DEN 150 final 1
1/104
Earn XP
Description and Tags
Includes 54, 55 MISSING: 60, 58, 56, 59, 57
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
105 Terms
What can the dental assistant assist with during periodontal procedures?
periodontal charting
periodontal surgeries
provide home care instructions to the patient
The Periodontal Practice
Patients are referred by the general dentist or dental hygienist for treatment of a periodontal condition
*After the periodontal treatment, the patient will return to the general dentist for routine dental care
*Frequently, periodontal patients will alternate periodontal maintenance (cleaning) appointments between the periodontist’s office and the general dentist’s office
The Periodontal Examination
A periodontal examination includes:
Medical and dental history
Radiographic evaluations
Examination of the teeth
Examination of the oral tissues
Supporting structures
Periodontal charting
Periodontal charting includes pocket readings, furcation's,*tooth mobility, exudate (pus), and gingival recession
Medical and Dental History
Systemic diseases such as acquired immunodeficiency syndrome, human immunodeficiency virus infection, and diabetes can decrease resistance of the tissue to infection
Dental history used to gather information about conditions that could indicate periodontal disease
For example, patients with periodontal disease often complain
* of bleeding gums
* loose teeth
* bad taste in the mouth
Dental Examination
Mobility
It is normal for teeth to have a slight amount of mobility (tooth movement) because of the cushioning effect of the periodontal membranes
Excessive mobility important sign of periodontal disease
Oral Tissues and Supporting Structures
The periodontal examination includes:
Assessment of the amounts of plaque and calculus
Changes in gingival health and bleeding
Assessment of the level of bone
Detection of periodontal pockets
Supporting Structures
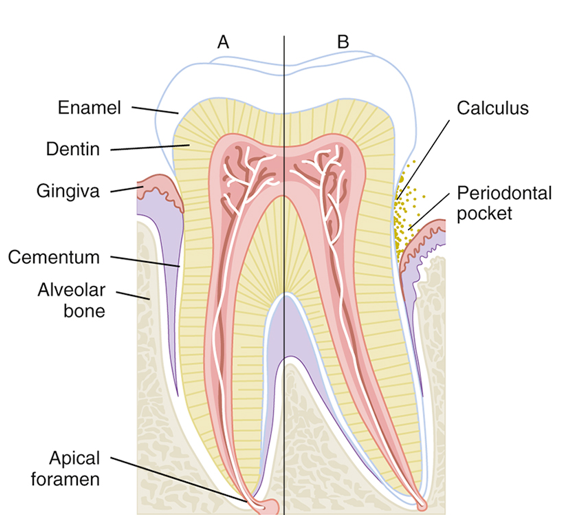
Periodontal Probing
A periodontal pocket results when the gingival sulcus becomes deeper than normal (<3 mm)
Periodontal probing measures how much epithelial attachment has been lost to disease
The greater the depth of the periodontal pocket results in
* the greater the loss of epithelial attachment
*the greater loss of bone
*more serious the periodontal disease
Periodontal pockets are very difficult, and sometimes impossible, for the patient to clean
Early Signs of Periodontal Disease
Changes in the gingiva (color, size, shape, texture)
Gingival inflammation
Gingival bleeding
Evidence of exudates
Development of periodontal pockets
Bleeding Index
The severity of gingival inflammation can be measured by the bleeding index
Several different systems of recording bleeding scores are used
Occlusal Adjustment
Patient’s bite is evaluated for areas of unequal pressure
Occlusal trauma can result if excessive biting pressure is noted in a specific area
Occlusal adjustment: Procedure that adjusts patient’s bite so that occlusal forces are equally distributed over all the teeth
Radiographic Analysis
Radiographs are a valuable aid for evaluating periodontal disease
Bitewing radiograph: Can accurately depict bone height along the root surface
Vertical bitewing radiographs are excellent for determining the extent of crestal bone loss
Periodontal Instruments
Periodontal therapy requires the use of specialized instruments
*to remove calculus,
*smooth root surfaces
* measure periodontal pockets,
*perform periodontal surgery
In general, the dentist or registered dental hygienist who uses these instruments takes responsibility for maintaining their sharpness
Periodontal Probes
Used to locate and measure the depth of periodontal pockets
On some types of probes, the tip is color-coded to make the measurements easier to read
Periodontal probe
* tapered to fit into the gingival sulcus
* shape is blunt or rounded tip
Six measurements are taken and recorded for each tooth
Scalers and Files
Sickle scalers are used primarily to remove large deposits of supragingival calculus
Chisel scalers are used to remove supragingival calculus in the contact area of anterior teeth
The blade on the chisel scaler is curved slightly to adapt to the tooth surfaces
Hoe Scalers are used to remove heavy supragingival calculus
Hoe Scalers are most effective when used on buccal and lingual surfaces of the posterior teeth
Curettes
Curettes are used to remove
*subgingival calculus,
*smooth rough root surfaces (root planning),
*remove the diseased soft tissue lining of the periodontal pocket (soft tissue curettage)
A curette has a rounded end, unlike a scaler, which has a pointed end
Two basic designs of curettes
Universal
Gracey
Types of Curettes
Universal curettes are designed so that one instrument can be used on all tooth surfaces
Gracey curettes have only one cutting edge and are area-specific
They are designed for use on specific tooth surfaces (mesial or distal)
Treatment of the entire dentition requires the use of several curettes
Pocket Markers
These perforations, which are referred to as bleeding points, are used to outline the area for an incision on the gingivae
Ultrasonic Scaler
Allows for rapid calculus removal and reduces hand fatigue for the operator
Works by converting very-high-frequency sound waves into mechanical energy in the form of very rapid vibrations
A spray of water at the tip prevents the buildup of heat and provides a continuous flushing of debris and bacteria from the base of the pocket
Because of the spray of water at the tip, there is a large amount of potentially contaminated aerosol spray
Highly desirable for the operator of an ultrasonic scaler to have the dental assistant help with using the high-volume evacuator to minimize aerosol contamination.
Indications for Use of the Ultrasonic Scaler
Removal of supragingival calculus and difficult stains
Removal of subgingival calculus, attached plaque, and endotoxins from the root surface
Cleaning of furcation areas
Removal of deposits before periodontal surgery
Removal of orthodontic cements; debonding
Removal of overhanging margins of restorations
Contraindications to Use of the Ultrasonic Scaler
Communicable disease: transmitted by aerosols, such as tuberculosis, poses a risk to the operator
Immunocompromised: A compromised patient is open to infection
Respiratory problems: Materials can be aspirated into the lungs of a patient with respiratory problems
Swallowing difficulty: Problems with swallowing or a severe gag reflex
Cardiac pacemaker: Consultation with the patient’s cardiologist is necessary
Precautions for Children
Young tissues are very sensitive to ultrasonic vibrations
These vibrations and heat may damage the pulp tissue of primary and newly erupted permanent teeth
Nonsurgical Periodontal Treatment
Dental prophylaxis
Prophylaxis is the complete removal of
*calculus
* soft deposits
* plaque
*stains from all supragingival
* unattached subgingival tooth surfaces
Dentist and dental hygienist are licensed to perform this procedure
Scaling, Root Planing, and Gingival Curettage
Scaling and root planing are done as part of a periodontal debridement
In some cases, gingival curettage, a nonsurgical technique, may also be indicated
A local anesthetic is usually administered before these procedures
Scaling
Scalers
*supragingival calculus from the tooth surface
Curettes
*remove supragingival and subgingival calculus
Root Planing
Root planing is performed after scaling procedures to remove any remaining particles of calculus and necrotic cementum embedded in the root surface
After root planing, the surfaces of the root are smooth and glasslike
Anesthetic is usually required for this procedure
Gingival Curettage
Curettage means scraping or cleaning with a curette
Some patients also require gingival curettage in addition to scaling and root planing
Gingival curettage, also known as subgingival curettage, is the scraping of the gingival lining of a periodontal pocket
This is performed to remove necrotic (dead) tissue from the pocket wall
Antimicrobial and Antibiotic Agents
Tetracycline is an antibiotic that is particularly useful for the treatment of periodontitis
Penicillin
Fluoride mouth rinses
A twice-daily chlorhexidine rinse (Peridex) is the most effective means available for reducing plaque and gingivitis
Locally Delivered Antibiotics
New methods can be used to apply antibiotics directly into the periodontal pockets
In one technique, a fiber that contains tetracycline is packed into periodontal pockets
Other methods include using a syringe to insert dissolvable materials such as a gel into the pocket
A dissolvable chip that releases chlorhexidine is inserted into deep pockets
Surgical Periodontal Treatment
When nonsurgical treatment is ineffective in stopping the disease process, periodontal surgery is indicated to control the progress of periodontal destruction and loss of attachment.
Advantages of Periodontal Surgery
*Allows access to the root surface for scaling and root planing
*Makes it easier for the patient to clean difficult areas
*Results in better access to furcations and other areas that are very difficult to reach during traditional scaling and root planing
Disadvantages of Periodontal Surgery
The health status of the patient, age of the patient as well as limitations of the procedures
From the patient’s point of view: Time, cost, esthetics, and discomfort
Excisional Periodontal Surgery
This surgery is used to remove the excess tissue
It is the most rapid means of reducing periodontal pockets
Common Types of Excisional Surgeries:
*Gingivectomy
*Gingivoplasty
Gingivectomy
Gingivectomy is the surgical removal of diseased gingival tissues
Performed when it is necessary to reduce the depth of the periodontal pocket and when fibrous gingival tissue must be removed
Recently, the use of dental laser equipment in gingivectomy has become popular
Gingivoplasty
*surgical reshaping
*contouring of the gingival tissues
Incisional Surgery
Incisional surgery known as periodontal flap surgery or simply flap surgery
Performed when an excisional surgery is not recommended
Osseous (Bone) Surgery
Periodontal surgery that involves modification of the supporting bone
This surgery is performed to eliminate pockets, remove defects, and to restore normal contours in the bone
Two types of bone surgeries are:
Osteoplasty
Ostectomy
Osteoplasty
In osteoplasty, or additive surgery,
*bone is contoured and reshaped
In addition, bone may be added, either through bone grafting (taking bone from one area and placing it in another) or placement of bone substance.
Ostectomy
In ostectomy, or subtractive surgery, bone is removed
This procedure is necessary when the patient has large exostoses (bony growths)
For example, ostectomy is performed if a patient needs a denture and the bony growth would interfere with the comfort and fit of the denture
Crown Lengthening
A surgical procedure that is designed
* to expose more tooth structure for the placement of a restoration such as a crown
Crown lengthening is becoming a very common procedure for esthetic anterior restorations
Soft Tissue Grafts
Pedicle graft
The pedicle graft is “freed” on three sides but remains attached on one side and retains its blood supply
Free gingival soft tissue graft
Has a donor site that is located away from the grafted site
Postsurgical Patient Instructions
After surgery, the periodontist will most likely prescribe an analgesic and possibly an antibiotic
Many periodontists recommend the use of an antibacterial rinse twice a day to help with plaque control
A chlorhexidine mouthwash may also be used during the first week to freshen the mouth and inhibit plaque formation during the early stages of healing
Postoperative instructions should be given to the patient to ease discomfort and promote healing
Periodontal Surgical Dressings
Periodontal dressings, also known as periopacks, are used to:
Hold the flaps in place
Protect the newly forming tissues
Minimize postoperative pain, infection, and hemorrhage
Protect the surgical site from trauma during eating and drinking
Support mobile teeth during the healing process
Types of Periodontal Surgical Dressings
The most commonly used materials are:
Zinc oxide–eugenol (ZOE) dressing
Noneugenol dressing
ZOE Dressing
Patient may experience redness and burning pain in the area of the dressing
ZOE dressings are supplied as a powder and a liquid that are mixed before use
Material may be mixed ahead of time, wrapped in waxed paper, and frozen for future use
ZOE has a slow set time, which allows for a longer working time
Sets to a firm, heavy consistency and provides good protection for tissues and flaps
Some patients are allergic to the eugenol
Noneugenol Dressing
Most widely used type of periodontal dressing
Supplied in two tubes: One of base material and the other of the accelerator
Easy to mix and place and has a smooth surface for patient comfort
Has a rapid setting time if exposed to warm temperatures
Cannot be mixed in advance and stored
Lasers in Periodontics
The term laser is an acronym for light amplification by simulated emission of radiation
A laser beam is a highly concentrated beam of light
Power of this beam can be adjusted to enable it to cut, vaporize, or cauterize tissue
The use of lasers is a promising new technology in dentistry
Use of Lasers on Soft Tissue
*Removal of tumors and lesions
*Vaporization of excess tissues, as in gingivoplasty, gingivectomy, and frenectomy
*Removal of or reduction in hyperplastic tissues
*Control of the bleeding of vascular lesions
*Aid in the removal of cold sores on the lip
Advantages of Laser Surgery over Conventional Surgery
Laser incisions heal faster than incisions made with electrosurgery
*Hemostasis (control of bleeding) is rapid
*The surgical field is relatively dry
*The opportunity for bloodborne contamination is reduced
*There are fewer traumas to adjacent tissues
*There is less postsurgical swelling, scarring, and pain
*Some procedures can be performed more quickly
*Patients who are afraid of “surgery” may accept this method
Laser Safety
Precautions must be taken to protect both the patient and dental staff during laser procedures
Any person who operates a laser or assists during a laser operation must be thoroughly trained in the use of this powerful instrument
Guidelines for Laser Safety
*Shielded eyeglasses: Protect the eyes; dental staff and patient must wear special shielded eyeglasses
*Matte-finished instruments: Reflective surfaces such as instruments, mirrors, and even polished restorations can reflect laser energy
*Protection of nontarget tissues: Nontarget oral tissue (tissues not being treated with the laser) should be shielded with the use of wet gauze packs
*High-volume evacuation: High-volume evacuation should be used to draw off the plume (cloud) created when tissue vaporizes
This plume should be considered infectious
Endodontics
The specialty of dentistry that manages the prevention, diagnosis, and treatment of the dental pulp and the perio radicular tissues surrounding the root of the tooth
Causes of Pulpal Nerve Damage
Physical irritation
Extensive decay moving into the pulp
Trauma
Blow to a tooth or jaw
Signs and Symptoms of Pulpal Nerve Damage
Pain when occluding
Pain during mastication
Sensitivity to hot or cold beverages
Facial swelling
Fever
Tenderness of surrounding gums
Cracked or discolored teeth
Endodontic Diagnosis: Subjective Examination – Patient Describes
Chief complaint
Painful stimuli
Character and duration of pain
Sensitivity to biting and pressure
Endodontic Diagnosis: Objective Examination – Dentist Findings
Extent of decay
Periodontal conditions
Extensive restoration
Tooth mobility
Swelling or discoloration
Pulp exposure
Percussion Test
Determines whether the inflammatory process has extended into the periapical tissues
The dentist taps on the incisal or occlusal surface with the end of the mouth-mirror handle held parallel to the long axis of the tooth
Palpation Test
Determines whether the inflammatory process has extended into the periapical tissues
The dentist applies firm pressure to the mucosa above the apex of the root
Thermal Sensitivity
Necrotic pulp will not respond to cold or heat
Cold test
Ice, dry ice, or carbon dioxide is used to determine the response of a tooth to cold
Heat test
A piece of gutta-percha or an instrument handle is heated and applied to the facial surface of the tooth
Electric Pulp Testing
A small electrical stimulus is delivered to the pulp-determine if tooth is vital or nonvital.
Factors that may influence readings include:
The patient has extensive restorations
The patient has teeth with more than one canal
Failing pulp produces a variety of responses
Control teeth don’t respond as anticipated
There is moisture on the tooth during testing
The batteries in the tester weaken over time
Five (5) Radiographic Imaging Taken for Endodontic Treatment
Initial radiograph: Diagnosis
Working length image: To determine the length of the canal
Final instrumentation image: Final size files in all canals
Root canal completion image: Taken after the tooth has been temporized
Recall image: Taken at posttreatment evaluations
Requirements of Radiographic Images
Must show apex of the tooth and the surrounding bone or pathologic condition
Must present an accurate image
Must exhibit good contrast so that all pertinent structures are readily identifiable
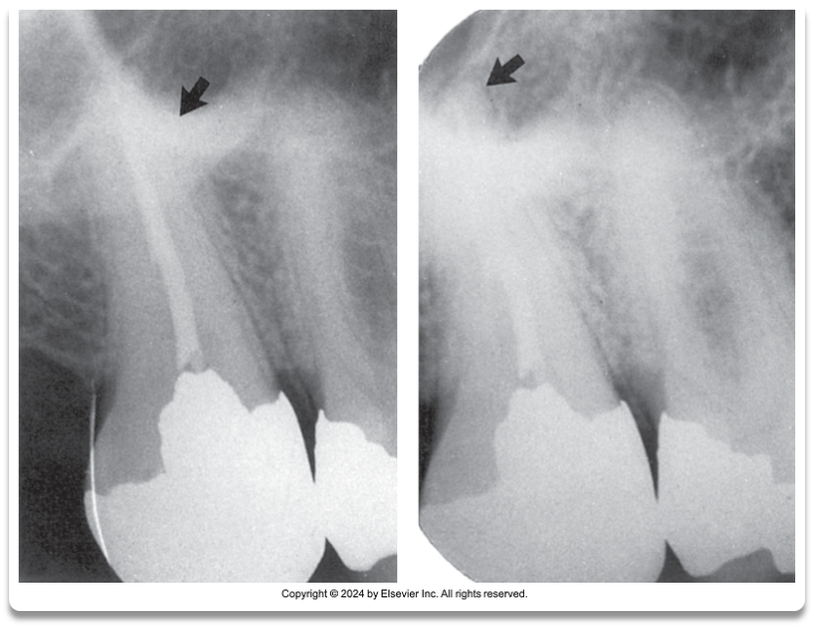
A. Good contrast around apex
B. Poor Contrast around apex
Diagnostic Conclusions
Normal pulp
No subjective symptoms or objective signs are noted
The tooth responds normally to sensory stimuli, and a healthy layer of dentin surrounds the pulp
Pulpitis
The pulp tissues have become inflamed
Reversible pulpitis
The pulp is irritated, and the patient is experiencing pain in response to thermal stimuli
Irreversible pulpitis
The tooth displays symptoms of lingering pain (pulp incapable of healing)
Diagnostic Conclusions: Periradicularor Periapical Abscess
This inflammatory reaction surrounding the tip of the root has pulpal infection which can be chronic or acute onset with pain, tenderness of the tooth due to pressure, pus(exudate), and swelling of the tissues.
Tooth has experienced bone loss and bacteria having access along the root.
Chronic-presence of a draining sinus tract
Acute-pain, tenderness, swelling because of the necrosis (dying)
Diagnostic Conclusions: Periodontal Abscess
Inflammatory reaction caused by bacteria trapped in the periodontal sulcus
A patient will experience rapid onset of pain, tenderness of the tooth in response to pressure, pus formation, and swelling
Chronic
Acute
Diagnostic Conclusions: Periradicular or Perioapical Cyst
This type of cyst develops at or near the root of a necrotic tooth
The cyst develops as an inflammatory response to pulpal infection and necrosis of the pulp
Diagnostic Conclusions: Pulp Fibrosis
A decrease in living cells within the pulp causes fibrous tissue to take over the pulpal canal
(Mostly seen in older patients.
Patients with recent trauma to a tooth may be susceptible)
Diagnostic Conclusions: Necrosis
The tooth may also be referred to as nonvital
The term is used to describe a tooth that does not respond to sensory stimulus
Endodontic Procedures: Pulp Capping
Pulp capping is an attempt to save the tooth.
Calcium hydroxide is placed over an exposed or nearly exposed pulp to encourage the formation of dentin at the site of injury
2 types of capping:
Indirect pulp capping (IPC) is indicated when a thin portion of dentin is still intact
Direct pulp capping (DPC) is indicated when the pulp has been slightly exposed
Endodontic Procedures: Pulpotomy
This procedure involves removal of the coronal portion of an exposed vital pulp
It is used to preserve the vitality of the remaining portion of the pulp within the root of the tooth
The procedure is commonly indicated for vital primary teeth, teeth with deep carious lesions, and emergency situations
Endodontic Procedures: Pulpectomy
This procedure involves the complete removal of the dental pulp
Also referred to as root canal therapy
Instruments and Accessories for Endodontic Procedures
Hand instruments
Explorer
Endodontic spoon excavator
Spreaders and pluggers
Glick Number 1-used to remove excess gutta
percha
ORDER OF INSTRUMENTS USED IN ENDO
TREATMENT
1. Endo Explorer
2. Files
3.Paper Points
4.Gutta Percha
5. Glick Number 1
Hand-operated files
K-type file- cleaning of canal initially
Hedstrom file- spiral edges, cutting occurs only in the pulling stroke
Reamer file- remove dentin, to smooth and increase size of canal
Broaches- remove necrotic pulp tissue from canal
Rotary-operated files and burs
Gates-Glidden burs-first instrument used to enlarge
the cervical portion of the root canal.
Pesso files-to prepare canal for endodontic post
Auxiliary instruments
Rubber stops
Paper points-used to dry canal
Microscopic Endodontics
Medicaments and Dental Materials in Endodontics
Irrigation solutions
Sodium hypochlorite (Bleach)
Ethylenediaminetetraacetic acid (EDTA)
Chlorhexidine (Peridex)
Intracanal medicaments
Calcium hydroxide
Chlorhexidine gel
Root canal sealers
Root canal filling materials
Gutta-percha points
Overview of Root Canal Therapy
Anesthesia and pain control
Isolation and disinfection of the operating field(rubber dam)
Access preparation
Estimated working length (files)
Electronic apex locator
Debridement and shaping of the canal
Obturation (filling and sealing a tooth with root canal material)
Surgical Endodontics
Indications for surgical intervention
Endodontic failure
Persistent infection, severely curved roots, perforation of the canal, fractured roots, extensive root resorption, pulp stones, or accessory canals that cannot be treated
Exploratory surgery
To determine why healing did not occur
Biopsy
Apicoectomy and Apical Curettage
To surgically remove the apical portion of the root with the use of a high-speed handpiece and bur
To evaluate the following:
Inadequate sealing of the canal
Accessory (extra)canals
Fractures of the root
Pathologic tissue around the root apex
Retrograde (root-end filling) Restoration
This procedure is undertaken when an apical seal is not adequate
A small class I preparation is made at the apex and sealed with filling materials such as gutta-percha, amalgam, or composite
Root Amputation and Hemisection
Root amputation
This surgery is performed to remove one or more roots of a multirooted tooth without removing the crown
Hemisection
The root and the crown are cut lengthwise and removed
abscess
a localized infected area with accumulating pus
acute
sudden or onset illness or pain with a short duration
apical curettage
a surgical procedure that involves the removal of tissue surrounding the apex of a tooth
apicoectomy
a surgical procedure to remove the apex of a tooth's root, usually to treat infection.
chronic
a long-lasting condition or illness that persists over time.
control tooth
A tooth that is used as a reference for comparison in dental studies or treatments.
debridement
The process of removing decayed or infected tissue from a tooth or surrounding area and cleaning out the pulpal canal
direct pulp cap
application of a dental material with an exposed or nearly exposed dental pulp
endodontist
A dental specialist who diagnoses and treats dental pulp and root canal issues, focusing on saving teeth with advanced procedures.
gutta-percha
A biocompatible material used to fill and seal the pulpal canal during root canal treatment.
indirect pulp cap
placement of a sedative material when pulp tissue is close to the surface but not completely exposed
irreversible pulpitis
A painful condition occurring when the dental pulp becomes inflamed and irreversibly damaged, often requiring root canal therapy.
nonvital
dead
obturation
The process of filling a root canal space after endodontic therapy to seal it and prevent reinfection.
palpatation
The act of applying pressure to a specific area of the body to assess for pain, swelling, or other abnormalities.
percussion
The act of tapping on a surface to elicit sounds or vibrations in order to assess underlying structures or conditions.
periodontal abscess
localized infection within the periodontal sulcus
periradicular
refers to the area of nerves, blood vessels, and connective tissue surrounding the apex of a tooth root.
periradicular abscess
inflammatory reaction to pulpal infection
pulpectomy
a dental procedure that involves the removal of the pulp tissue from the tooth to treat infection or decay.