Neurology 2
1/128
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
129 Terms
What is Neurological Rehabilitation?
A process helping individuals with disability achieve optimal function and health.
6 Key Characteristic in Neurorehabilitaion
Motor learning
Outcome based & Inclusive
Collaborative care
Culturally responsive practice
Tailored treatment
Critical Evaluation
What does neurological rehab require?
Knowledge, skills, education, advice, and active partnership with patient/family.
Requires active partnership between the patient, their family and health and social care professionals.
Why is participation highly valued?
Because changes at impairment/activity level only matter if they improve participation
What are the three major historical approaches to Neurorehabilitation?
Motor Learning
Orthopedic
Neuro-facilitation
What is collaborative care?
Team‑based, interdisciplinary partnership improving outcomes
Improved survival rates
Earlier discharge home
Improved independence
Improved learning and development
What is patient-centered care?
Shared decision‑making based on patient values and goals
What are common neurological impairments?
Weakness (← most common after a stroke, followed by spasticity)
Fatigue
Tone disorders
Coordination issues
Visuospatial & vestibular disorders
Sensation issues
What are 5 common functional challenges?
Mobility
Self-care
Communication
Community participation
Domestic life (e.g. meal prep)
5 Key Aspects of Any Neurological Physiotherapy Treatment Plan
Functional movement re-education
Strength & Motor control
Flexibility
Exercise
Impairment-specific interventions
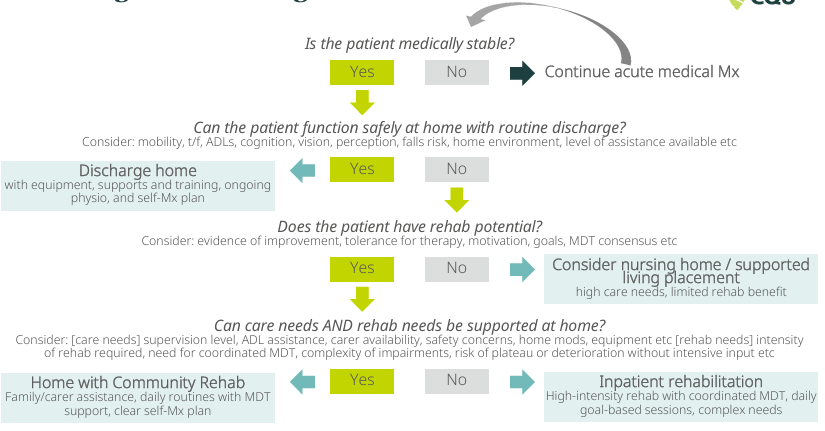
What determines discharge?
Medical stability → safe home function → rehab potential → ability to support rehab at home
Common causes of an Acquired Brain Injury (ABI)
Stroke (leading cause)
Trauma
Infection
Poisoning
Hypoxia
Degenerative neurological diseases
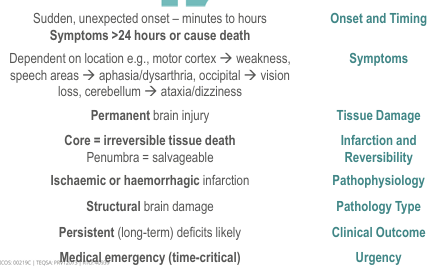
What defines a Cerebrovascular Accident (stroke/CVA)?
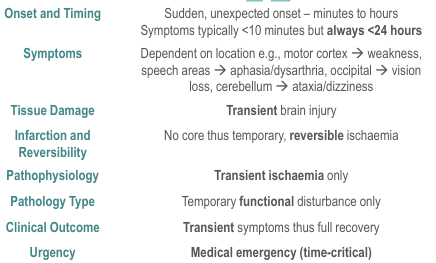
What defines a Transient Ischemic Attack (TIA)?
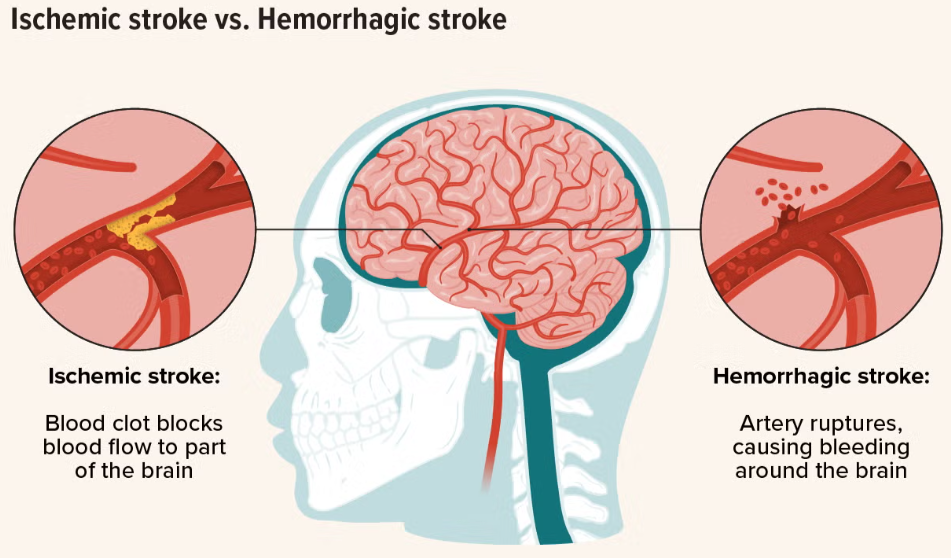
What are the two major stroke types?
Ischaemic (~80%)
Thrombotic, Embolic, Systemic hypo-perfusion
Haemorrhagic (~20%)
Subarachnoid, Intracerebral
3 Modifiable & 3 Non-modifiable risk factors for a stroke
Modifiable
Obesity
Inactivity
Smoking
Non-modifiable
Increasing age
Family history
Male gender
What are the key steps in acute stroke care?
FAST recognition, reperfusion, stroke unit care, early rehab, care plan
F - Face droop
A - Arm weakness
S - Speech slurred
T - Time is critical 000
What is the time window for thrombolysis/reperfusion in an acute ischemic stroke (clot breakdown) + what is it?
Within 4.5 hours of symptom onset
Administration of a clot-busting medication (a thrombolytic agent) through a vein
It works by dissolving the blood clot that is blocking cerebral blood flow
When should rehab needs be assessed?
Within 24-48 hours of admission
What are the 3 priorities in acute neuro assessment?
Cardiorespiratory → Manage potentially life-threatening complications first
Functional → Early mobilisation = gold standard = maximises rehab potential and reduces complications
Impairments → Supports determination of diagnosis and prognosis
Minimum requirements to attempt standing?
Medically stable, cooperative, pain managed, DVT clear, ≥3/5 LL strength
3 Common Acute Measurement Tools
Coordination
Muscle strength
Balance
What are the aims of acute physiotherapy? POPD
Provide respiratory care
Optimise musculoskeletal integrity
Promote restoration of motor function
Discharge planning
What are the 5 steps of motor learning‑based rehab?
Establish baseline → Prepare task → Instruction → Determine practice strategy → Perform repetitive practice
4 Steps of starting Functional Rehab?
Develop ocular control
Develop postural control
Develop coordination
Retrain UL and LL function
What mechanisms cause ischemic stroke?
Large artery atherosclerosis (~50%)
Small vessel disease (~20–25%)
Cardioembolism (~20%)
Other (5–10%): dissection, vasculitis, pro‑thrombotic disorders
Why does stroke mechanism matter for physiotherapy?
It influences lesion size, location, stroke syndrome, prognosis, and expected motor/sensory/cognitive deficit
2 Types of a Hemorrhagic Stroke
Intracerebral - Bleeding within the brain tissue itself
Caused by: Trauma + chronic HTN
Subarachnoid - Bleeding between the brain and arachnoid space
Caused by: Aneurysm rupture or vascular malfunctions
Other causes - anticoagulation, drugs, bleeding disorders
What happens when blood flow to the brain is disrupted in a large vessel?
Internal carotid Posterior: monocular blindness
Vertebrobasilar system:
contralateral motor/sensory deficits
4D’s
vertigo
nausea/vomiting
limb ataxia
coma
Examples of what happens when blood flow to the brain is disrupted in a medium vessel?
ACA: “motor“
gait apraxia (forgetting how to walk)
rigidity
MCA:
Homonymous hemianopia (loss of half visual field in both eyes)
Neglect
PCA: “visual“
Alexia (cant read)
hallucinations
What happens when blood flow to the brain is disrupted in a small vessel?
pure motor hemiparalysis
pure sensory deficit
hemiparesis ataxia
Dysarthria + clumsy hand syndrome
4 types of Stroke Classifications
Total Anterior Circulation Syndrome (high mortality) (low likelihood of indep. walking)
contralateral hemiplegia, homonymous hemianopia, cerebral dysfunction
Partial Anterior Circulation Syndrome (high chance recovery) (much higher likelihood of independence)
Any two of hemiplegia/sensory loss, hemianopia or higher cortical dysfunction
Lacunar Syndrome (less disability)
Pure motor, pure sensory, sensorimotor, or ataxic hemiparesis.
No cortical signs or visual field loss.
Posterior Circulation Syndrome (good recovery)
Brainstem/cerebellar signs, CN palsies, bilateral deficits, eye movement disorders, isolated hemianopia
Primary vs secondary injury in intraceberbal haemorrage?
Primary: haematoma + mass effect
Secondary: blood toxicity, oxidative stress, inflammation → peri‑haematoma oedema
Key predictors of good recovery?
Mild initial severity
Presence of cortical signs
Early sitting balance
Early voluntary movement
Intact cognition
When should mobilization begin? + recommended therapy dose?
Avoid intensive mobilization in first 24 hours
Brain vulnerability, fatigue, not advantageous
Mobilize by 48 hours if medically stable
support neuroplasticity
Dose → 2 hours active task practice (in a time frame of 3 scheduled hours) but still encourage practicing outside of scheduled therapy time!
What must be screened before rehab?
UL sensory-specific training, visual acuity, visual fields & eye movement disorders
What improves ADL performance?
Individualized goals, tailored strategies, assistive technology, VR adjunct
What should physios do with cognitive/communication issues?
Recognize → adapt → refer (SP, OT, neuropsych)
Other complications physios must recognise?
Nutrition, hydration, oral hygiene, mood, behaviour, fatigue, sleep disorders
Ischemic cascade: What is the “Ischemic core” and the “penumbra?”
Ischemic core → Brain tissue destined to die
Penumbra → Salvageable brain tissue area (viable for a few hours (around 3–6 hours)
Why is this clinically important?
This is the tissue that can be saved with rapid treatment
Deciding on a Discharge Location: Clinical Decision Flow
The earlier stroke rehabilitation is commenced, the better the patient’s outcome
When does a stroke (e.g. TACS) become an infarct (e.g. TACI)??
when brain imaging confirms there is actual tissue death (infarction) in that vascular territory
What is Hemiparesis vs Hemiplegia?
Hemiparesis: weakness on one side of the body, Hemiplegia: paralysis on one side of the body
What are the 3 stages of Stroke Recovery?
Acute → First 24hours, medical stability is the priority
Stabilize, Prevent & Mobilize
Subacute → 1 week-6 months, intensive rehab to promote neurological recovery
Chronic → +6months, focus shifts to long-term management & adaptation
What are the 4 key physio focus areas in stroke rehab?
Gait training
Task-specific training
Balance
Strength
What is a TBI (Traumatic Brain Injury)?
It’s a type of Acquired Brain Injury
Caused by external mechanical force (e.g. blunt impact)
Results in permanent or temporary impairments
Affect 15–45-year-olds mainly (due to risk taking behaviours/sports)
“Concussion”
TBI Mechanisms of Injury (3)
Primary → Mechanical forces acting on brain (e.g. deceleration)
Secondary → The physiological aftermath (e.g hypoxia)
Associated → lead to associated peripheral injuries
3 Key features (each) of a Primary TBI and Secondary TBI
Primary → Immediate, axonal injuries, hemorrhages
Secondary → Delayed, reduced blood flow, disrupted autoregulation
What domains are commonly affected after TBI?
Physical, cognitive, behavioral, sensory, perceptual, lifestyle
What are 5 common health issues after TBI?
Seizures
Dizziness
Pain
Post-concussion syndrome (PCS)
Mental health disorders
Coma vs post-traumatic amnesia (PTA) vs Vegetative state in a TBI patient
Coma: No eye opening, no response to pain, no sleep‑wake cycles, unresponsive
PTA: period from accident until person is oriented to surroundings (less than 5 minutes to more than 28 days)
Vegetative → wakeful, reduced responsiveness with no evident cerebral function, brainstem usually intact
What makes up the Glascow Coma Scale?
Eye opening response (1-4 score)
Best verbal response (1-5 score)
Best motor response (1-6 score)
^ Higher the total, better the patient
Physio aims of Acute Medical Management
Stabilize patient
Prevent further neurological damage
Cease bleeding
Monitor ICP + conscious state
2 common autonomic, sensory and motor changes after TBI?
Autonomic → sweating and dilated pupils
Sensory → visual field loss and dizziness
Motor → dysphagia and poor balance
2 common cognitive, behavioral + participation changes after a TBI?
Cognitive → impaired memory and language difficulties
Behavioral → depression and irritability
Participation → social roles and driving
Recovery timeline for a TBI?
Mild TBI → days to months; 1-20% still symptomatic after 3 months
Moderate TBI → rapid in first 3-6 months, slower over years (due to neuroplastic factors)
Recovery is non-linear and highly variable
Severity indicators:
Duration of coma
Length of PTA
Initial GCS score
Severe TBI often results in:
Long-term disability
Cognitive/behavioural changes > physical deficits
TBI vs CVA patient presentation
TBI often multi-system trauma
Higher prevalence of impairments
Coexisting musculoskeletal injures more common
Fatigue, headaches, sleep disturbances more common
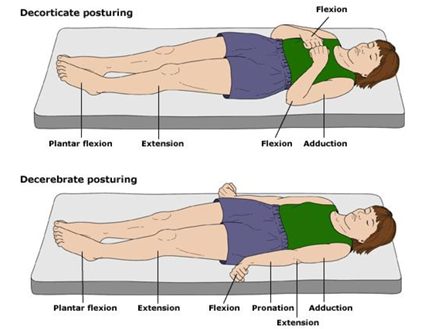
Decorticate positioning vs Decerebrate positioning (TBI)
Decorticate → PF, leg extension, arms tucked into chest
Decerebrate → PF, leg extension, arm extension, wrist flexion
Key PT assessment priorities in TBI?
Arousal, safety, posture, movement, tone, sensation, vestibular function, functional tasks, cognition/perception
What is the key message from the evidence about TBI management?
More therapy, earlier therapy, task‑specific practice!
Improves cardiovascular fitness, general health
Reduce depression
Somatosensory Impairments: Apraxia vs Visual Perceptual Impairments vs Neglect
Apraxia → prevents a person from performing purposeful movements or gestures despite having the physical ability and desire to do so
Visual Perceptual Impairments → inability to interpret and understand visual information
Neglect (unilateral) → Failure to attend to stimuli on the side opposite the lesion.
Somatosensory Impairments: Proprioception vs Tactile Functions
Proprioception → body’s ability to sense its position, movement, and force without relying solely on vision, sense of force, and timing of contraction
Tactile Function → sensory functions that involve localization and discrimination of stimuli.
Dysphasia vs Dysarthria vs Dysphonia vs Dyspraxia
Dysphasia → disturbances of language (Wernicke’s & Broca’s)
Dysarthria → disturbance of articulation
Dysphonia → disturbance in vocalization
Dyspraxia → impaired planning & sequencing of muscles required for speech
What is a spinal cord injury (SCI)?
Acute traumatic or non-traumatic damage to the spinal cord causing motor, sensory, and/or autonomic dysfunction
Difference between tetraplegia and paraplegia?
Tetraplegia/quadriplegia: C1–T1 → affects arms, trunk, legs
Paraplegia: Below T1 → affects trunk, legs
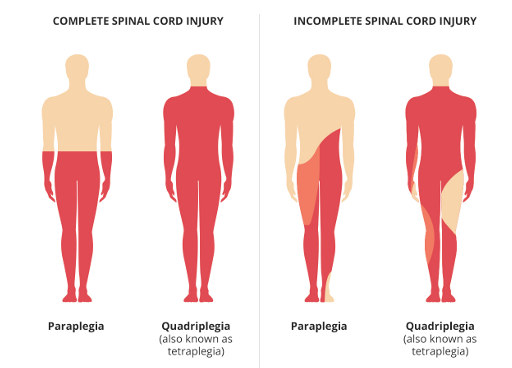
Complete vs incomplete SCI?
Complete: No motor/sensory function below S4–S5, no neurological recovery
Incomplete: Some function preserved below injury, preservation of motor and/or sensory function in S4-S5
2 Traumatic vs 2 non-traumatic SCI causes? F Rt T D
Traumatic: Falls + road trauma
Non-traumatic: Tumours + degeneration,
Most common injury levels in SCI patients?
Traumatic SCI: Cervical
Non-Traumatic SCI: Thoracic
Primary vs Secondary injury in SCI
Primary → Immediate damage (compression, laceration, concussion)
Secondary → Inflammatory cascade → ischemia, apoptosis, myelin damage
What is spinal shock in SCI?
Flaccid paralysis lasting ~2–6 weeks
What is Anterior Cord syndrome in incomplete SCI?
Damage towards the front of spinal cord (affects corticospinal tract)
Trauma MOI: Flexion, dislocation or disc protrusion
Loss of motor + pain/temp, preserved proprioception
What is Central Cord syndrome in incomplete cervical SCI?
Damage is in the centre of the cervical spinal cord
Arms worse than legs weakness, some recovery possible
Trauma MOI: Hyperextension
What is Brown-Sequard syndrome in incomplete SCI?
Damage is towards one side of the spinal cord
Same side: motor + proprioception loss
Opposite side: pain/temp loss
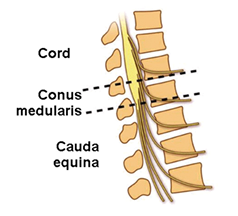
What is Conus Medullaris syndrome in incomplete SCI?
Trauma affects the spinal cord at L1-L2
Bowel/bladder dysfunction + saddle sensory loss
What is the most important impairment in SCI?
Muscle weakness (key determinant in motor function)
Why is respiration impaired in SCI? + complications
Paralysis of diaphragm/intercostals/abdominals
Pneumonia, atelectasis, respiratory failure
When does Autonomic Dysreflexia occur in SCI patients?
+ 4 key symptoms
+3 common causes
+3 managements
Lesions at or above T6
overreaction of the autonomic nervous system causing sudden severe high blood pressure.
Symptoms: Hypertension, headache, sweating, bradycardia
Causes: Bladder (UTI), bowel (constipation), skin (pressure sores)
Management: Sit upright, monitor BP, remove cause CALL FOR HELP!
What is spasticity?
Velocity-dependent increase in muscle tone (UMN lesion)
3 examples of musculoskeletal impairments in SCI patients? O C Ho
Osteoporosis (due to reduced WB)
Contractures (due to soft tissue muscle imbalance)
Heterotopic ossification (bone in soft tissue)
Functional Outcomes by Spinal Level: C1-C3, C4, C5, C6, C7-C8, T1-T12, L2-S5
C1–C3 outcomes → Ventilator dependent, fully dependent
C4 → ventilator dependent, small shoulder control
C5 function → Can eat/groom but not transfer, have biceps/deltoids
C6 function → Wrist extension (tenodesis grasp)
C7–C8 function → Independent transfers + ADLs
T1–T12 function → Independent, possible limited walking with aids
L2-S5 function → Full independence in any environment; rapid come back.

Main goals in acute SCI? Ss Pc Mmf Em
Stabilize spine
Prevent complications
Maintain muscle function
Early mobilization
When is surgery indicated in an SCI patient?
Spinal instability or displacement
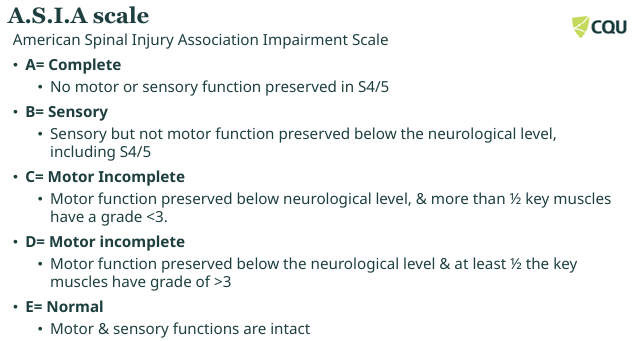
What does ASIA assess? (International Standards for Neurological Classification for Spinal Cord Injury (ISNCSCI)) + AIS A/B-D/E
Motor + sensory function to classify SCI severity
AIS A → Complete injury
AIS B → Sensory preserved, motor loss
AIS C → More than half key muscles have less than G3
AIS D → More than half key muscles have more than G3
AIS E → Normal function
International Standards for Neurological Classification for Spinal Cord Injury (ISNCSCI): same as ASIA
Supine
Myo/derma
ASIA
Anal
Comp/inco
Assessment in supine for acutely unstable injured person
Evaluation of 10 key myotomes and 28 dermatomes (light touch and pinprick)
Denotes level of SCI and the degree of impairment: level (C2-S4/5) represents the highest (most cephalad) myotome and dermatome in which normal function is preserved. Neurological Level Injury (NLI)
AIS: ASIA Impairment Scale (A, B, C, D, E): describes how much function is maintained below the level of injury: A no function to S4 and S5; E: normal function
S4-5: motor function ax by voluntary anal contraction (VAC); sensory ability to feel deep anal pressure (DAP)
AIS: determine complete or incomplete SCI.
ISNCSCI or ASIA steps in classification
Sen
Mot
Neuro Lev
Com/Inco
Grade
Determine sensory levels for R and L sides
Determine motor levels for R and L sides
Determine neurological level of injury (NLI): most cephalad of sensory and motor levels (step 1 and 2). Normal fx rostrally (3+)
Determine complete or incomplete: Voluntary anal contraction (VAC) and deep anal pressure (DAP)
Determine ASIA Impairment scale (AIS) grade: (A-B-C-D-E)
When does most recovery occur in SCI patients?
First 8 months
Key components of physio assessment in SCI patients? S S S F R/CV
Strength
Sensation
Spasticity
Function (SCIM, FIM)
Respiratory + CV fitness
Pressure Injury Prevention with braces: How often reposition in bed?
Every 2 hours
Sitting → every 30 minutes
Sitting and Standing Objectives in the Acute phase of SCI
Sitting → appropriate cushion, consider compression socks, monitor vitals
Standing → orthostatic hypertension, balance training, stretching
What are the 5 Principles of Management in SCI patients?
Assessing impairments, activity limitations and participation restrictions (e.g. strength, pain, mobility, QOL)
Setting goals with respect to activity limitations and participation restrictions (e.g. activity limitations, participation, impairments)
Identifying key impairments that are limiting achievement of goals (keep in mind some impairments are non-responsive to interventions)
Identifying and administering physiotherapy treatments (e.g. bed mobility, gait, contractures, UL function)
Measuring the outcome of treatments.
Recommended exercise for SCI?
60–80% HR
2–3x/week
20–60 min
SCI patients provided with a hard or electronic copy of their individualised exercise programs
Nociceptive vs neurogenic pain?
Nociceptive pain arises from actual or potential tissue damage, while neurogenic pain results from damage or dysfunction of the nervous system itself (stabbing/burning)
When to assess respiratory function in an SCI patient?
Assessed by a physiotherapist within 24 hours of admission to hospital
What is Multiple Sclerosis?
A chronic autoimmune demyelinating disease of the central nervous system (brain and spinal cord).
Autoimmune inflammatory demyelination → disrupted nerve conduction; axons initially preserved but may degenerate in chronic plaques.
More common in females 20-25 years
Autoimmune disease
6 examples of Common Multiple Sclerosis symptoms? W F S S P E
Fatigue (most disabling - heat dependent) (common)
Weakness
Spasticity
Sensory loss
Pain
Emotional disorders
What is the main Diagnostic Criteria for Multiple Sclerosis?
McDonald Criteria, which require evidence of:
1. Dissemination in space (DIS)
Lesions in different CNS regions
“Two separate attacks”
Demonstrated via MRI (90% positive)
2. Dissemination in time (DIT)
Evidence that lesions occurred at different points in time
“Two separate lesions”
What are the 4 subtypes of Multiple Sclerosis (MS)
CIS RRMS SPMS PPMS
Clinically Isolated Syndrome (CIS)
Relapsing Remitting MS (RRMS) → most common
Secondary Progressive MS (SPMS) → develops 10-15 yrs after diagnosis
Primary-Progressive MS (PPMS) → steady progression
What are 3 Sensory and 3 motor impairments in Multiple Sclerosis
P L D
W S A
Sensory:
Proprioception loss
Lhermitte’s sign (cervical flex. causes shock sensation in upper limbs)
Dyasthesisa (burning sensation)
Motor:
Weakness
Spasticity
Ataxia
Others: Facial weakness, vertigo, oculomotor abnormalities
What is the most disabling MS symptom?
Fatigue
Worsens with heat
Occurs in 75-95% of patients
3 Restorative & 3 Compensatory Approaches to Physio Assessment and Management of MS
A T A
Q P F
Restorative:
Optimize performance of ADLs
Target weakness, spasticity, pain
Avoid heat
Compensatory/Participation:
Improve QOL
Ensure interventions are patient-specific
Manage fatigue
Aerobic exercise 10–30 min, 2–3×/week
Resistance training 2–3×/week
Balance training
Cooling + intermittent exercise for heat intolerance
BWSTT improves gait parameters