OMFS (Exam 4): Management of Mandibular Fractures
1/50
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
51 Terms
male
The majority of facial trauma patients are what gender?
interpersonal violence
What is the most common cause of facial trauma?
condyle
What is the most common location for mandibular fractures:
angle of the mandible
What is the 2nd most common location for mandibular fractures:
symphysis of the mandible
What is the 2nd most common location for mandibular fractures:
true
t/f: Typically, mandibular fractures come in pairs
ramus
All of the following locations, if a fracture occurs in these areas, it will almost always traverse the alveolus as well, EXCEPT for:
- symphysis
- body
- angle
- ramus
distal canine
what tooth separates the mandibular symphysis from the body?
Greenstick
ID the type of mandibular fracture:
•an incomplete fracture
•Typically in soft, flexible bone, often in children
•No mobility (both cortices are not fractured)
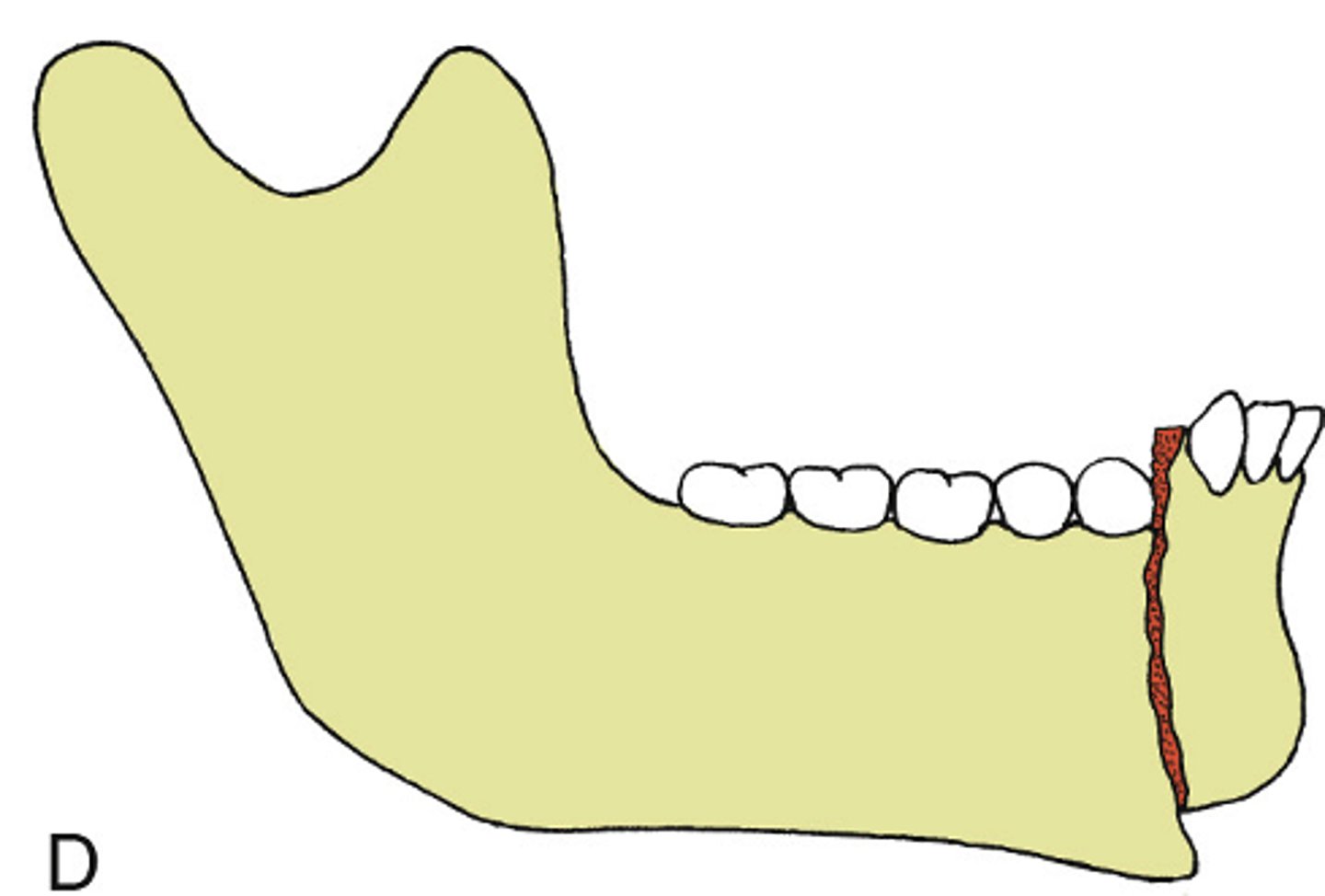
Simple
ID the type of mandibular fracture:
•complete fracture with little fragmentation
•"A clean break"
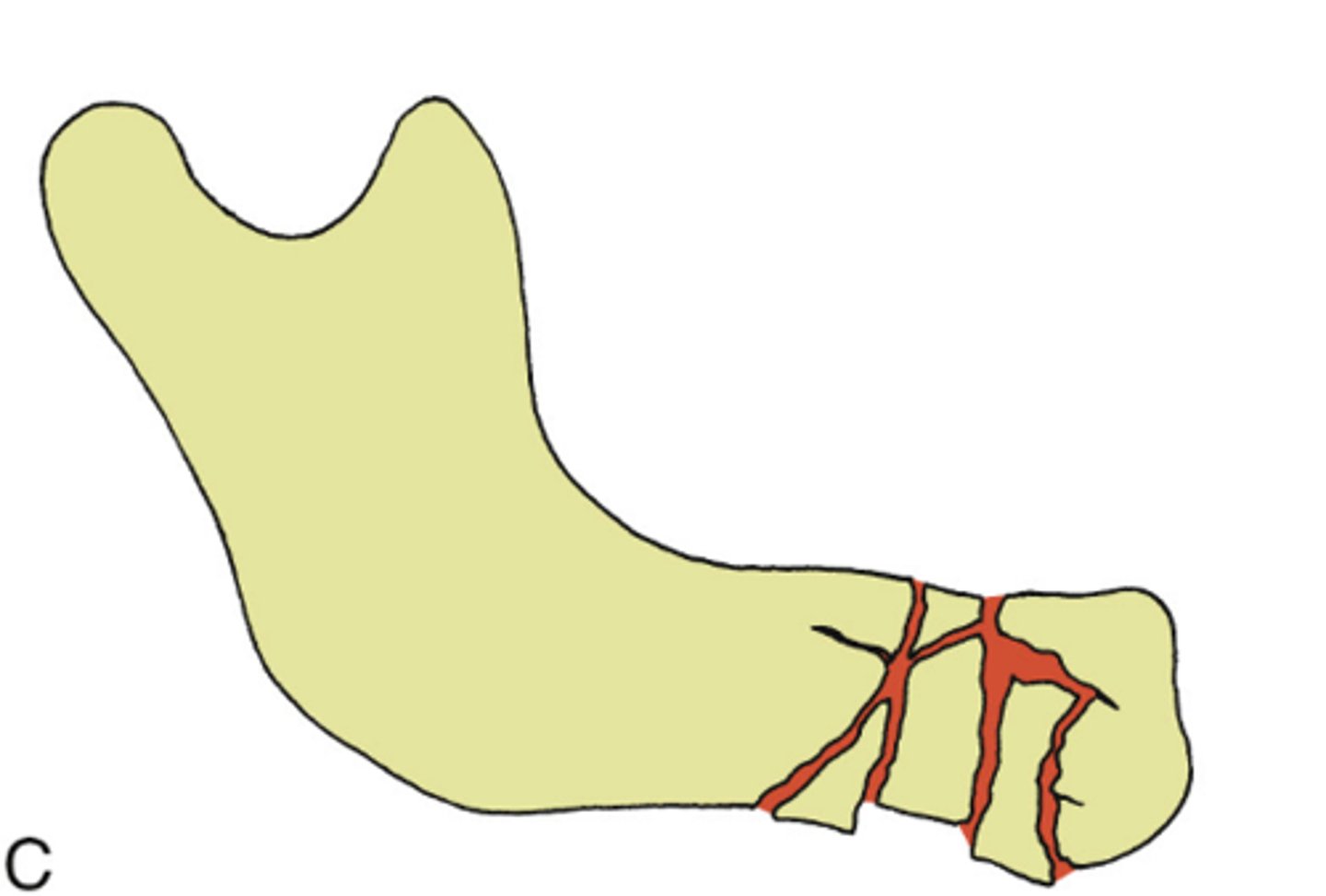
Comminuted
ID the type of mandibular fracture:
•a fracture in multiple pieces
•Often from a high energy injury
Compound
ID the type of mandibular fracture:
•a fracture that communicates with the oral or external environment
•A fracture that is open into the mouth (via the periodontal ligament/gingival sulcus or a visible step
•A fracture open to the sinus or the skin
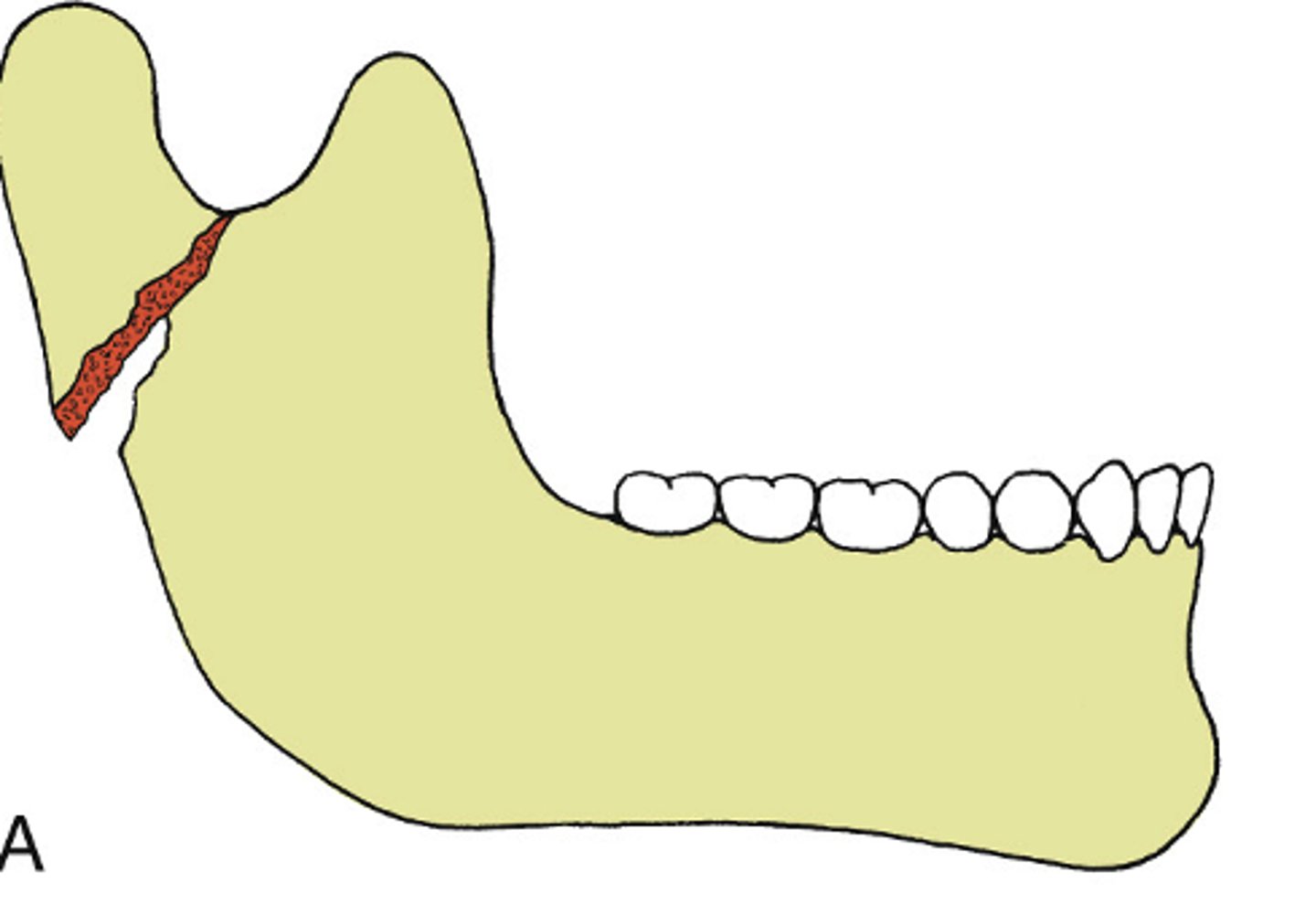
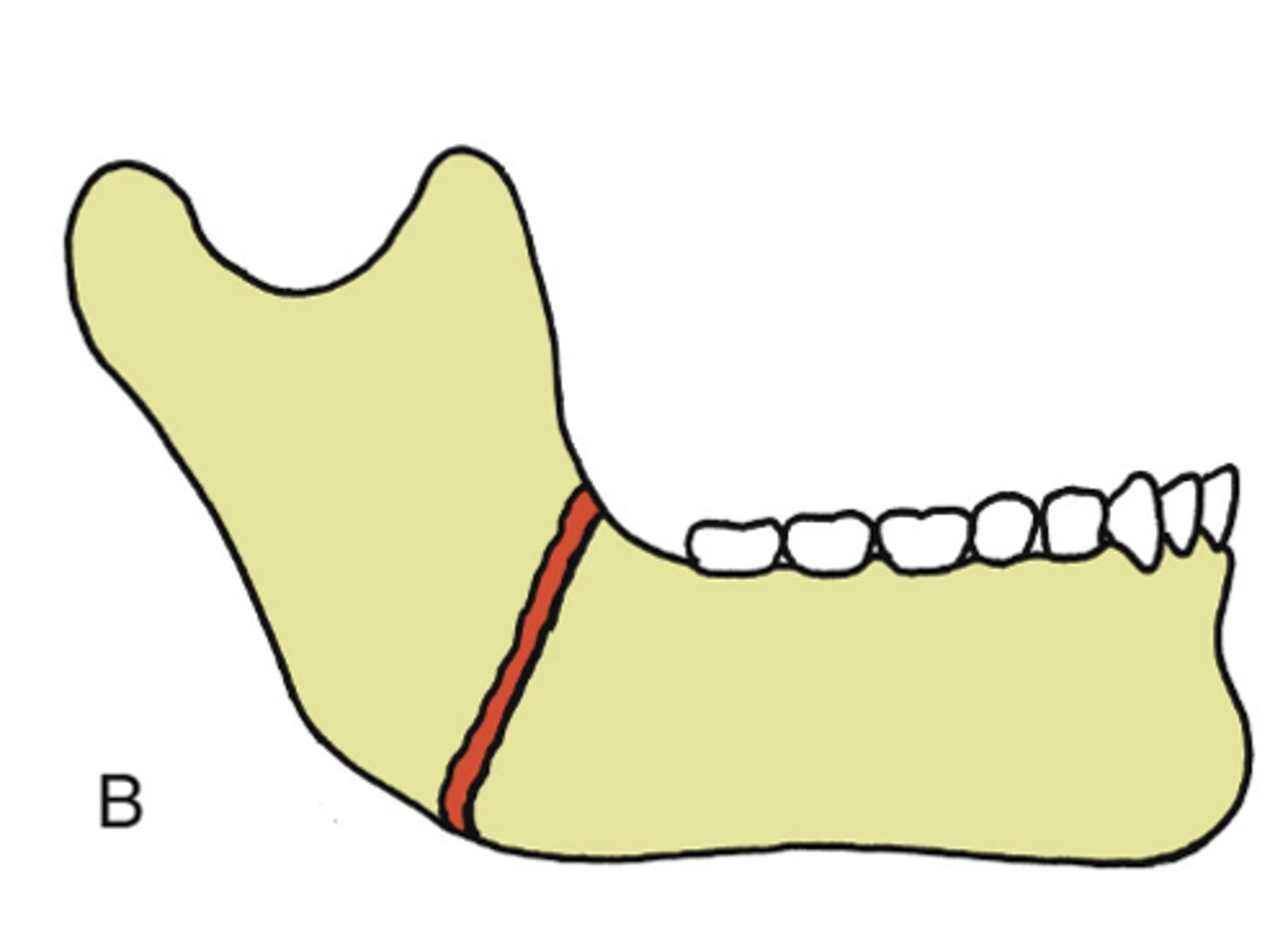
Favorable fractures
A mandibular fracture where the natural muscle pull resists displacement:
Unfavorable fractures
A mandibular fracture where the natural muscle pull displaces the fractured segments:
immobilization
Rapid bone healing requires ________ to allow bone healing
soft diet
What is the appropriate management for a patient with Greenstick fractures:
soft diet
What is the appropriate management for a patient that is highly adherent:
soft diet
What is the appropriate management for a patient with condylar head fractures:
soft diet
What is the appropriate management for a patient with no malocclusion fractures:
closed treatment/ maxillomandibular fixation
What is the appropriate management for a patient with non-displaced favorable fractures:
closed treatment/ maxillomandibular fixation
What is the appropriate management for a patient with severe comminution fractures:
closed treatment/ maxillomandibular fixation
What is the appropriate management for a patient with extensive soft tissue injury:
closed treatment/ maxillomandibular fixation
What is the appropriate management for a patient that is medically unable to undergo general anesthesia:
closed treatment/ maxillomandibular fixation
What is the appropriate management for a patient with infected fractures:
open reduction/ internal fixation
What is the appropriate management for a patient with displaced and/or unfavorable fractures:
open reduction/ internal fixation
What is the appropriate management for a patient with medically contraindications to MMF:
open reduction/ internal fixation
What is the appropriate management for a patient with bilateral displaced subcondylar fractures:
open reduction/ internal fixation
What is the appropriate management for a patient that are non-adherent :
Erich Arch Bars
ID the closed treatment/ maxillomandibular fixation:
•Allows for some movement during reduction
•24- or 26- gauge wire applied around the arch bar and the teeth

Erich Arch Bars
Which MMF device is the most time consuming?
Erich Arch Bars
Which MMF device is a poor choice for patients with significant periodontal disease?
Hybrid Arch Bars
ID the closed treatment/ maxillomandibular fixation:
•Less time consuming, less skin puncture risk to provider
•Fixates arch bars directly to the bone with screws
•Possible damage to tooth roots

IMF screws
ID the closed treatment/ maxillomandibular fixation:
•Screw directly into the bone
•Typically not used for extended periods (usually intraoperative only)

Ivy Loops
ID the closed treatment/ maxillomandibular fixation:
•Appropriate when few teeth are present
•Typically used for limited fixation period

Gunning Splint
ID the closed treatment/ maxillomandibular fixation:
- used for patients will large edentulous spaces

•Can be performed under local anesthesia
•Less costly
•No concern for future hardware removal
•No incisions/risk for damage to adjacent nerves
•Less bleeding risk
What are the advantages of closed treatment/ maxillomandibular fixation:
•Longer duration of treatment (typically 4-6+ weeks)
•Difficult to perform oral hygiene
•Sometimes difficult to maintain nutrition
•Contraindicated for patients with seizures and sleep apnea
•Relatively contraindicated in patients with alcohol abuse, poor adherence to medical recommendations, etc.
What are the disadvantages of closed treatment/ maxillomandibular fixation:
Open Reduction Internal Fixation
direct surgical access to the fracture is obtained, the fracture is reduced, and hardware is used to fixate the fractured segments
•Earlier return to function
•Allows direct visualization of the fractures and anatomic reduction
What are the advantages of Open Reduction Internal Fixation:
•Longer procedure, requires general anesthesia
•Greater risk of complications including nerve injury or bleeding
•Potential for scarring depending on approach
•Greater cost
What are the disadvantages of Open Reduction Internal Fixation:
•Restoration of Form
•Restoration of Function
•Rapid bone healing
•Minimize discomfort
What are the Goals of Treating Mandibular Fractures?
Inflammatory stage
ID the stage of bone healing:
•Clot forms between the bone ends
Inflammatory stage
ID the stage of bone healing:
•Fibroblasts and osteoblasts migrate from periosteum, endosteum, and circulating pluripotent cells
Fibroblast proliferation stage
ID the stage of bone healing:
• collagen is laid down, eventually becomes a callus
Fibroblast proliferation stage
ID the stage of bone healing:
•New capillaries develop, vascularizing the new bone
Remodeling stage
ID the stage of bone healing:
•Callus resorbed
•Osteoclasts resorb excess bone
Remodeling stage
ID the stage of bone healing:
•Ostoblasts build new Haversian canals
Primary Intention
if a Fracture ends are <1mm apart, it will heal by:
Secondary Intention
if a Fracture ends are >1mm apart, it will heal by:
ossification
Excessive forces on healing site causes macro- or micro-mobility which inhibits ______
true
t/f: If there is poor vascularity or oxygen delivery to the tissues, ossification will not occur