Hormonal control of menstrual cycle and contraception
1/13
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
14 Terms
Menstrual cycle
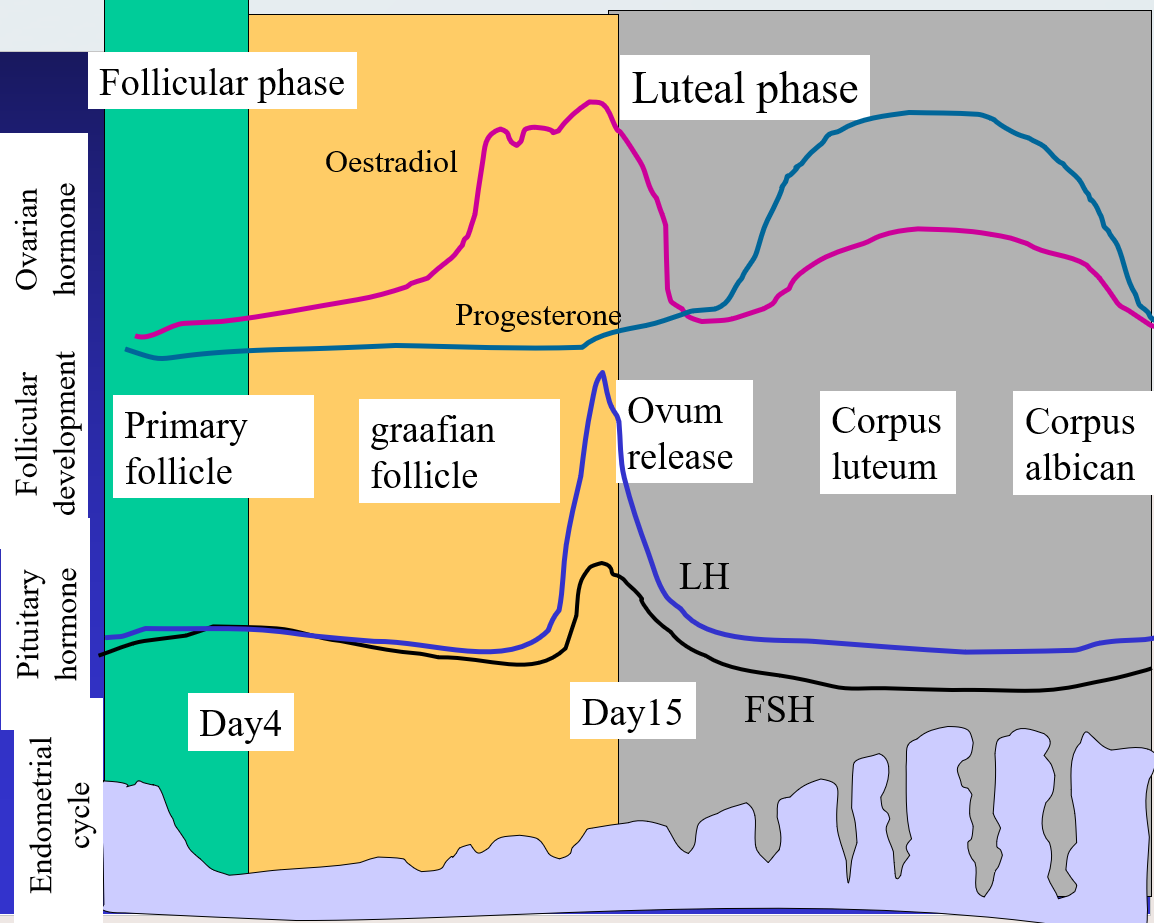
Follicular Phase (Day 1-14) (proliferative phase)
Start 1st day of menstruation until ovulation.
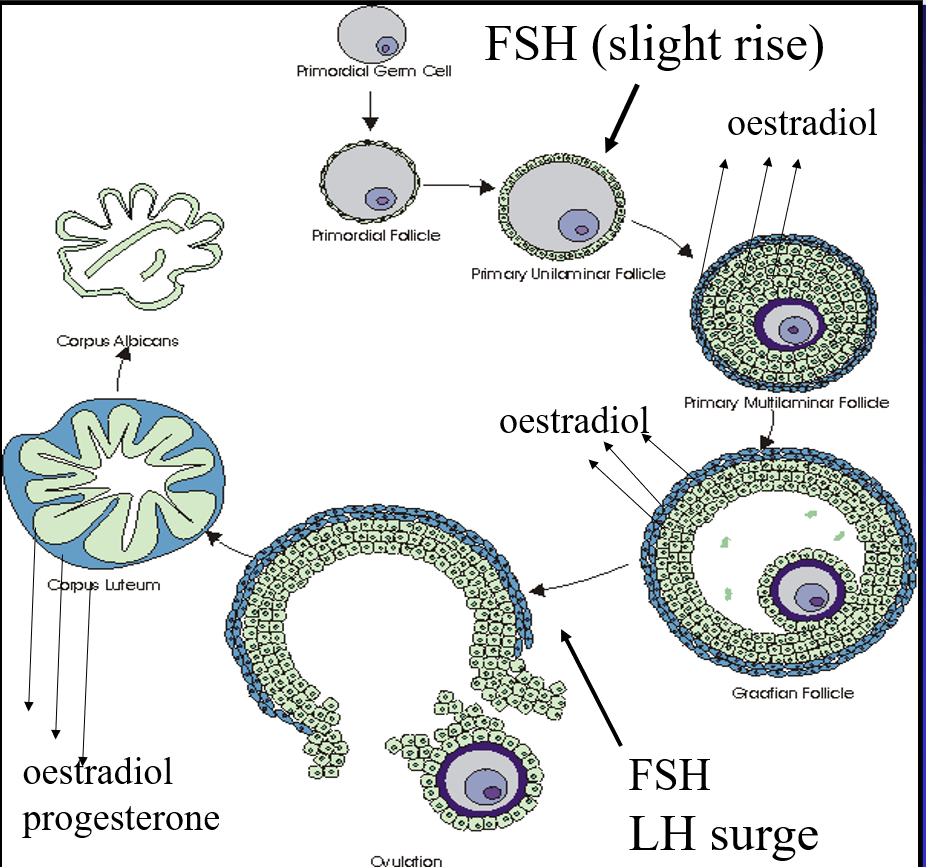
Development of a follicle capable of undergoing ovulation.
1 Early phase (day 1-6): slight rise in FSH levels.
FSH stimulates 15-20 follicles to develop and stimulate follicular secretion of oestradiol.
2 Late follicular phase (day 7-14).
As oestradiol levels increase, FSH secretion decreases.
One follicle evolves into the dominant follicle (Graafian follicle) destined for ovulation.
The others degenerate (atresia).
It is not known how the dominant follicle is selected (possibly depends on FSH receptor number).
The dominant follicle continues to synthesise estradiol, essential for its complete maturation.
3 The dominant follicle expels the oocyte into the uterine tube while the zona granulosa cells remain in the ovary.
Slight increase in FSH at the beginning will favour the recruitment of a few follicles which mature.
Follicles release oestradiol
On day 14 (end of follicular stage) lots of oestradiol is release
Oestradiol has effect on endometrium (lining of the uterus cavity)
At the beginning of cycle lining is shed off. Then slowly starts to regenerate due to oestradiol
Then positive feedback is induced and oestradiol is reduced. Leads to release of LH and FSH
Big follicle release ovum into ovarian cavity and then uterus
Endometrium becomes thicker
If becomes fertilises it attaches to uterus
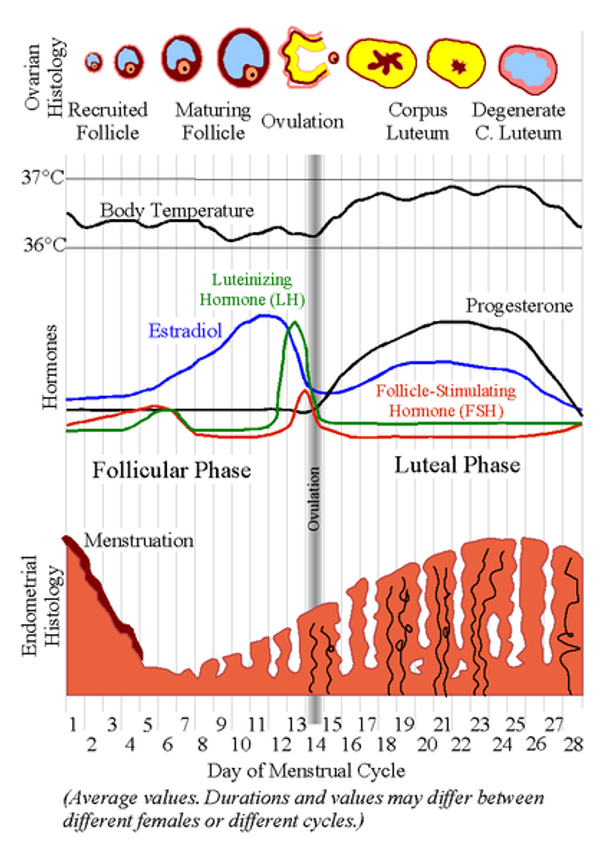
Luteal Phase
Luteal Phase (Day 14-28)
4 The zona granulosa and surrounding theca cells develop into the corpus luteum, which in turn becomes atretic (degenerates) after 14 days.
After several months, the corpus luteum has fully devolved into the corpus albicans.
Hormonal changes during the late follicular: Phase details
1 The level of oestrogen is at its highest level and feedback positively on the pituitary to generate the preovulatory LH surge required for ovulation (note: it is only at this precise stage of the menstrual cycle that oestrogen can exert positive feedback).
Oestrogen induces a prolific secretion by the cervix of a type of “fertile” mucus which facilitates the journey and the survival of the spermatozoa and causes the lining of the uterus (endometrium) to grow, or proliferate .
2 LH surge promotes the final stage of the first meiotic division, and give rise to the secondary oocyte which will undergo another meiosis and maturate into an ovum. LH also induces the release of proteolytic enzymes which will help for the follicle rupture. The ovum will be released into the fallopian tube.
3 LH and FSH begin to decrease back to baseline levels almost immediately by the time ovulation occurs.
Positive feed-back process:
The dominant follicle is possibly the one which possesses the greatest number of LH/FSH receptors (receives enough gonadotrophic support to continue to develop).
During the late follicular phase the dominant follicle responds to FSH and LH by greatly increasing oestradiol synthesis.
The sustained high level of oestradiol acts at the hypothalamus and pituitary to cause a positive feed-back effect such that a large outpouring of LH/FSH will be released.
In women, oestradiol positive feed-back occurs when oestradiol levels reach appr. 150 ng/l for at least 36 hours.
The mechanism underlying the estradiol positive feed-back is unknown. It does not seem that GnRH release during the surge is pulsatile.
Luteal Phase
Day 15-28.
The cells of the collapsed follicle reorganised into a transiently functional steroid-producing endocrine gland (made of theca and granulosa cells), the corpus luteum. They secrete oestrogens and progesterone.
Theca cells secrete progesterone.
High progesterone levels:
1) feedback negatively on the secretion of GnRH (hypothalamus) producing the decline of LH/FSH
2) stimulate the secretory phase and regeneration of the endometrium in concert with oestrogens (induces the endometrial glands to secrete glycogen, mucus, and other substances to favour the fertilised egg implantation).
3) Stimulate the secretion of G-mucus from the cervix (see slide 12)
Luteal phase Day 15-28
If pregnancy occurs, progesterone, estrogens and gonadotrophins are secreted by the placenta.
In the absence of fertilization by day 23, the corpus luteum begins to degenerate and consequently estrogen and progesterone levels decrease, the endometrium undergoes involution.
At days 25-28, vasoconstriction of the spiral arteries begins, subsequent ischemia cause mass apoptosis of the functionalis. Arteries rupture, releasing blood into the uterus, and the apoptosed endometrium is sloughed off (lasts 4-7 days), the functionalis is completely shed.
Combined pill
Can be Monophasic combined (identical amount of oestrogens/progestin taken daily for 21 days, followed by 7 days placebo or biphasic/triphasic: varying amount of oestrogen/progestin for 21 days, followed by 7 days placebo.
Mechanism of action: effective through the negative feedback loop of the HPG axis. Oestrogen (ethinylestradiol, mestranol) inhibits the release of FSH and prevents development of follicles. Suppress ovulation in about 98% cycle.
Progestogen (levonogestrel…) also inhibit the release of LH and prevent ovulation and makes the cervical mucus less suitable for sperm.
Continuous progestogen is intended to induce endometrial atrophy and hence to prevent oestrogen-stimulated endometrial proliferation.
Therefore, CP affects the natural functioning of endometrium and cervix, disrupts the normal growth pattern so that it cannot sustain an embryo (atrophy of the endometrium).
Percentage of unwanted pregnancy: app. 0.1%
Progestogen only pills
Norethisterone, levonorgestel, ethynodiol same dose through the cycle.
Feedback negatively on GnRH release and also LH/FSH, but do not prevent ovulation at each cycle (40%).
Act more specifically on mucus production, stimulate the production of G-mucus (G-mucus = impenetrable Gestagenic mucus formed in the lowest cervical crypts. Prevents sperm entry to the cervix and is part of the immune system which protects the woman's reproductive system from infection, secreted during the luteal phases under progesterone stimulation), and prevent sperm penetration and sperm survival.
Conteract the effect of oestrogen on the endometrium mucus, preventing implantation due to atrophic endometrium.
Percentage of unwanted pregnancy (if correctly administered): app. 0.5%
Contraindications
Absolute:
History of DVT (deep vein thrombosis), stroke, CAD (coronay artery disease), Breast cancer, liver problem, smoking>35 yrs,
Relative:
Hypertension, diabetes, headache
Advantages:
Decreased menstrual cramp and pain, decrease menses blood loss, improve hirsutism, decreased incidence of ovarian and endometrial cancer, ovarian cyst and pregnancy. Can improve acne (cp), high dose of estrogen (day-after-pill, can be used as emergency contraception).
Disadvantages:
Small risk of breast cancer, increase appetite/weight gain, hypertension (cp), thromboembolic events (cp), breast tenderness (cp), visual change, hypomenorrea, Fatigue (PO), depression (PO), acne (PO).
Emergency contraceptives:
Usually the same hormones as in regular contraceptives but at higher doses, often progestin only EC.
Mifepristone (potent abortive antiprogestogen) at lower dose than for medical abortion)
Other important drugs
Clomiphene/cyclofenil:
antioestrogens inhibit oestrogen binding in the anterior pituitary,
causing increased secretion of GnRH and gonadotrophins. Ovarian stimulant, induce ovulation.
Mifepristone:
antiprogestogens, given in combination (48 hrs) before a prostaglandin analogues to induce abortion.
GnRH agonists (Nafarelin, gonadorelin) given continuously, they suppress gonadotropin release (desensitization).
Danazol: modified progestogen suppress gonadotrophin release