Peripheral/Cranial Nerve Disorders and Complex Regional Pain Syndrome
1/87
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
88 Terms
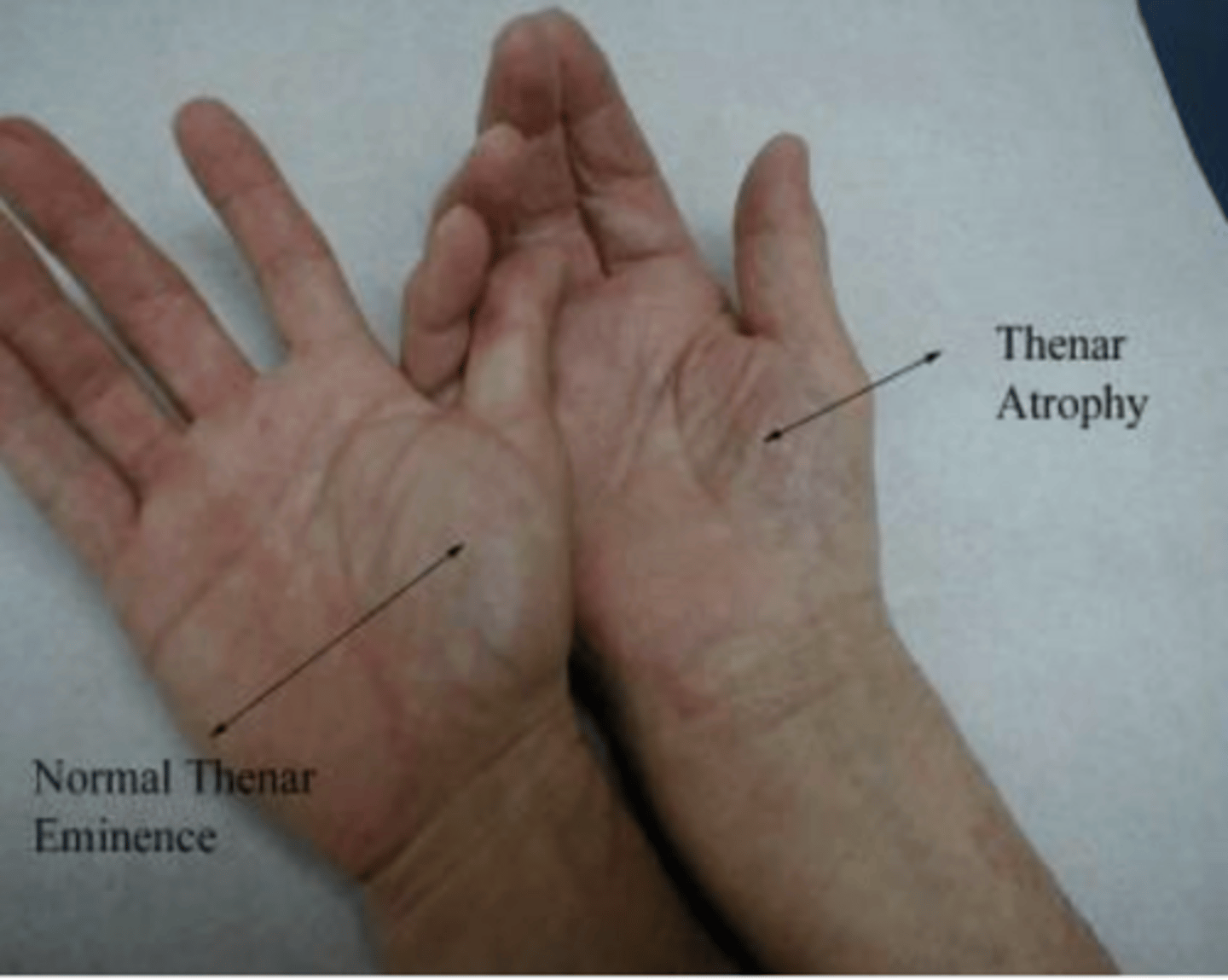
What is carpal tunnel syndrome?
compressive neuropathy of the median nerve that is extrinsic or intrinsic and increases with age and affects women > men
What are the risk factors of carpal tunnel syndrome?
repetitive use, obesity, pregnancy, diabetes, RA, and hypothyroidism
What are the symptoms of carpal tunnel syndrome?
numbness, paresthesias, pain, aching on the lateral aspect of the hand at the first three digits and helf of the 4th
What is the 'flick sign' in the context of Carpal Tunnel Syndrome?
A patient waking at night and shaking their hand to relieve symptoms
What are potential physical exam findings of carpal tunnel syndrome?
Thenar atrophy, decreased sensation over median nerve distribution to sharp/dull and light touch. Decreased strength to thumb opposition
What are the two common special physical exam tests for Carpal Tunnel Syndrome?
Tinel's sign and Phalen's sign
What diagnostics are used for carpal tunnel syndrome?
EMG and Nerve Conduction Study (NSC)
What is the treatment for carpal tunnel syndrome?
NSAIDs, wrist splint, PT/OT, ergonomic modifications, steroid injections, and surgical release
What causes ulnar neuropathy?
Exposure of ulnar nerve to pressure or trauma
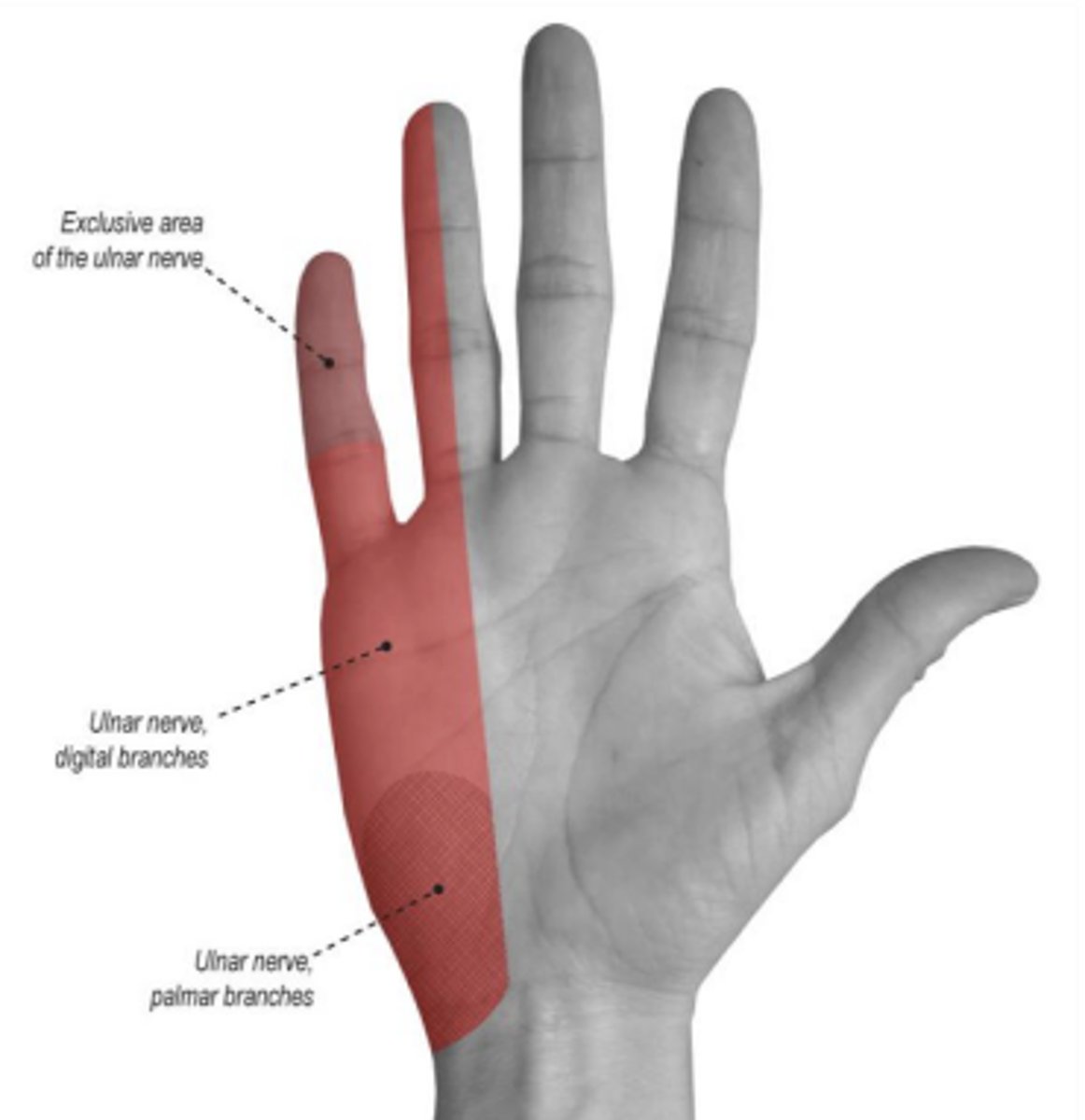
What is the clinical presentation of Ulnar Neuropathy (Cubital Tunnel Syndrome)?
Numbness, paresthesias, and pain in the medial hand, fifth digit, and half of the fourth digit, often with intrinsic hand muscle weakness.
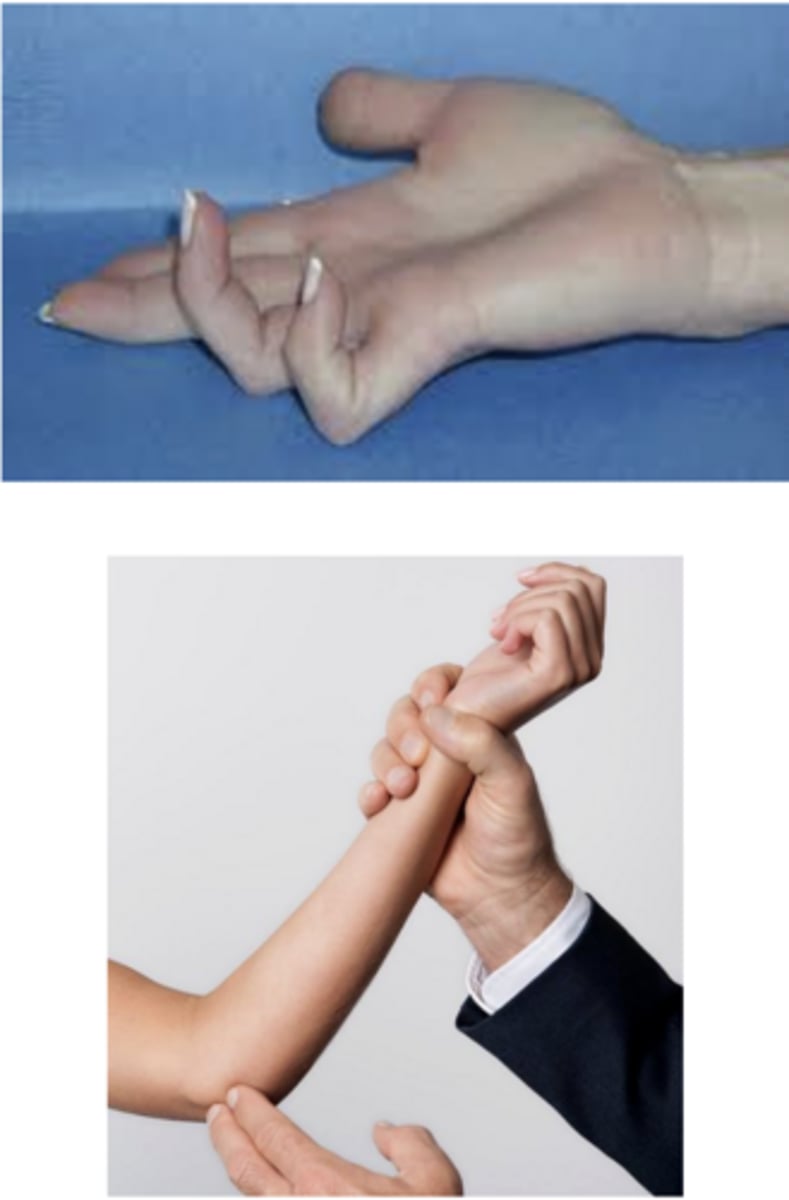
What are the physical exam findings of ulnar neuropathy?
intrinsic muscle atrophy, claw hand, decreased sensation over ulnar nerve distribution, motor weakness, positive tinel sign at elbow
What is the management of ulnar neuropathy?
avoid aggravation, splinting, elbow pads, PT/OT, nerve decompression (no improvement after 6-12 weeks or long-standing lesion)
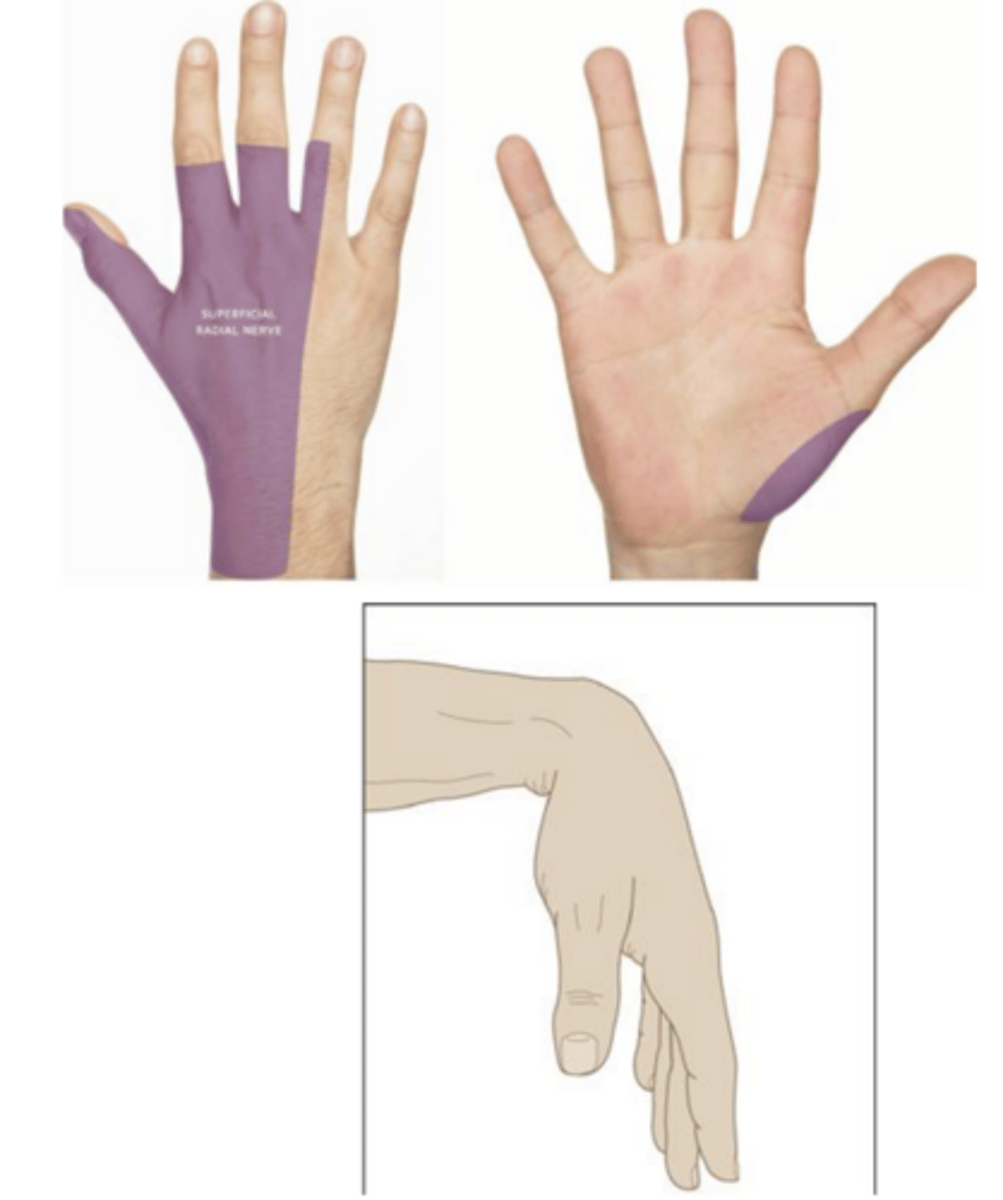
What is radial neuropathy (saturday night/crutch palsy)?
transient compressive injury that can be from crutch use or post-operative
What are the physical exam signs of radial neuropathy?
wrist drop, weakness with finger extension of first and second digit, sensory loss at dorsal web +/- hyporeflexia
what is the average time for spontaneous recovery of radial neuropathy?
6-8 weeks
What are the conservative management options for radial neuropathy?
cock-up wrist/finger splints, avoidance of further compression, PT/OT

What causes lateral cutaneous femoral neuropathy (Meralgia Paresthetica)?
mechanical entrapment, increased subcutaneous fat, wearing tight clothes/belts, post-operative
What are the primary symptoms of lateral cutaneous femoral neuropathy?
Paresthesias, numbness, or pain in the lateral thigh worse with standing typically without motor weakness
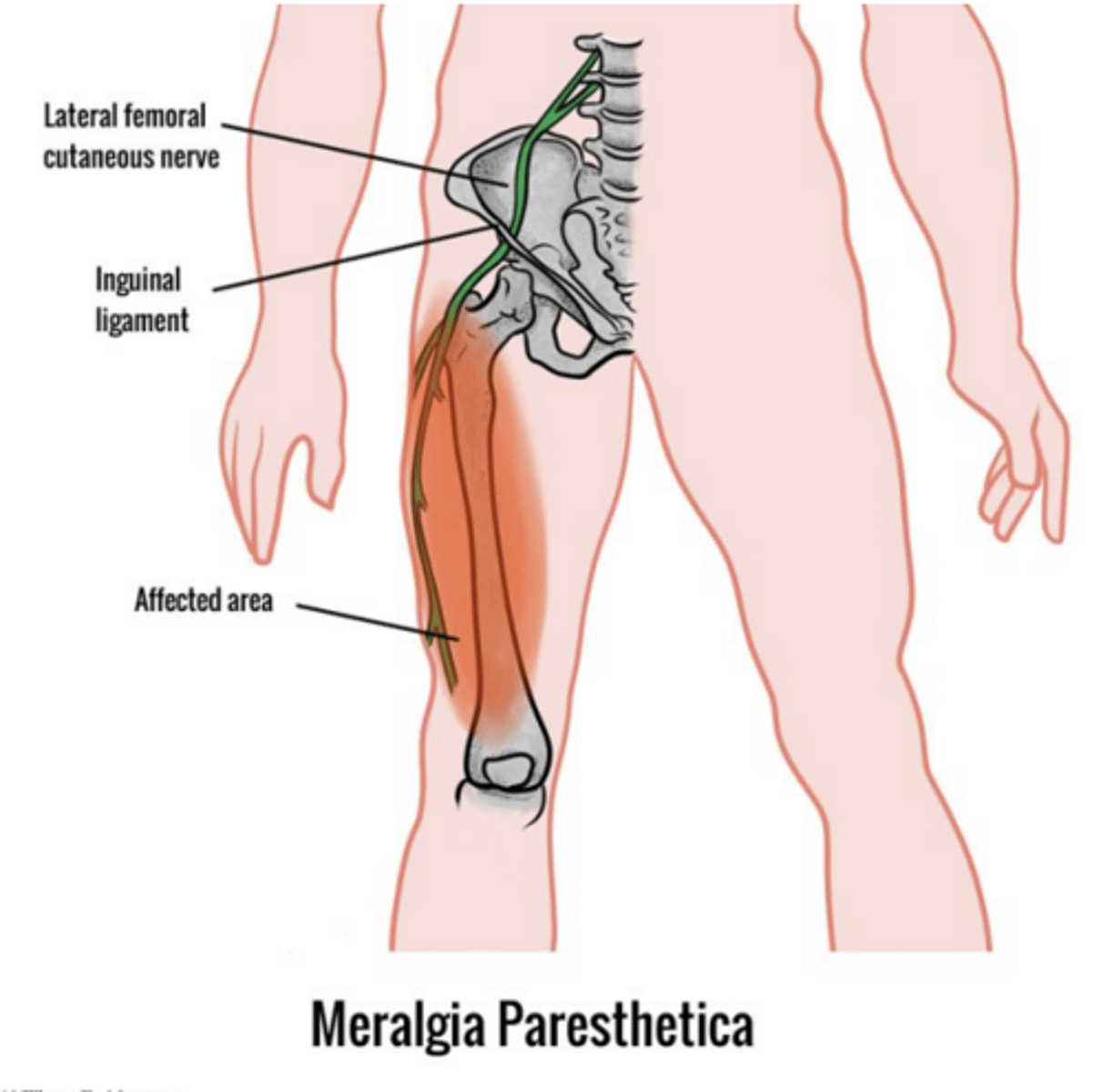
what is the management of lateral cutaneous femoral neuropathy?
natural course over weeks-months, weight loss, avoid tight belts/jeans, NSAIDs, lidocaine, patch
What causes peroneal neuropathy?
Compression, trauma, Crossing legs, Rapid weight loss, Diabetes
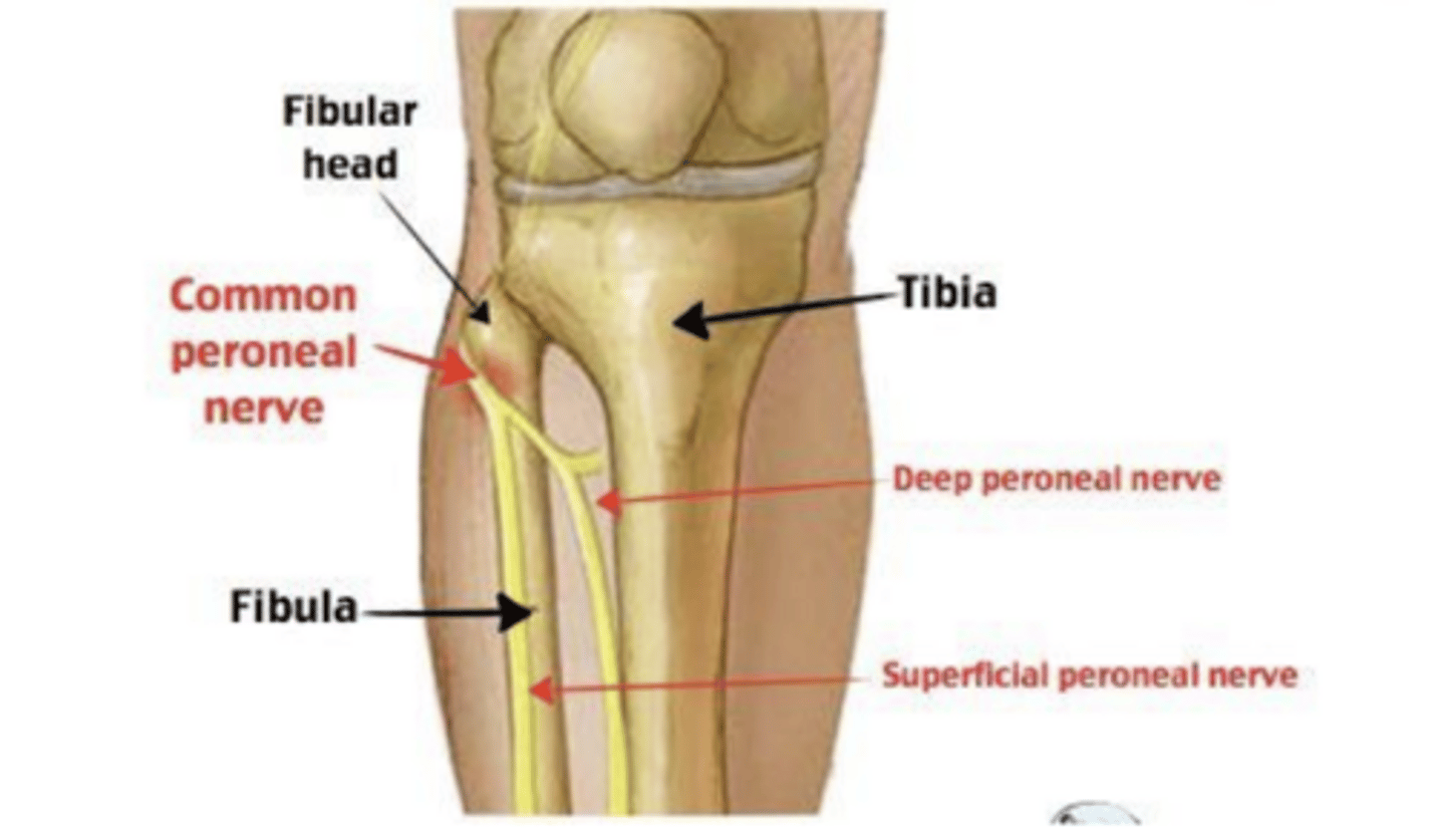
What are the physical exam signs of peroneal neuropathy?
Foot drop (weakness in ankle dorsiflexion, toe extension, and ankle eversion), sensory loss over the lateral calf
what is the management of peroneal neuropathy?
spontaneous recovery over weeks-months, weight loss, avoid leg crossing, ankle brace for foot drop, knee pad over lateral knee
What is the most common form of diabetic neuropathy?
Distal symmetric sensory or sensorimotor polyneuropathy (DSPN), which is typically axonal and length-dependent.
What are the primary clinical symptoms of diabetic sensory neuropathy?
Numbness, paresthesias, and pain, following a distal-to-proximal stocking-glove distribution.
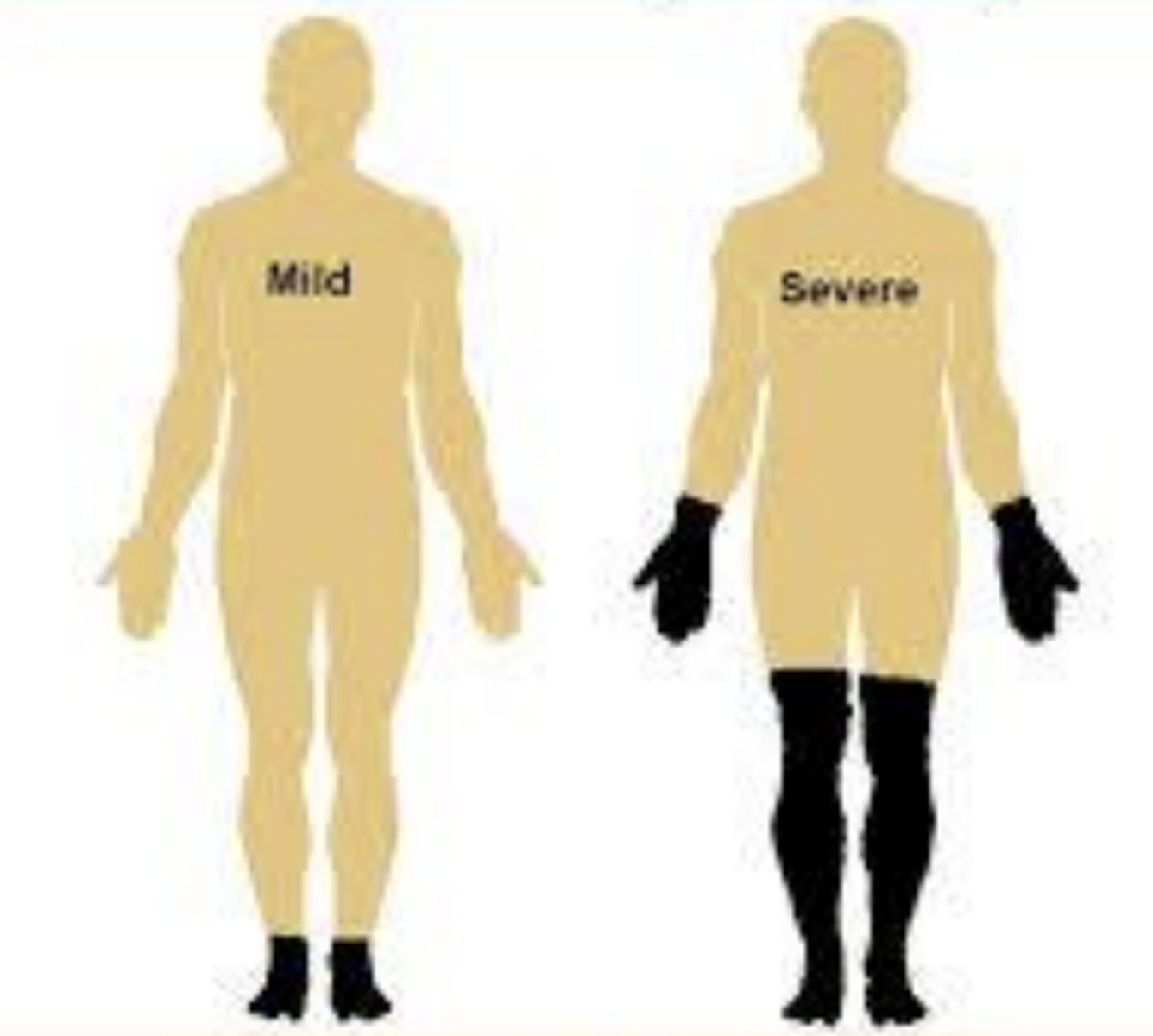
What physical exam findings are characteristic of diabetic neuropathy?
Distal-to-proximal sensory impairment, hyporeflexia, and potential weakness in the same distribution.
What diagnostics are used in diabetic neuropathy?
HbA1c, fasting blood sugar +/- EMG to confirm if uncertain
What are the main management pillars for diabetic neuropathy?
Strict glucose control, foot care education (podiatry referral), and medications for pain and autonomic dysfunction.
What are the three main clinical presentations of B12 deficiency neuropathy?
Polyneuropathy (non-length dependent), myelopathy (subacute combined degeneration), and cognitive decline.
What are common medications that can contribute to B12 deficiency?
H2 blockers, PPIs, and metformin.
What are the signs of B12 Deficiency Neuropathy?
symmetric numbness and paresthesia with diminished proprioception/vibration, positive Rhomberg, gait instability
What lab findings are diagnostic for B12 deficiency?
Low serum B12 and elevated methylmalonic acid levels.
What is the prognosis for B12 deficiency-related neuropathy after treatment?
Complete reversal is often not attained, with approximately 50% of patients having residual deficits.
What are the two main clinical forms of Thiamine (B1) deficiency (Beriberi)?
Dry Beriberi (neurologic) and Wet Beriberi (cardiac).
What are the causes of Thiamine deficient neuropathy?
poor nutrition, chronic alcohol, recurrent vomiting, TPN, bariatric surgery
What are the sensory and motor symptoms of Thiamine deficiency?
distal-to-proximal distribution numbness/weakness with associated hyporeflexia.
What is the management of neuropathy from thiamine deficiency?
test serum thiamine and use par/enteral thiamine replacement until proper nutrition restored
What are the various causes of toxic neuropathy?
ETOH, recreational drugs, heavy metals, biological toxins, and industrial agents
What is the typical clinical presentation of alcohol-related neuropathy?
A length-dependent, sensory-predominant axonal neuropathy often described as a stocking/glove distribution.
What is the management of peripheral neuropathy?
remove the toxin, neuropathic pain medication +/- chelation for heavy metal poisoning
What is the most common hereditary peripheral neuropathy?
Charcot-Marie-Tooth (CMT) disease.
What are the characteristics of Charcot-Marie-Tooth (CMT) disease?
typically in 1st or 2nd decade of life, + family history, demyelinating > axonal
What are the classic physical signs of Charcot-Marie-Tooth (CMT) disease?
High arches, hammer toes, distal atrophy, foot drop, and hyporeflexia or areflexia.

How is CMT diagnosed?
EMG
What is the treatment of CMT?
PT/OT, Bracing (ankle-foot orthotics)
What is the most common neuropathic manifestation of hypothyroidism?
Carpal tunnel syndrome.
What are the primary neurologic syndromes associated with late-stage Lyme disease?
Polyradiculoneuropathy (painful), multiple mononeuropathies, cranial neuropathies, and meningitis.
What is the recommended treatment for Lyme disease-related neuropathy?
Doxycycline PO or IV Ceftriaxone, cefotaxime, or penicillin G for 14-21 days.
What is critical illness polyneuropathy?
A complication of shock, multiple organ failure, or prolonged ICU stay that often presents as an inability to wean from a ventilator.
What is the pathophysiology of Guillain-Barré Syndrome (GBS)?
An immune-mediated process where antibodies (often triggered by antecedent infection) attack peripheral nerve axons or myelin via molecular mimicry.
What pathogens can cause Guillain-Barré Syndrome?
Campylobacter jejuni, CMV, EBV, HIV, and Zika
What is the presentation of Acute inflammatory demyelinating polyradiculoneuropathy (AIDP)?
distal > proximal weakness and numbness that progresses up limbs rapidly and can be very painful
What is the presentation of Acute Motor Axonal Neuropathy (AMAN)?
No sensory involvement, DTRs may be preserved
What is the presentation of Acute Motor and Sensory Axonal Neuropathy (AMSAN)?
AMAN + sensory nerve involvement
What are the clinical features of Miller Fisher Syndrome?
ophthalmoplegia, double vision ataxia, incoordination and hyporeflexia/areflexia.
How does the weakness/numbness present in GBS?
Typically starts in LEs and then symmetrically spread to the UE, trunk and even face
What ocular symptoms may be present in GBS?
ophthalmoplegia, diplopia, and double vision
What are the bulbar signs and symptoms in GBS?
face/oral weakness, dysarthria, voice deterioration, dysphagia, and excessive salivation/drooling
What autonomic disturbances occur in GBS?
Bradycardia, tachycardia, BP instability, SIADH, Urinary retention, Diarrhea/constipation
What are the significant complications of CBS?
aspiration, upper airway obstruction, respiratory failure
What is the hallmark CSF finding in Guillain-Barré Syndrome?
Albuminocytologic dissociation: elevated CSF protein with a normal white blood cell count.
What imaging should be obtained in GBS?
MRI spine to rule out myelopathy and may show enhancement of affected nerve roots/cauda equina
What labs are obtained in GBS?
IgG anti-GM1 positive, AMAN, GQ1b Ab positive, Miller Fisher Syndrome
What is the supportive care for GBS?
close monitoring, DVT prophylaxis, and pain control
What are the primary immunotherapy treatments for GBS?
Plasmapheresis or IVIG; corticosteroids are not beneficial.
What is the typical recovery pattern for GBS?
Recovery begins 3-4 weeks after onset, following a gradient inverse to the direction of involvement (bulbar function recovers first, lower extremities last).
What are the predictors of poor outcome in GBS?
Axonal/CN involvement, Intubation, maximal disability, antibody positive
What is Bell's Palsy?
An acute, idiopathic unilateral facial nerve (CN VII) mononeuropathy with peak incidence in the 4th decfade of life
What are the risk factors for Bell's Palsy?
Diabetes and pregnancy (specifically the 3rd trimester).
What is the typical onset pattern for Bell's Palsy symptoms?
Sudden onset, usually peaking by 3 days.
What are the common subjective signs of Bell's Palsy?
facial weakness, difficulty eating/drinking, facial stiffness, eye dryness, "numbness, posterior auricular pain, decreased taste, hyperacusis (phophobia)
What are the common objective signs of Bell's Palsy?
Unilateral facial muscle paralysis, disappearance of facial creases/nasolabial fold, drooping corner of the mouth, and incomplete eye closure.
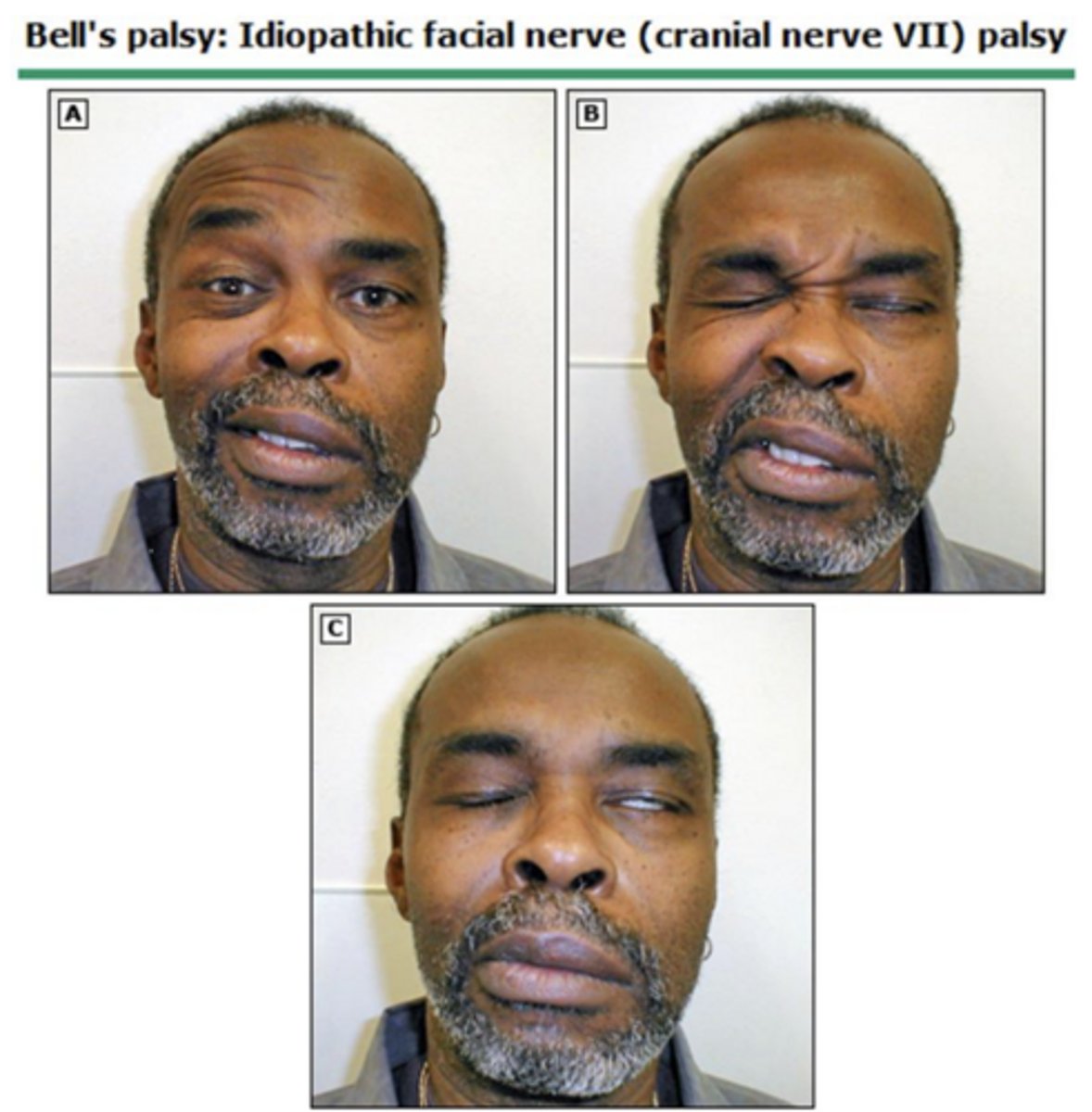
How does facial muscle involvement differ between Bell's Palsy and a central stroke?
Bell's Palsy involves both the upper and lower face (lower motor neuron pattern), whereas a central stroke typically spares the forehead.
What is the standard pharmacological treatment for Bell's Palsy?
Prednisone in 3 days of onset (60 mg daily for 5 days, followed by a 5-day taper) Valacyclovir (1000mg TID x 7 days)
What is the prognosis for patients with Bell's Palsy?
Approximately 30% of patients do not fully recover.
What characterizes the pathophysiology of Complex Regional Pain Syndrome (CRPS)?
Peripheral and central sensitization following injury, which activates an abnormal sympathetic reflex and lowers the pain threshold.
How is the pain described in CRPS?
burning, stinging, tearing pain felt deep in limb that is aggravated by movement, contact, temperature variation, and strength
what physical exam findings are seen in CRPS?
hyperalgesia, allodynia, weakness, decreased movement, skin color and temperature changes

What are the trophic changes commonly observed in chronic CRPS?
Increased hair growth, altered nail growth, skin atrophy, and joint contraction/fibrosis.
What is the typical presentation of CRPS Stage 1 (weeks after injury)?
Pain at the injury site, localized edema, altered color/temperature (bright red, warm), and increased diaphoresis.
What is the typical presentation of CRPS Stage 2 (3-6 months)?
increased edema, brawniess of skin, cool/diaphoretic, and muscle wasting
What is the typical presentation of CRPS Stage 3 (chronic)?
limited movement, digit contracture, waxy trophic skin, brittle nails, demineralization of bone
What is the symptomatic criteria for CRPS diagnosis?
≥ 1 symptom in 3/4 categories:
- sensory
- Vasomotor
- sudomotor/edema
- motor/trophic
What is the sign criteria for CRPS diagnosis?
≥ 1 sign in 2/4 categories:
- Sensory
- Vasomotor
- Sudomotor/edema
- Motor/trophic
what is seen on imaging in CRPS?
Bone scan showing diffuse increased uptake in affected extremity or x-ray showing generalized osteopenia

What medications can be used to manage CRPS pain?
NSAIDs, topical lidocaine/capsaicin, gabapentin, pregabalin, tricyclic antidepressants, bisphosphonate (abnormal uptake of bone)
What interventional procedures may be considered for refractory CRPS?
trigger point injections, regional sympathetic nerve block, spinal cord stimulation, epidural clonidine, mechanical sympathectomy
What is the risk of recurrence for CRPS?
There is a 10-30% risk of recurrence, often triggered by cold, trauma, surgery, or emotional stress.
What is the long-term prognosis for many CRPS patients?
Many patients do not fully recover; studies show a significant portion remain stable or continue to meet diagnostic criteria years after diagnosis.