Reabsorption + Secretion
1/28
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
29 Terms
Reabsorption is the process by which any essential molecules or ions are transported from the filtrate…
back into the blood!
Transport out of nephron lumen into peritubular capillaries or vasa recta can take 2 paths…
Transepithelial transport
Paracellular pathway
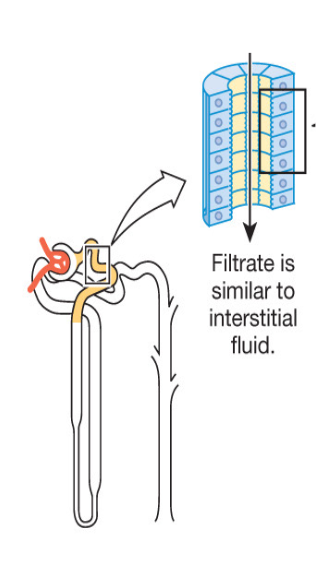
Transepithelial transport
substances cross both apical and basolateral membranes using membrane transporters (channels and/or carrier proteins) via passive or active transport
→ Apical = faces lumen of nephron and the filtrate
→ Basolateral = faces interstitial fluid and peritubular capillaries or vasa recta
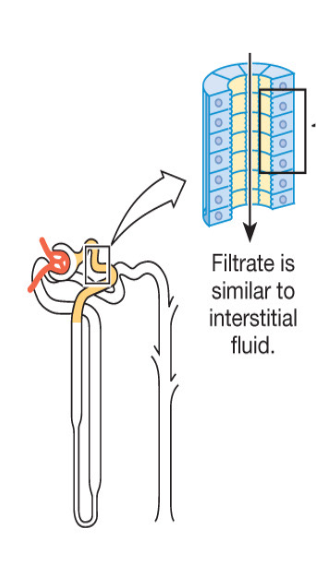
Paracellular pathway
if small enough, some substances can pass through the junction between two adjacent cells that line the wall of the nephron
this form of transport is ALWAYS passive, using simple diffusion or osmosis
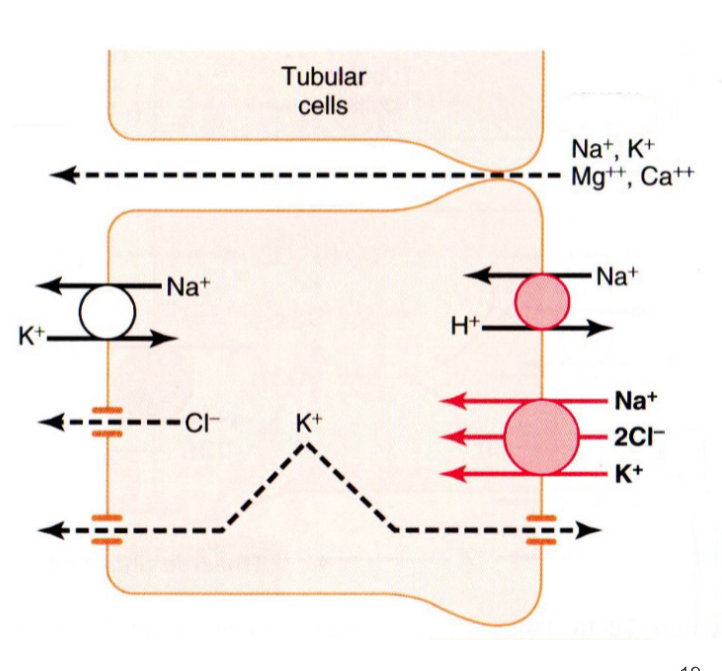
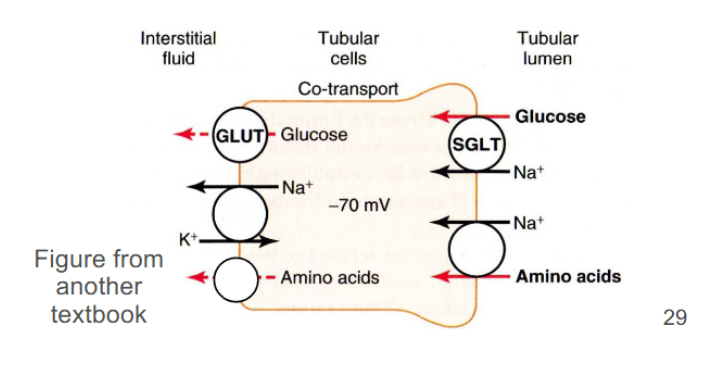
if this diagram is primarily showing reabsorption label the basolateral membrane and apical membrane of these tubular cells…
→ right side is apical; left side is basolateral
on this diagram, all ions being reabsorbed via paracellular transport
→ Na+, K+, Mg++, Ca++ (on top)
on this diagram, all ions being reabsorbed via transepithelial transport
→ Na+ and K+, Cl-. some K+
Reabsorbed substances at the proximal tubule
Essential ions
Sodium, chloride, bicarbonate, potassium
Essential Organic Molecules
Glucose and amino acids
→ via membrane transporters
→ limited in rate of transport (saturation can occur)
Small proteins
→ via transcytosis
Water follows these solutes by osmosis to maintain osmotic equilibrium
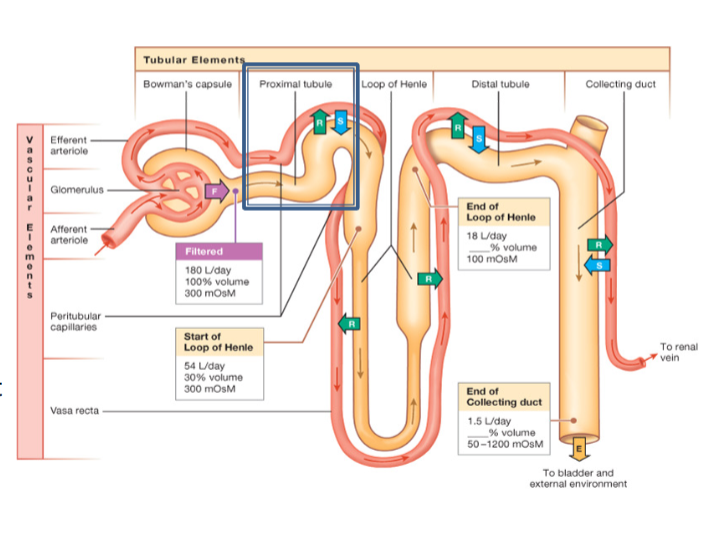
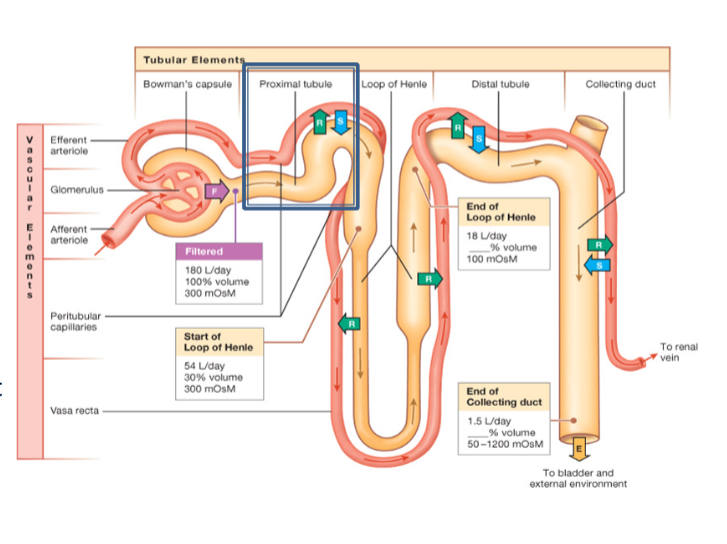
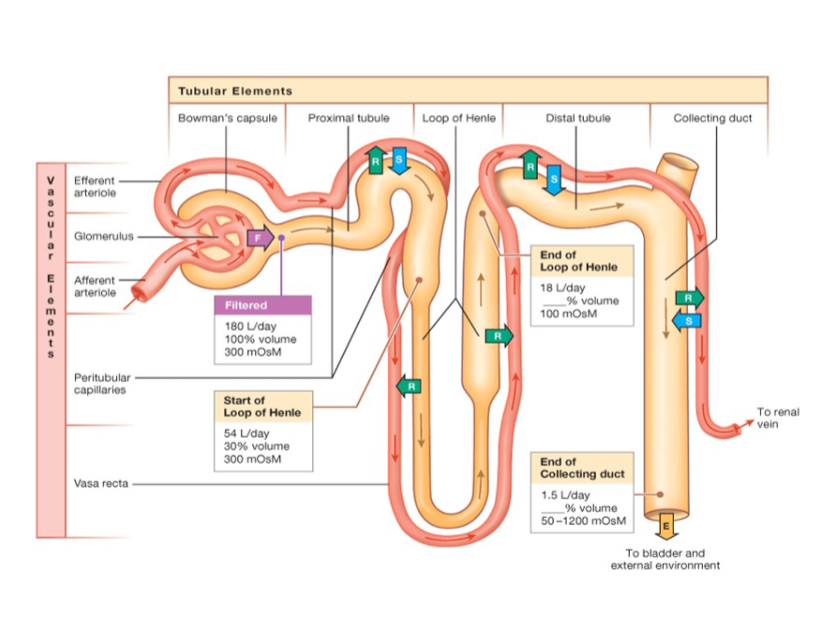
By the end of the proximal tubule, ____ of the original filtrate volume is reabsorbed in the proximal tubule
65-70%
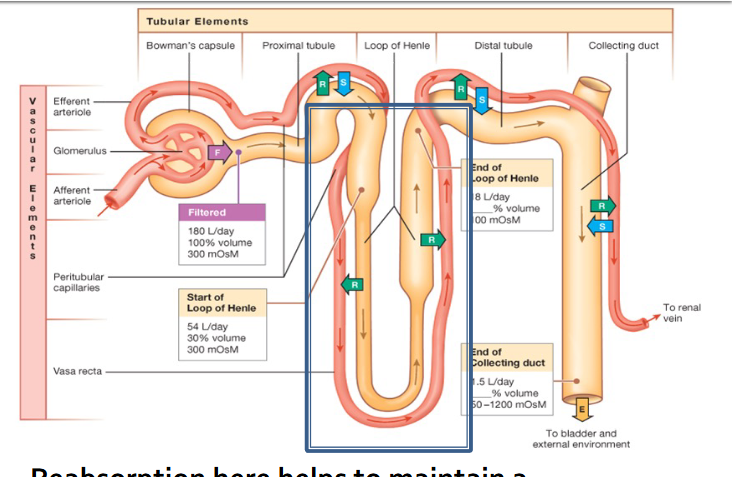
Descending limb of the loop of Henle
Water only
as water is removed, filtrate becomes concentrated with solutes
Water is transported via osmosis
Ascending limb of the loop of Henle
Solutes only (water-tight)
Sodium (Na+)
Potassium (K+)
Chloride (Cl-)
→ as solutes are removed, filtrate becomes less concentrated
By the end of the loop, up to _____ of the original filtrate volume has been reabsorbed
80-90%
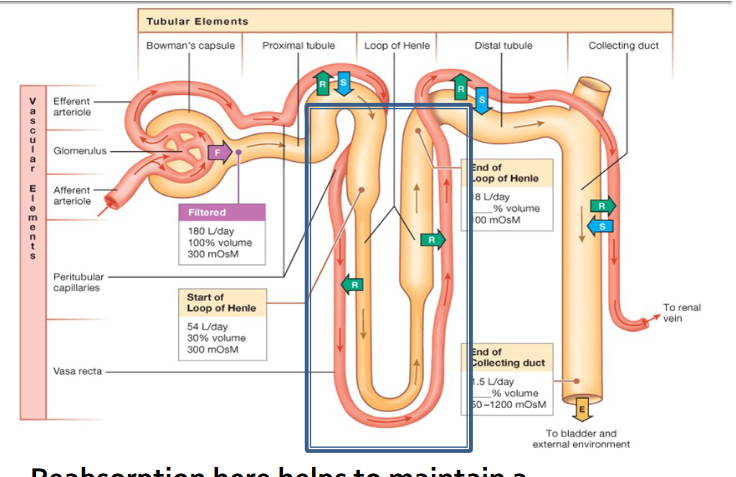
Reabsorption here helps to maintain a concentration gradient in the interstitial fluid of the renal medulla
the interstitial solute concentration gets higher and higher as the tubule and capillaries dip deeper into the renal medulla
This creates an osmotic pressure gradient which helps reabsorb as much water as possible from the collecting duct before filtrate leaves the nephron as urine
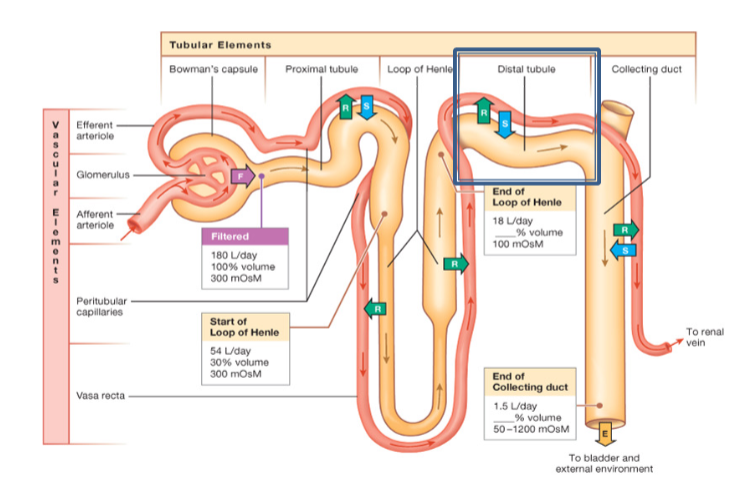
Reabsorbed substances at the distal tubule
only ions and water
→ amounts reabsorbed can be increased or decreased based on hydration and osmolarity status
→ regulated by hormones such as vasopressin and aldosterone
by the end of the distal tubule, 95+% of the original filtrate volume is reabsorbed
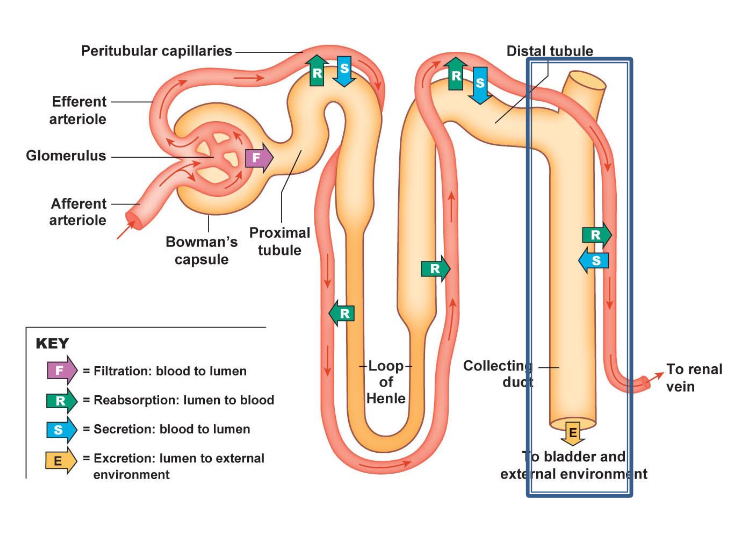
Reabsorption at the collecting duct
only ions and water again
fine tuning of filtrate occurs here based on your hydration and osmolarity status at any given time
→ reabsorption here is HEAVILY regulated by vasopressin and aldosterone
→ this fine tuning ensures that the nephron’s goal is met… to eliminate all wastes and excess nutrients with as little water as possible
by the end of this duct, ~99% of the original filtrate volume has been reabsorbed
filtration
reabsorption and secretion, small proteins, amino acids, glucose, water and ions
descending: reabsorbed water; ascending reabsorption of ions
reabsorption and secretion, water and ions, vasopressin + aldosterone
reabsorption and secretion, water and ions, vasopressin + aldosterone
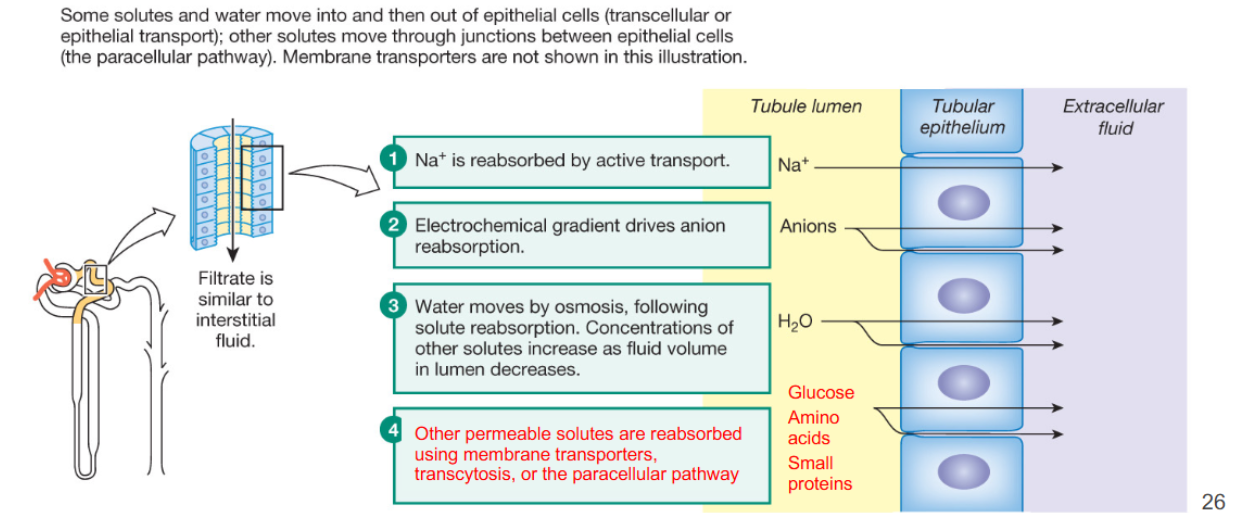
Ionic, molecular, and water reabsorption at the proximal convoluted tubule
Reabsorption of ions, water, and important biomolecules (like glucose and amino acids) occurs through a combination of paracellular and transepithelial transport
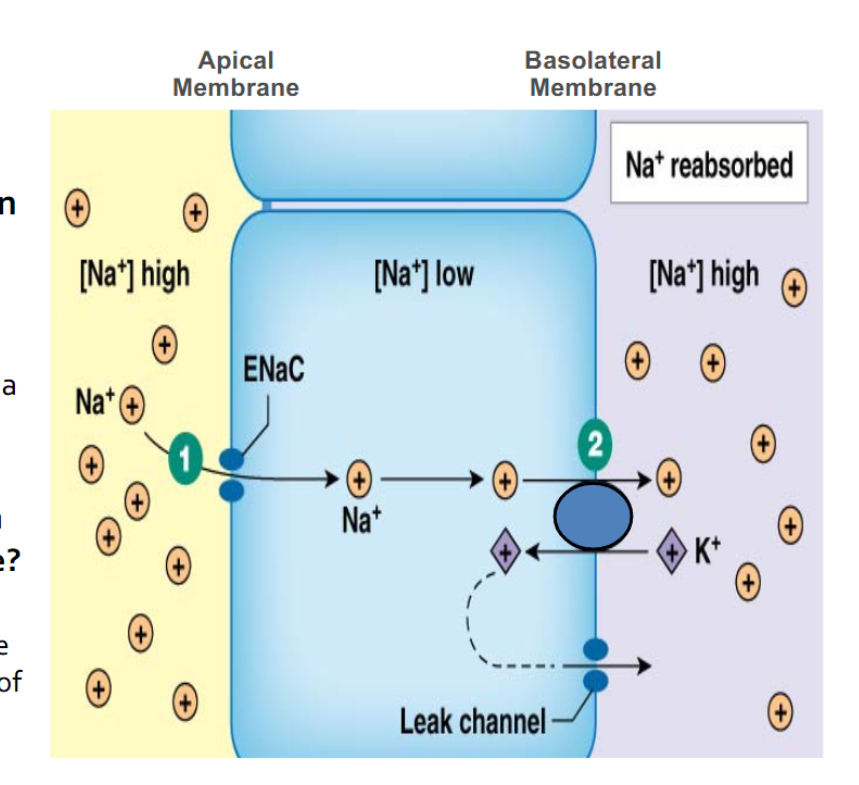
Where is Na+ reabsorbed?
at proximal convoluted tubule, ascending limb, distal convoluted tubule, collecting duct
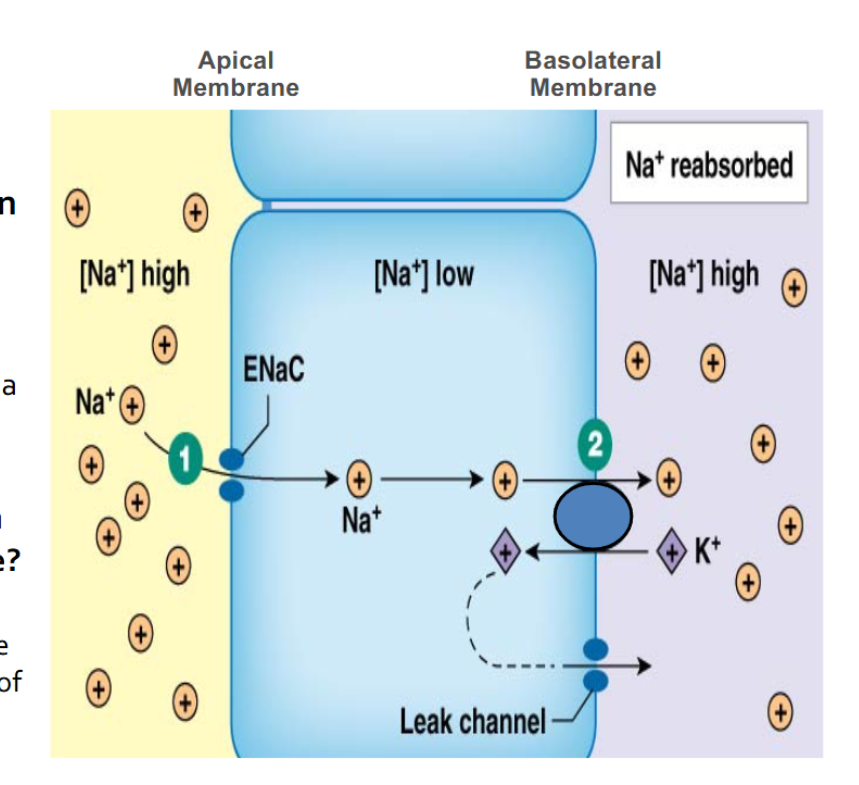
How is Na+ transported on the apical membrane?
thats the ENaC or epithelial Na+ channel
→ facilitated diffusion (high to low concentration)
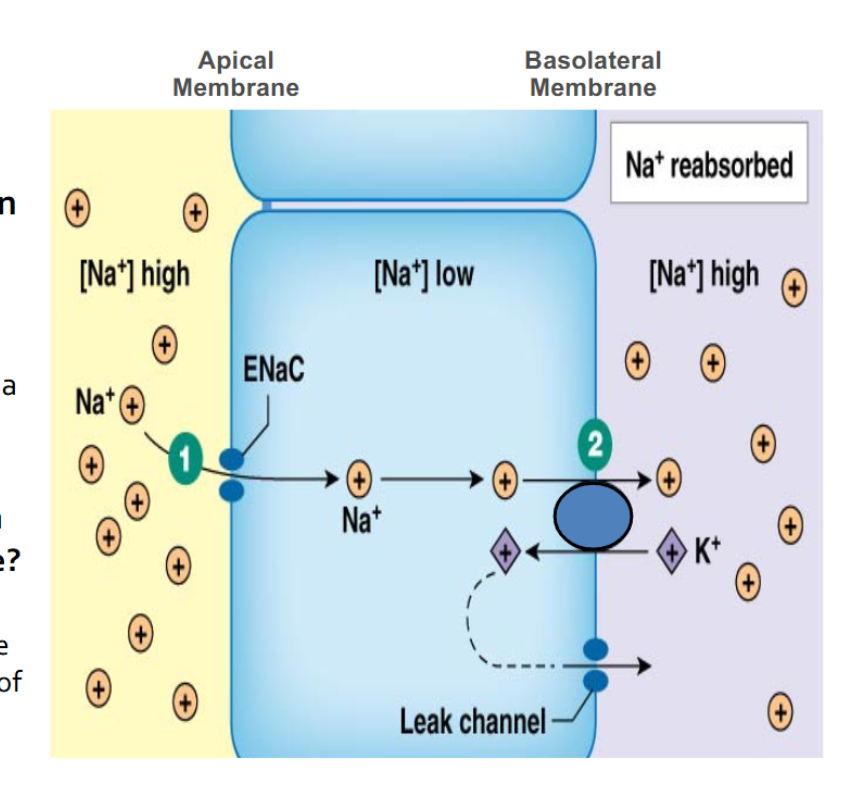
How is Na+ transported on the basolateral membrane?
antiport transport carrier protein
→ Na+ from low to high — going against concentration gradients
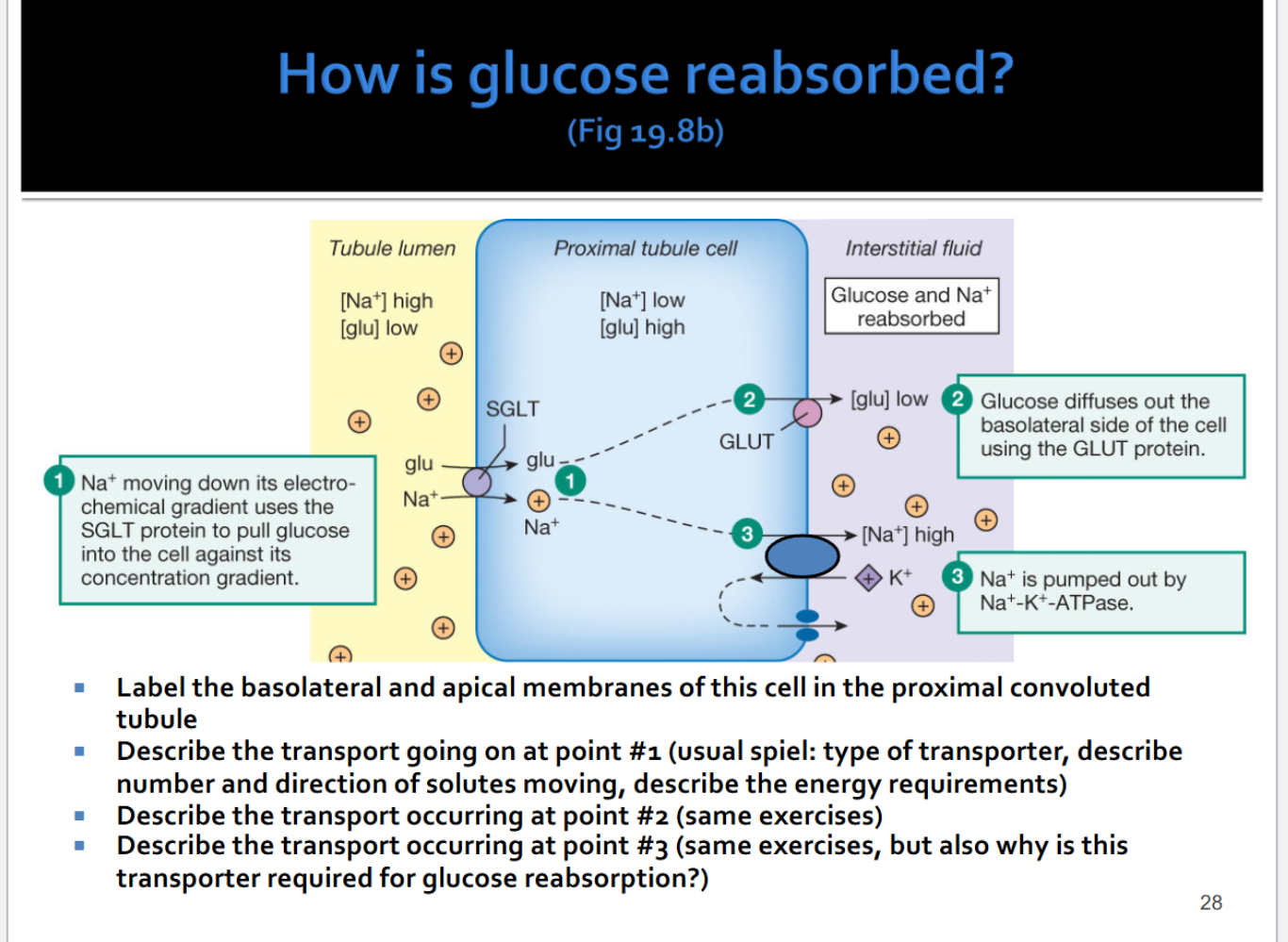
How is glucose reabsorbed?
Apical membrane: tubule lumen; Basolateral membrane: interstitial fluid
carrier protein; secondary active transport, symport
carrier protein; uniport, facilitated diffusion
carrier proteins, antiport, primary active transport
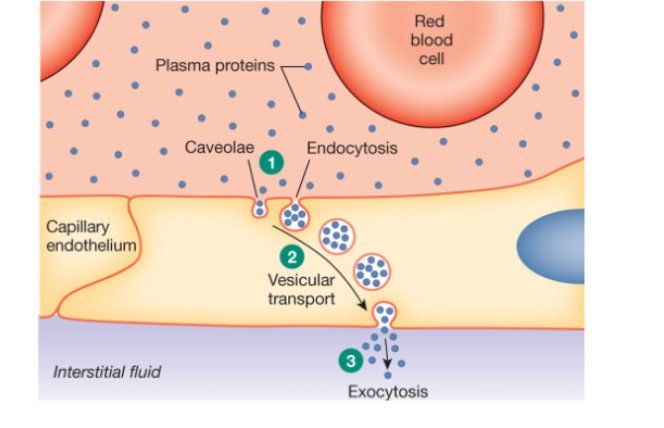
How are small proteins reabsorbed at the proximal tubule?
Transcytosis!
endocytosis on apical
exocytosis on basolateral
→ some examples of small proteins in blood would be hormones (insulin) and neurohormones (vasopressin) or blood enzymes (plasmin, renin)
How are amino acids reabsorbed at the proximal tubule?
co transport with sodium
same mechanism as glucose
Reabsorption at the descending limb
highly permeable to water
not to ions (there are no membrane transporters leave)
why would water leave?
what would this water reabsorption do to the osmolarity of the filtrate?
Reabsorption at the ascending limb
impermeable to water due to composition of plasma membranes
ions (Na+, K+, and Cl-) are reabsorbed here
how does this transport happen? see next slide
What would this reabsorption of solutes do to the osmolarity of the filtrate?
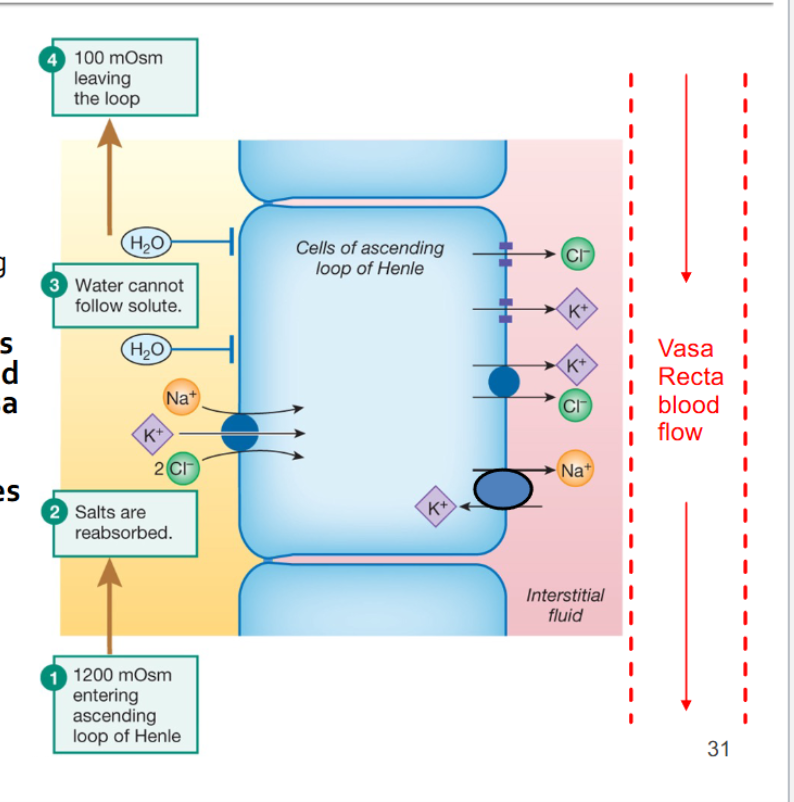
Reabsorption of solutes from the ascending limb (fig 20.7d)
What is being transported across the apical (luminal) membrane through the Na+, K+, and Cl- cotransporter (NKCC)
→ what is driving the movement?
→ what is maintaining that driving force?
How is each ion moving across the basolateral membrane and back into the blood of the vasa recta
This active transport of solutes from the filtrate into the interstitial spaces creates an osmotic gradient in the renal medulla
→ the filtrate and the interstitial fluid gets more and more concentrated the deeper it is in the medulla
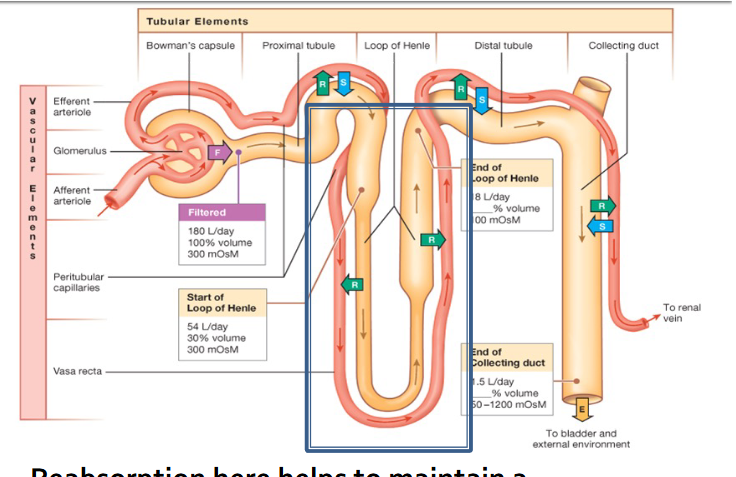
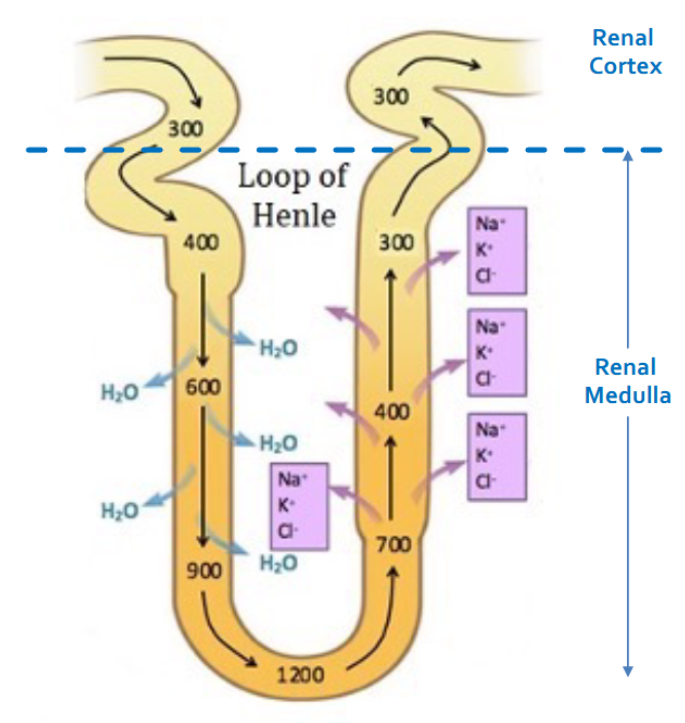
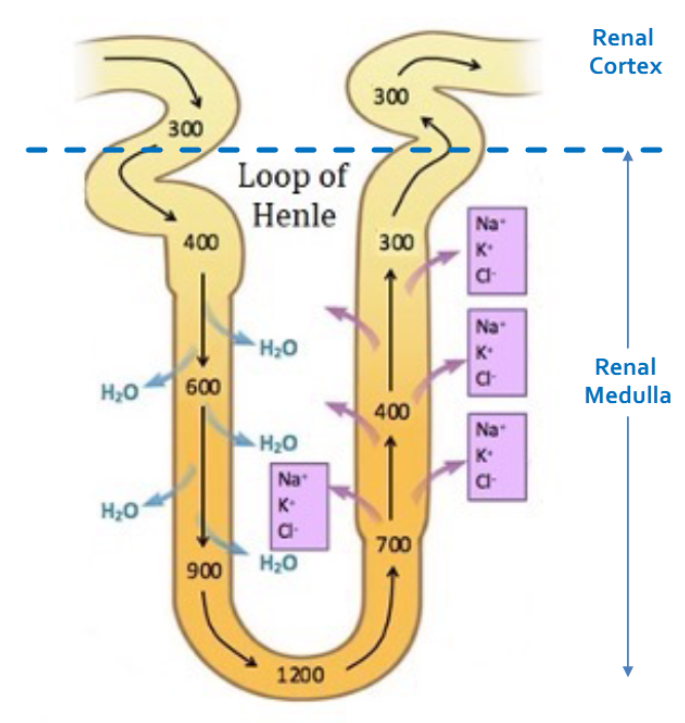
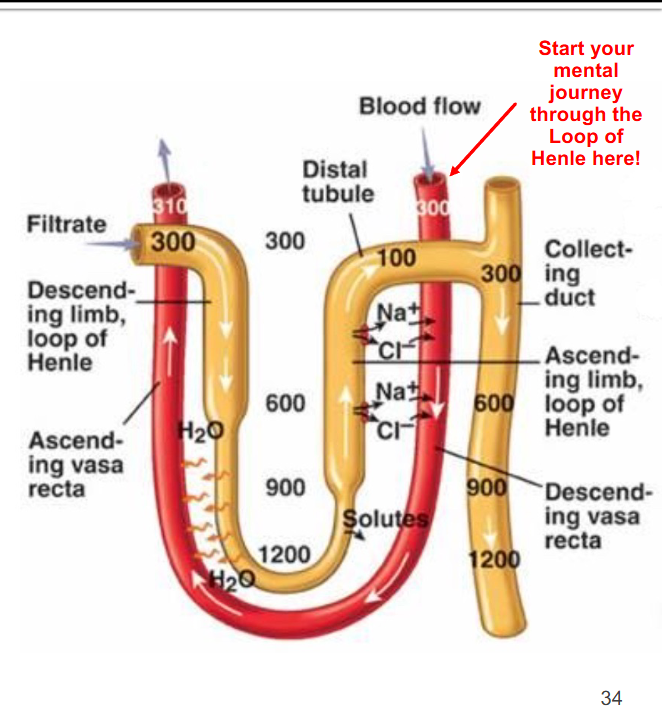
The Loop of Henle and vasa recta
There are two “countercurrent” mechanisms operating in the Loop of Henle
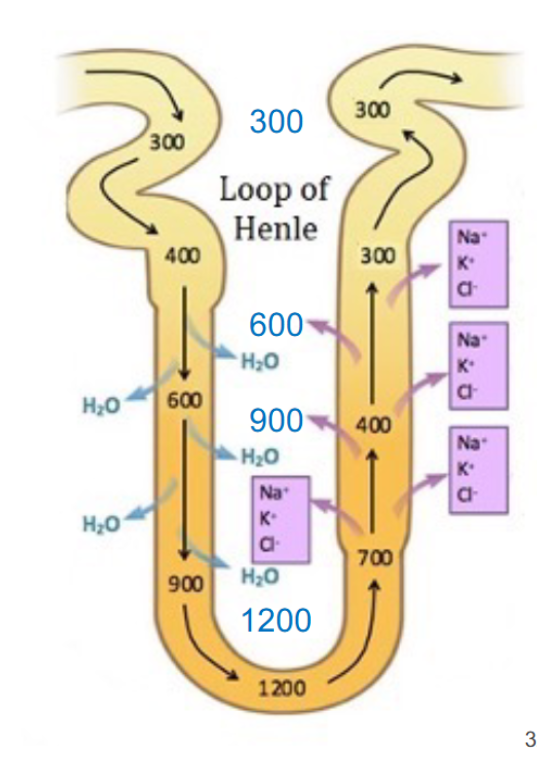
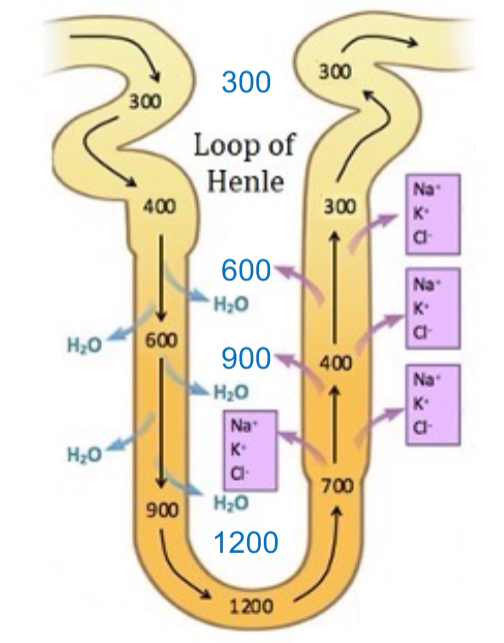
The first is called the “countercurrent multiplier system”
→ it is created by the filtrate in each limb moving in opposite directions AND the permeability differences for each limb
→ this causes the osmolarity of the filtrate (black numbers in diagram) and interstitial fluid (blue numbers) to INCREASE as they go deeper into the renal medulla
this countercurrent multiplier system creates an osmotic gradient in the renal medulla interstitial fluid
→ important for maximizing the water reabsorption that occurs later in the collecting duct to minimize water loss in urine
The countercurrent multiplier also creates a problem
it causes more and more solutes to be deposited in the renal medulla over time
That would then cause more and more water to be retained in the kidneys over time (due to osmosis)
Carry this logic over time….
→ the kidneys would eventually swell and rip themselves apart
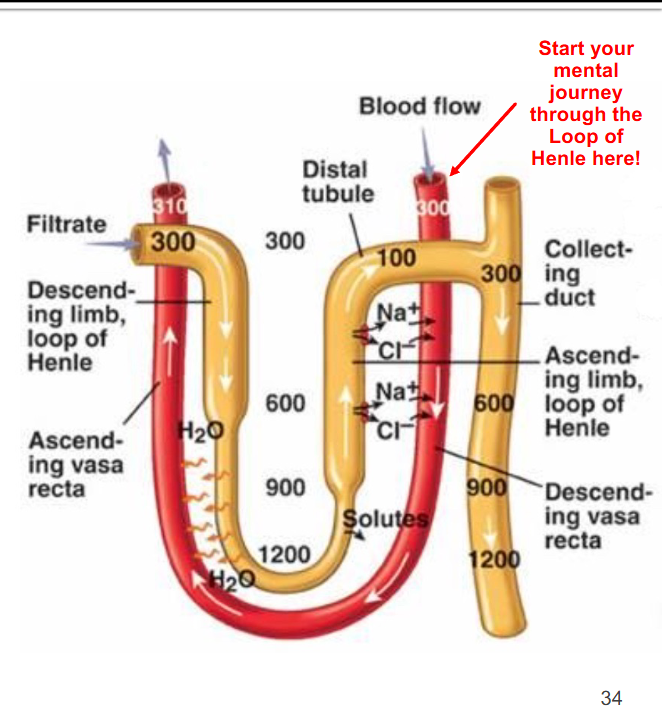
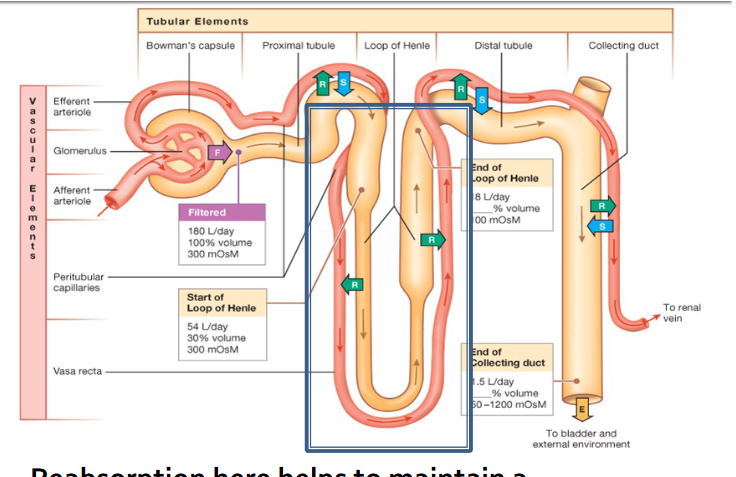
The countercurrent exchange system!
blood flow of the vasa recta
Blood in the vasa recta moves in the opposite directive relative to the filtrate in the loop of Henle
Ions diffuse into the blood as it dips deeper and deeper into the renal medulla, making the blood briefly hypertonic
Water then moves into the blood by osmosis as it flows back towards the cortex
→ this re-establishes the normal osmolarity of blood before it returns to the systemic circulation
This mechanism prevents water and ion accumulation in the renal medulla
Which ensures that the countercurrent multiplier stays constant long term which itself airs in the production of hypertonic urine by the collecting duct
Secretion occurs at 3 sites in the nephron
Proximal tubule
→ H+ (pH regulation)
Distal tubule and collecting duct
→ H+ (pH regulation)
→ K+
Secretion is handled by specialized epithelial cells (called intercalated cells) in the walls of those secretions of the tubule
→ Na+/H+ pumps or Na+/K+ pumps on apical and basolateral membranes actively transport the K+ and H+ into filtrate to maintain pH and K+ homeostasis