essay 26 - teeth extractions in medically compromised patients teeth extractions in medically compromised patients(disorders of cardiovascular and respiratory systems). management
1/21
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
22 Terms
list some cardiovascular diseases
ineffective endocarditis prophylaxis
hypertension
ischemic heart disease
cardiac arrhythmias
What is ineffective Endocarditis prophylaxis, provide some symptoms
it is a serious, potentially fatal microbial infection of the heart's endothelial lining or valves, often associated with congenital or acquired cardiac defects
Symptoms = fever, heart murmur, Positive blood cultures, petechiae, splinter haemorrhages
what are some cardiac conditions for prophylaxis before tooth extraction (ineffective endocarditis prophylaxis)
prosthetic heart valves
previous infective endocarditis
congenital heart disease
heart transplant recipients with valvulopathy
what are some procedures requiring prophylaxis (ineffective endocarditis prophylaxis)
manipulation of gingival tissue
manipulation of periopical region of teeth
manipulation of periopical region of teeth perforation of oral mucosa
what are some procedures not requiring prophylaxis (ineffective endocarditis prophylaxis)
radiographs
routine local anaesthesia through healthy tissue
prostodontic/ orthodontic appliance placement
appliance adjustments
shedding of primary teeth and trauma related bleeding
antibiotic regimen (30-60 minutes Before procedures) - ineffective endocarditis prophylaxis
amoxicillin - oral = adult 2g; Child 50 mg/kg
ampicillin - IM/IV = adult 2g; child 50 mg/kg
clindamycin - if allergic to penicilin = adult 600mg, child 20 mg/kg
Azithromycin - if allergic to penicilin) = adult 500 mg, child 15 mg/kg
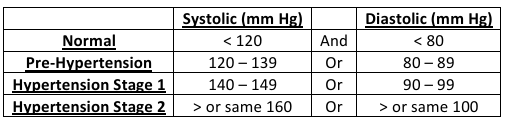
define hypertension and the classifications
it is abnormal elevation in arterial blood pressure. the primary concern for dental treatment of hypertensive patients is that there is an extreme danger that there is an acute elevation in blood pressure as it can lead to stroke or myocardial infarction, this acute elevation can be caused by the release of catecholamines in response to stress or anxiety, or from vasoconstrictors (can be from the retraction code or from local anaesthetic)
causes of hypertension
90% of cases are primary Idiopathic hypertension
chronic kidney disease
thyroid or parathyroid disease
glucocorticoid excess
drug induced - chronic use of NSAIDs
what is the dental management of hypertension
short, stress free morning appointments
medical history e.g diagnosed with hypertension, how it's being treated, presence of symptoms
monitor blood pressure pre and intraoperatively
used modest amounts of epinephrine (max 0.036 mg)
caution in patients on non selective beta blockers
avoid orthostatic hypotension (change chair positions slowly)
consider anxiolytic premedication if anxiety is high
avoid extraction if BP is dangerously high (>179/109 mmHg) until stabilised
describe ischemic heart disease, give symptoms
narrowing of coronary arteries due to atherosclerosis leading to myocardial ischemia
Symptoms = chest pain chest pain(angina), breathlessness, fatigue and signs of congestive heart failure
what are the three determinants of dental management of ischemic heart disease
severity of disease
type and magnitude of dental procedure
stability and reserve of patient
dental management for stable angina or past MI (>6 weeks ago)
short, morning appointments
stress reduction and pain control(operative and post operative)
nitroglycerin readily available
Limit vasoconstrictor use (epinephrine </= 0.036mg, 0.2mg levonordefrin)
avoid anticholinergics e.g atropine
antibiotic prophylaxis not required for stents or bypass history
if patient had MI (myocardial infarction) in past 30 days or has unstable angina, what precautions should be made
defer elective procedures
emergency care only with physician consultation
consider: sedation, oxygen, prophylactic Nitro glycerine, ECG monitoring, blood pressure monitoring, pulse oximeter, cautious use of epinephrine in local anaesthetic
what are Cardiac arrhythmias, provides symptoms
any variation in heartbeat, rhythm, rate or conduction pattern of the heart
symptoms- palpitations, dizziness, syncope, shortness of breath, below 60 BPM, above 100 BPM, irregular rhythm, angina
dental management of cardiac arrhythmias
stress and anxiety reduction - short morning appointments, comfortable chair position, post operative and intraoperative sedation
limit vasoconstrictor (</= 0.036 mg epinephrine), risk of complications increases with dose
avoid ultrasonic instruments and Electro surgery if pacemaker is present
monitor INR If on anticoagulant (INR 2-3.5 is safe for extraction if patient takes anticoagulant)
use local hemostatic measures
avoid digoxin interactions and watch for toxicity, if on digoxin avoid epinephrine or levonodefrin
consult physician for high risk cases, provide only a monthly treatment if necessary
precautions that should be taken if patient is on anticoagulants for example warfarin or sinthrome
must have INR determined before any invasive procedure is performed
if the procedure is extensive you must do the following:
discontinue watering four days before surgery, there is a danger here as the patient may be in the temporary hypercoagulable state
begin 30 mg of containers enoxoparine every 12 hours starting 3 days before surgery
last dose of enoxaparin is at 9:00 PM the evening before surgery
INR is checked on mroning of surgery and must be 1.0 or less
an enoxoparin injections begin again on the evening after the surgery and warfarin too
three days post OP the patients can stop enoxoparin
list some respiratory disorders
chronic obstructive pulmonary disease
asthma
what is chronic obstructive pulmonary disease - for respiratory disorder
irreversible chronic air flow limitation due to chronic bronchitis or emphysema
dental management of chronic obstructive pulmonary disease
Upright Chair Position
avoid rubber dams and nitrous oxide sedation
use pulse oximetry
Administer supplemental oxygen if saturation <95%
avoid barbiturates, narcotics, anticholinergics
avoid macrolides and ciprofloxacin in patients on theophylline
do not use outpatient general anaesthesia
describe asthma - Respiratory disorder - provide symptoms
chronic inflammation and hyper responsiveness of airway
Symptoms = dyspnea, wheezing, coughing (especially at night), chest tightness , tachypnea, chest tightness
dental management of asthma
identify asthma severity and triggers, provide stress free environment
ask patient to bring inhaler to the appointment
avoid NSAID, aspirin, barbiturates and narcotics. Avoid macrolides in theophyline uses
discontinued use of cimetidine 24hrs before intravenous sedation in patients taking theophyline
use sulfite free anaesthetic if needed
provide stress free environment
sedation with nitrous oxide is OK in mild/ moderate asthma
what should be done during an asthma attack
use short acting Beta 2 Agonist inhaler (e.g ventolin)
Administer oxygen
give epinephrine (0.3-0.5 ml of 1:1000) is severe
repeat bronchodilator every 5 minutes if needed
activate EMS