Week 9 the heart and blood pressure II
1/33
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
34 Terms
systolic and diastolic blood pressure:
troughs are diastolic, peaks are systolic
ventricles have larger range than arteries, ventricle go almsot to 0 arteries don’t
pulse pressure
systolic pressure minus diastolic pressure
mean arterial pressure
diastolic pressure + 1/3 (pulse pressure)
MAP = 80 + 40/3 = 93.3
should be between 70-100
when MAP is too low (<60) - organs don't get enough oxygen, syncope shock
when MAP is too high - the heart has to work too hard, muscle will enlarge. Increase oxygen demand by the heart, vascular injury, end organ damage, stroke
pulse pressure should be:
40mmHg, this is typically 30-40 in a healthy adult
extremely low like 25mmHg or less: low stroke volume, weak ventricular contractions
pulse pressure > 60: predictor of heart attacks or other cardiovascular disease
arterial baroflex system is:
key regulator of MAP
factors that influence mean arterial pressure:
effectiveness of the heart as a pump/cardiac output (heart rate, stroke volume), fast autonomic
resistance of the system to blood flow (diameter of the arterioles), fast, autonomic, local control mechanisms
blood volume determines by fluid intake, fluid loss (passive, regulated at kidneys), slower, hormonal regulation
relative distribution of blood between arterial and venous blood vessels (diamter of veins), fast autonomic
heart valve opening:
A: aortic valve opens
B: aortic valve closes
C: mitral valve close
D: mitral valve open
E: end diastolic volume
F: end systolic
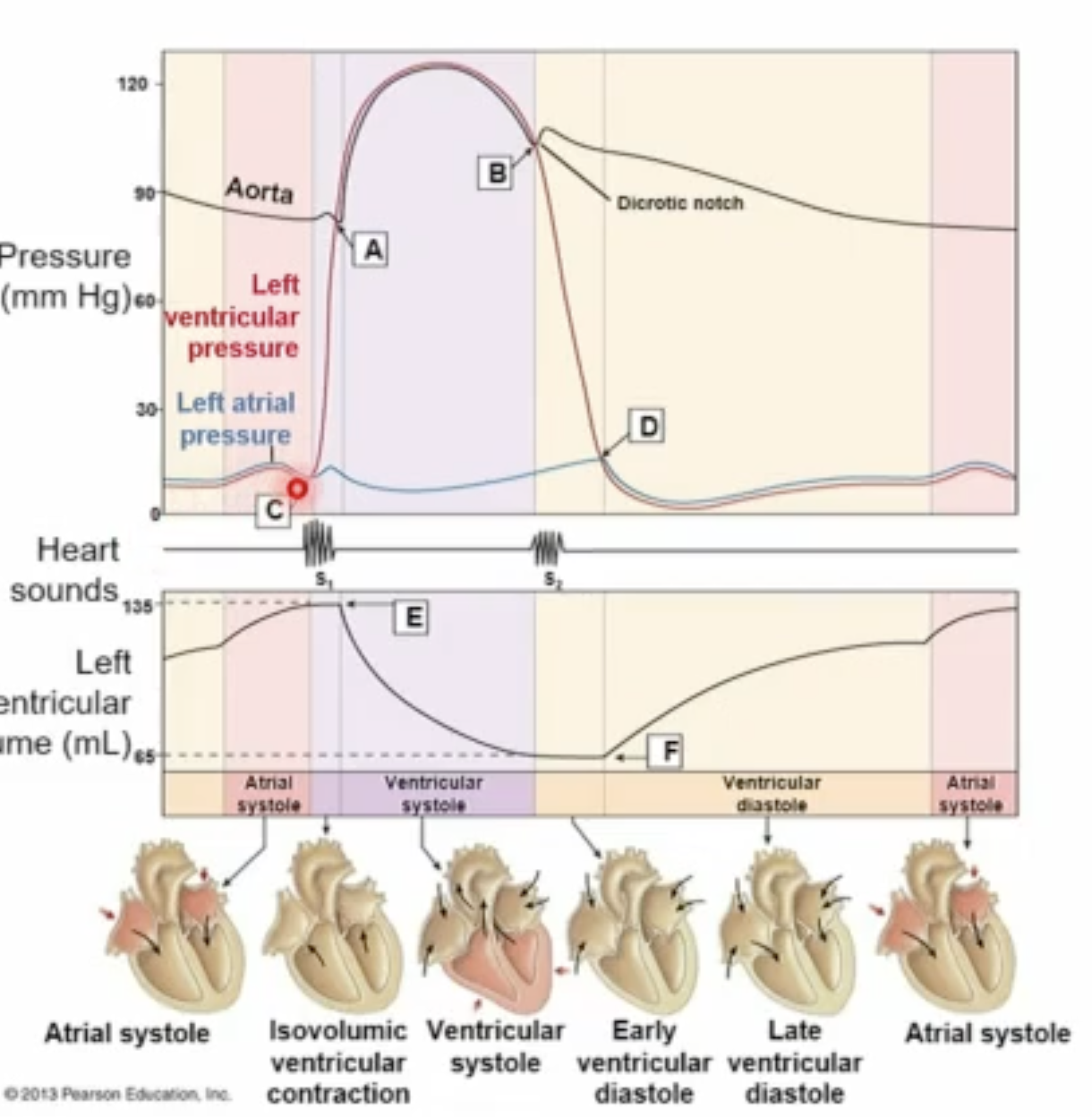
volume
what determines mean arterial pressure?
mean arterial pressure is proportional to your cardiac output times the resistance of your arterioles
Frank Starling Law
The relationship between end-diastolic volume (EDV) and stroke volume (SV) (amount of blood flowing back into the heart before systole determines the stroke volume)
As a larger volume of blood flows into the ventricle, the blood will stretch the walls of the heart, causing a greater expansion during diastole, which in turn increases the force of the contraction and thus the quantity of blood that is pumped into the aorta during systole
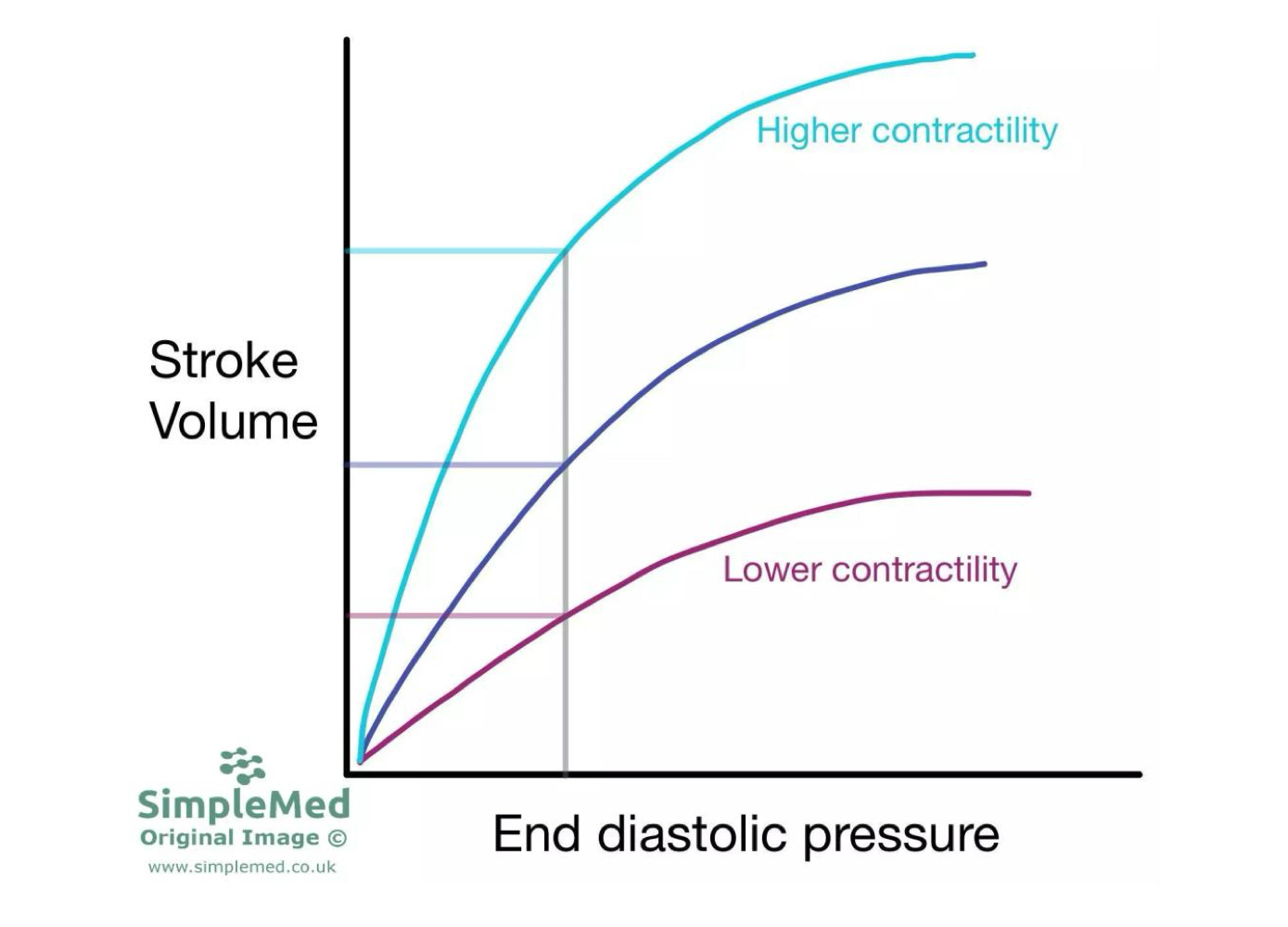
frank-starling law graph
Factors that increase cardiac contractility will lead to an upward and leftward shift of the curve.
In contrast, factors that decrease cardiac contractility will lead to a downward and rightward shift of the curve
Stronger contraction = more blood out, less left behind and vice versa
the frank-starling mechanism in vertebrate cardiac myocytes
The cellular mechanisms underlying the Frank–Starling response include an increase
in myofilament sensitivity for Ca2+, decreased myofilament lattice spacing and
increased thin filament cooperativity.
sympathetic nervous system regulation of heart rate
Pathway
Preganglionic neurons originate in the thoracic spinal cord.
Postganglionic neurons release norepinephrine (NE) onto the heart.
NE binds β₁-adrenergic receptors on cardiac cells.
Results
SA node fires action potentials more frequently.
AV node conducts signals faster.
Ventricles contract more strongly.
Overall effects:
↑ Heart rate (positive chronotropy)
↑ Conduction velocity (positive dromotropy)
↑ Contractility (positive inotropy)
Cellular Mechanism
β₁ receptor activation increases cAMP, which:
Opens more pacemaker ion channels.
Increases Ca²⁺ entry.
Causes the SA node membrane potential to reach threshold faster.
parasympathetic nervous system regulation of heart rate
Effect: Decreases heart rate.
Pathway
Mainly through the vagus nerve (cranial nerve X).
Postganglionic neurons release acetylcholine (ACh).
ACh binds M2 muscarinic receptors.
Results
SA node fires more slowly.
AV node conduction slows.
Overall effects:
↓ Heart rate (negative chronotropy)
↓ Conduction velocity (negative dromotropy)
Cellular Mechanism
M2 receptor activation:
Decreases cAMP.
Opens K⁺ channels.
Hyperpolarizes pacemaker cells.
Slows the rate of spontaneous depolarization.
As a result, it takes longer to reach threshold for the next heartbeat.
where blood is needed most to least:
lungs
brain
heart
liver and digestive tract
kidneys
skeletal muscle
skin
bone and other tissues
myogenic auto-regulation - regulation of blood flow at the tissue level
activation of a mechanoreceptor depolarizes muscle, contraction
Myogenic autoregulation is the ability of certain blood vessels (especially arterioles) to automatically adjust their diameter in response to changes in blood pressure, helping keep blood flow relatively constant.
paracrine: active and reactive hyperemia - regulation of blood flow at the tissue level
some vasoactive paracrines are related to inflammation
Paracrine regulation of blood flow refers to local chemical signals released by tissues that act on nearby blood vessels to adjust blood flow according to metabolic demand.
decrease O2, increase CO2, NO lead to vasodilation
active hyperemia
Definition: Increased blood flow to a tissue when its metabolic activity increases.
What happens?
When a tissue becomes more active (e.g., exercising skeletal muscle):
O₂ consumption increases.
CO₂ production increases.
H⁺, K⁺, adenosine, lactate, and other metabolites accumulate.
These metabolites act as paracrine signals that cause arterioles to dilate.
reactive hyperemia
Definition: A temporary increase in blood flow after blood supply has been blocked and then restored.
What happens?
Blood flow is reduced or occluded.
Tissue continues metabolizing.
Vasodilatory metabolites accumulate.
Oxygen levels fall.
When the blockage is removed, arterioles are already strongly dilated.
Result
Blood flow temporarily rises above normal.
Excess flow repays the "oxygen debt."
Accumulated metabolites are washed out.
Blood flow gradually returns to baseline.
sympathetic nervous system controls most:
vascular smooth muscle
APs in vascular smooth muscle
more firing - more contraction
less firing - less contraction
the microcirculation
1) every cells is within 0.1µm of a capillary
2) capillary density is related to the metabolic activity of the tissue (even in bones)
3) capillaries are the only “open” part of the vasculature system
4) an adult human has 50,000 miles of capillaries'
5) capillaries are made of a single layer of flattened endothelial cells
6) diameter of a capillary is 1 red blood cell, many types of white blood cells are too big
arteriole
controllable diameter
smooth muscles
capillaries
precapillary sphincters
sympathetic control
regulate blood flow at the tissue level
neuron firing tells them to contract
metarterioles
can act as bypass channels
there is also the arteriovenous bypass, bypasses capillaries if sphincters are closed
sphincters relaxed vs contracted
more blood flow when relaxed, less blood flow when contracted
velocity of blood flow:
velocity is reduced with larger cross-sectional areas
ex: capillaries have least velocity and largest cross-sectional area
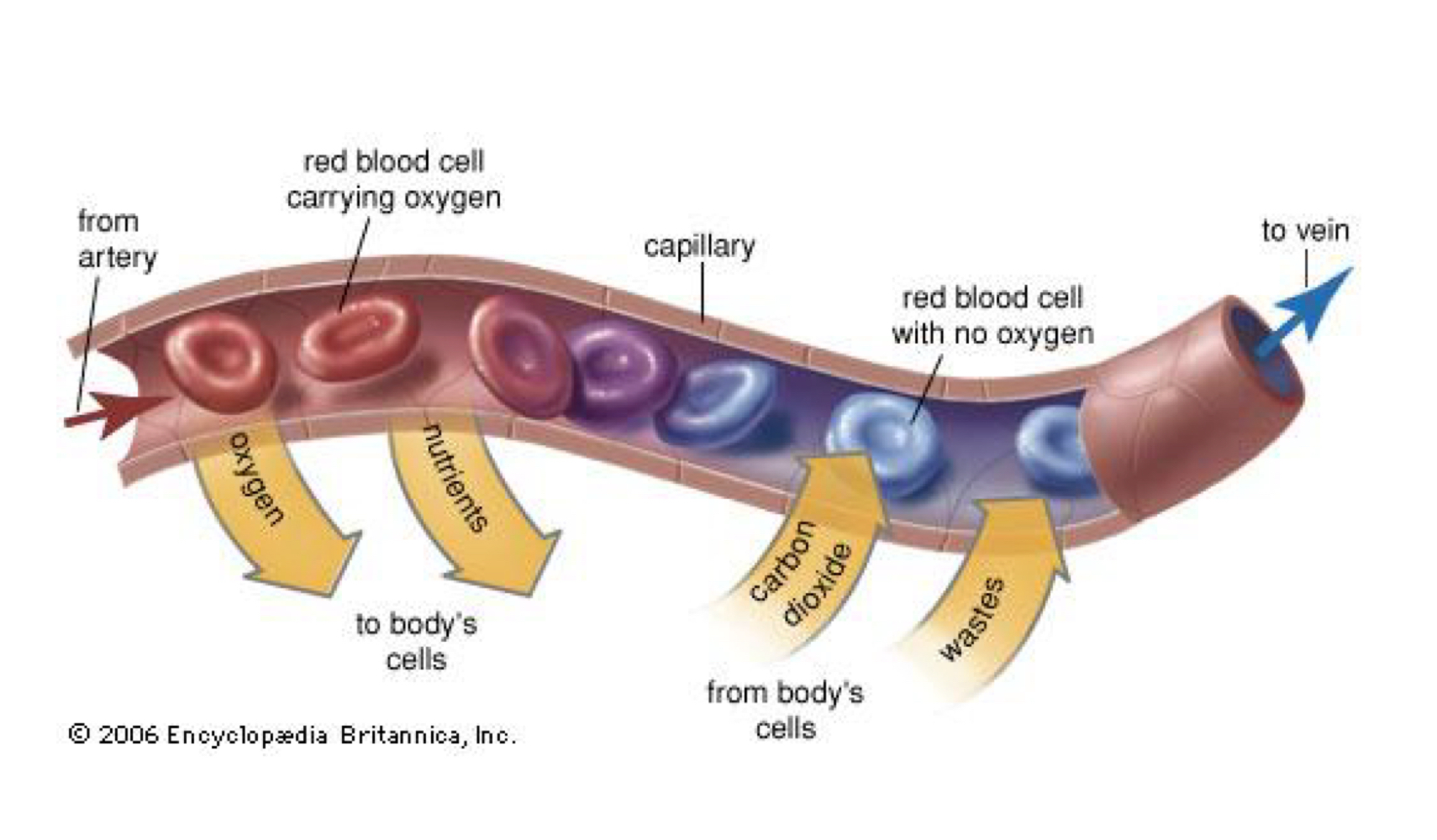
exchange of material takes place at the capillaries:
most capillaries are continuous capillaries with leaky junctions
endothelial cell junctions allow water and small dissolved solutes to pass
transcytosis: brings proteins and macromolecules across endothelium, some vesicles may fuse to create temporary channels
fenestrated capillaries
large pores
eg posterior pituitary, OT and AVP and kidney
help transport material as well as junctions and transcytosis
pressure does what through arterial system?
decreases
arteries high pressure
capillaries/veinous low pressure
bulk flow of fluid:
arteriole to net filtration to lymph vessels and net absorption, out to venous circulation and venule
bulk flow is driven by hydrostatic and osmotic pressure (Starling forces)
filtration - flow from blood into tissue. absorption back into venous side, a function of pressure
bulk flow in systemic capillaries
hydrostatic pressure forces fluid out of the capillary
colloid osmotic pressure of proteins with the capillary pulls fluid into the capillary
filtration:
arteriel end net filtration pressure = +10mmHg
fluid exits capillary since hydrostatic pressure is GREATER than blood colloidal osmotic pressure
no net movement
mid capillary net filtration pressure = 0mmHg
bc hydrostatic and blood colloidal osmotic pressure are equal
reabsorption
venous and net filtration pressure = -7mmHg
fluid re-enters capillary since capillary hydrostatic pressure is less than blood colloidal osmotic pressure (25mmHg)