general and oral pathology exam 3
1/318
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
319 Terms
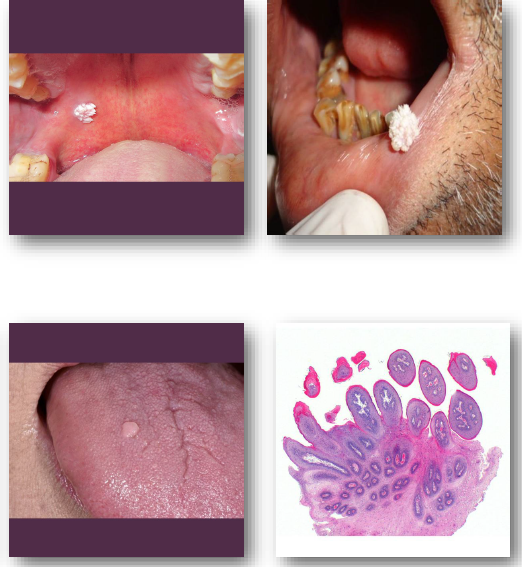
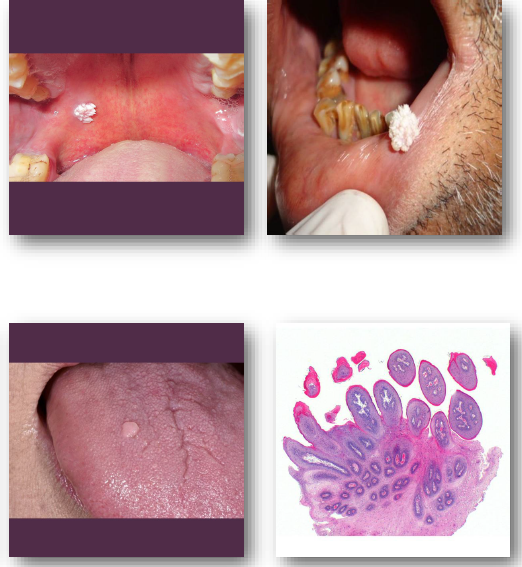
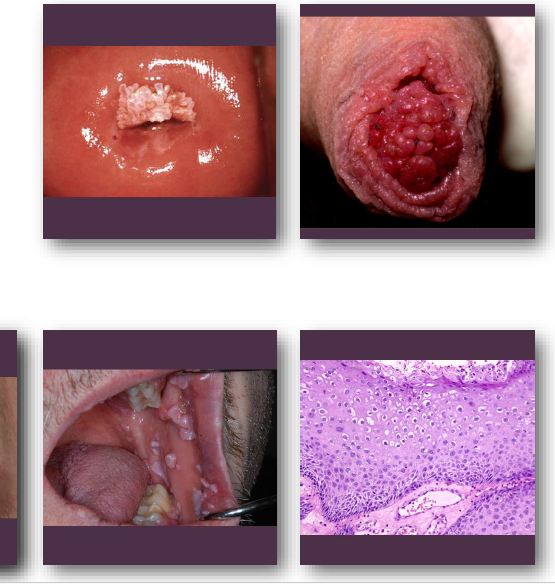
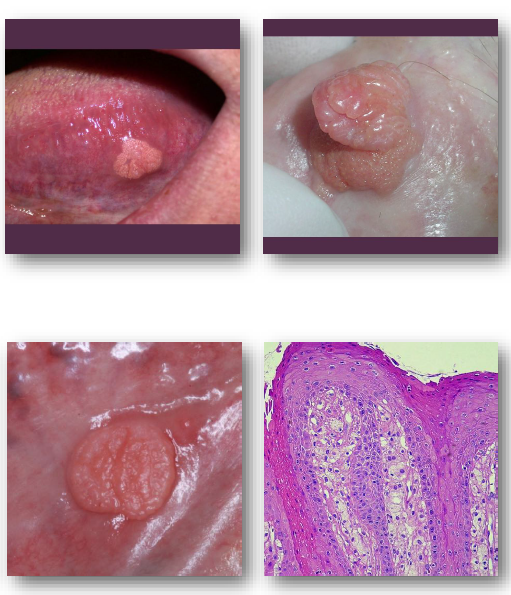
squamous papilloma
benign HPV-induced epithelial proliferation
most linked to HPV types 6 and 11 infection
produces localized papillary epithelial growth
no association with dysplasia or malignancy
host immune status affects lesion persistence
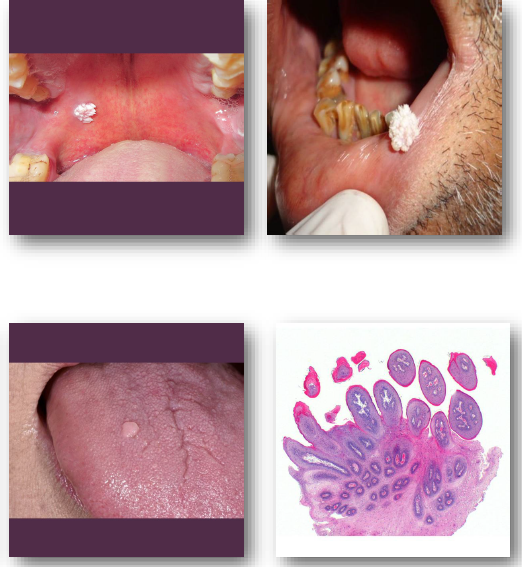
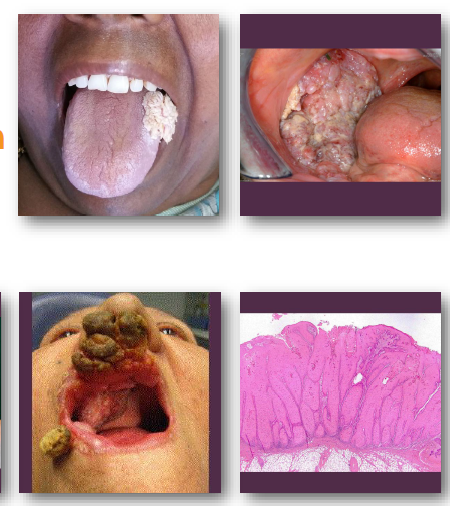
squamous papilloma clinical features
Soft, painless exophytic papillary nodule
•Surface shows classic cauliflower-like pattern (pebbly, finger-like projections)
•Color varies from white to normal mucosa (excess keratin gives white appearance)
•Typically solitary and less than 0.5 cm
•Common on palate, tongue, and lips- particularly areas subject to minor trauma
squamous papilloma management and prognosis
Conservative excision is treatment of choice
• Removal should include lesion base fully (to prevent recurrence)
• Recurrence uncommon after complete removal
• No reports of malignant transformation exist
• Submit tissue for histologic confirmation
verruca vulgaris
• “common wart” not to be confused with sarcoma version
Benign HPV-induced epithelial hyperplasia
• Most commonly associated with HPV type 2
• Lesions spread by contact or autoinoculation
• Occurs more frequently on skin than oral
• Immune response influences lesion duration

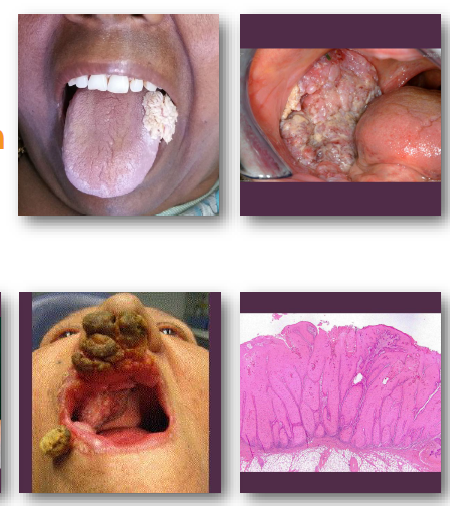
verruca vulgaris clinical features
rough, pebbly papule or small nodule
appears white when present intraorally
may be sessile or pedunculated in form
typically small and stable over time
common on hands, lips, and tongue
histologically intracellular edema

verruca vulgaris management and prognosis
• Many lesions regress spontaneously over time
• Topical or cryotherapy used for skin lesions
• Surgical removal if diagnosis is uncertain
• Recurrence uncommon after adequate treatment
• No evidence of malignant transformation

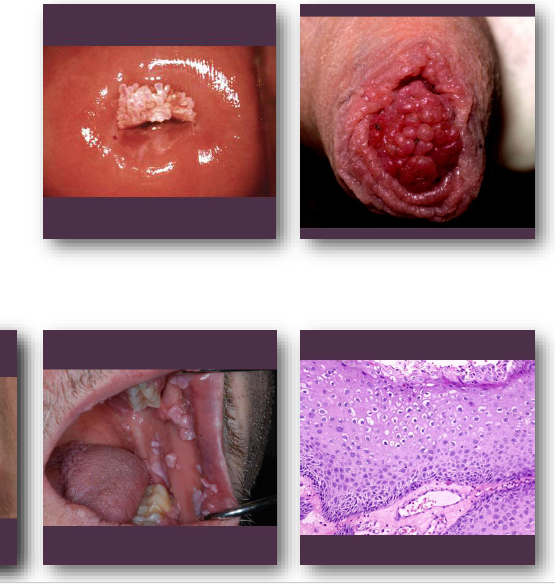
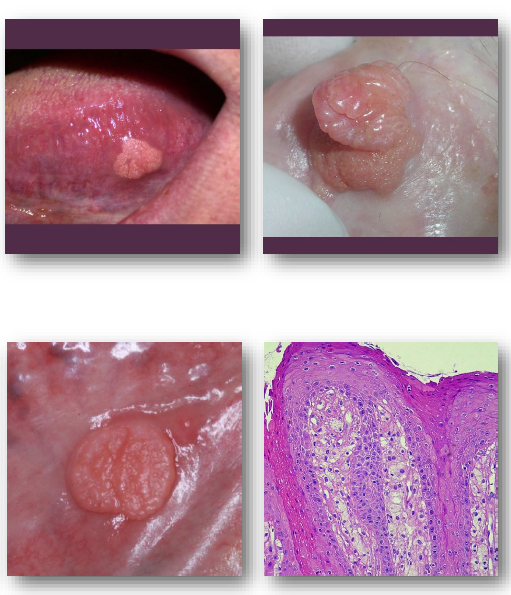
condyloma acuminatum
Benign epithelial proliferation caused by HPV
• Low-risk types 6 and 11 most common cause
• High-risk HPV types linked to dysplasia risk
•Spread by sexual contact or autoinoculation
•More common in young, sexually active adults
sessile
fixed in one place; immobile.
cannot “get up under it”
pedunculated
a growth, tumor, or polyp attached to a surface by a narrow, elongated stalk or stem, rather than being flat against it
compared to broccoli as they both have stalks etc
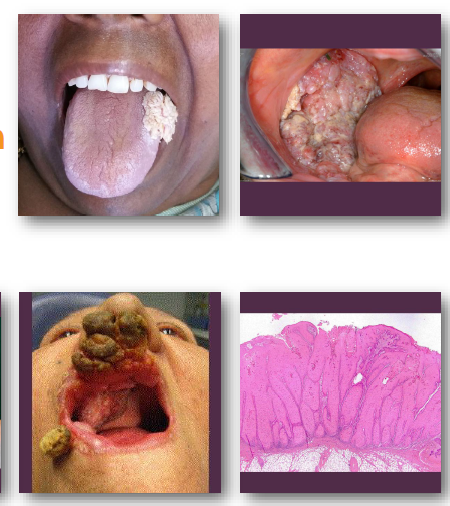
condyloma acuminatum clinical features
•Sessile, pink exophytic mass with broad base
•Surface shows blunted papillary projections
•Often larger than papilloma and clustered
•Color ranges from pink to white or gray
•Common on labial mucosa and lingual frenum
condyloma acuminatum management and prognosis
Excisional biopsy or surgical removal indicated
• Encourage barrier protection and risk reduction
• HPV vaccination helps prevent future infection
• Recurrence possible, especially if immunosuppressed
•Low malignant risk but monitor for changes
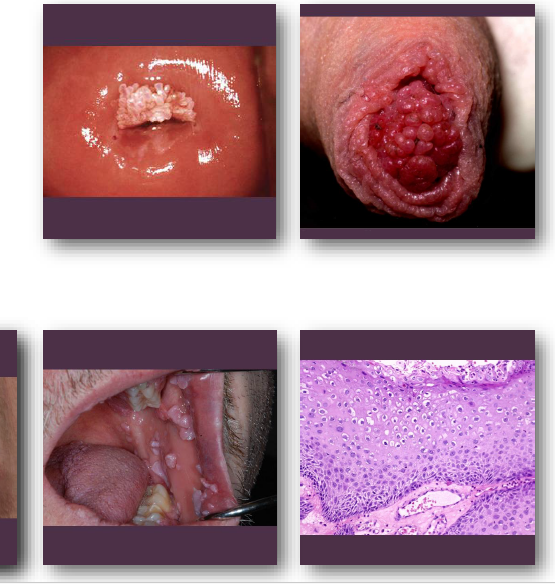
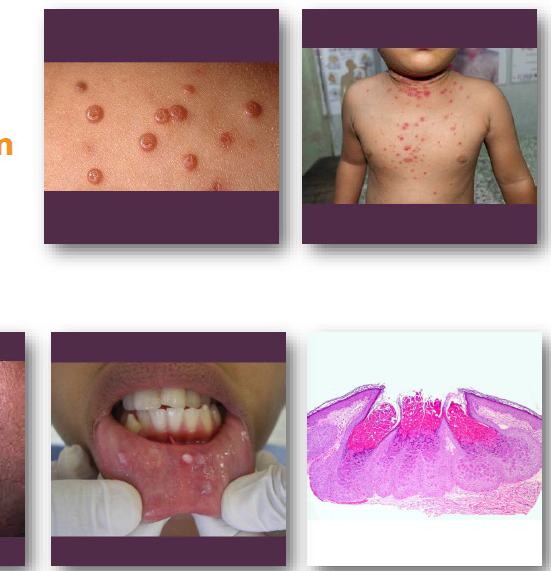
multifocal epithelial hyperplasia
• Benign HPV-related epithelial proliferation
•Associated with HPV types 13 and 32
•Often occurs in children and adolescents
•Linked to genetic and environmental factors
•May regress spontaneously over time

multifocal epithelial hyperplasia clinical features
•Multiple smooth papules on oral mucosa
•Pink, white, or mucosal-colored lesions
•Common on lips, tongue, and buccal mucosa
•Lesions may coalesce into cobblestone pattern (when multiple)
•Usually asymptomatic and slow growing
typically appears flat, not frequently white due to limited keratin

multifocal epithelial hyperplasia management and prognosis
• No treatment needed in most cases
• Excision if lesions are traumatized or persistent
• Cryotherapy or laser for symptomatic lesions
• Recurrence possible after removal or regression
No malignant transformation risk reported

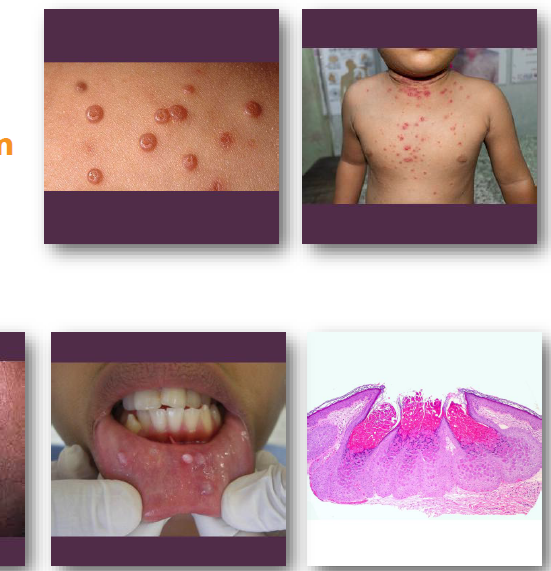
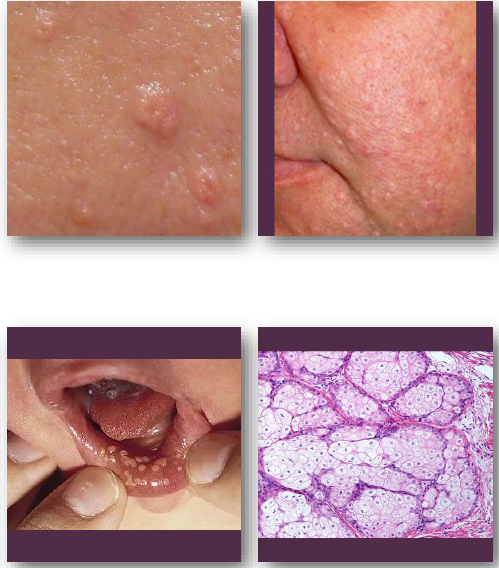
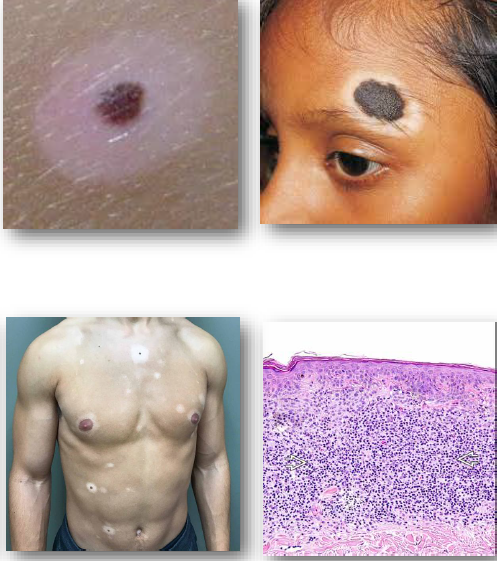
molluscum contagiosum
Viral epithelial lesion caused by poxvirus
•Spread by contact or contaminated surfaces (towels common)
•Common in children and immunocompromised
•Lesions may persist for months to years
Oral involvement is uncommon but possible
commonly called “swimmers wart”
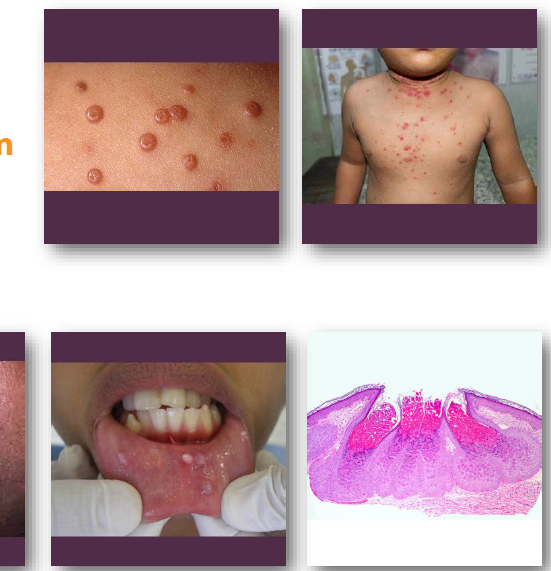
molluscum contagiosum clinical features
• Small, smooth papules with central depression
• Pink or white lesions, often clustered
• Central plug may express curd-like material
•Common on skin of face, neck, and trunk
•Oral lesions may occur on lips or mucosa
molluscum contagiosum management and prognosis
• Many lesions resolve spontaneously over time
•Curettage or cryotherapy for persistent lesions
•Biopsy recommended for oral involvement
•Address underlying immunosuppression if present
•Excellent prognosis with self-limited course
verruciform xanthoma management and prognosis
• Conservative excision is treatment of choice
• Recurrence rare after complete removal
• Biopsy required for definitive diagnosis
• Important to rule out carcinoma clinically
• No malignant transformation reported
verruciform xanthoma overview
• Benign epithelial hyperplasia with foam cells
• Not associated with HPV infection
• Likely reactive to epithelial injury
• Often linked to inflammatory conditions
• Not related to lipid disorders

verruciform xanthoma clinical features
Well-defined sessile lesion with rough surface
• Color ranges from white to yellow or red
• Usually small and less than 2 cm
• Common on gingiva and alveolar mucosa
• May mimic papilloma or carcinoma
NOT VIRAL, COMMON ON GINGIVA AND ALVEOLAR MUCOSA
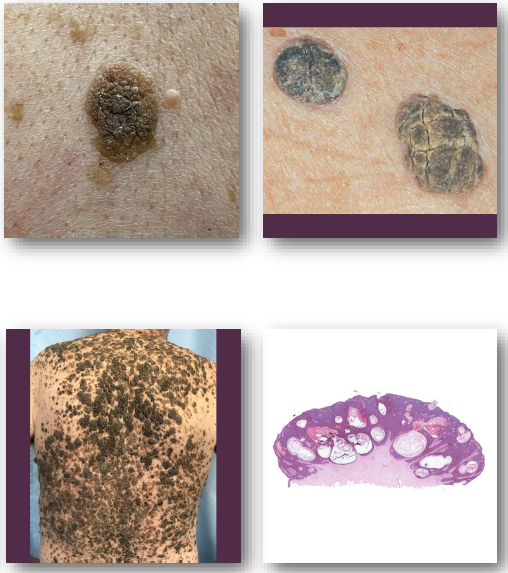
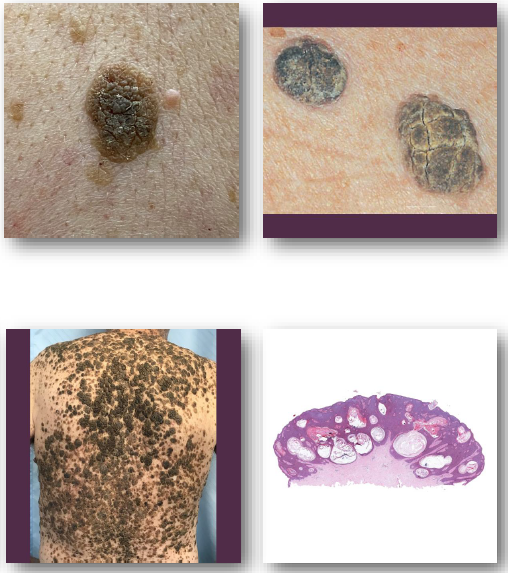
Seborrheic Keratosis
Benign proliferation of epidermal basal cells
• Etiology linked to aging and sun exposure
• Associated with FGFR3 and PIK3CA mutations
• Extremely common in older adult population
• Oral involvement is extremely rare
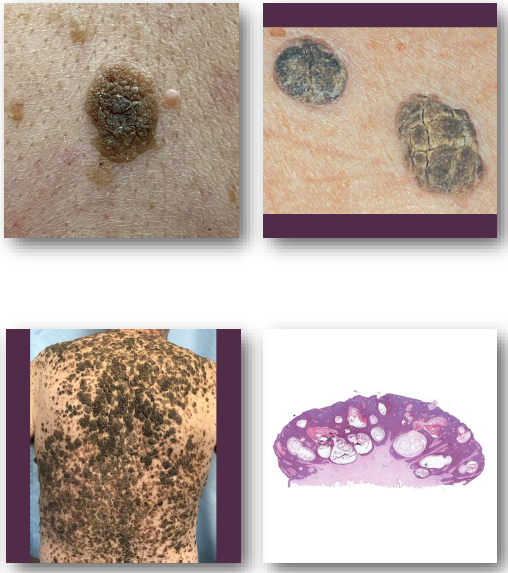
seborrheic keratosis clinical features
Well-demarcated, “stuck-on” appearing plaque
• Surface may be waxy, greasy, or verrucous
• Color ranges from tan to dark brown
• Typically less than 2 cm in size
• Common on face, trunk, and extremities
seborrheic keratosis management and prognosis
No treatment needed if diagnosis certain
• Excision for esthetic or diagnostic reasons
• Refer if lesion is pigmented or atypical
• Oral lesions should be biopsied to confirm
• No malignant transformation potential
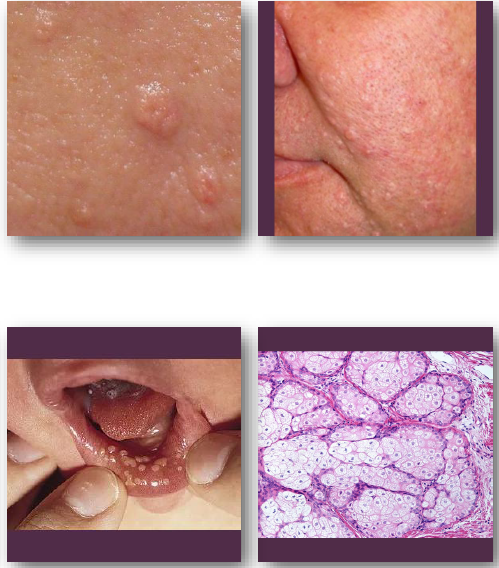
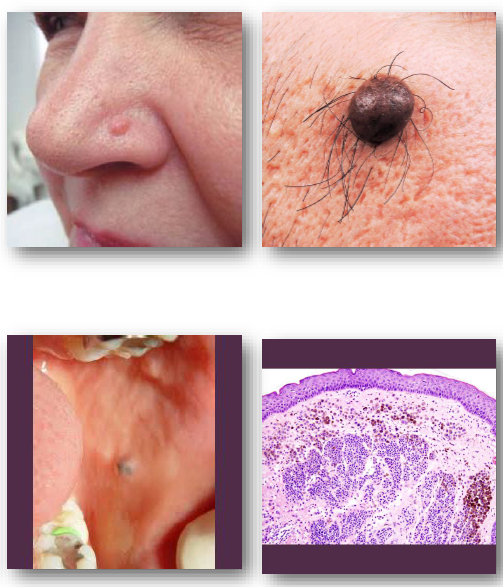
Sebaceous hyperplasia
•Benign proliferation of sebaceous glands
• Etiology linked to aging and hormonal factors
• Associated with medications and immunosuppression
• May occur in Muir-Torre syndrome patients
• Important due to similarity to basal cell carcinoma
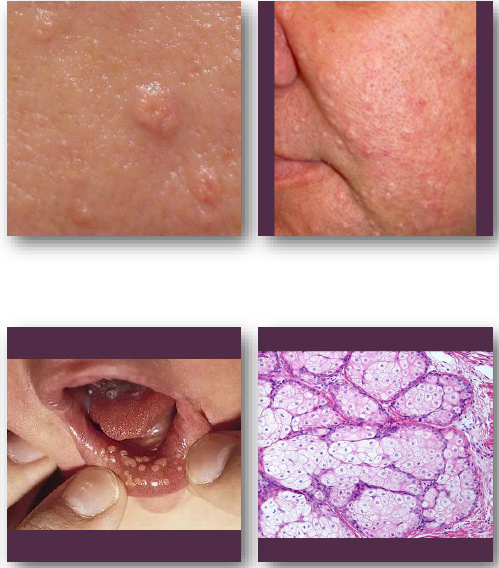
sebaceous hyperplasia clinical features
• Small, soft papules with central depression
• White, yellow, or normal skin color
Often shows central umbilication
•Common on nose, cheeks, and forehead (oil glands!)
•Sebum may be expressed with pressure
sebaceous hyperplasia management and prognosis
• No treatment needed if diagnosis certain
Biopsy if lesion appears atypical
•Refer for cosmetic or uncertain cases
•Laser or radiofrequency may be used
•No malignant transformation risk
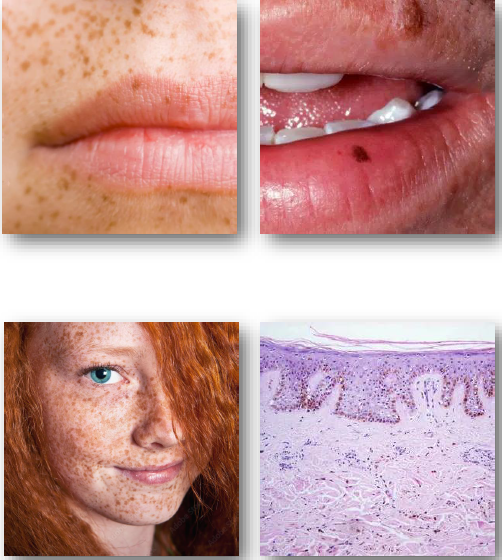
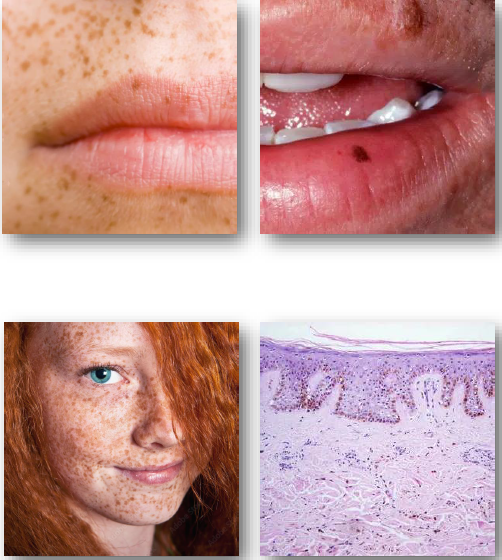
ephelis (freckle)
• Benign hyperpigmented macule of the skin
• Caused by increased melanin without proliferation
• Associated with UV exposure and genetics
•Linked to MC1R gene variants
•Common in fair-skinned individuals
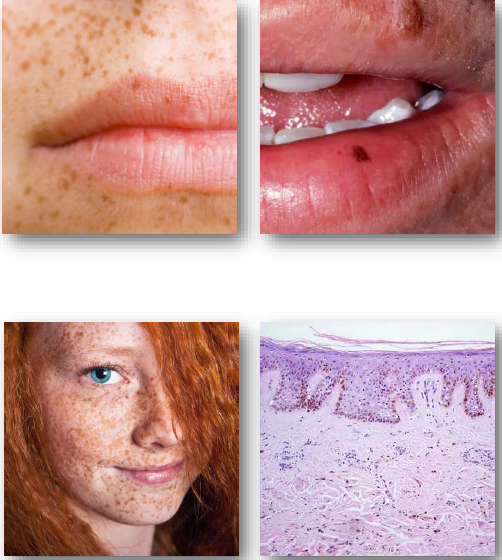
ephelis (freckle) clinical features
• Small, flat, light brown macules
• Sharply defined and uniform in color
• Typically less than 3 mm in size
• Common on face, arms, and back
• Darken with sun exposure over time
ephelis (freckle) management and prognosis
• No treatment required for typical lesions
• Sun protection reduces darkening
• Reassure patient of benign nature
• Refer if lesion appears atypical
• No risk of malignant transformation
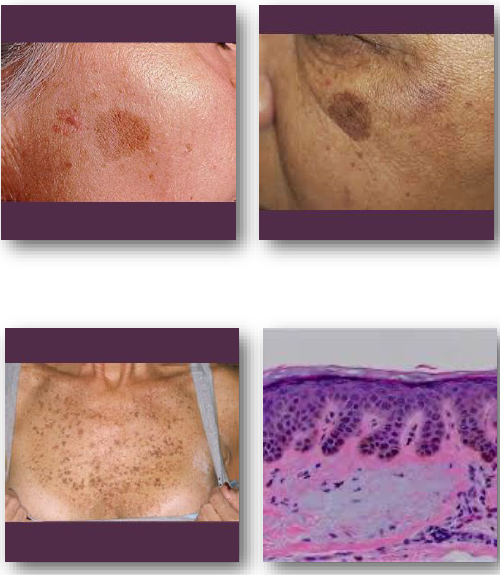
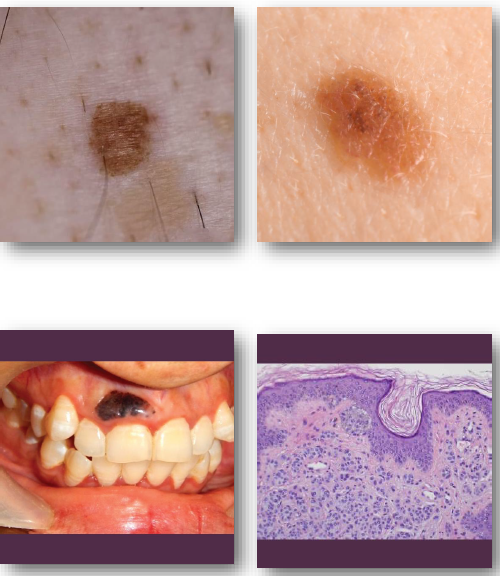
lentigo overview
• Benign pigmented lesion with increased melanocytes
• Includes simplex and actinic (sun-related) types
• Results from increased melanin and melanocyte activity
• Actinic type linked to cumulative UV exposure
• Simplex type occurs without relation to sunlight
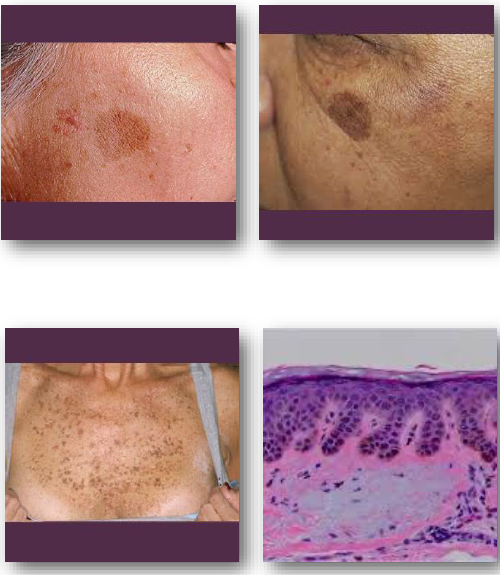
lentigo clinical features
• Well-defined brown macule with uniform color
• Typically darker than freckles and more stable
• Usually less than 5 mm but may be larger
• Common on face, hands, and sun-exposed areas
• Does not fade significantly with sun avoidance
lentigo management and prognosis
• No treatment required for typical lesions
• Biopsy if lesion appears irregular or changing
• Sun protection reduces new actinic lesions but does not regress lesion already present (does not fade over time)
• Cosmetic removal may be performed if desired
• No malignant transformation potential exists
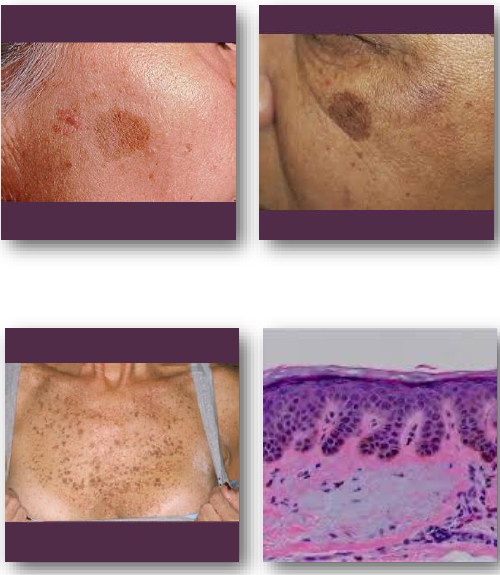
actinic type lentigo
linked to cumulative UV exposure
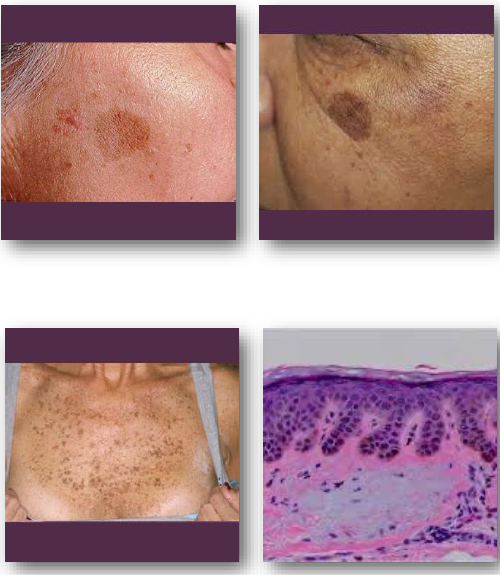
lentigo simplex type
occurs without relation to sunlight
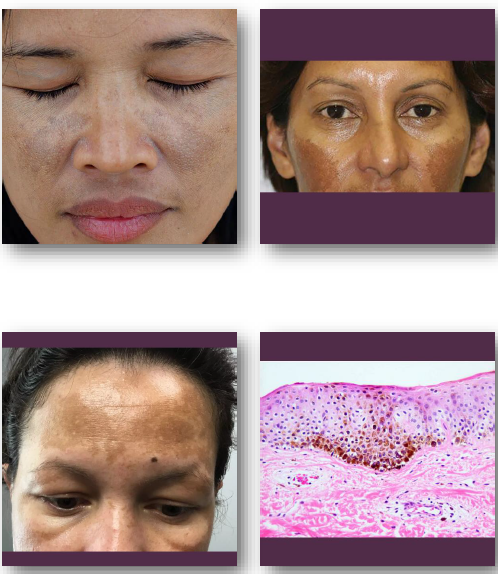
melasma overview
Acquired hyperpigmentation of sun-exposed facial skin
•Caused by UV exposure and hormonal influences
•Associated with pregnancy and hormonal therapy
•More common in women with darker complexions
•Results from increased melanin production

melasma clinical features
• Symmetric brown or gray macules on the face
• Common on cheeks, forehead, and upper lip
• Gradual onset with continued sun exposure
• Lesions may darken over time
•Typically asymptomatic but cosmetically concerning
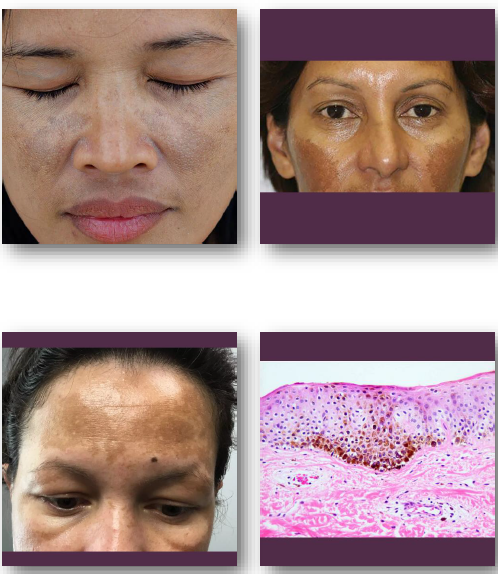
melasma management and prognosis
• Sun protection is essential for control
• Topical agents used to reduce pigmentation
• Avoid hormonal or medication triggers
•Dermatology referral for persistent cases
•Chronic condition with tendency to recur

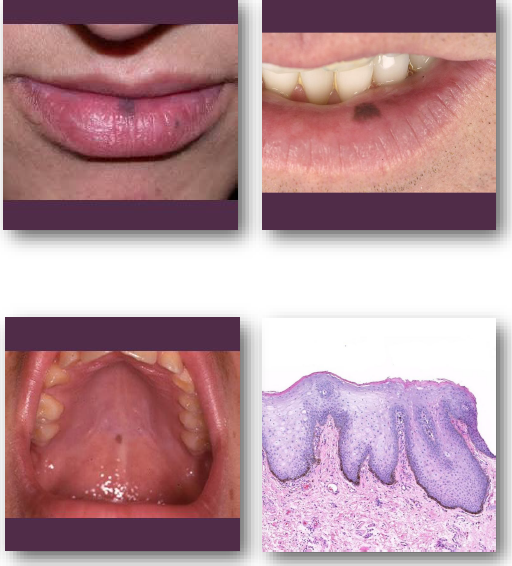
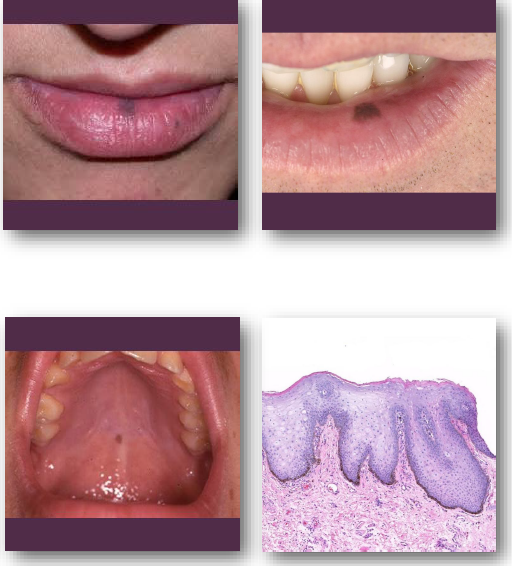
oral melanotic macule
• Benign focal increase in melanin deposition
• May show slight increase in melanocyte number
• Not related to ultraviolet exposure intraorally
• Most common oral melanocytic lesion
• Represents localized melanocytic hyperactivity
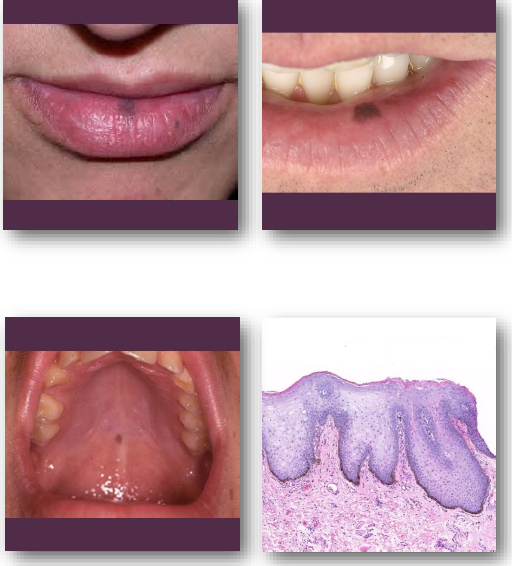
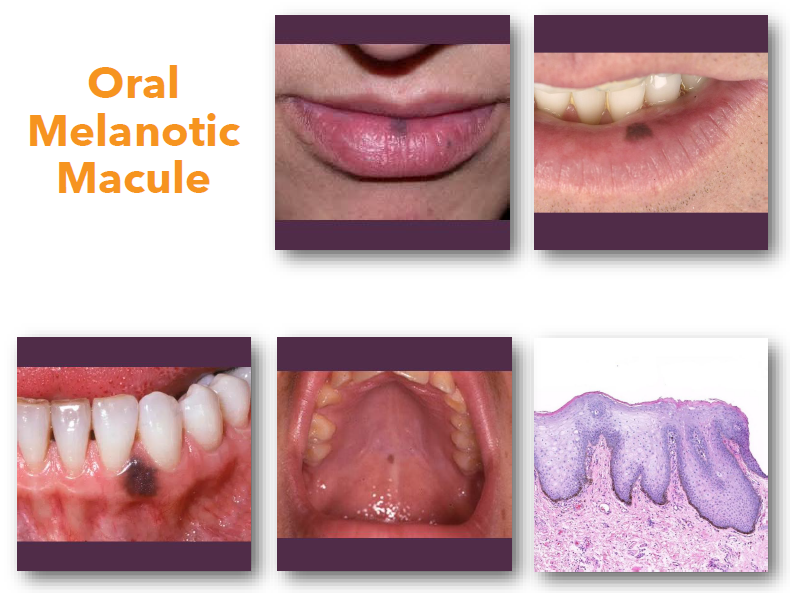
oral melanotic macule clinical features
• Flat well-defined brown mucosal macule
• Usually solitary and uniformly pigmented
• Typically, less than 7 mm in greatest size
• Common on lip, gingiva, and buccal mucosa
• Color remains stable over time

oral melanotic macule: management and prognosis
• Biopsy recommended for intraoral pigmented lesions to confirm diagnosis
• Observe labial lesions if diagnosis is certain
• Document size and color at baseline
• Refer if lesion shows change over time
• No malignant transformation has been reported
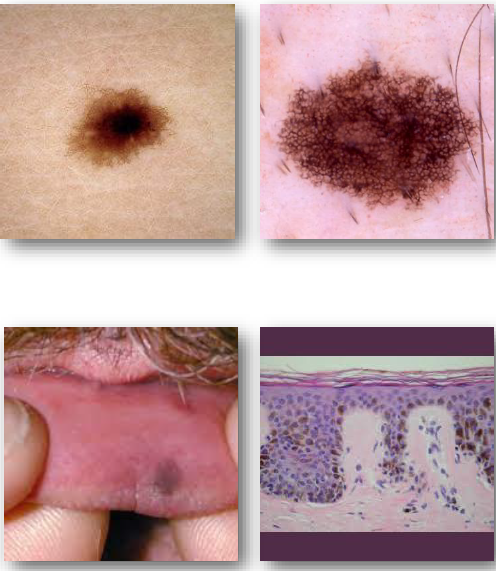
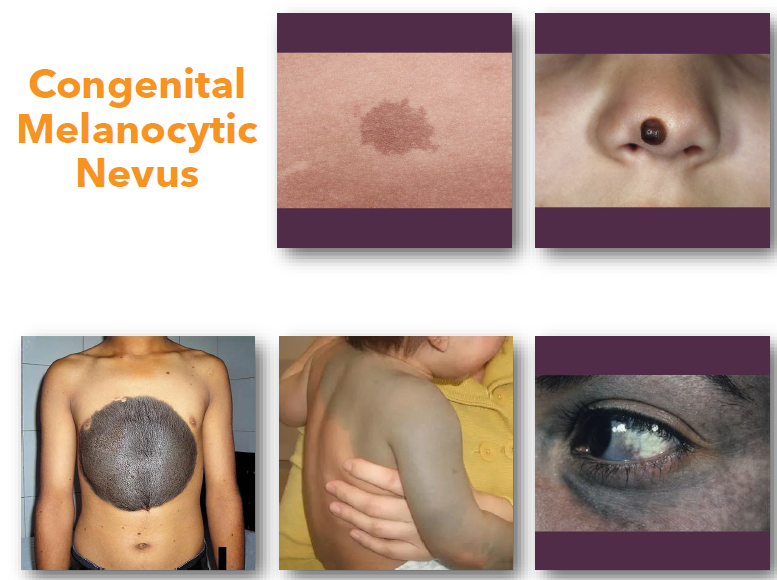
melanocytic nevi
• Benign proliferation of melanocytes in epithelium
• Includes junctional, compound, and intradermal types
• Associated with BRAF or NRAS gene mutations
• Common on skin but rare in oral cavity
• Represents developmental melanocytic lesion
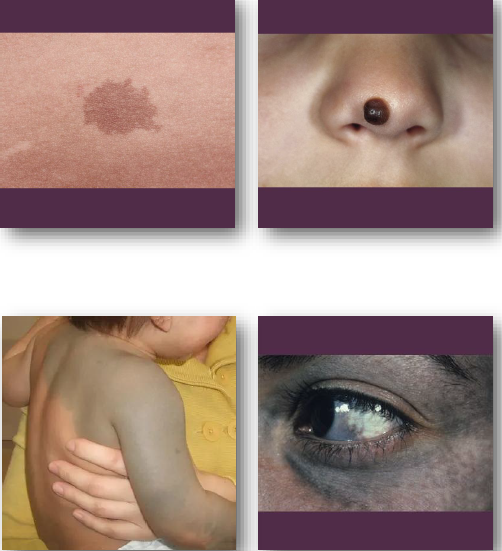
melanocytic nevi clinical features
Small well-defined pigmented macule or papule
•Color ranges from tan to dark brown
•May be flat or slightly elevated in appearance
•Usually stable in size and color over time
•More common on skin than oral mucosa
melanocytic management and prognosis
Biopsy recommended for oral pigmented lesions
•Observe cutaneous lesions if typical in appearance
•Refer if lesion changes in size or color
•Document baseline appearance carefully
•Small risk of malignant transformation exists
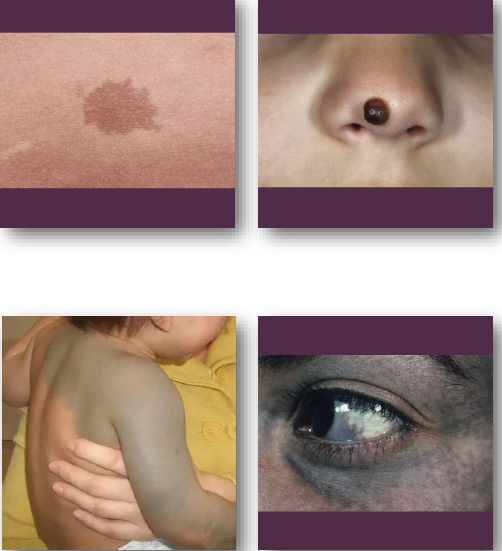
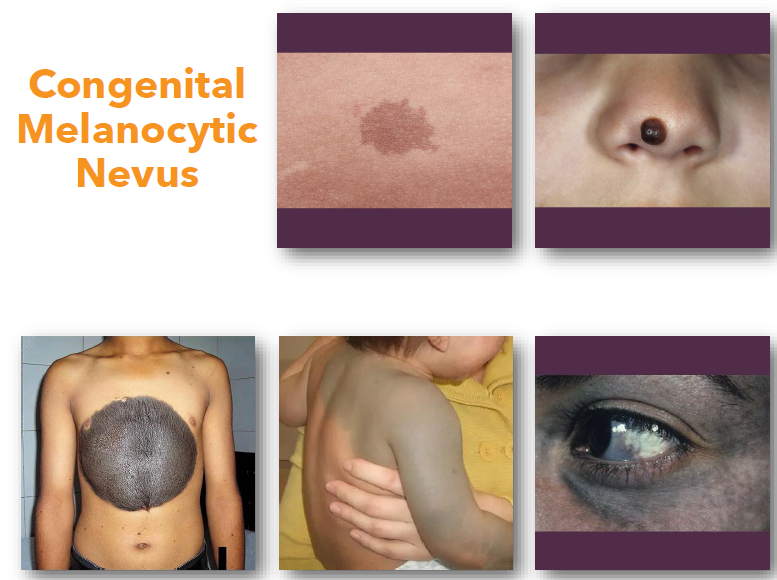
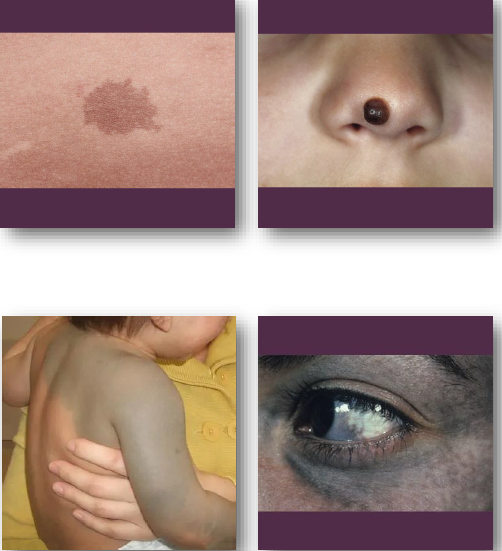
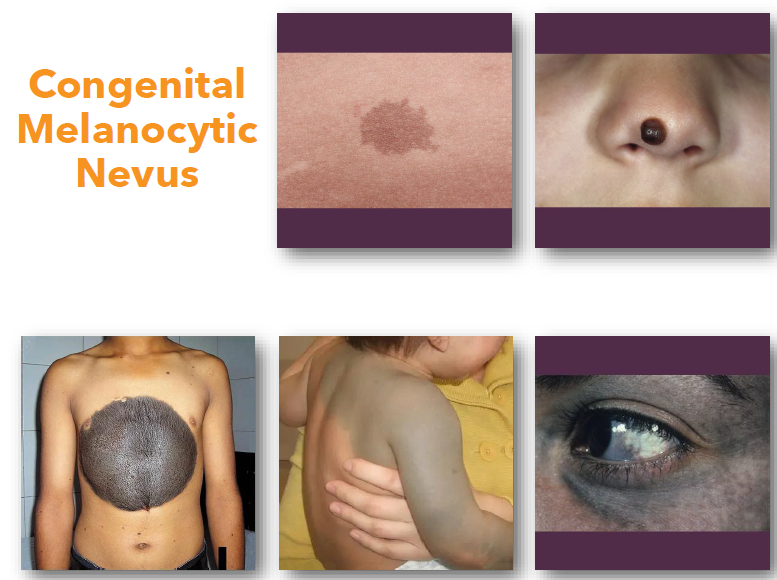
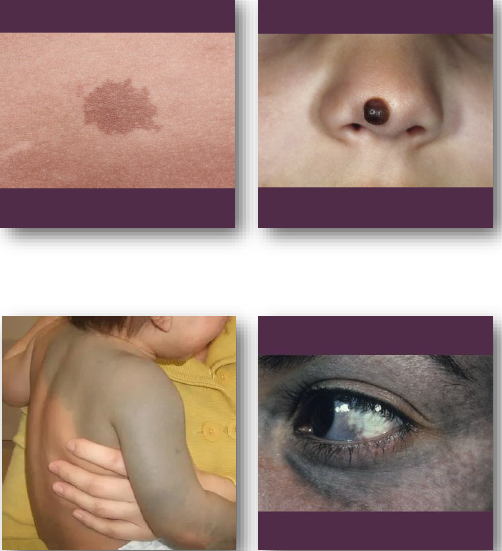
congenital melanocytic nevus
junctional nevi
usually flat
singular
all melanocytes at junction of epithelium and connective tissue
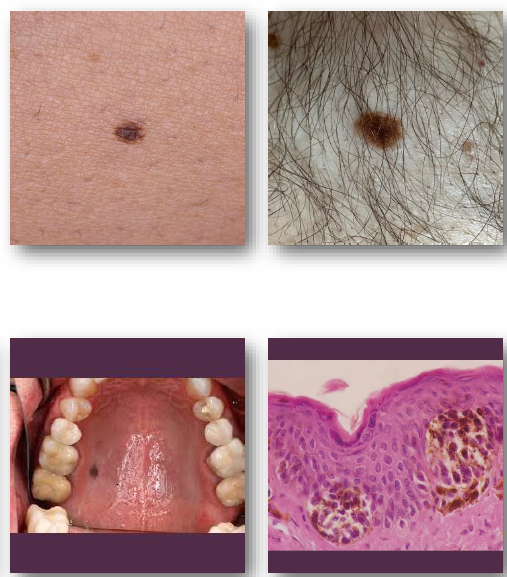
dermal nevi
more into dermis than epidermis
limited pigment
fleshy appearance
compound nevi
characteristics of both dermal and junctional nevi
halo nevus
inflammatory reaction that causes depigmentation around nevus
spitz nevus
more common in children
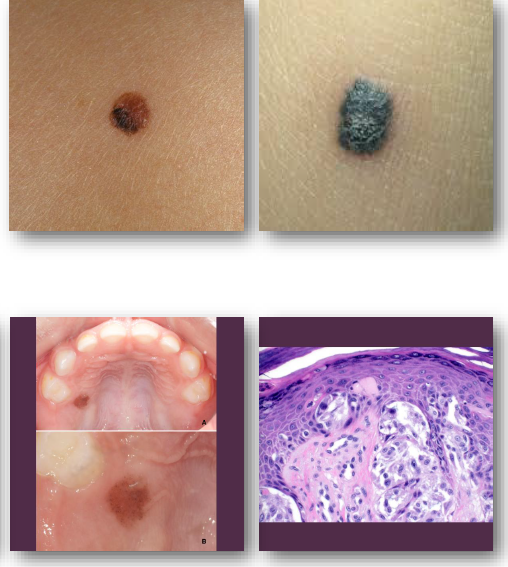
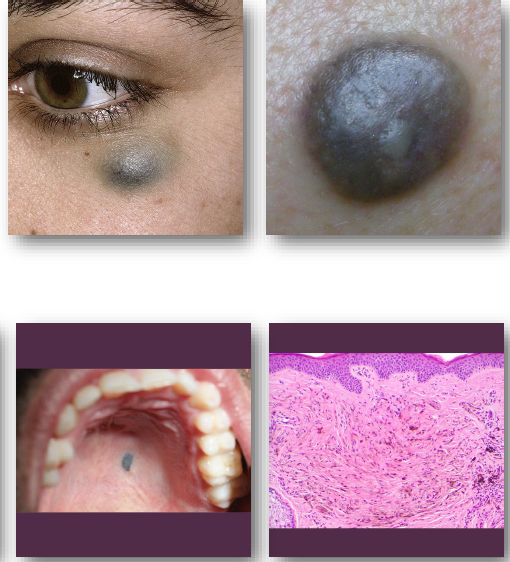
blue nevus
blue-grey appearance
common site is on palate
appears like amalgam tattoo
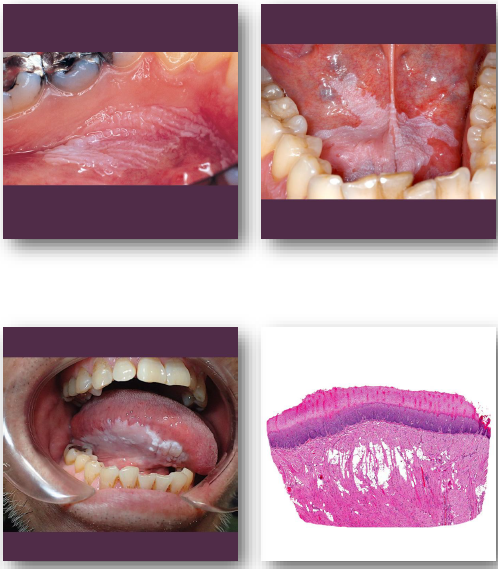
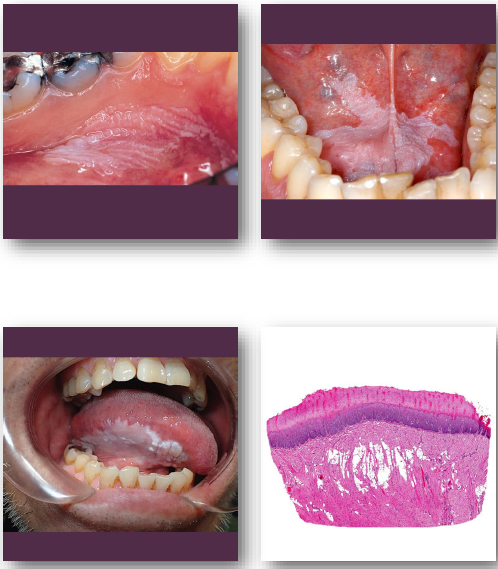
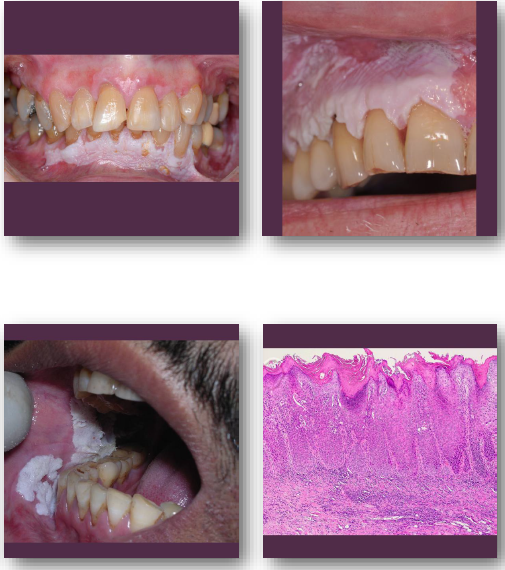
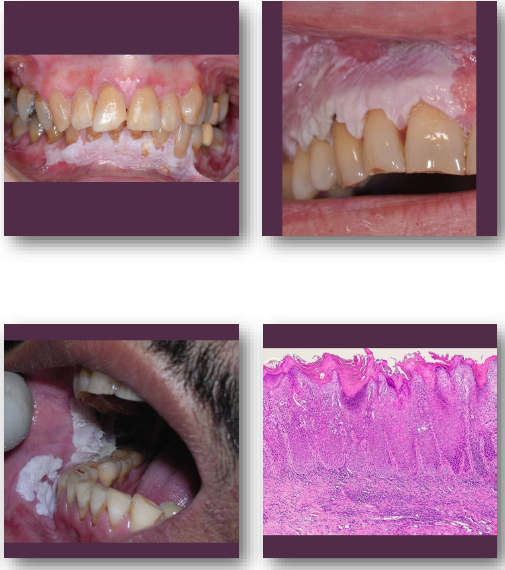
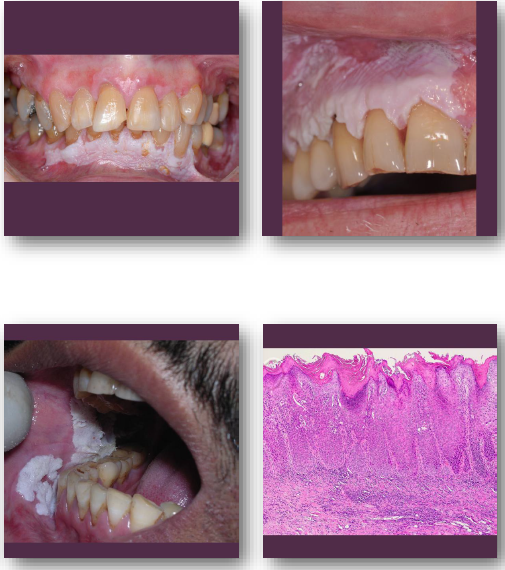
leukoplakia (white plaque)
•White plaque of uncertain malignant potential
•Cannot be wiped off or clinically defined
•Strongly associated with tobacco exposure
•Represents spectrum from keratosis to dysplasia
•Diagnosis requires exclusion of other causes
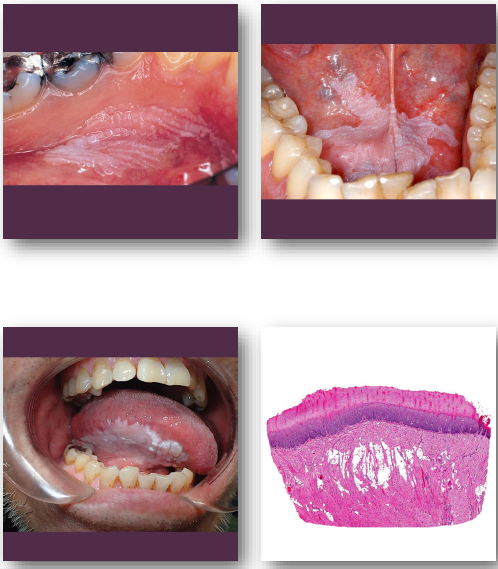
leukoplakia clinical features
• White patch or plaque with variable thickness
• Surface may be smooth, fissured, or verrucous
• Cannot be wiped off during clinical exam
• Common on buccal mucosa, tongue, and alveolar ridge of edentulous patients
• Usually asymptomatic and incidentally found
verrucous
refers to warty, rough, or elevated skin lesions
leukoplakia management and prognosis
• Biopsy required to evaluate degree of dysplasia
•Eliminate risk factors such as tobacco use
•Surgical removal for dysplastic lesions
•Requires regular follow-up and monitoring
•Variable malignant transformation risk exists
proliferative verrucous leukoplakia
• Aggressive multifocal variant of leukoplakia
•Not strongly associated with tobacco exposure
•Progressive and persistent over long duration
•High risk for malignant transformation
•More common in older female patients
proliferative verrucous leukoplakia clinical features
• Multifocal white plaques with verrucous surface
•Slowly enlarging and spreading over time
•Often involves gingiva and alveolar mucosa
•May develop red areas or ulceration
•Persistent despite multiple treatments
proliferative verrucous leukoplakia management and prognosis
• Multiple biopsies required during progression
• Surgical treatment often unsuccessful long term
• Requires lifelong follow-up and surveillance
• High recurrence rate after treatment
• Very high malignant transformation risk
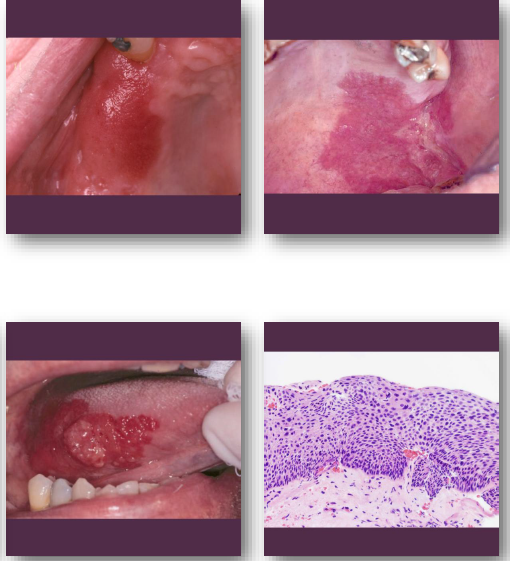
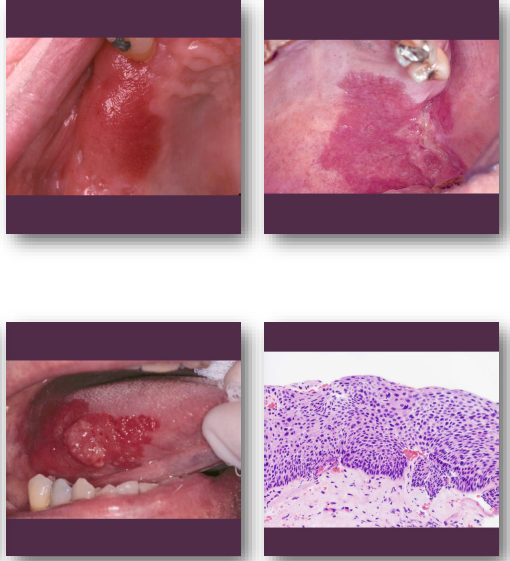
erythroplakia overview
• Red patch with very high malignant potential
•Often represents severe dysplasia or carcinoma
• Less common but more dangerous than leukoplakia
•Strongly linked to tobacco and alcohol use
•Requires immediate diagnostic evaluation
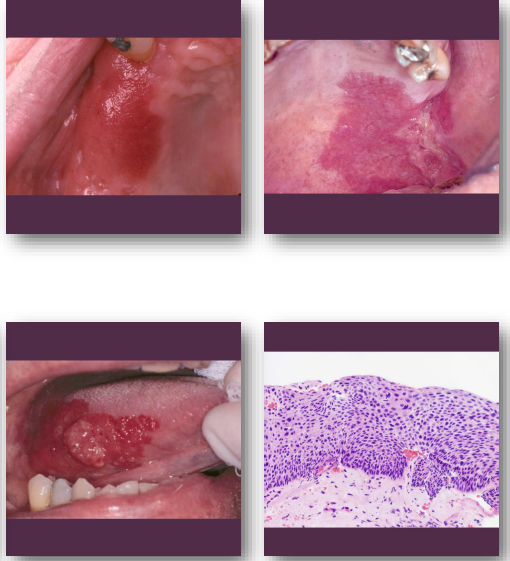
erythroplakia clinical features
Bright red velvety mucosal patch
• Well-defined but may show irregular borders
• Often flat without early ulceration
• Common on floor of mouth and soft palate
• Usually asymptomatic in early stages
erythroplakia management and prognosis
• Immediate biopsy required for diagnosis
• Often reveals severe dysplasia or carcinoma
• Surgical excision usually indicated
• Close follow-up required after treatment
• High risk of malignant progression
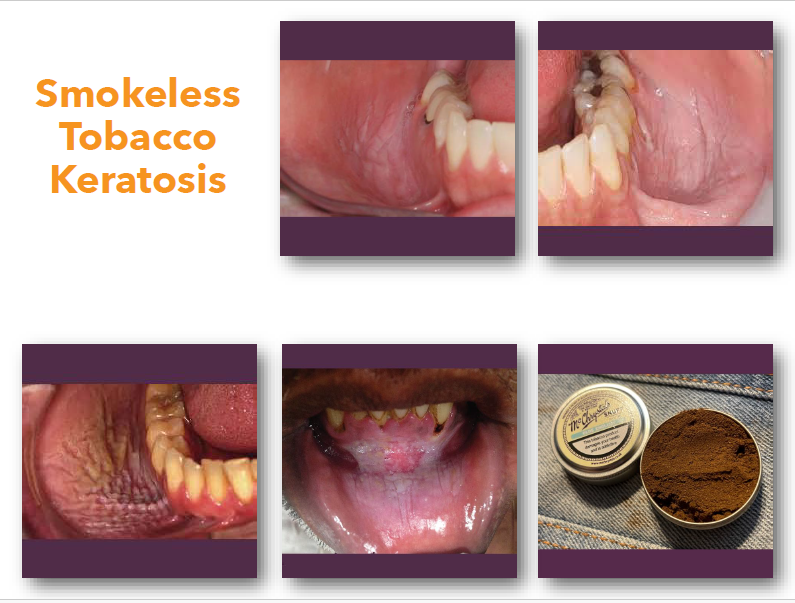
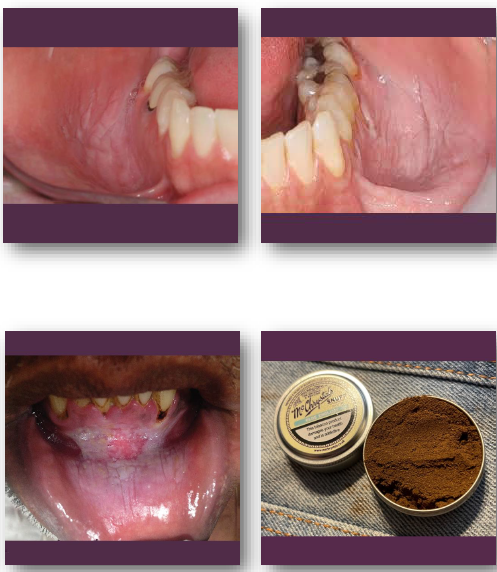
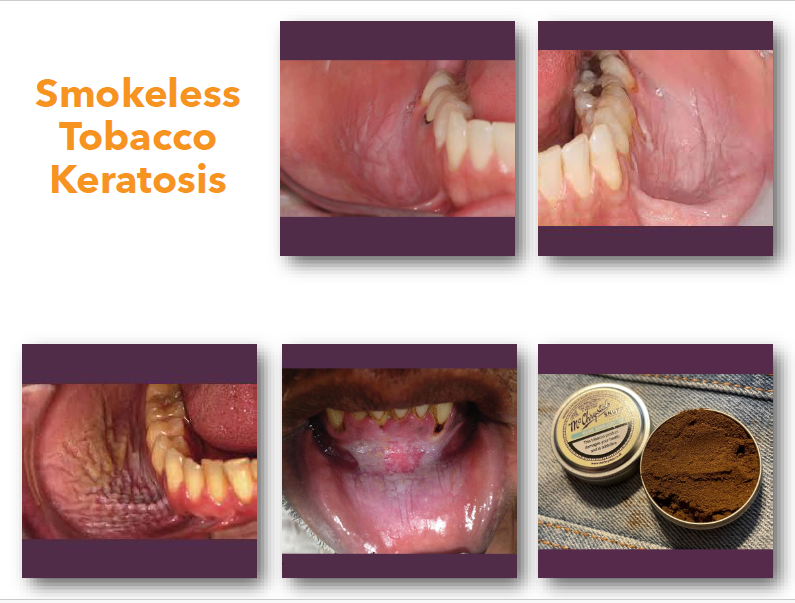
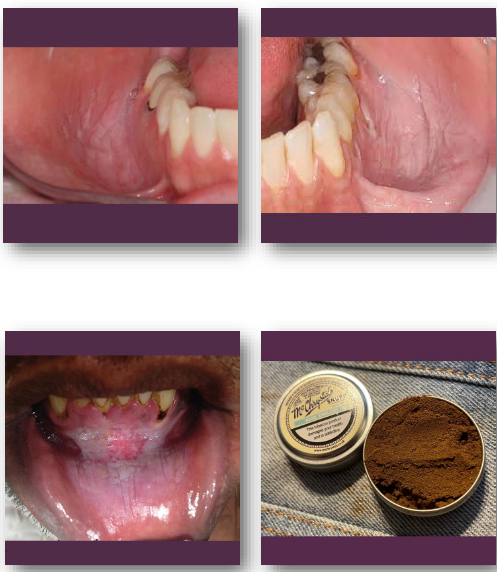
smokeless tobacco keratosis overview
Reactive epithelial change from smokeless tobacco use
•Caused by chronic chemical and mechanical irritation
•Common in areas of tobacco placement
•Represents reversible keratotic mucosal change
•May progress to dysplasia in long-term users
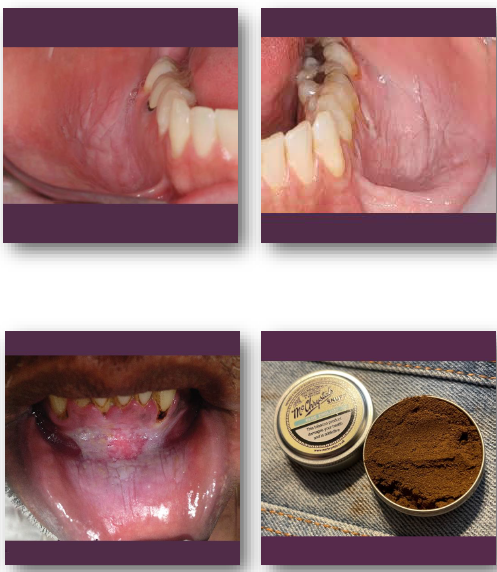
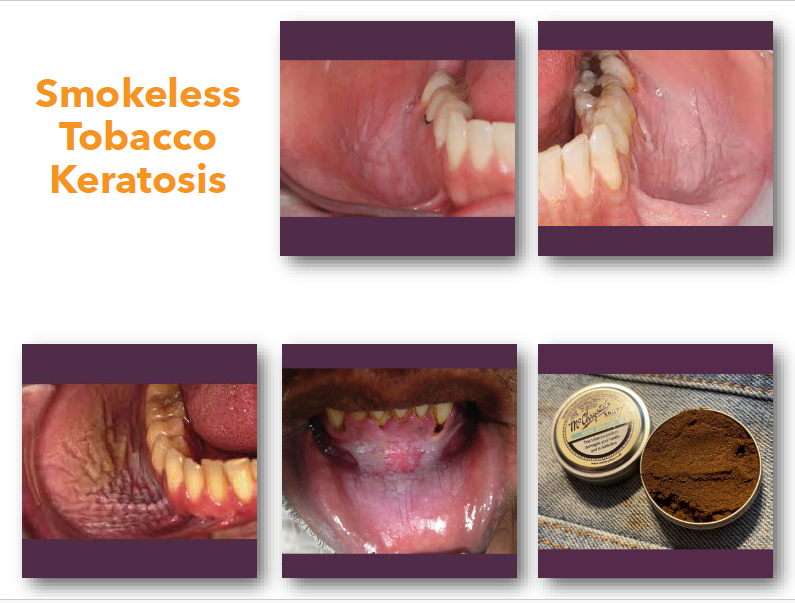
smokeless tobacco keratosis clinical features
• White or gray plaque at tobacco placement site
• Surface may appear wrinkled or fissured
• Common in mandibular vestibule or sulcus
• Lesion thickness varies with duration of use
• Usually asymptomatic
smokeless tobacco keratosis management and prognosis
•Discontinue smokeless tobacco use immediately
•Lesions often resolve after habit cessation
•Biopsy if lesion persists after cessation
•Monitor for dysplastic changes over time
•Low malignant risk if habit is discontinued
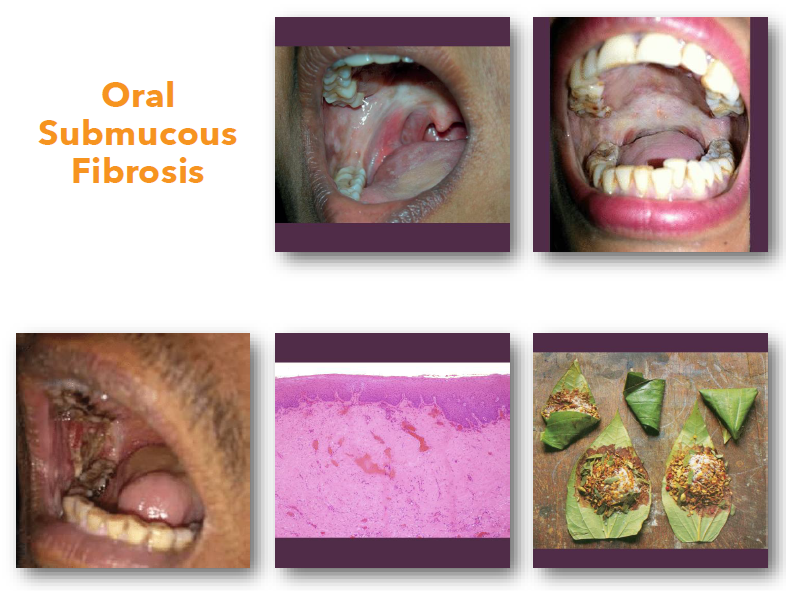
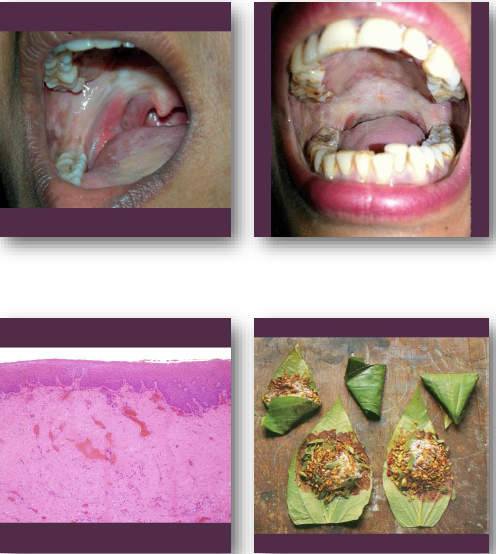
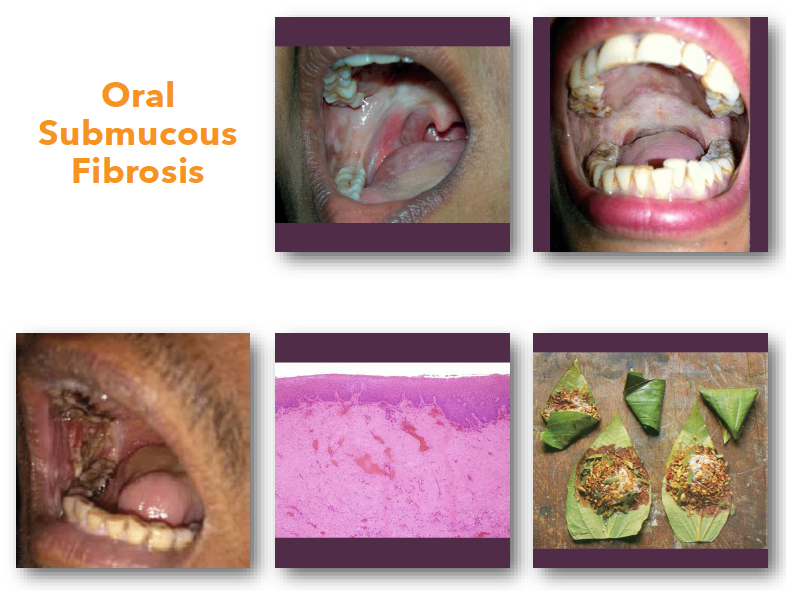
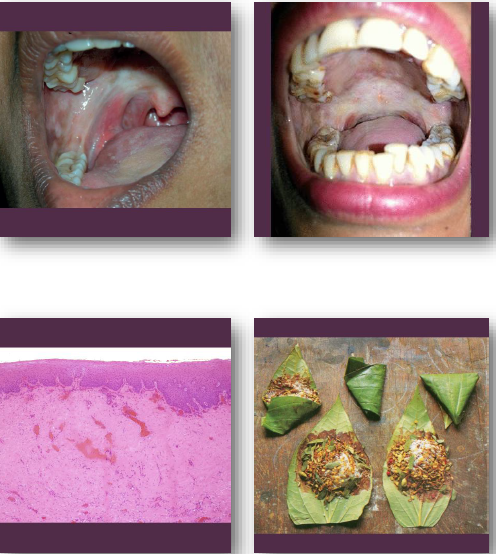
oral submucous fibrosis overview
• Chronic progressive fibrosis of oral mucosa
• Strongly associated with areca nut use
• Leads to reduced elasticity and function
• Considered a premalignant condition
• Common in South Asian populations
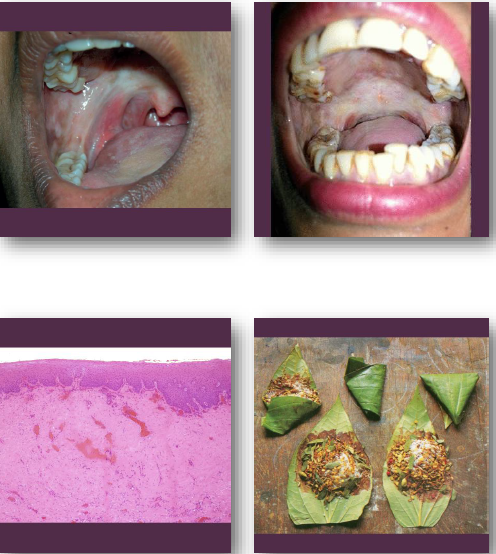
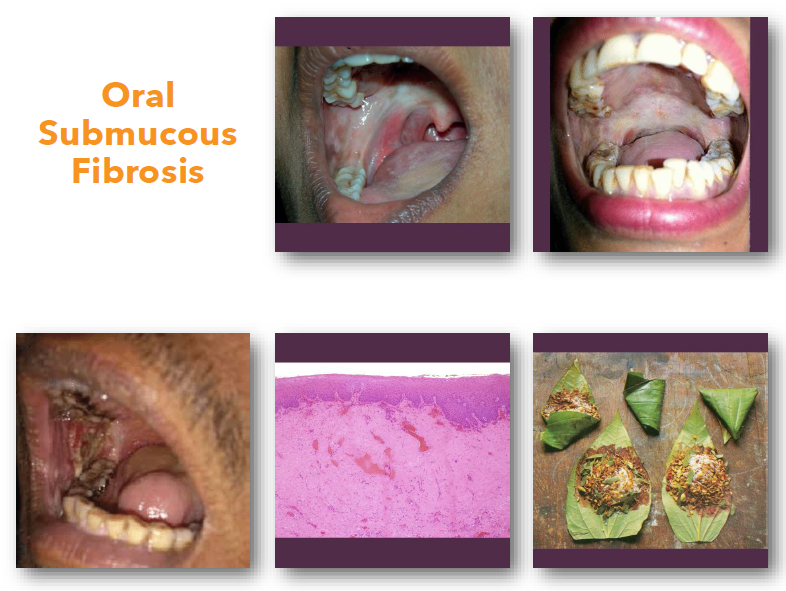
oral submucous fibrosis clinical features
• Blanched stiff oral mucosa with fibrosis
•Progressive reduction in mouth opening
•Burning sensation with spicy foods
•Palpable fibrous bands in mucosa
•Reduced tongue mobility in advanced cases.
oral submucous fibrosis management and prognosis
•Eliminate areca nut and irritant habits
•Nutritional support and medical therapy
•Physical therapy to improve mouth opening
•Requires close monitoring for malignancy
•Significant transformation risk over time
corrugation
a series of parallel ridges and grooves or alternating wrinkles on surface
commonly seen in smokeless tobacco keratosis
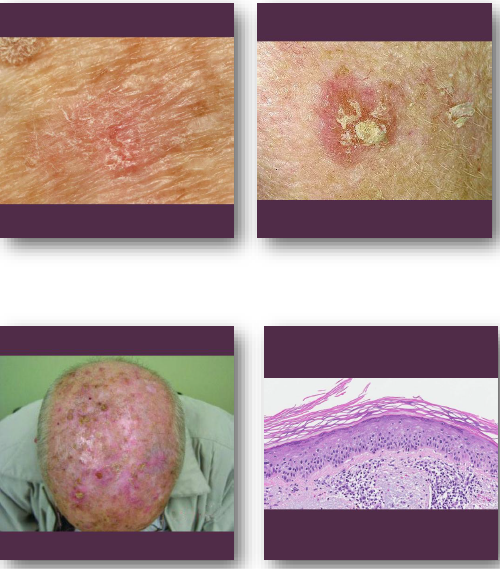
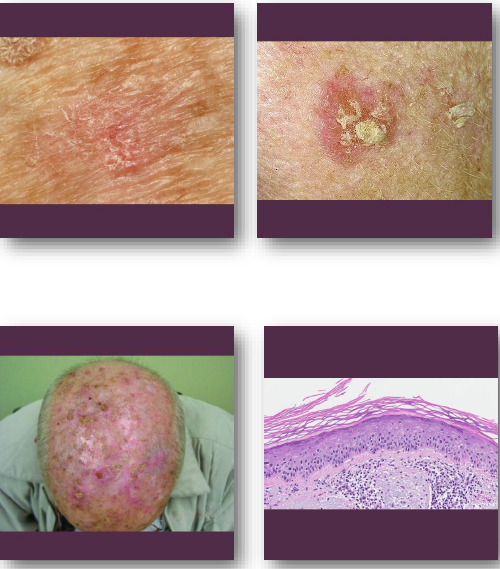
actinic keratosis overview
•Premalignant lesion caused by chronic UV exposure
•Represents early epithelial dysplasia of skin
•Strongly associated with sun-damaged skin
•Precursor to cutaneous squamous cell carcinoma
•Common in fair-skinned older adults
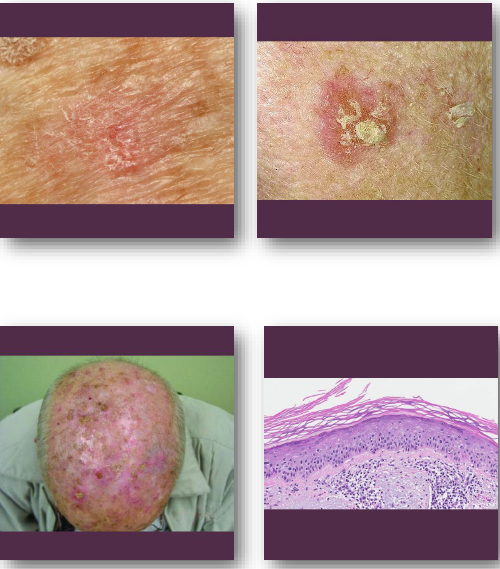
actinic keratosis clinical features
• Rough scaly patch on sun-exposed skin surfaces
• Color ranges from red to tan or brown
• Often easier to feel than to see
• Common on face, ears, and hands
• May be tender or completely asymptomatic
actinic keratosis management and prognosis
• Treated with cryotherapy or topical agents
• Sun protection prevents development of lesions
• Biopsy if lesion thickens or ulcerates
• May progress to squamous cell carcinoma
• Excellent prognosis with early treatment
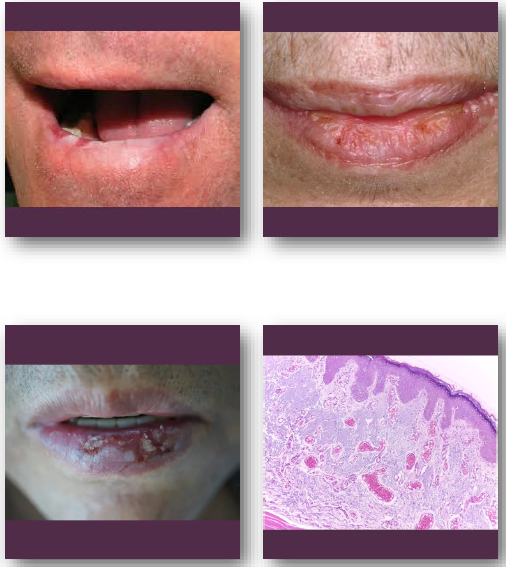
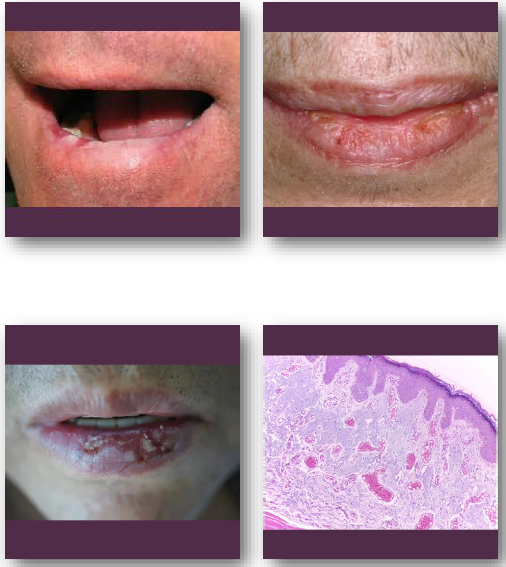
actinic cheilitis overview
•Premalignant lesion of lip from chronic UV exposure
• Represents epithelial dysplasia of vermilion border
•Strongly associated with fair skin and sun exposure
•Most commonly affects lower lip region
•Considered precursor to lip squamous cell carcinoma
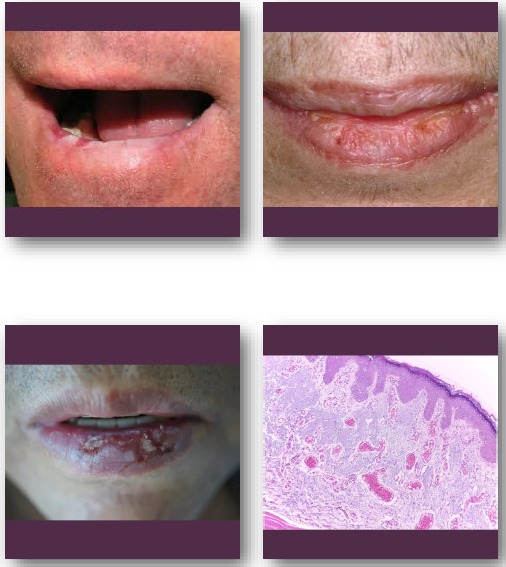
actinic cheilitis clinical feature
•Atrophic, dry, or scaly appearance of lower lip
•Blurring of vermilion border is common finding
•May show fissures, ulceration, or crusting
•Color ranges from pale to erythematous areas
•Usually chronic and slowly progressive
actinic cheilitis management and prognosis
•Biopsy recommended for suspicious or persistent areas
•Sun protection is essential preventive measure
•Topical therapy or surgical treatment may be used
•Regular follow-up required due to cancer risk
•Risk of progression to squamous cell carcinoma
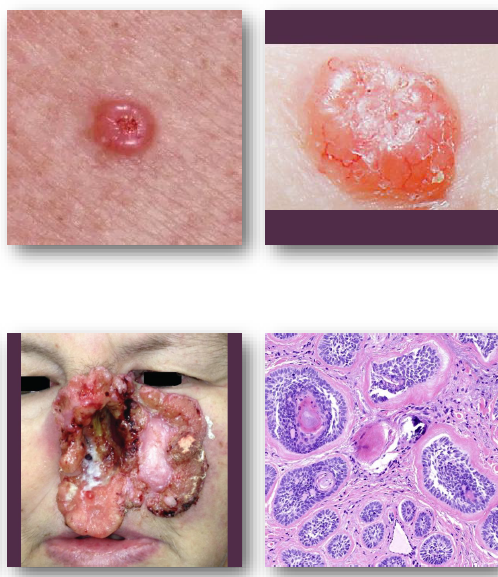
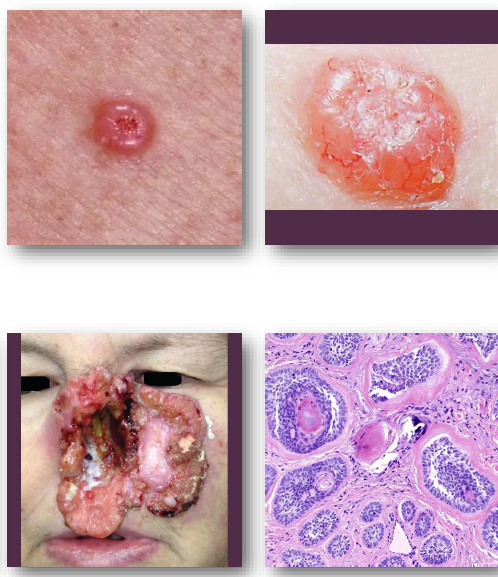
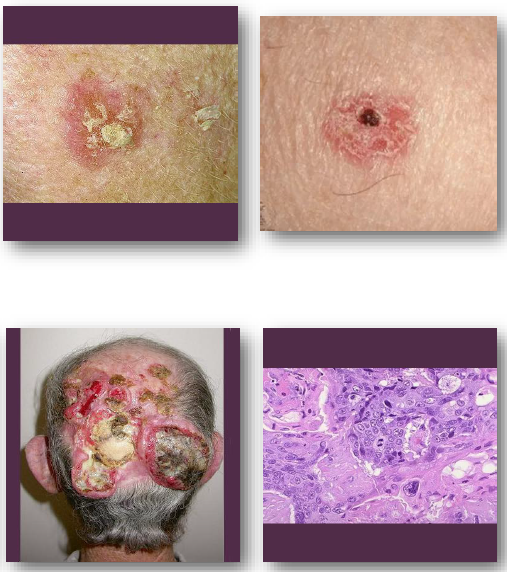
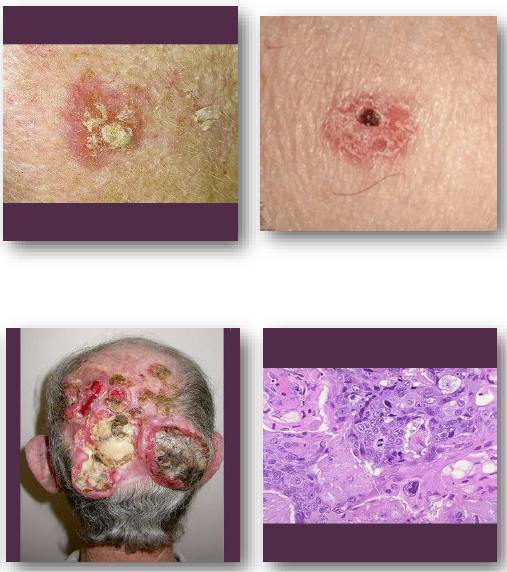
basal cell carcinoma overview
• Most common malignant tumor of the skin
• Arises from basal layer of epithelium
• Strongly associated with UV exposure
• Locally invasive but rarely metastasizes
• Common in fair-skinned individuals
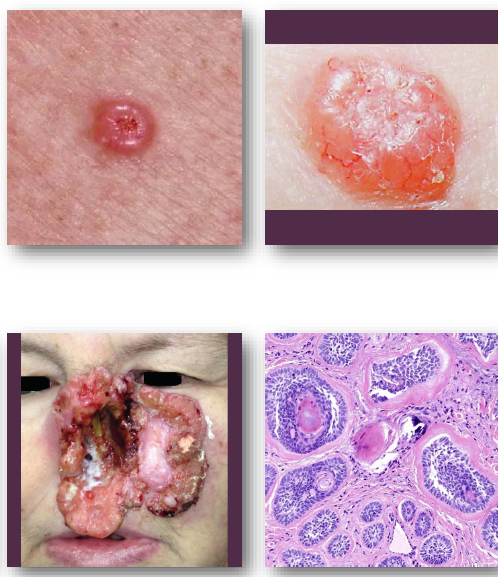
basal cell carcinoma clinical features
pearly papule with rolled and raised borders
central ulceration may be present
surface shows fine blood vessels
common on face and nose region
slow-growing but locally destructive
basal cell carcinoma management and prognosis
Surgical excision is treatment of choice
•Mohs surgery used for high-risk areas
•Excellent prognosis with early detection
•Recurrence possible if incompletely removed
•Rarely metastasizes to distant sites
cutaneous squamous cell carcinoma overview
•Malignant tumor of keratinizing epithelium
•Strongly linked to chronic UV exposure
•May arise from actinic keratosis lesions
•More aggressive than basal cell carcinoma
•Risk increased in immunocompromised patients
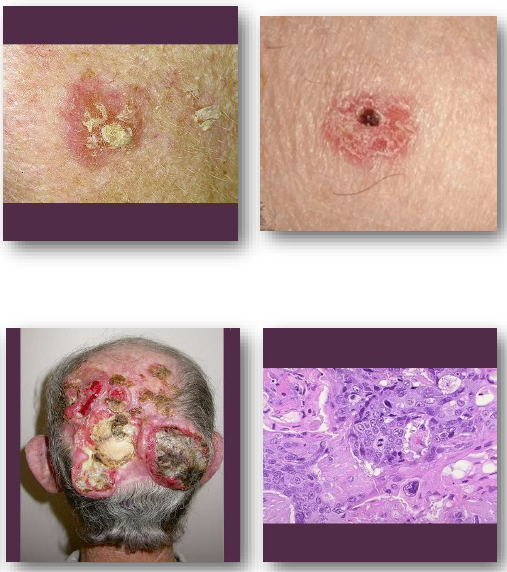
cutaneous squamous cell carcinoma clinical features
•Firm scaly or ulcerated skin lesion
•May present as non-healing ulcer
•Surface may crust or bleed easily
•Common on sun-exposed areas
•Often grows faster than basal cell carcinoma
cutaneous squamous cell carcinoma management and prognosis
•Surgical excision with adequate margins required
•Radiation therapy used in selected cases
•Early detection improves clinical outcomes
•Greater risk of metastasis than BCC
•Requires close follow-up after treatment

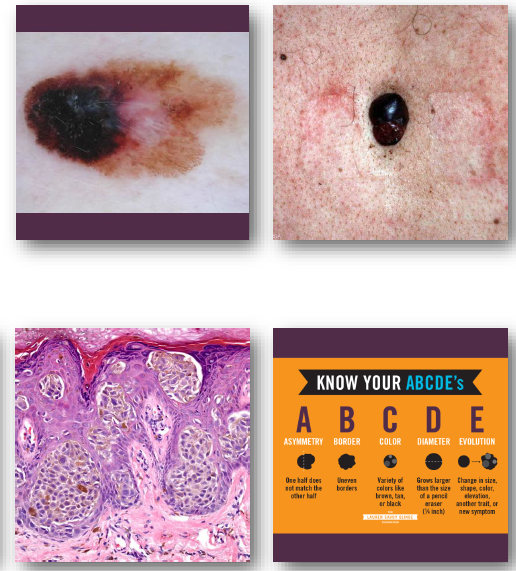
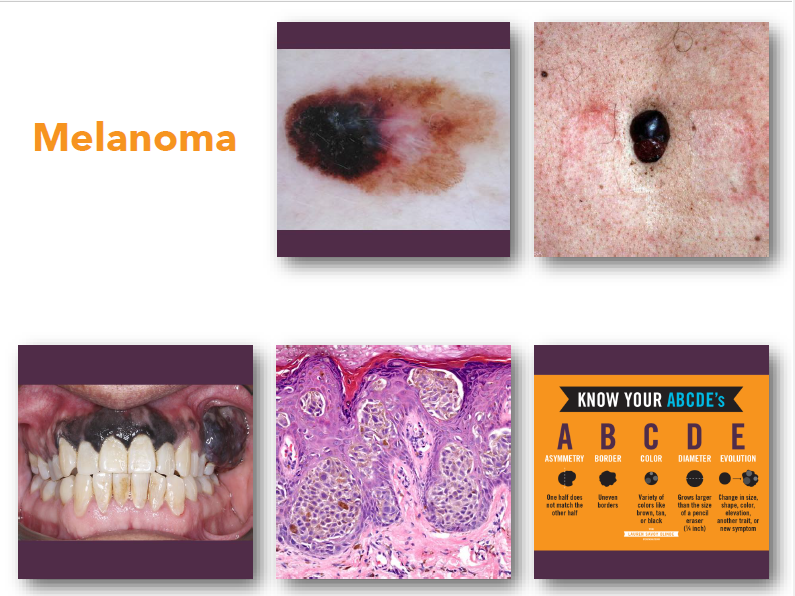
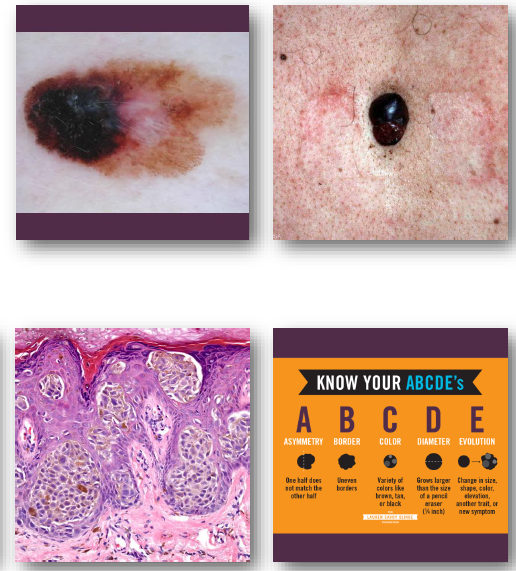
melanoma
•Malignant tumor arising from melanocytes
•Strongly associated with ultraviolet exposure
•Most dangerous form of skin cancer
•Early detection critical for survival
•May occur on skin or mucosal surfaces
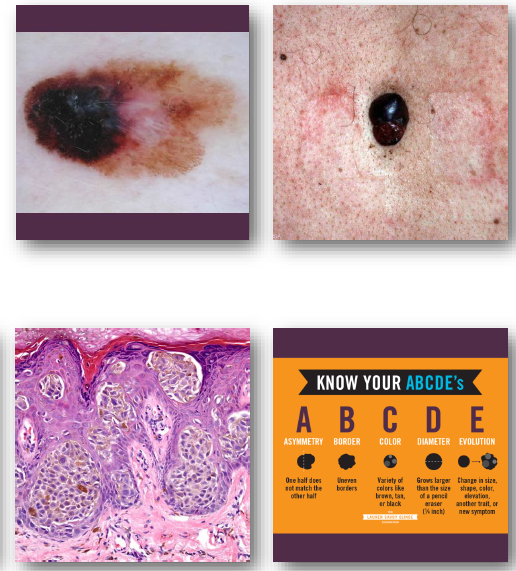
melanoma clinical features
•Irregular asymmetric pigmented lesion
•Varied colors including black and brown
•Borders often irregular or notched
•Diameter often greater than 6 millimeters
•Changes over time are critical warning sign
melanoma management and prognosis
•Early surgical excision is essential
•Prognosis depends on depth of invasion
•High risk of metastasis if advanced
•Requires urgent referral and treatment
•Survival improves with early detection
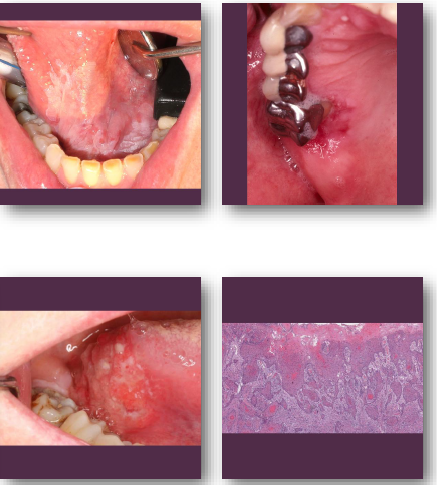
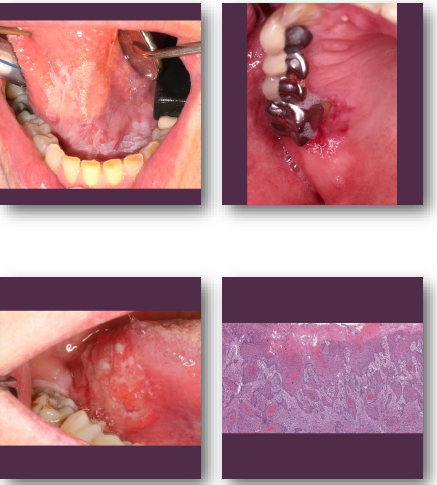
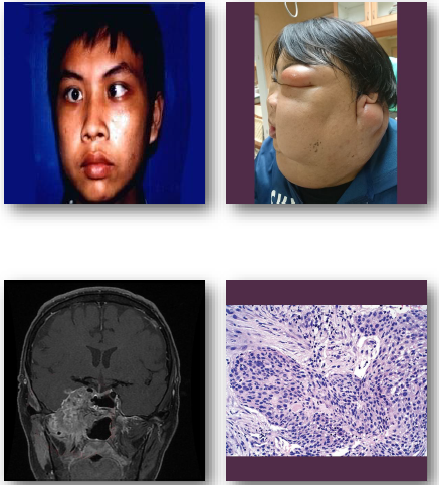
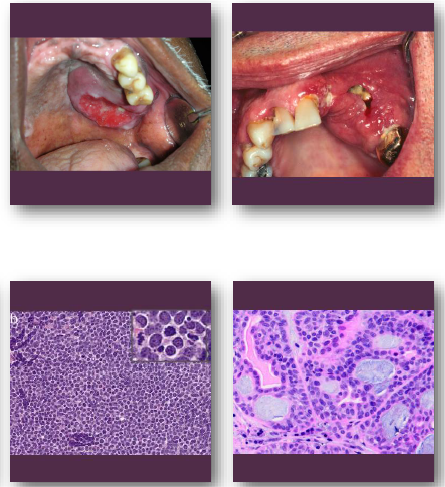
oral squamous cell carcinoma overview
•Malignant tumor of oral stratified epithelium
•Strongly linked to tobacco and alcohol use
•HPV-related cases occur in oropharynx
•Often arises from premalignant lesions
•Includes several aggressive histologic variants

oral squamous cell carcinoma clinical features
•Non-healing ulcer or exophytic mass lesion
•Mixed red and white mucosal appearance
•Induration on palpation is key finding
•Common on tongue and floor of mouth
•May be painless early and painful later
oral squamous cell carcinoma management and prognosis
•Requires biopsy for definitive diagnosis
•Treated with surgery, radiation, chemotherapy
•Prognosis depends on stage at diagnosis
•Variants may show more aggressive behavior
•Risk of recurrence and metastasis exists
Verrucous carcinoma overview
•Low-grade variant of squamous cell carcinoma
•Strongly associated with tobacco use
•Slow-growing but locally invasive lesion
•Rarely metastasizes to distant sites
•Often arises from leukoplakic lesions
verrucous carcinoma clinical features
•Thick white verrucous or papillary mass lesion
•Broad-based lesion with slow enlargement
•Often involves buccal mucosa or gingiva
•Surface appears rough and warty (verrucous)
•Typically painless in early stages
verrucous carcinoma management and prognosis
•Wide surgical excision is treatment of choice
•Radiation often avoided due to risk factors
•Recurrence possible if incompletely removed
•Excellent prognosis compared to SCC
•Very low metastatic potential
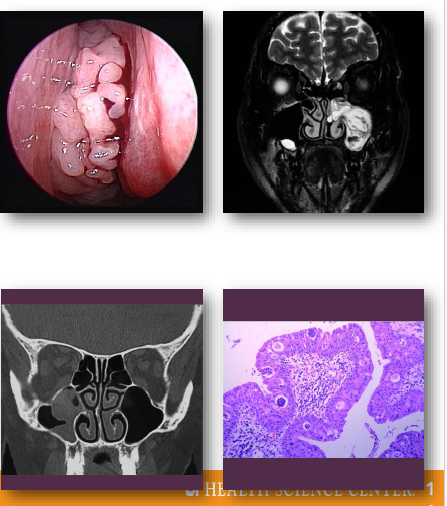
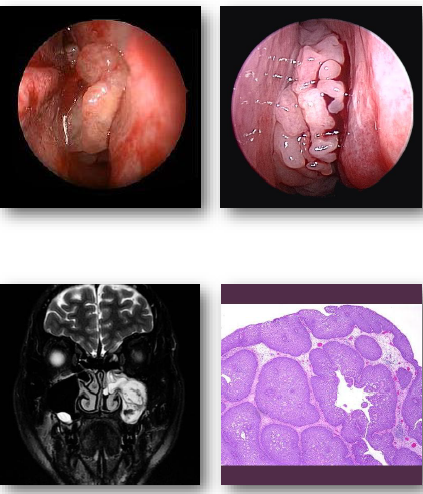
sinonasal papillomas overview
Benign epithelial tumors of sinonasal mucosa
•Includes inverted and exophytic variants
•Associated with HPV infection in some cases
•Locally aggressive with recurrence potential
•Small risk of malignant transformation exists
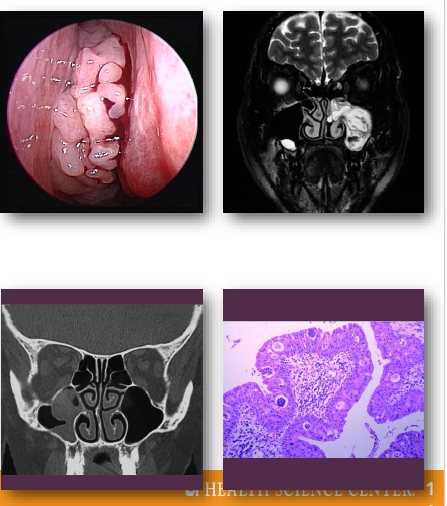
sinonasal papillomas clinical features
•Unilateral nasal obstruction or visible mass
•May present with epistaxis or discharge
•Often arises from lateral nasal wall
•May extend into adjacent sinus spaces
•Symptoms depend on size and location
sinonasal papillomas management and prognosis
•Surgical excision required for treatment
Complete removal reduces recurrence risk
•Long-term follow-up recommended
•Recurrence relatively common
•Small risk of malignant transformation
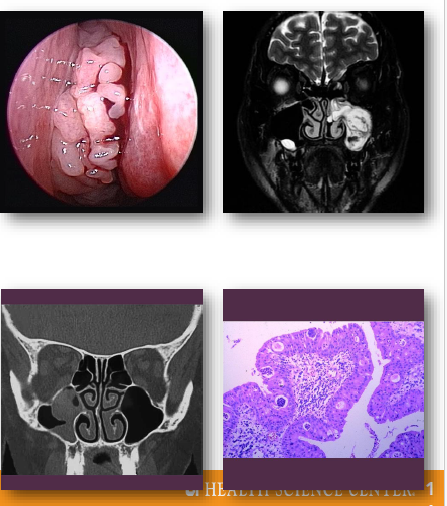
fungiform sinonasal papilloma
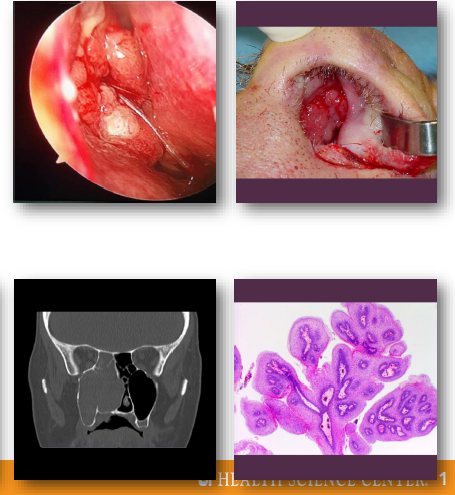
inverted sinonasal papilloma
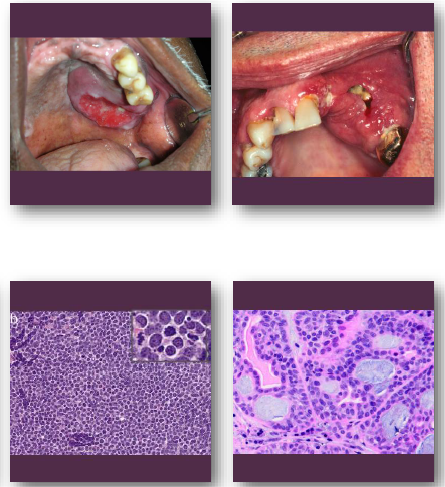
nasoparyngeal carcinoma overview
•Malignant epithelial tumor of nasopharynx
•Strongly associated with Epstein-Barr virus
•Higher incidence in specific populations
•Often presents late due to hidden location
•Early metastasis to regional lymph nodes
nasopharyngeal carcinoma clinical features
•Nasal obstruction or recurrent epistaxis
•Neck mass from lymph node involvement
•Hearing loss or ear fullness symptoms
•Headache or cranial nerve deficits
•Symptoms often subtle in early stages
nasopharyngeal carcinoma management and prognosis
•Primarily treated with radiation therapy
•Chemotherapy used for advanced disease
•Prognosis depends on stage at diagnosis
•High risk of regional metastasis
•Early detection improves survival rates
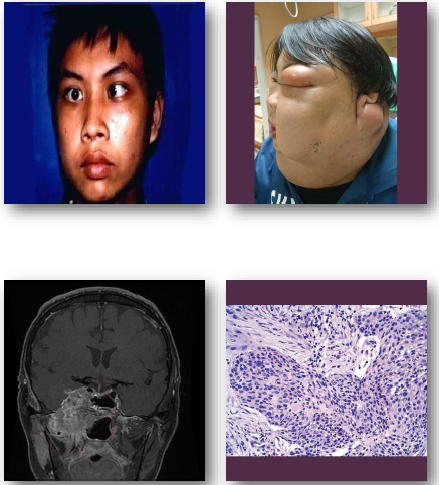
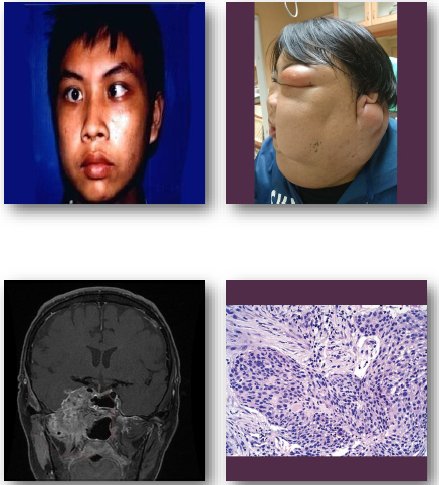
carcinoma of the maxillary sinus overview
•Malignant epithelial tumor of maxillary sinus
•Often squamous cell carcinoma histologically
•Associated with occupational and environmental exposures
•Frequently presents at advanced stage
•Close proximity to orbit and cranial structures
carcinoma of the maxillary sinus management and prognosis
• Requires combined surgical and oncologic therapy
• Radiation therapy commonly included in treatment
• Prognosis depends on stage at diagnosis
•Often poor due to delayed detection
Requires multidisciplinary management approach
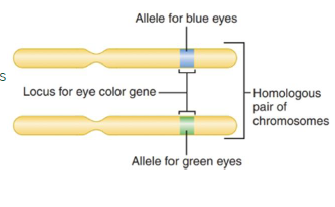
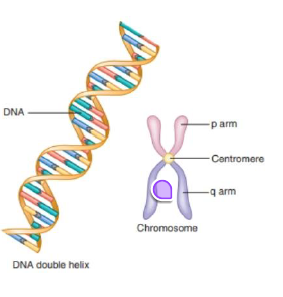
chromosomes: structure and organization
DNA packaged into organized units
• visible only during active cell division
• Centromere divides _ into two distinct arms
Short p arm and long q arm define shape
• Gene locations identified using chromosomal addresses
genes and alleles
basic functional units
Genes are DNA segments that determine traits
• Genes direct structure and function of cells and tissues
• Each gene carries instructions for inherited characteristics
• Traits include eye color, hair color, and tooth shape
• Alleles represent specific variations within a gene