Pupils
1/67
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
68 Terms
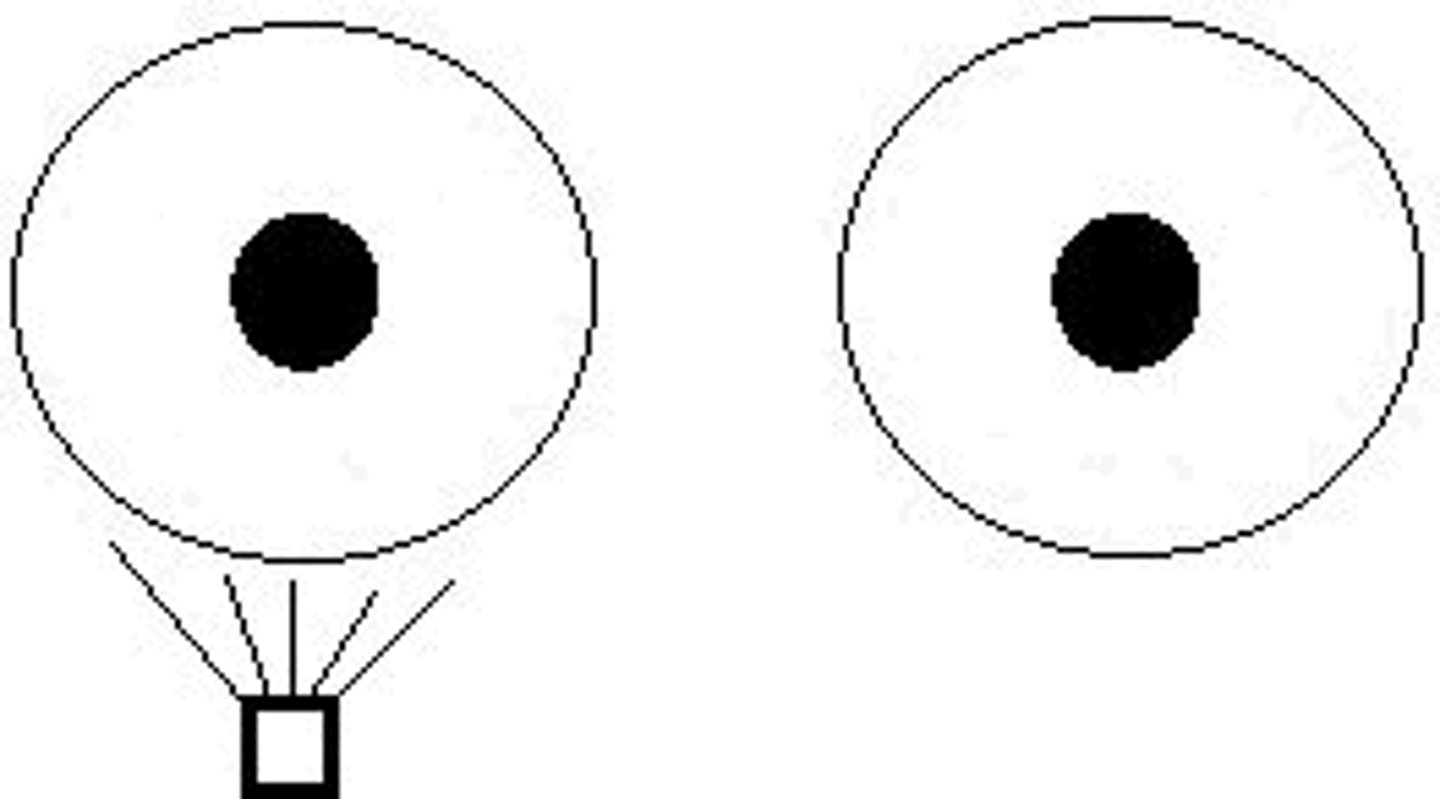
A condition where the two pupils have different diameters?
Anisocoria

Is anisocoria always related to pathology?
No
A condition where the post-ganglionic parasympathetic supply is impared.
Efferent pupillary defect
In an efferent pupillary defect, the pupil cannot (constrict/dilate) and is abnormally (small/large).
Constrict
Large
In an efferent pupillary defect, the path from the ________ _______ nucleus to the iris (sphincter/dilator) is impared.
Edinger Westphal
Sphincter
A condition where there is a lesion to the sympathetic supply to the iris?
Horner's syndrome

In Horner's syndrome, the pupil cannot (constrict/dilate) and is abnormally (small/large).
Dilate
Small

A condition where one pupil is less responsive to light than the other?
Afferent pupillary defect
Will an APD create an anisocoria?
No
How do we reveal an APD?
Swinging flashlight test
Where is an APD-causing lesion most common?
Optic nerve
Normal pupil diameter in light?
1-2 mm
Normal pupil diameter in dark?
7-9 mm
Our pupil (increases/decreases) in size as we age.
Decreases
Latency of pupillary response varies with _____ ________.
Light intensity
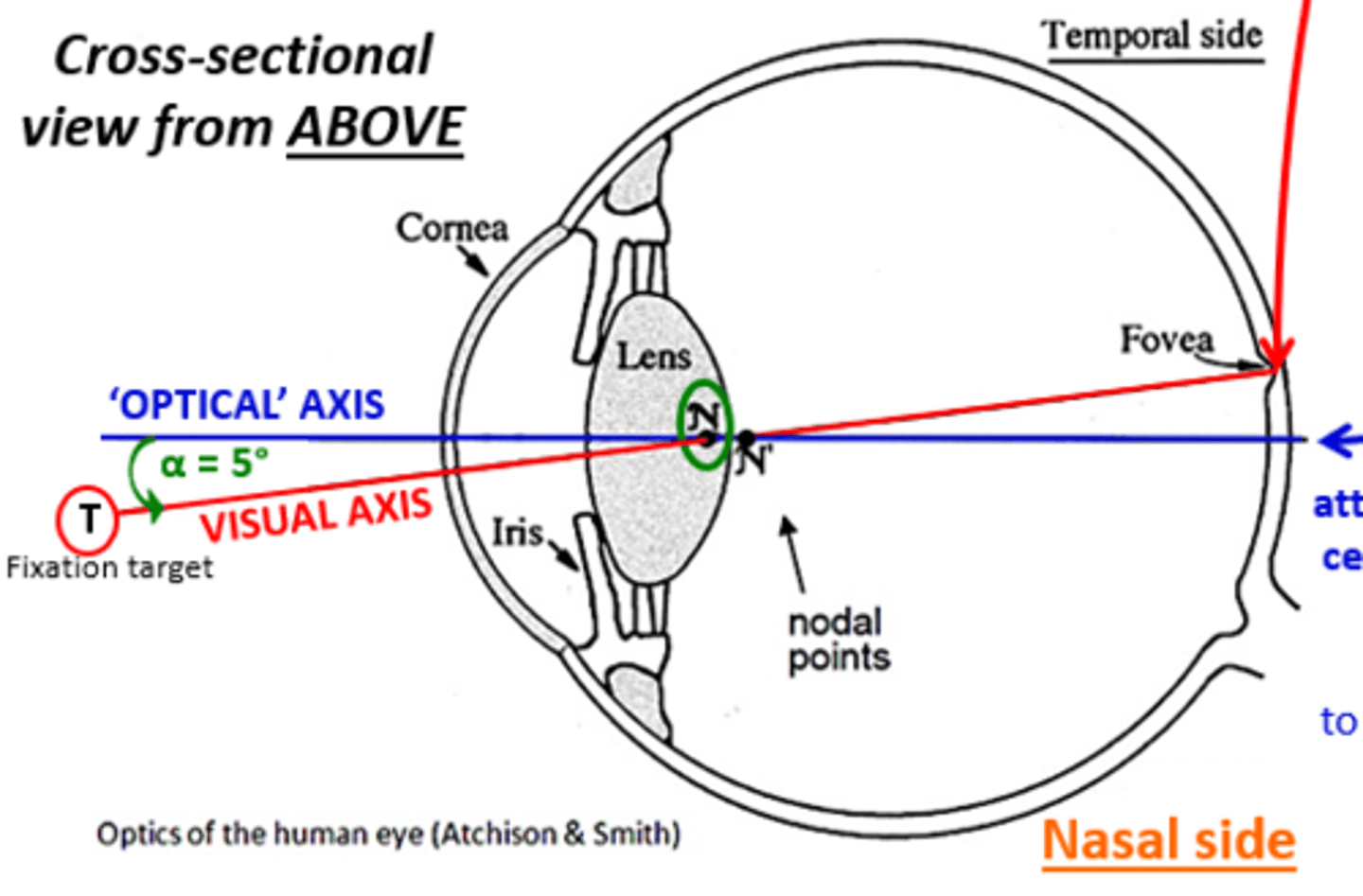
The pupil is positioned (nasal/temporal) and (superior/inferior) within the iris
Nasal
Inferior
The position is (nasal/temporal) in reference to the visual axis
Nasal
_________ ______ is the normal physiological "unrest" that oscillates more with more light
Pupillary hippus
Pupillary muscles embryonic origin?
Neuro ectoderm
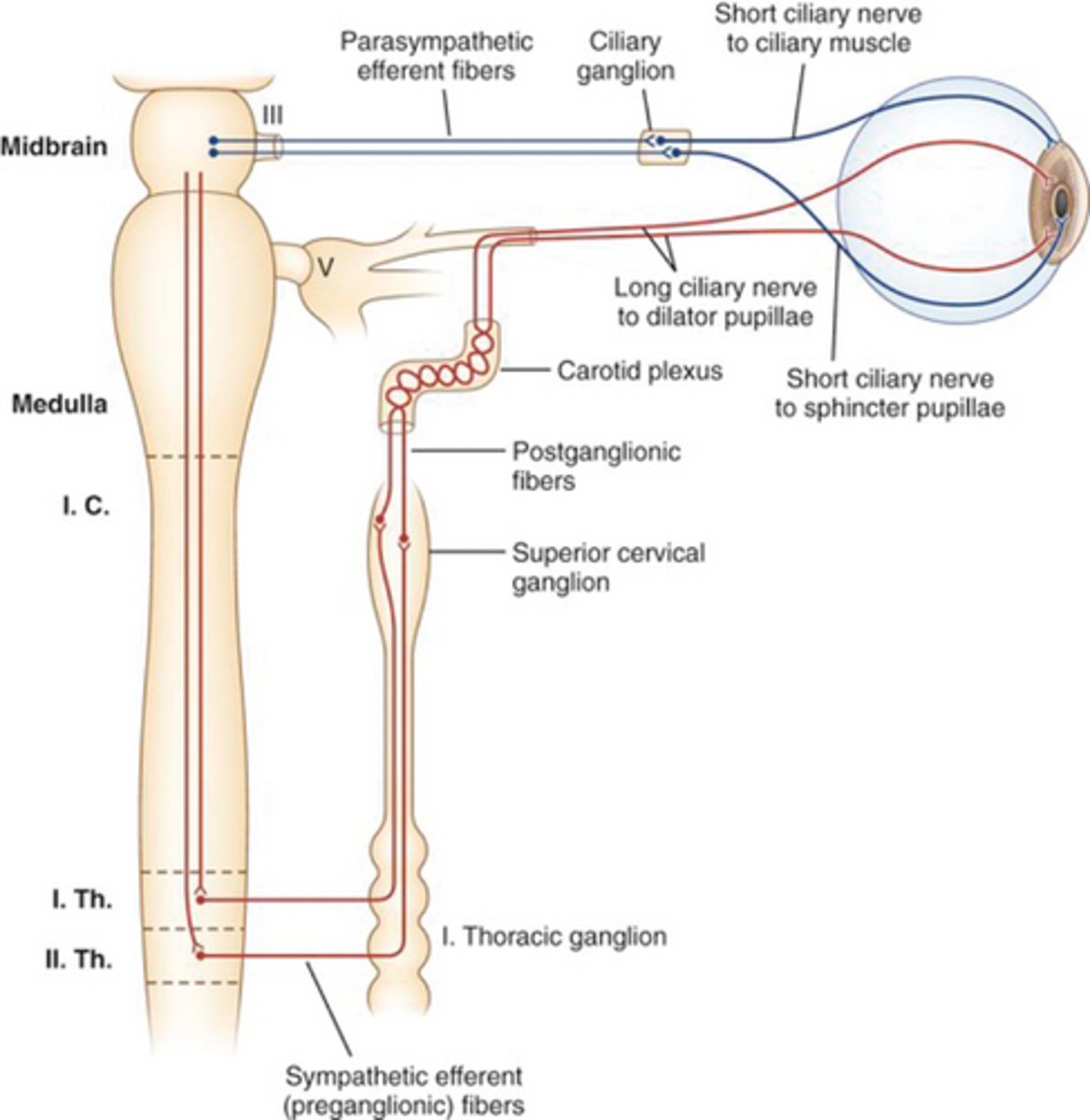
Nerves that innervate sphincter iridis?
Short ciliary nerves
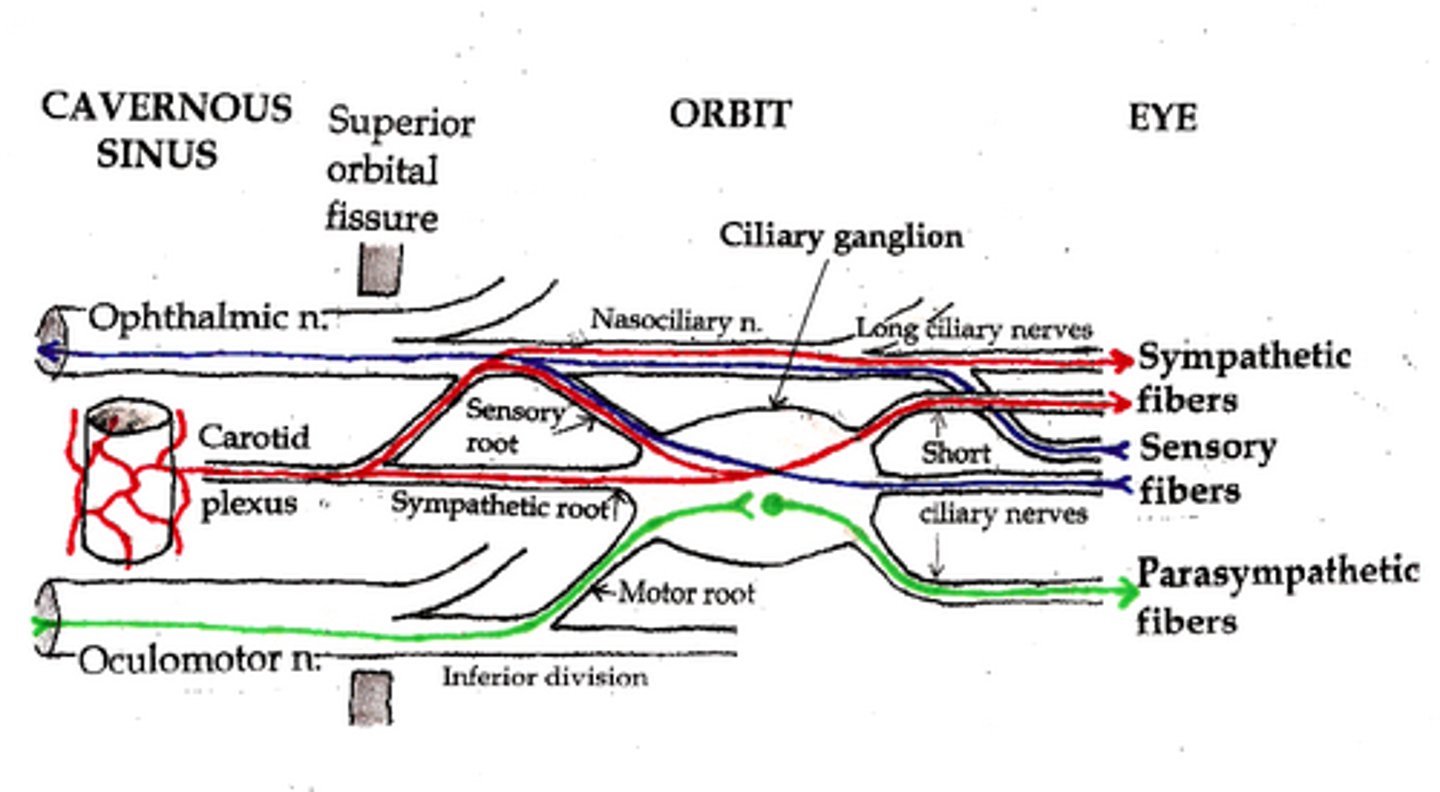
Nerves that innervate dilator pupillae?
Long ciliary nerves
Which iris muscle is stronger?
Sphincter iridis
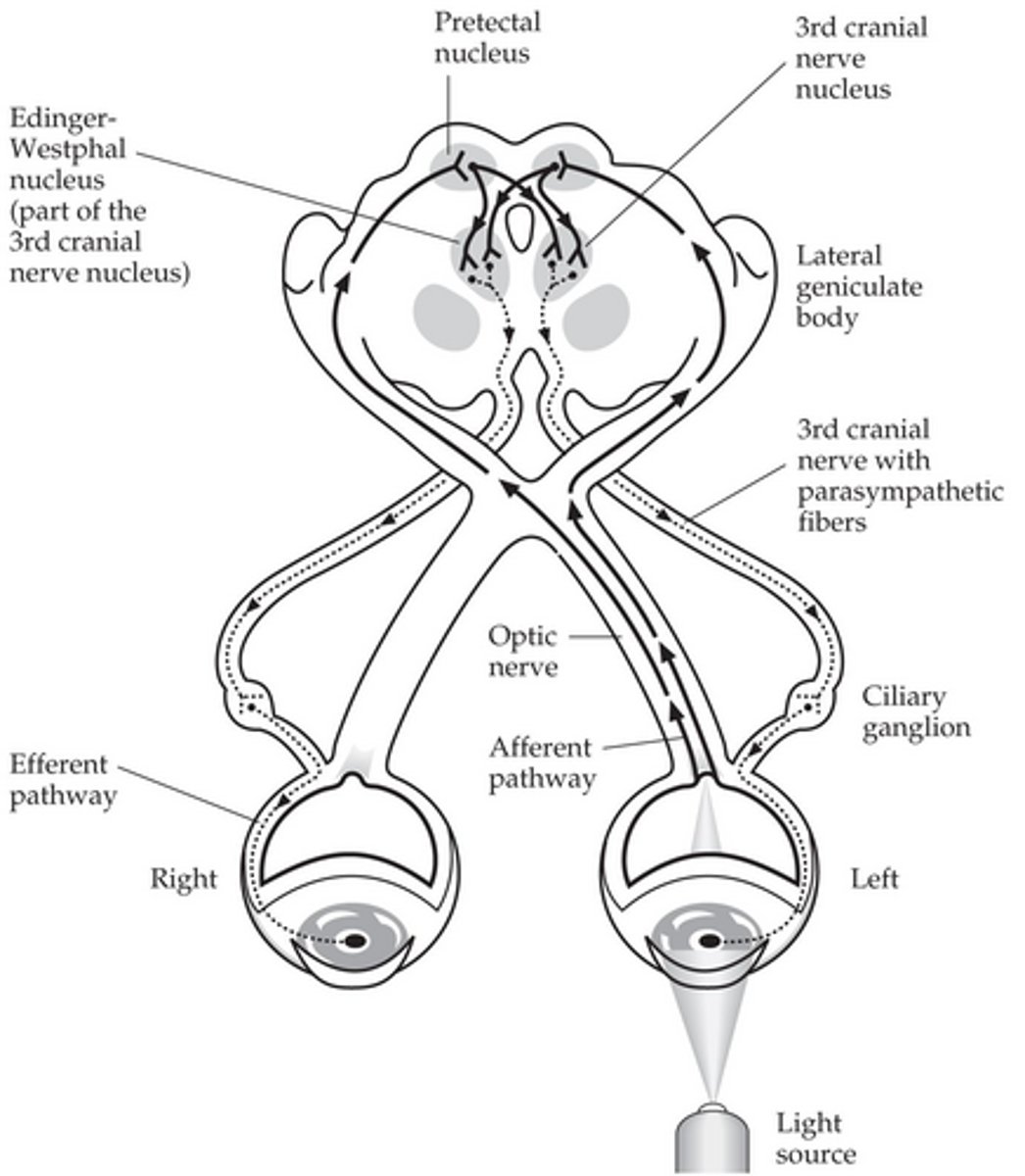
The neurological pathway for pupillary constriction begins at the ______________
Photoreceptors
Afferent pathway of pupillary constriction? (6)
Optic chiasm
Optic tract
Bifurcation of pupillomotor fibers in superior colliculus
Pretectal area
Bilateral interneurons
Edinger Westphal nuclei
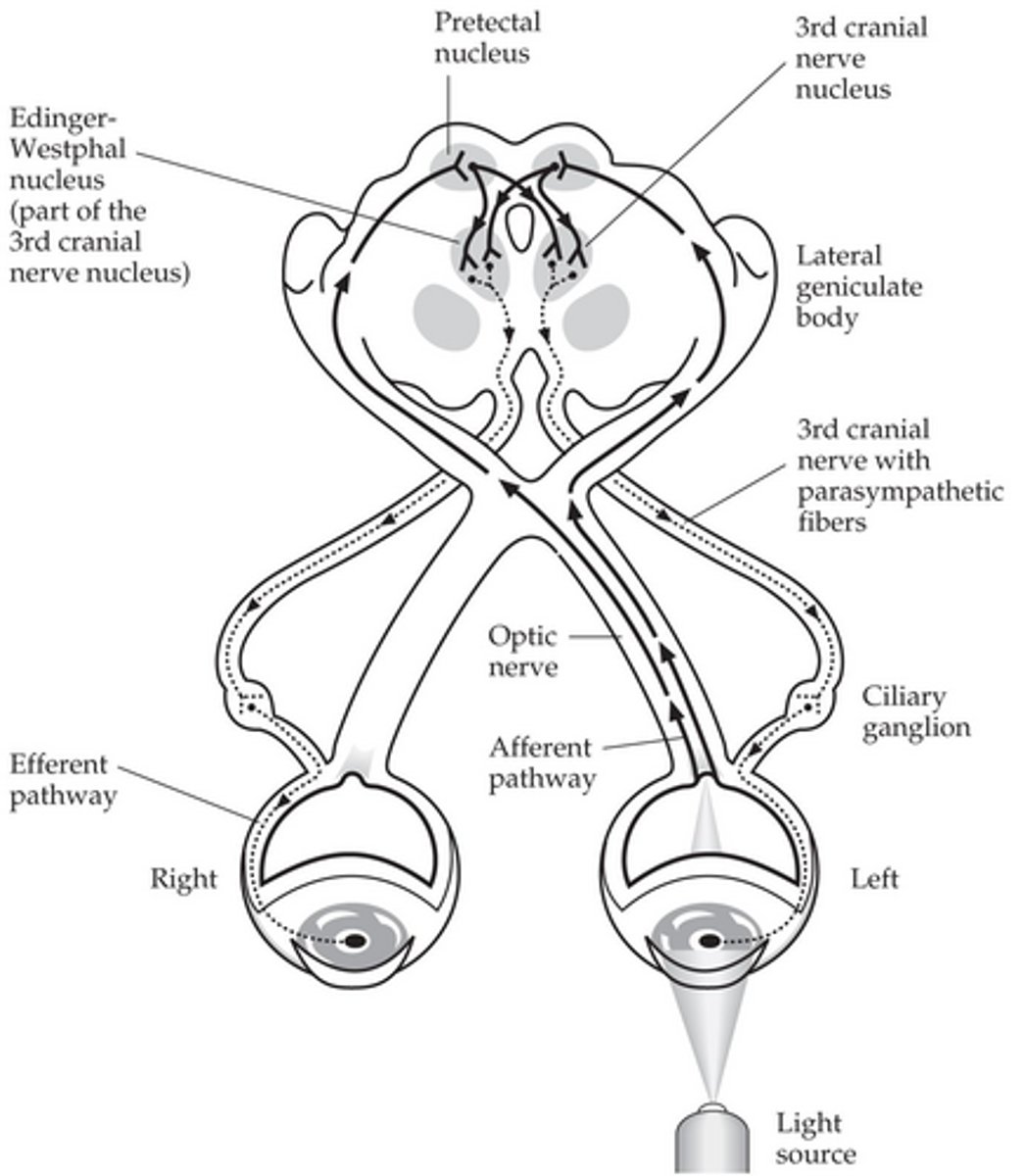
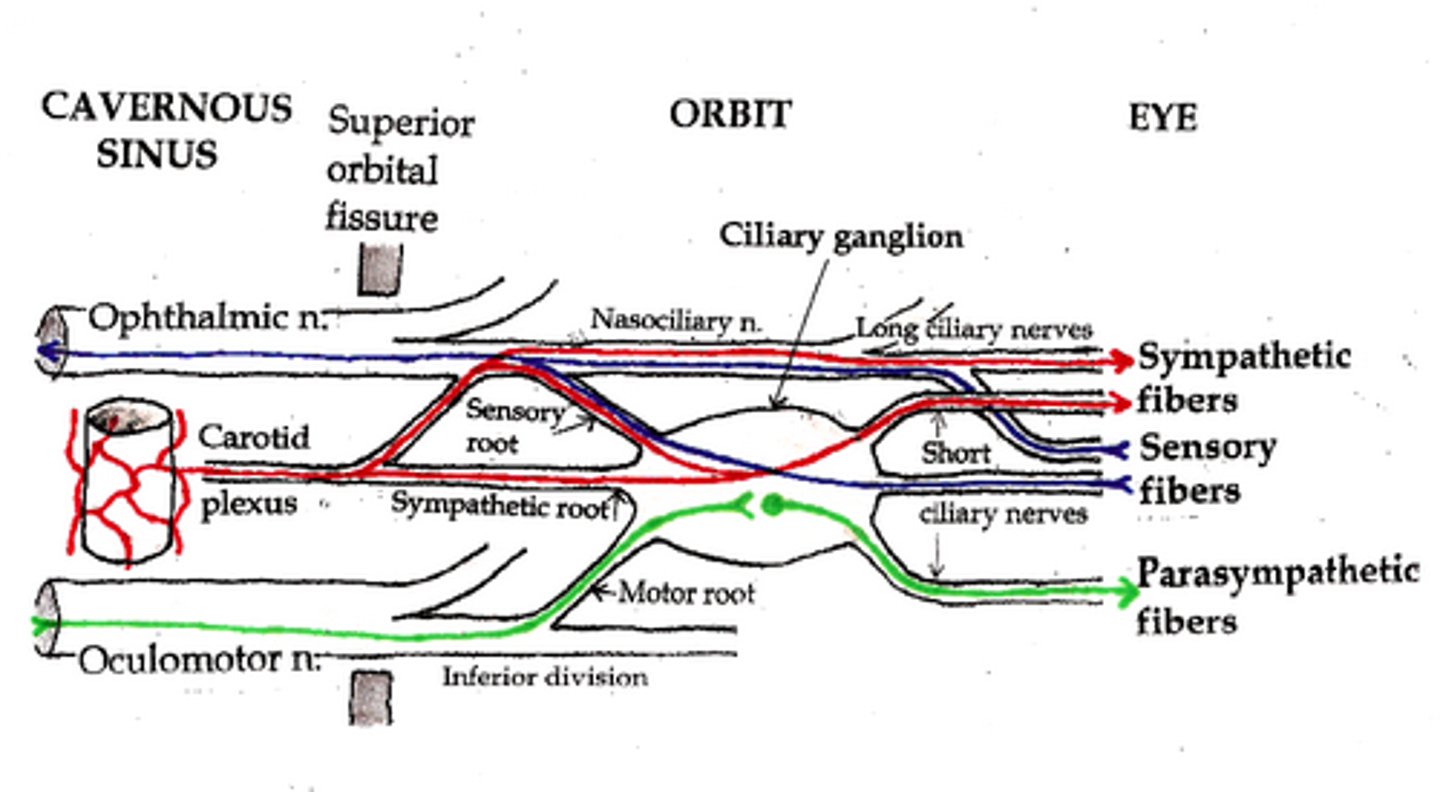
Efferent pathway of pupillary constriction? (5)
Caudal Edinger Westphal nucleus
CN III inferior division
Ciliary ganglion
Short ciliary nerves
Iris sphincter of both eyes
Does pupillary constricting involve cerebral cortex processing?
No
Are there more accommodative or pupillomotor fibers in the ciliary ganglion?
Accommodative
________________ loops to pupillary constriction pathway inhibit it when we are awake.
Corticomesencephalic
Does pupillary constriction to a light stimulus cause change in the other 2 of the near triad?
No
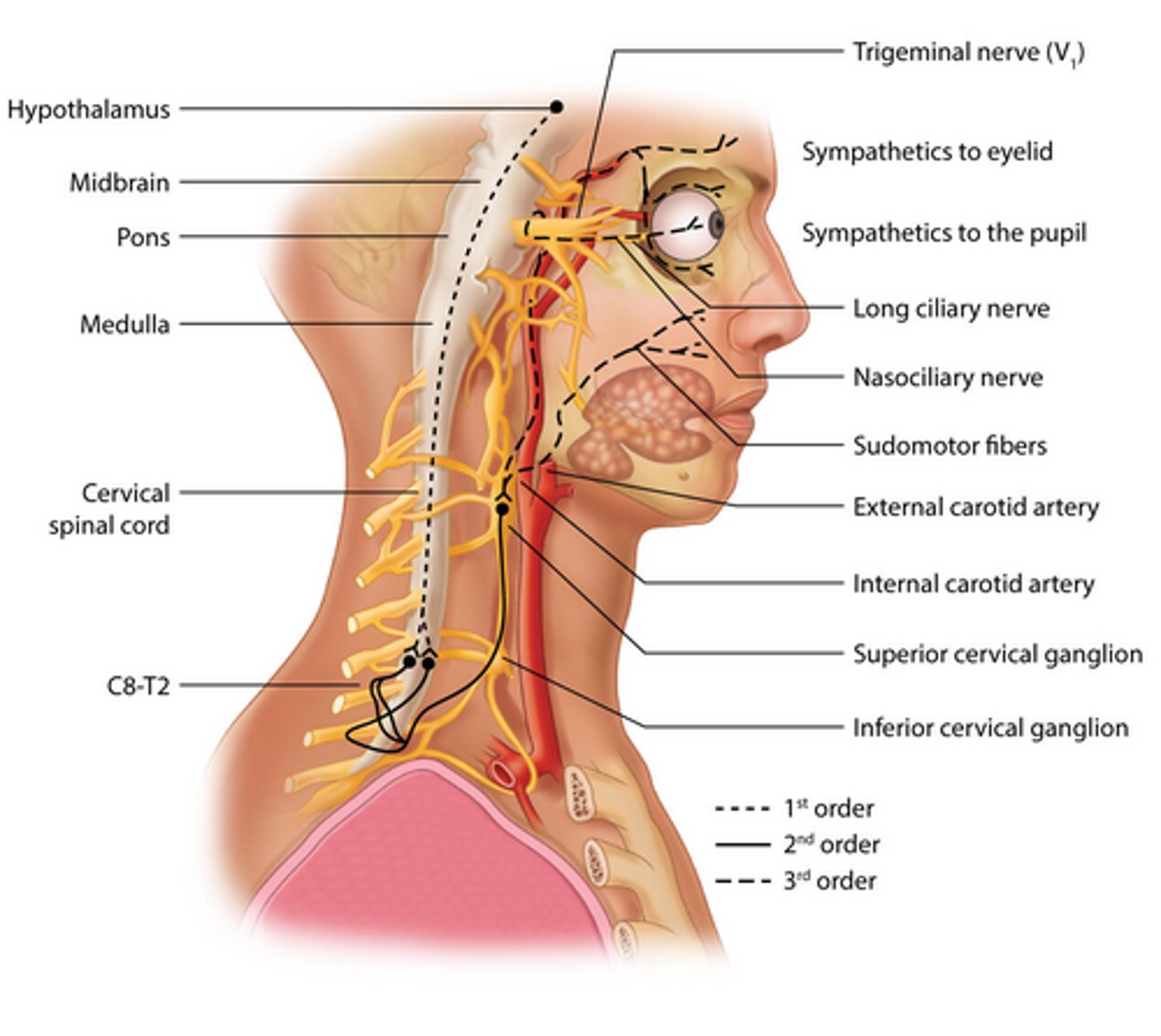
Where does the pathway of pupillary dilation begin?
Posterolateral hypothalamus
Path of central fibers in pupillary dilation? (3)
Descend ipsilaterally
Terminate in intermediolateral cell column
Synapse in ciliospinal center of Budge
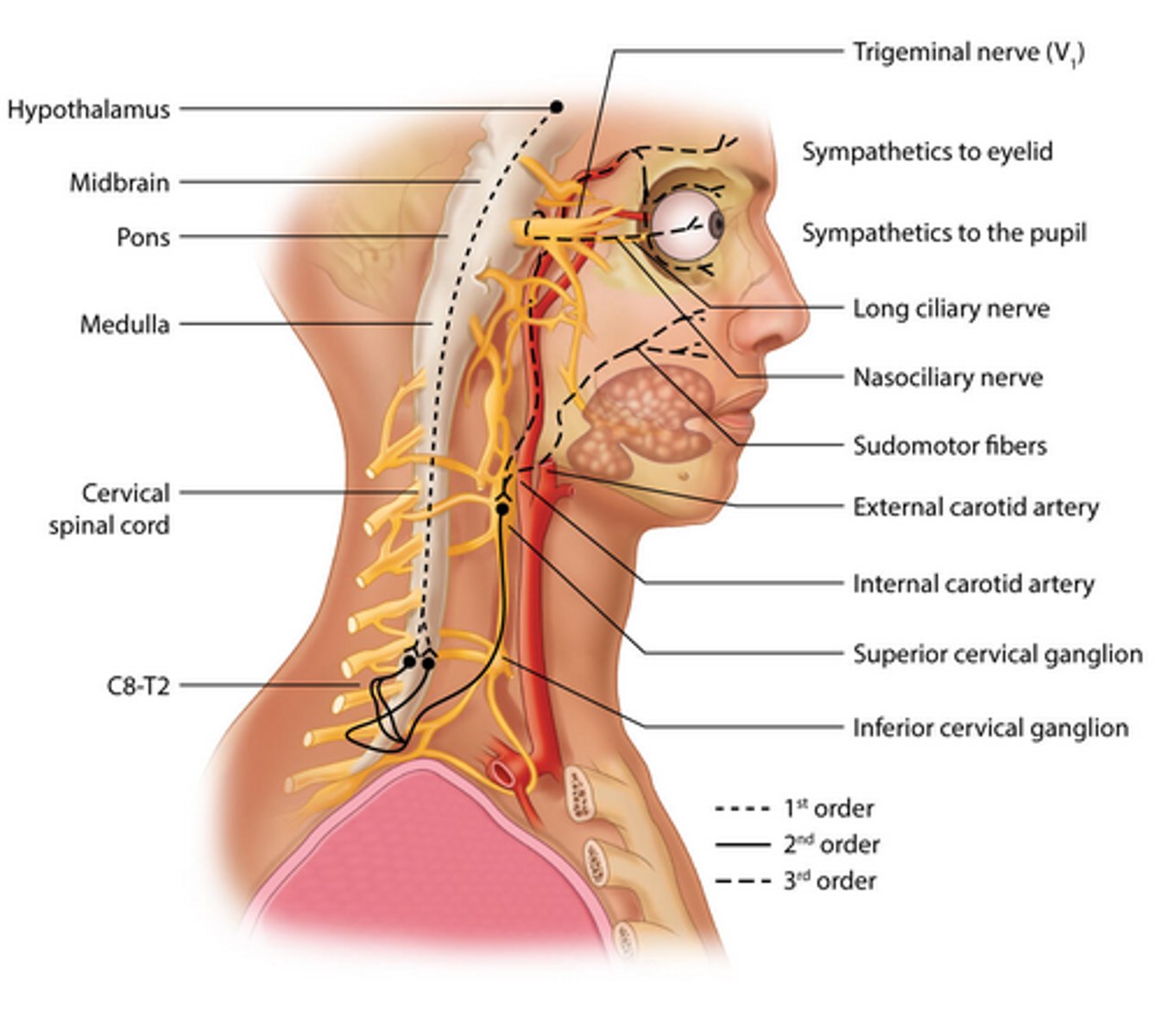
Path of second order/pre-ganglionic fibers in pupillary dilation? (5)
Exit via T1
White rami commuicantes
Sympathetic chain of paravertebral column
Inferior and middle cervical ganglia
Synapse at superior cervical ganglion
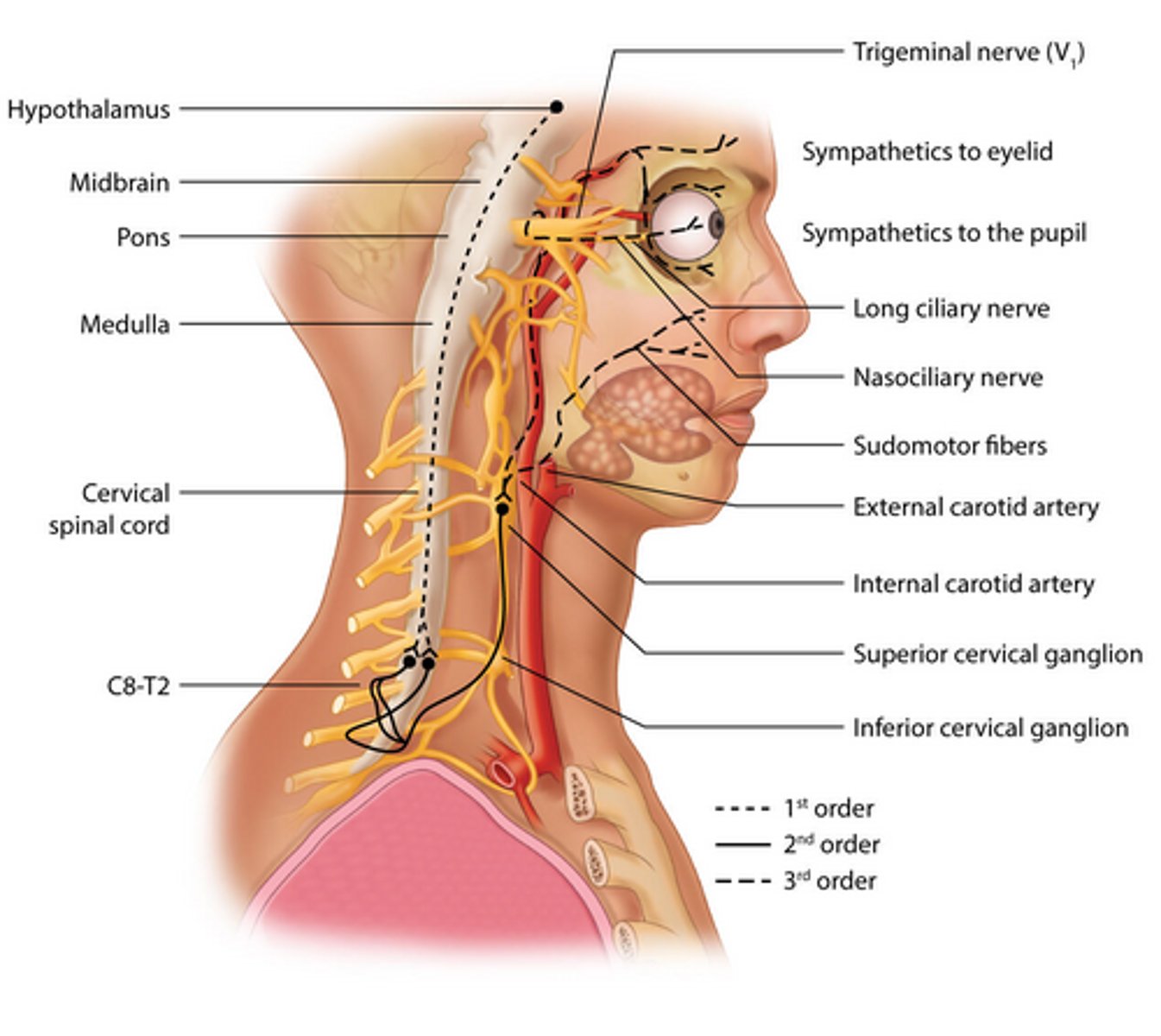
Path of third order/post-ganglionic fibers in pupillary dilation? (5)
Travel with internal carotid
Joins ophthalmic division of trigeminal nerve
Forms a cavernous plexus in the sinus
Through superior orbital fissure
Long ciliary nerves reach iris dilator
Are third order oculosymathetic fibers myelinated?
No
________________________ projections to pupillary dilator pathway stimulate it when we are awake.
Hypothalamomesencephalic
______ anisocoria is a difference of <.5 mm and present in 1/5 of the population
Simple/Essential
Simple anisocoria is more present in (bright/dim) light
Dim
When the larger pupil is the abnormal one, the defect is usually (afferent/efferent)
Efferent
What can cause a large abnormal pupil? (5)
Midbrain damage
Damage to CN III
Damage to ciliary ganglion/nerves
Damage to sphincter muscle
Mydriatic drugs
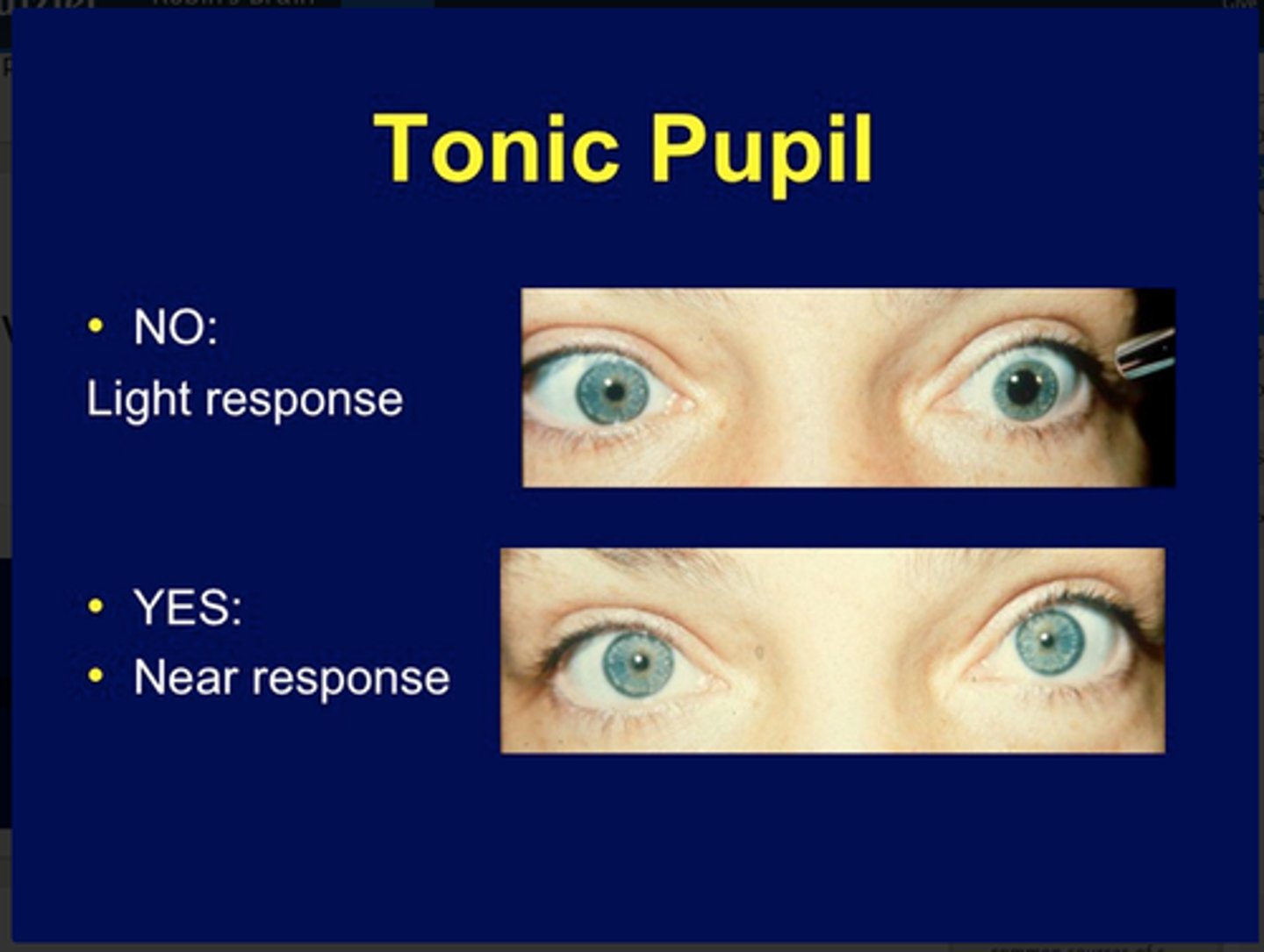
Characteristics of a tonic pupil? (4)
Poor response to light
Stronger response to near target
Accommodative paresis
Cholinergic supersensitivity
Most common efferent pupillary defect?
Adie's tonic pupil
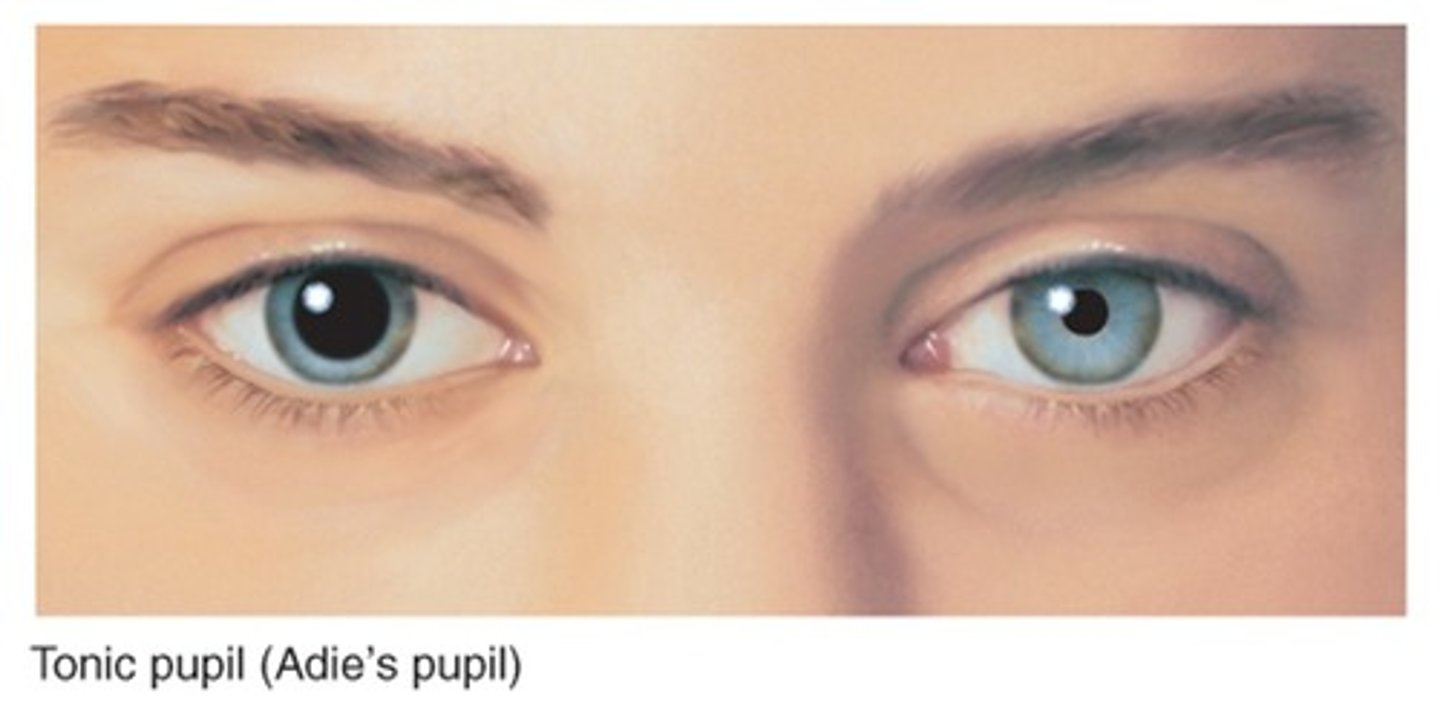
Adie's tonic pupil affects (men/women) more
Women (ladies get Adies!)
Near targets elicit a more robust pupillary response than light response?
Light/near dissociation
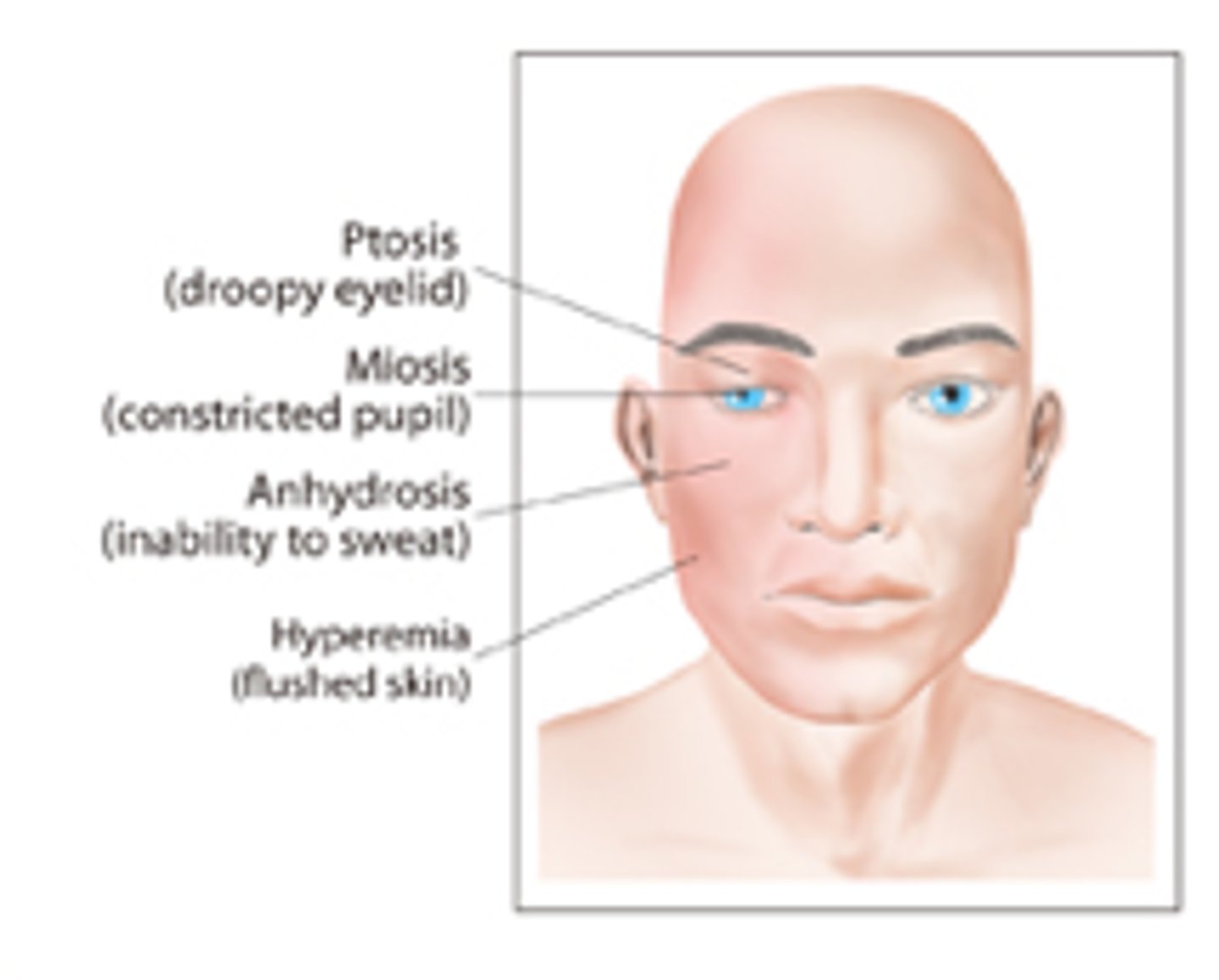
Horner's Syndrome characteristics? (4)
Pupil miosis
Eyelid ptosis
Anhydrosis of half the face/body
Ocular hypotony
_______ Horner's syndrome occurs with damage to the first-order neuron of the pathway
Central
What can cause a central Horner's syndrome? (2)
Medullary infection
Cervical cord injury or disease
Distinguishing symptoms of a central Horner's syndrome? (3)
Vertigo
Sensory defects (audition)
Insufficient sweating on BODY
______________ Horner's syndrome occurs with damage to the second-order neuron.
Pre-Ganglionic
If an infant acquires a Horner's syndrome after a few months of life, why would we refer them for a chest x-ray?
Possible carcinoid tumor and pleuropulmonary blastoma
Tumor that can cause a pre-ganglionic Horner's in adults?
Thoracic/cervical blastoma
________________ Horner's syndrome occurs with damage to the third order neuron.
Post-ganglionic
Symptoms that a patient may have along with a post-ganglionic Horner's? (2)
Cluster headache
Migraine
Diseases that may result in a post-ganglionic Horner's? (2)
Cavernous sinus disease
Carotid dissection
An eye that is positive for APD will have a (direct/consensual) response but will NOT have a (direct/consensual) response to light.
Consensual
Direct
Rare cause of APD?
Optic tract disease
What does retrobulbar mean?
Behind the eye, like ON damage behind lamina cribosa
What begins as optic neuritis may become _____ ______.
Optic atrophy
Can we regenerate function following optic atrophy?
Not usually
Which 3 factors decide if a retinal disease can cause an APD?
One eye must be more affected
Over 1/2 of retinal function affected
Significant macular involvement
What are some examples of retinal diseases that could cause an APD? (4)
Retinal detachment
Macular disease (AMD)
Amblyopia
Posterior staphyloma
"Most famous" example of a light/near dissociation?
Argyll Robertson pupil
Characteristics of an Argyll Robertson pupil? (4)
Light sensitive retina
Little to no light response
Brisk response to accommodative target
Small, difficult to dilate pupil
Argyll Robertson pupil was commonly found in patients with _____ _____.
Tabes dorsalis (a dysfunction associated with syphillis)
Is an Argyll Robertson pupil common?
No
Other causes that can mimic an Argyll Robertson pupil? (3)
Vascular anomalies in cerebral aqueduct
Diabetes
Alcoholic neuropathy
Dorsal midbrain syndrome that can cause a light/near dissociation?
Parinaud's syndrome
What is the cause of Parinaud's syndrome?
Lesion, typically in dorsal midbrain centered on paraqueductal gray
Other symptoms of Parinaud's syndrome?
Vertical gaze paralysis
Eyes converge and retract
pseudo-Argyll Robertson pupil