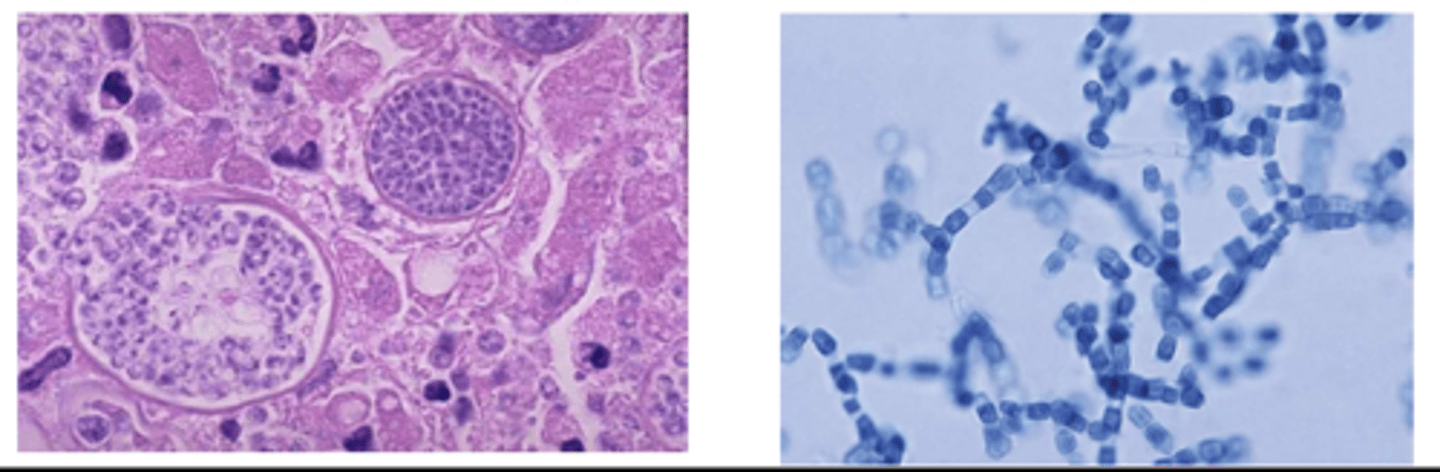
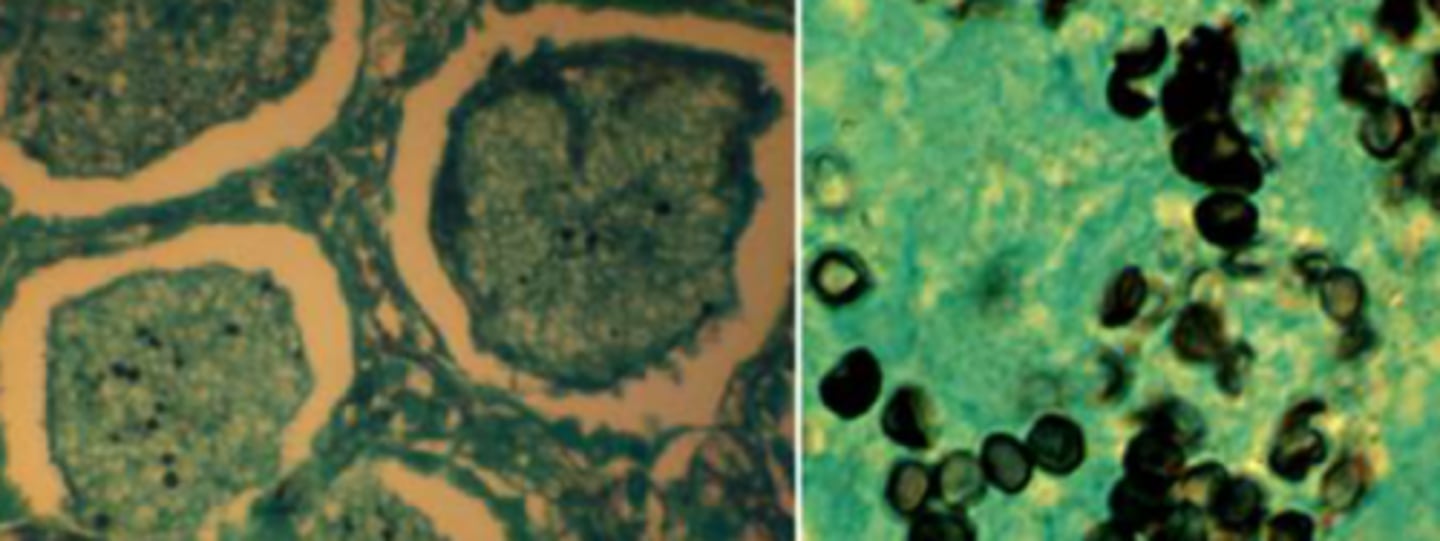
Coccidioidomycosis
AKA San Joaquin Valley fever
Coccidioides immitis
• Dimorphic fungus (mold in soil, spherules in body)
• Septate hyphae with 90° branching; boxcar pattern (thicker arthroconidia alternating with empty cells)
Coccidioides immitis
Primary Coccidioidal Pneumonia
• Looks like community-acquired pneumonia
• Chest pain, cough, fever
• Cutaneous manifestations more common in women
Coccidioidomycosis
• Systemic: fever, night sweats, weight loss
• Desert rheumatism
• Fever, erythema nodosum, arthralgias
• Erythema nodosum, erythema multiforme
Persistent Pulmonary Coccidiodomycosis
• Residual pulmonary nodules
• Coccidioidal cavities
• Usually single, peripheral
• Thin walls
Chronic Fibrocavitary Pneumonia
• When 1° coccidioidal pneumonia doesn't resolve
• More likely in diabetics, immunocompromised, and patients with underlying lung disease
Coccidioidomycosis
Disseminated Coccidioidomycosis
• More common in immunocompromised patients, pregnant women, and patients of African, Filipino, Hispanic, and Native American descent
• Osteomyelitis and synovitis
• Soft tissue infections
• Cutaneous disease
• Meningitis
Coccidioidomycosis
• Arthroconidia are easier to phagocytose
• Spherules are resistant to phagocytosis
• Macrophages can't kill fungi
• Infected macs carry spherules and disseminate pathogen
• Neutrophils and eosinophils are attracted when spherules rupture and release endospores
• Granulomas contain mature unruptured spherules
• Th2 response helps control infection
Coccidioidomycosis
Coccidioidomycosis
• Usually do serology first
• EIA detects IgM or IgG
• May need repeat tests if early in disease
• Stain sputum with KOH or calcofluor white
• Cough is not usually productive
• Stain tissue with H&E, PAS, or Gomori methenamine silver
• Culture takes time and not all labs can do it
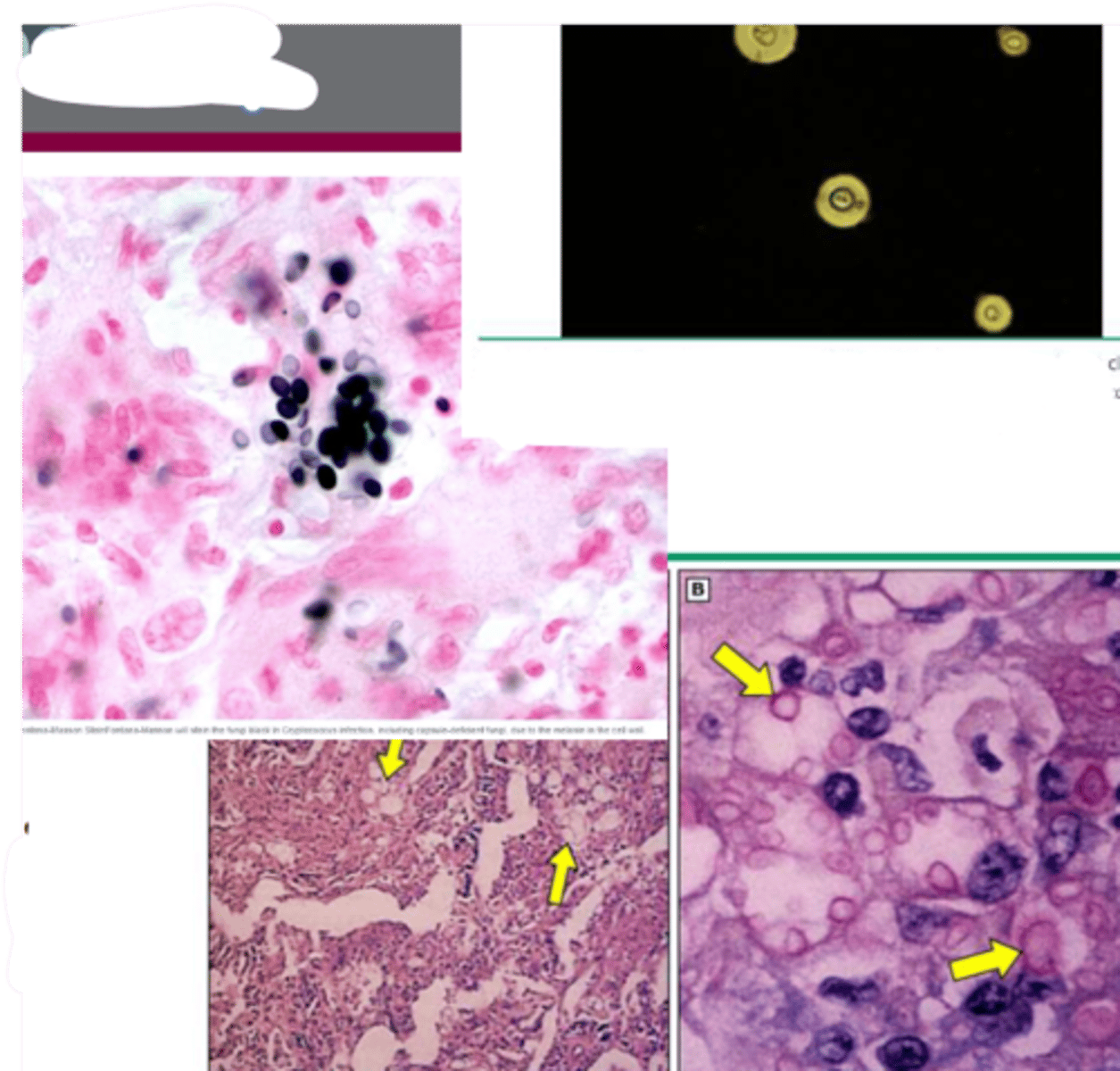
Cryptococcosis
• Encapsulated yeast with narrow based budding
• Urease positive, produces melanin
• Found in soil, associated with birds (esp. pigeons and chickens)
• Risk factors: AIDS, glucocorticoids, organ
transplant, cancer, liver disease, sarcoidosis
Cryptococcosis
Pulmonary infection:
• Cough, hemoptysis, chest pain, fever, malaise,
night sweats, weight loss
Cryptococcal Meningitis
• Fever, malaise, headache
• Photophobia, nausea, vomiting
• Cough, dyspnea, rash suggest disseminated disease
• Most patients have CD4 count <100 cells/uL
• Elevated diastolic pressure indicates ↑ intracranial pressure
Cryptococcosis
• Spores inhaled, fungi disseminates hematogenously
• Localizes to CNS
• CSF is favorable to growth
• Dopamine is a substrate for melanin production
• Inflammatory response is milder than bacterial meningoencephalitis
Cryptococcosis
• Methenamine silver stain in histopathology
• Mucicarmine stains both yeast and capsule,
specific for Cryptococcus
• Fontana-Masson stain shows melanin
• Stain CSF with India ink
• Cryptococcal antigen (CrAg)
• Detects glucuronoxylomannan (GXM)
Cryptococcosis
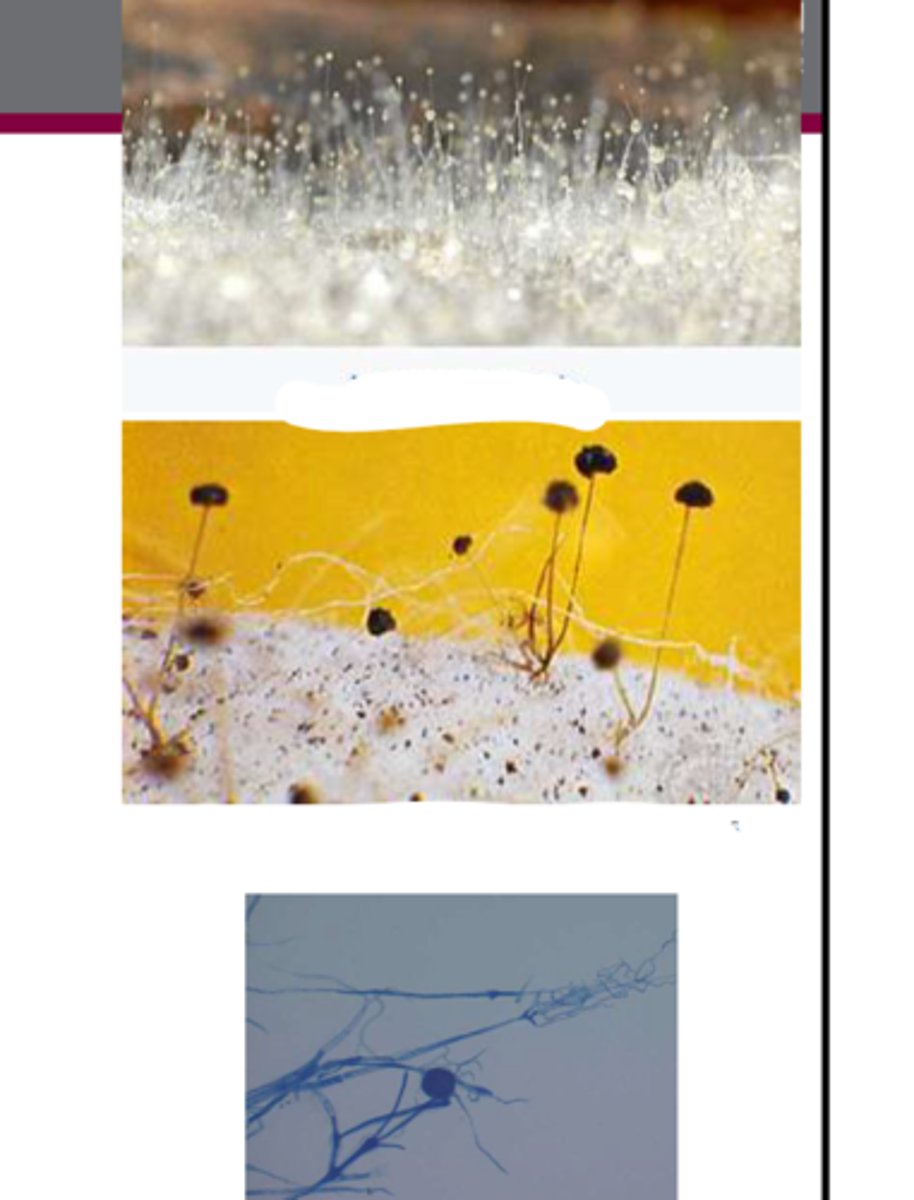
Mucormycosis
AKA zygomycosis
Mucormycosis
• Genera from order Mucorales
• Rhizopus, Mucor, and Rhizomucor
• Broad, irregularly branching hyphae with rare septation
Mucormycosis
• Found in soil and on decaying vegetation
• Causes disease in immunocompromised patients
• Risk factors: diabetes mellitus, hematologic malignancies, organ transplant, burns, deferoxamine
Mucormycosis
Rhinocerebral infection
Rhinocerebral infection
• Most commonly caused by R. oryzae
• Most common risk factor: diabetes, esp. with ketoacidosis
Rhinocerebral infection
• Presents as acute sinusitis with fever, purulent nasal discharge, headache, and sinus pain
• Orbital involvement: periorbital edema, blurred vision, blindness
• Facial numbness
• Usually progresses rapidly
• Black eschar results from necrosis after vascular invasion
Rhinocerebral infection

Pulmonary Mycormycosis
• Bilateral pneumonia, very similar to aspergillosis
• Fever, hemoptysis, dyspnea, cough
• Seen in patients with hematological disease, organ transplants, deferoxamine
• Endobronchial mucormycosis can lead to massive hemoptysis
• Imaging may show reversed halo sign
Mucormycosis
• Inhaled spores become hyphae; hyphae bind to blood vessels and then penetrate
• Angioinvasion leads to infarction, ischemic necrosis
• Ketone reductase allows fungi to survive in acid medium (diabetic ketoacidosis)
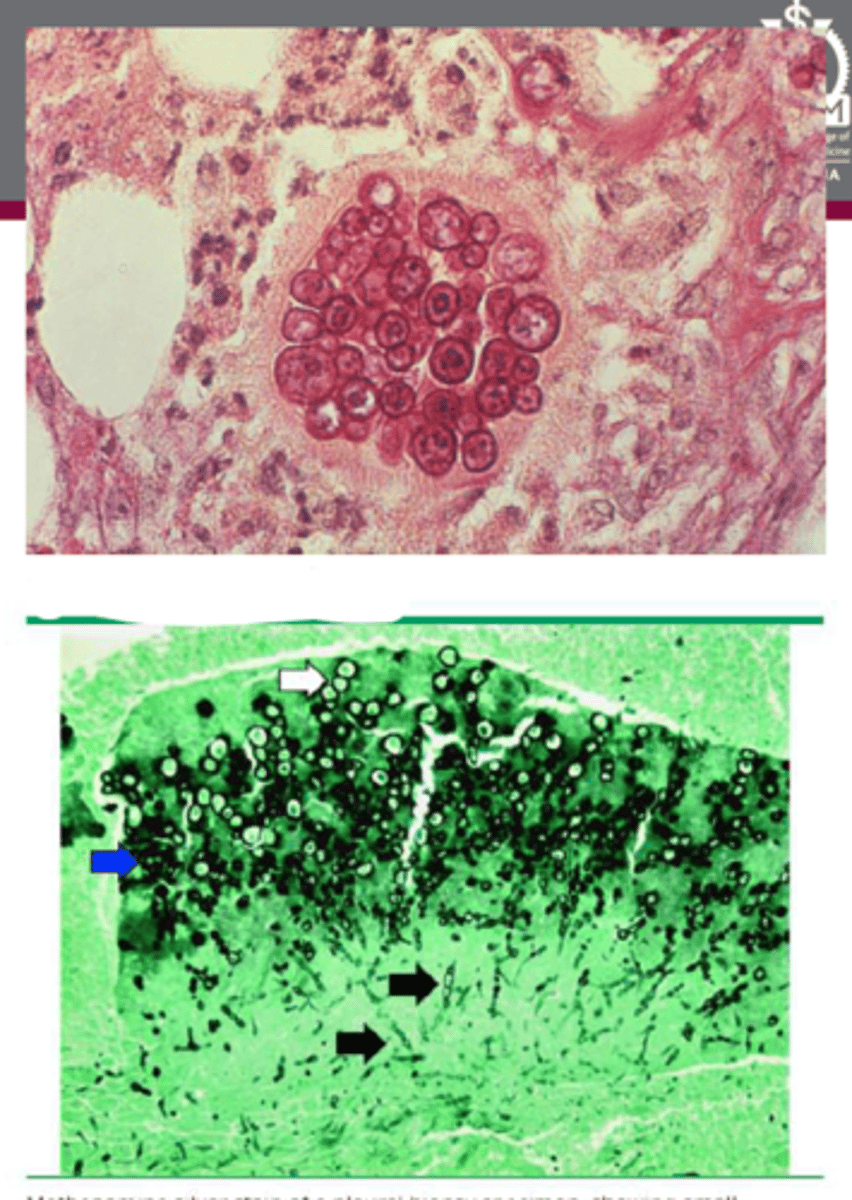
Pneumocystis jirovecii
• Now known to be an Ascomycete; originally thought to be protozoa
• Doesn't grow in fungal culture
• Cell wall contains cholesterol
• Worldwide distribution, both humans and animals
• Likely spread person-to-person
• Causes infections in immunocompromised patients
• Cases in AIDS patients have decreased since ART/HAART
Pneumocystis jirovecii
• Pneumocystis pneumonia in HIV+ patients
• Gradual onset of fever, cough, dyspnea that
progresses
• Fatigue, chills, chest pain, weight loss
• AIDS-defining infection
• Hypoxemia at rest or with exertion; increase in
Aa O2 tension gradient
Pneumocystis jirovecii
Pneumocystis jirovecii
• Trophic forms attach to alveolar epithelium
• Beta glucan in cell walls drives inflammation, variations in major surface glycoprotein (MSG) helps evade immune response
• Host inflammatory response causes damage and impairs gas exchange
Pneumocystis jirovecii
• Can't be cultured, so must identify in respiratory samples
• Preferred technique: IF staining with labeled mAbs
• Stains: Giemsa, GMS, PAS, toluidine blue, calcofluor
• PCR of BAL samples is becoming more widespread
C. albicans
the most common Candida spp.
Candida spp.
• Elliptical budding cells; filaments on solid substrate
• Produces germ tubes in serum within 2 hours at 37°C
• Part of normal GI and genitourinary flora
• Causes infections in immunocompromised patients
• More prevalent in infants and elderly
• Cases associated with HIV patients
Primary Pulmonary Candidiasis
-rare
-pts tend to have widespread systemic illness
-hematogenous spread leads to microabscesses throughout parenchyma

Candidemia
-more common
• Immunocompromised and ICU patients at highest risk
• Presentation is variable
• Skin lesions: painless pustules with erythematous base
Candida spp.
• Commensal organism overgrows when host becomes
immunodeficient
• Blood culture
• Scrape and stain skin lesions
• Gram positive
• Punch biopsy of skin or tissue shows microabscesses, budding yeast, and hyphae or pseudohyphae
• Beta-D-glucan is not specific for Candida
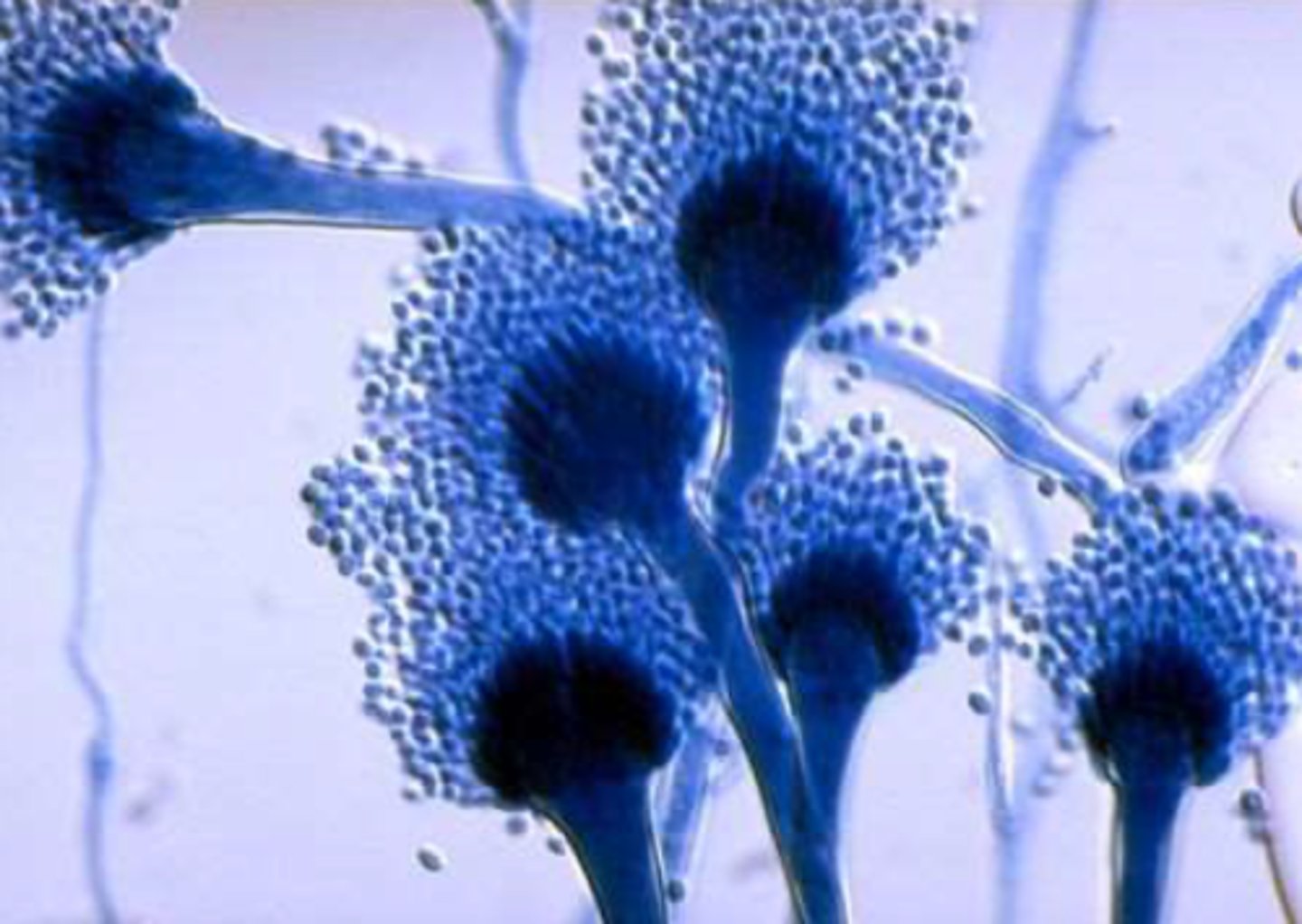
Aspergillus
• Mold in nature and in hosts
• Hyphae have 45° branching
• Worldwide distribution, lives in soil and decaying vegetation
• Transmitted by inhaling spores
• Infections in immunocompromised patients
A. fumigatus, A. flavus, A. niger, and A. terreus
most common aspergillus spp. in humans
Aspergillus
Invasive Aspergillosis
• Incidence is increasing
• Classic presentation in neutropenic patients: fever, pleuritic chest pain, hemoptysis
• Dyspnea, chills, headache, arthralgias
• Pulmonary nodules and/or infiltrates
• Prognosis is poor
-vascular invasion with subsequent infarction and necrosis
Allergic Bronchopulmonary Aspergillosis (ABPA)
• Almost always in asthma or CF patients
• Bronchial obstruction, fever, malaise, production of brown mucus plugs, +/- hemoptysis
-IgE-mediated allergic response to Aspergillus colonization of airway
Chronic Pulmonary Aspergillosis
• Presents with chest pain, weight loss, cough, hemoptysis, SOB, fatigue
• Patients are generally immunocompetent, but have prior lung disease/damage
Aspergilloma
a fungal ball generally found in a preformed cavity of the lung, composed of a mass of Aspergillus hyphae
Aspergilloma
• Visualize with air crescent or meniscus sign
• Preexisting cavities are colonized with Aspergillus
Chronic Cavitary Pulmonary Aspergillosis
-regions of consolidation progress to form cavities
• Cavities are thin-walled
• New cavity formation or expansion of existing
cavities over time is characteristic
-prior lung damage leaves places for Aspergillus to grow
Invasive Aspergillus
Diagnosis:
-Galactomannan and beta-D-glucan serum biomarkers
Allergic Bronchopulmonary Aspergillosis (ABPA)
Diagnosis:
-asthma of CF
-elevated IgE
-+aspergillus skin test
Chronic Pulmonary Aspergillosis
Diagnosis:
-negative for TB
-positive for Aspergillus IgG
Nontuberculous Mycobacteria (NTM)
• Acid-fast bacilli, ubiquitous in environment
• Stain with Ziehl-Neelsen or carbol-fuchsin
• Grow on Middlebrook 7H11 or Lowenstein-Jensen agar
• Slow growing; takes 2-4 weeks
M. avium Complex (MAC) and M. kansasii
Most common disease-causing NTM in the US
Mycobacterium Avium Complex (MAC)
• Disease in patients with underlying lung disease (fibro-cavitary disease)
• White males, middle-aged or older, with COPD
• Alcohol abuse or smokers
• CF patients
• Disease in patients without underlying lung disease (nodular bronchiectatic form)
• Nonsmoking females >50 years old
• Disseminated disease
• CD4 count <50 cell/uL
Mycobacterium Avium Complex (MAC)
• taken up by alveolar macrophages
• Bacteria survive inside phagocytes
• Granulomas form to wall off infected cells
• Damage caused by cytolytic enzymes and other cytotoxic proteins leads to necrosis and fibrosis of tissues
• Positive culture from sputum, BAL, or• Positive culture from sputum, BAL, or biopsy
• Biopsy stainin biopsy
• Biopsy staining
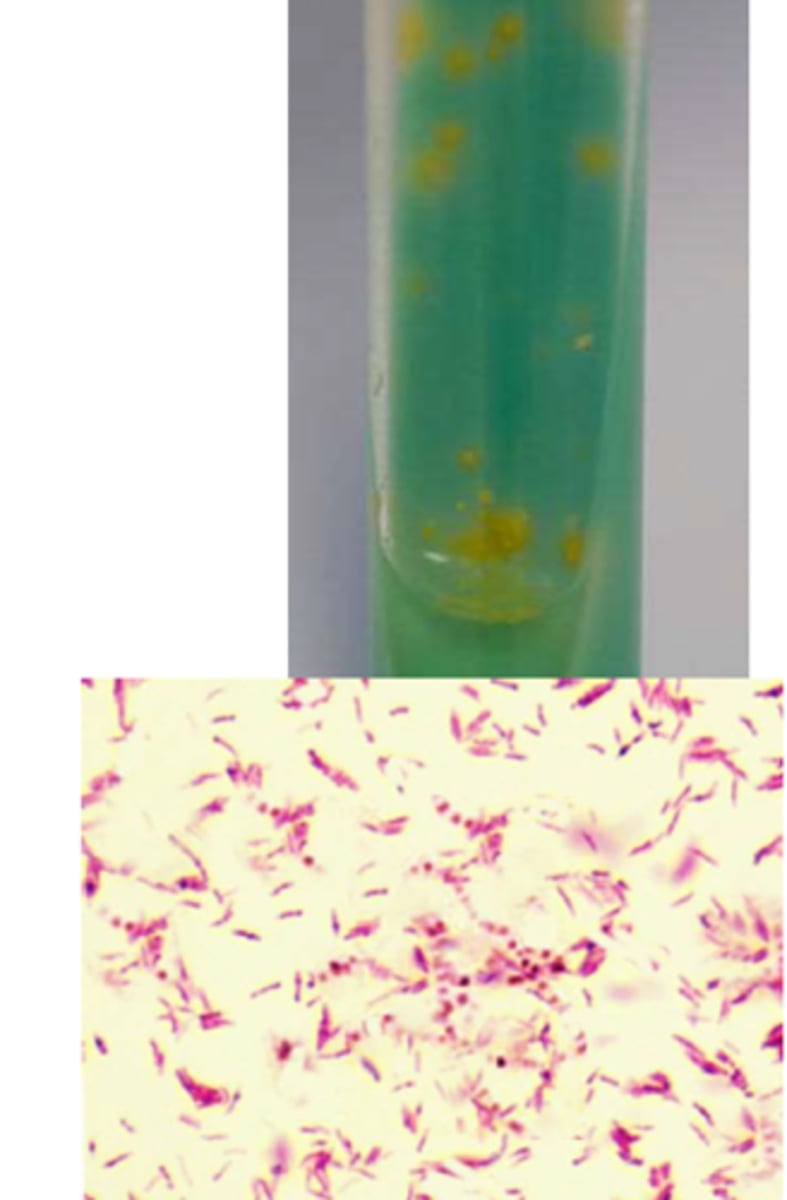
Mycobacterium kansasii
• Not found in soil, but is in tap water
• Produces rough colonies that turn bright yellow when exposed to light (photochromogen)
• Unusual beading when stained with acid-fast stains
• More common in southern and central U.S. and urban areas
• May be associated with mining
• Was the most common NTM infection in the 1960-70s, but surpassed by MAC
Mycobacterium kansasii
Mycobacterium kansasii
• Presents like TB
• Productive cough, weight loss, SOB, chest pain, hemoptysis, fever/sweats
• Older age, male, smoking, and underlying lung disease are risk factors
• Causes disseminated disease in HIV+ patients
Cytomegalovirus
-AKA human herpesvirus 5 (HHV-5)
• Herpesviridae
• Enveloped, with dsDNA genome
Cytomegalovirus
• Majority of adults are seropositive
• Transmitted via blood, breastfeeding, perinatally, sex, and close contact
• Reactivation is associated with increased morbidity and mortality
Cytomegalovirus
• If symptomatic, illness presents like infectious mononucleosis
• Fever, rash, fatigue, leukocytosis
• Don't see heterophile antibodies; helps differentiate from EBV infection
• Immunocompromised patients may have specific organ diseases
• Lung transplant patients may have pneumonitis
Cytomegalovirus
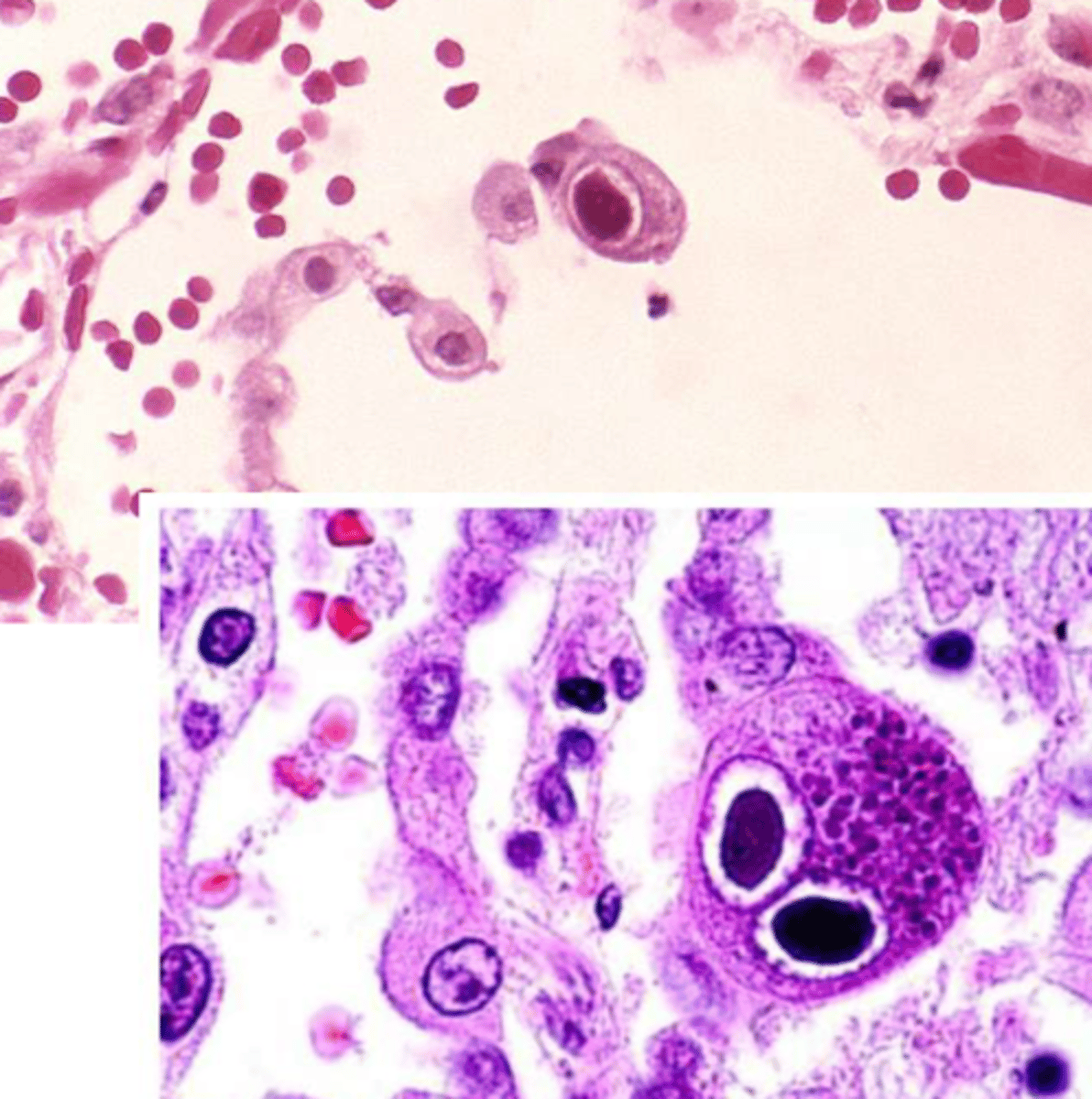
Cytomegalovirus
• Lytic infection leads to dramatic cell enlargement
• Virus rearranges cellular protein production to create large perinuclear replication compartment
• Viral load
• Owl's eye appearance of inclusion
bodies
Usually resolves before diagnosis
treatment of acute pulmonary forms of Blastomycosis
Itraconazole for 6-12 months
treatment of mild to moderate forms of Blastomycosis
• Amphotericin B until initial improvement (several weeks)
• Then itraconazole for at least 12 months
treatment of severe forms of Blastomycosis (CNS involvement and immunosuppressed pts)
Steroids
if a pt with Blastomycosis is in respiratory distress, what can you give them?
• Typically resolve spontaneously before diagnosis is made
• If not resolved after 1 month - itraconazole for 6-12 weeks
Treatment of Asymptomatic or mild to moderate forms of primary pulmonary histoplasmosis
Amphotericin B for 1-2 weeks +/- steroids, then itraconazole for 3 months
treatment of severe forms or immunosuppressed pts with primary pulmonary histoplasmosis
Itraconazole (at least 1 year)
treatment for Chronic Cavitary Pulmonary Histoloplasmosis
itraconazole for 12 months or more
treatment for mild to moderate Disseminated Histoplasmosis
Amphotericin B for 1-2 weeks, then itraconazole (up to 2 years)
treatment of moderately severe to severe disseminated histoplasmosis
No treatment
treatment for primary coccidioidomycosis
Itraconazole or fluconazole for at least 1 year
Treatment for Secondary and Disseminated Forms of Coccidioidomycosis