(L15) IMED2002 - Lymphoma
1/32
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
33 Terms
Lymphoma: Overview of Lecture
DIAGRAM ON SLIDE 2
Normal Lymphoid Tissue
- Primary and secondary lymphoid organs
- All potential sites of lymphoid malignancy
.
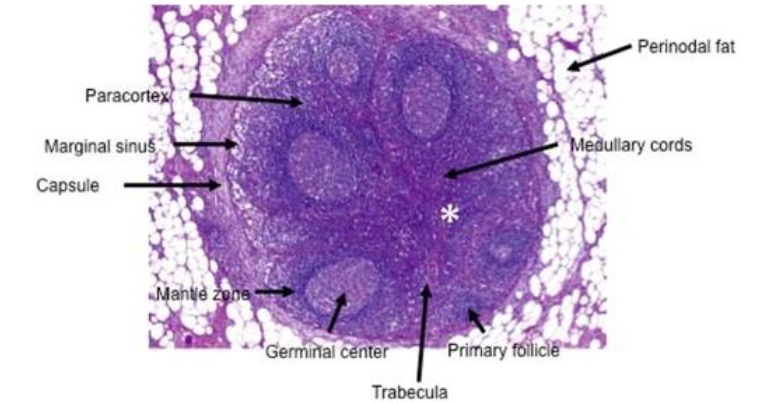
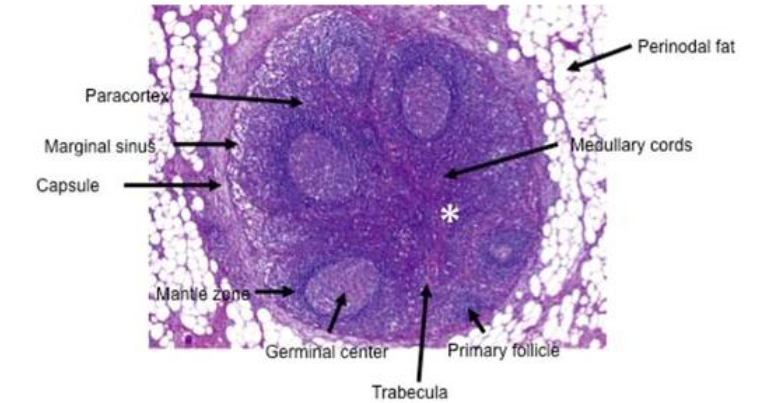
Lymph node structure:
- primary and secondary follicles
- Germinal centres
- Mantle zone
- Interfollicular zone
.
- Contain T and B cells
Normal Lymphoid Tissue INFO
Lymph node structure:
- primary and secondary follicles
- Germinal centres
- Mantle zone
- Interfollicular zone
- Contain T and B cells
.
- germinal centre is where lot of immunoglobulins are produced
.
germinal centres: specialized, transient structures formed within secondary lymphoid organs (lymph nodes, spleen, tonsils) during an immune response.
The mantle zone is the outer ring of small, mature B lymphocytes surrounding the germinal center within a secondary lymphoid follicle (e.g., in lymph nodes). It consists of B cells pushed out from the center during activation
Malignant Lymphomas
- Leukaemia = blood/BM ; Lymphoma = solid
- Replacement of normal lymphoid tissue by abnormal cells
- WHO classification of lymphoma
.
Two main types:
- Non-Hodgkin lymphoma (many sub-types)
- Hodgkin lymphoma
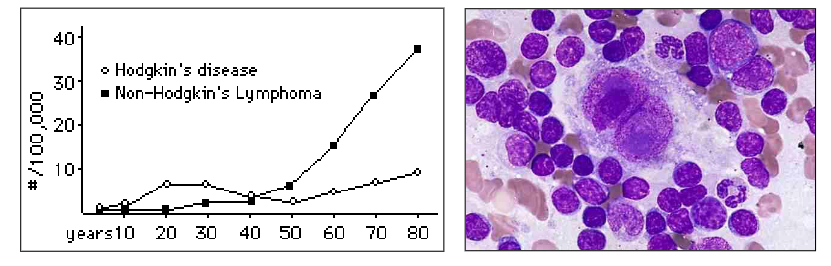
A. Non-Hodgkin Lymphoma (NHL) (Subtypes, Grade)
- NHL: 6th most common cause of cancer death
- Increasing incidence and mortality
.
Several subtypes:
- WHO Classification of NHL: B vs T cell origin
- Cells: correlate with morphology and immunology and stage of normal lymphoid cell maturation
.
Grade:
- Low: slow growing; indolent (lazy); generally incurable
- High: fast growing; aggressive; potentially curable
.
- Stage: extent (amount) of disease. Sites; marrow
- Type, grade and stage all have impact on prognosis
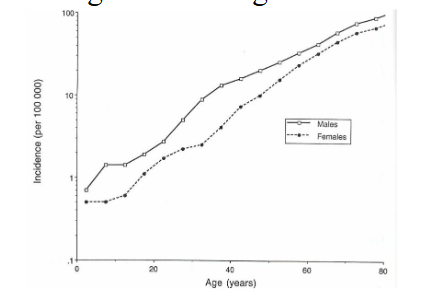
Aetiology and Epidemiology of NHL
Immune suppression:
- Organ transplant
- AIDS
.
Viral causes:
- EBV: Burkitt lymphoma
- HTLV-I: Adult T cell leukemia / lymphoma
.
Geography:
- Burkitt: tropical Africa
- Adult T cell leukemia / lymphoma: Japan & Caribbean
.
Chronic inflammation / antigenic stimulation:
- Helicobacter pylori: MALT lymphoma of stomach
.
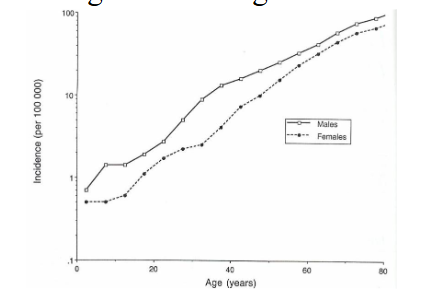
Age:
- Low grade: rare in young; increase in incidence with age
- Large cell: less age related
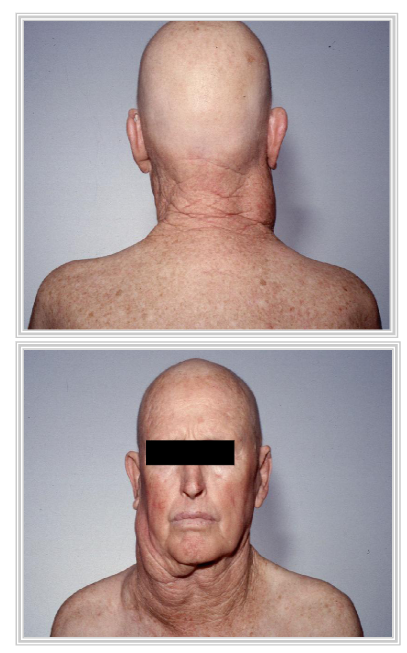
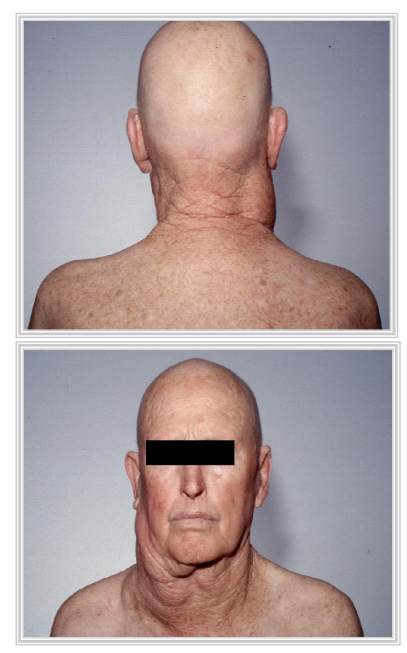
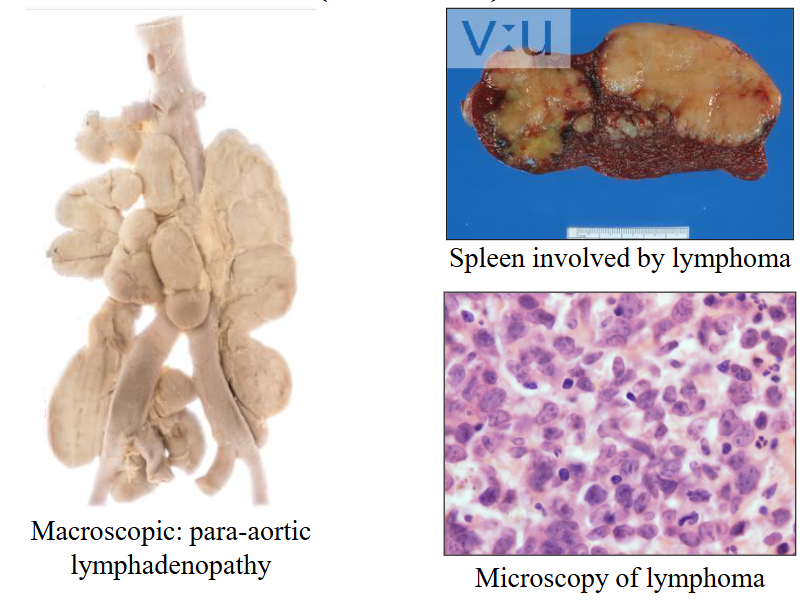
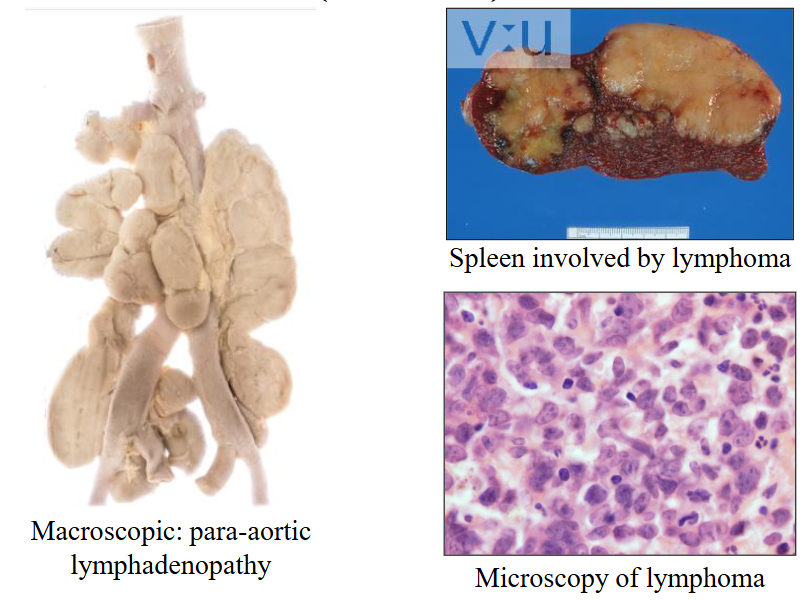
Clinical Features of NHL
- Systemic symptoms: Fever; night sweats; weight loss
- Lymphadenopathy
- Hepato-splenomegaly
.
Interference with normal organ function:
- Solid organ infiltration:-kidneys, liver, other
- Skin, brain
.
- Bone marrow failure
Diagnosis of NHL
Biopsy:
- Obtain tissue of the involved region
- Pathology of involved tissue
.
Pathological features:
- Pattern: e.g. nodular; diffuse
- Cell size: small, large
- Cell differentiation: well or poorly differentiated
.
Ancillary tests:
- Cell phenotype / lineage: B / T; other antigens
- Genetics: chromosomal rearrangements
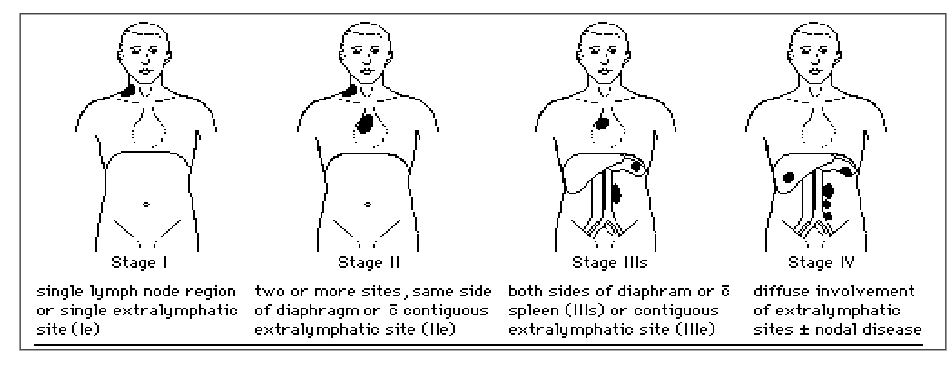
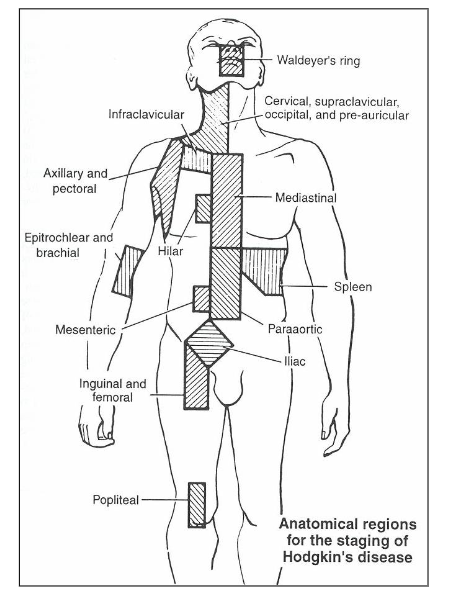
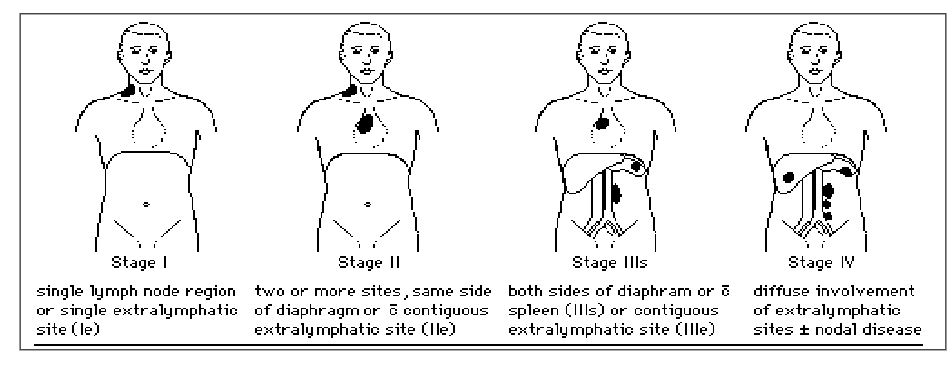
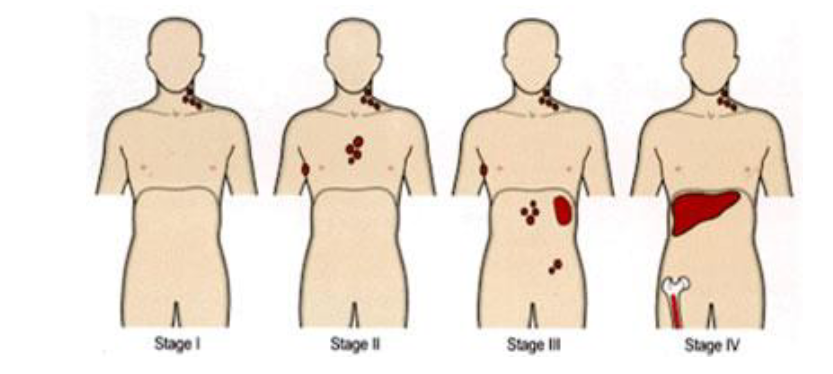
Clinical Staging of NHL
- Extent of disease; determines therapy and prognosis
- Based on physical, radiologic examination, BM
- B symptoms: fever, weight loss > 10%, night sweats
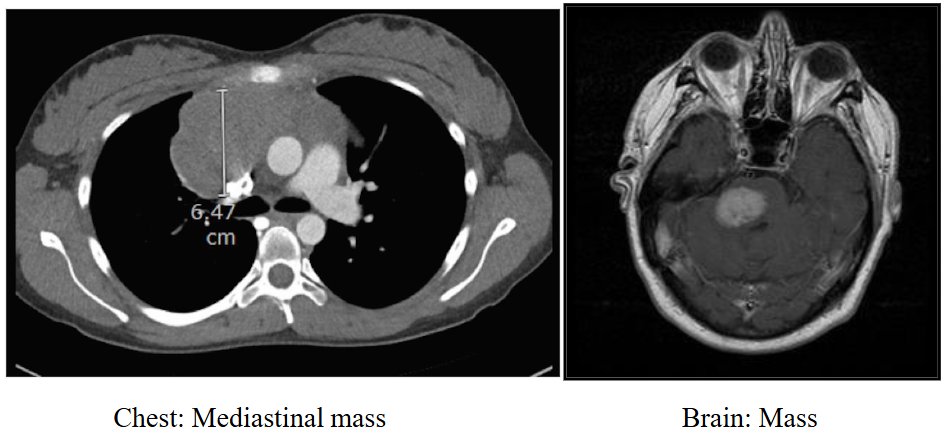
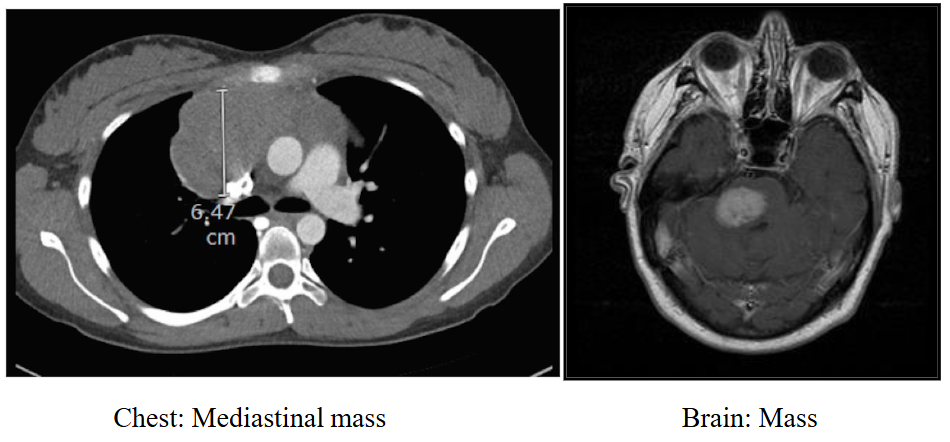
CT and MRI Scan: staging
DIAGRAM ON SLIDE 11
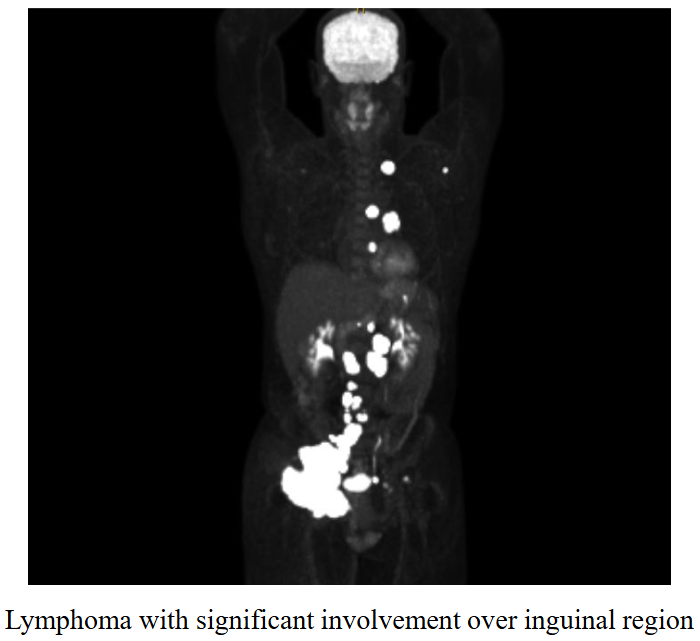
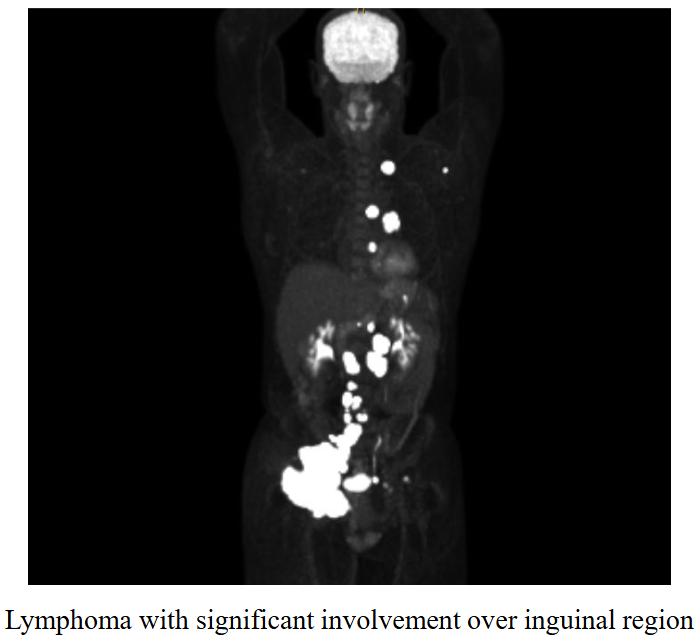
PET Scan: staging
- lymphoma with significant involvement over inguinal region
.
- PET scan is nuclear medicine scan
- gives information about activity of organs or lesions
- patient injected with glucose (he metions a radioactive dye)
- in other words, sugar is injected, carries radiation
- anything that picks up the most sugars or glucose will emit the most radiation (bright spot)
- all the dots where glucose isnt meant to be is lymphoma
.
this is to fuel the increased number of cells in these areas (which indicates increase cells in the lymph nodes)
Types of non-Hodgkin Lymphoma
Examples of non Hodgkin lymphoma:
- Low grade: Follicular lymphoma
- High grade: Burkitt lymphoma Diffuse large B cell lymphoma
1. Follicular Lymphoma
- 2nd most common type of non Hodgkin lymphoma
- Age: Adults >40 years (median age 60)
- Widely disseminated at diagnosis, incl. BM
.
Low grade B cell NHL
- B-cell phenotype: CD20, CD10, BCL2 positive
.
Clinical:
- 5-year survival 70-80% (rarely curable)
- Can be indolent
- Can transform to aggressive high-grade NHL
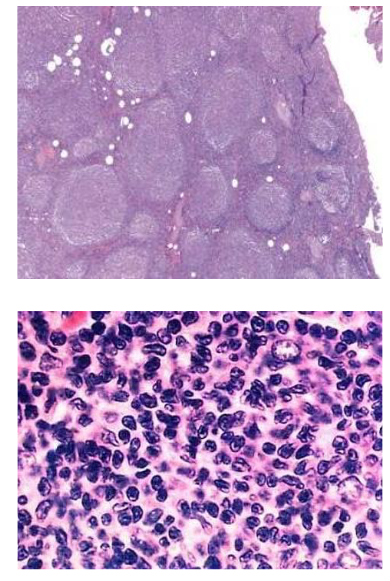
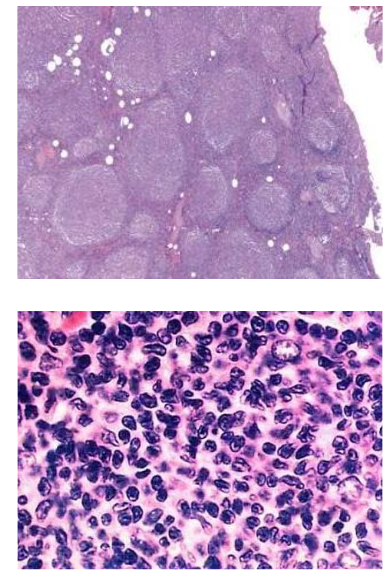
Follicular Lymphoma
- Follicular pattern
- Predominantly small cells
- t(14;18)(q32,q21);IGH/BCL2
.
Up-regulates expression of anti- apoptotic protein Bcl-2
- Survival advantage of B cells
- Anti-apoptotic: inhibits programmed cell death
Treatment of Follicular Lymphoma
- Watch and wait if indolent
.
Indications to treat:
- Constitutional symptoms; painful lymph nodes
- Anatomic obstruction or organ dysfunction
- Cytopenias: marrow failure
.
Options:
- Radiotherapy
- Chemotherapy: Bendamustine regimen
- Antibody-based therapy: anti-CD20 Obinutuzumab
- Combination therapy with antibody + chemotherapy
- Bone marrow transplantation Treatment of Follicular Lymphoma

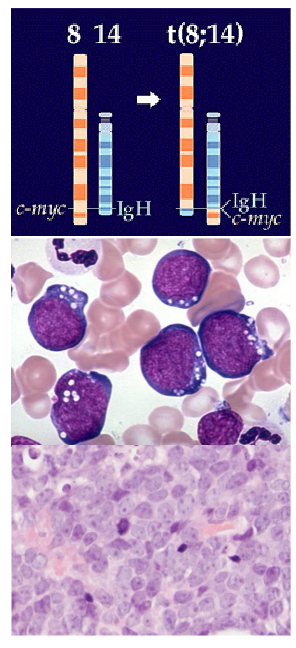
2. Burkitt Lymphoma
- Described in 1958 by Denis Burkitt
- Tumour cells derived from the germinal centreof lymph nodes
.
Aetiology: sporadic and endemic
- African variety: jaw tumor; EBV-driven
- Commonest childhood tumor in sub-Saharan Africa
.
- Age: Child or adult; 2% AIDS
- Sites: Jaw, abdominal mass, orbit
- Biology: Rapidly growing
.
- description of it is as if you are looking at a starry sky (cell apperance)

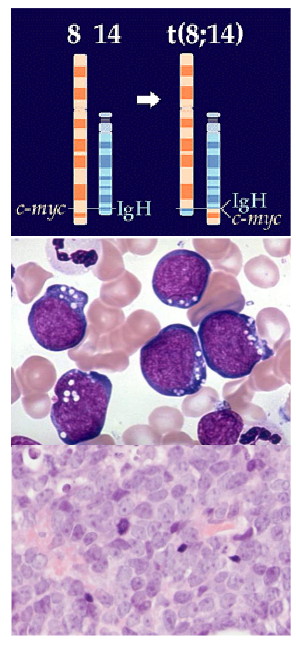
Burkitt Lymphoma
Genetics: 90% t(8;14);MYC/IGH
- Translocation of proto-oncogene c- MYC from chromosome 8 to IGH gene on chromosome 14
.
Biopsy:
- Monotonous B cell infiltrate
- "starry-sky"; high mitotic rate
- Derived from germinal centre B-cells
.
- Treatment: aggressive chemotherapy
- Potentially curable
3. Diffuse Large B-cell lymphoma
- Most common lymphoma: 30% NHL
- Disease of adults: median age 65 years
- Presents with rapidly enlarging masses
.
Pathology:
- Diffuse infiltration by large cells (usually B cells)
- Diverse histology; high proliferation rate
Diffuse Large B-cell lymphoma (DLBCL)
Most common form of NHL
Prognosis for DLBCL
Aggressive NHL: International prognostic index (score)
- Age: < 60 vs > 60 years
- Performance status: 0 or 1 vs 2-4
- LDH: <1 or >1x normal
- Disease stage: 1, 2 vs 3, 4
- Extra-nodal involvement: <1 vs >1 site
.
Treatment: depends on site/s, stage, age
- Combination chemotherapy + CD20; radiotherapy
.
- Radiological monitoring: CT, PET/CT
Treatment of DLBCL
- Mortality if not treated given aggressive disease (watch and wait is not an option)
.
Treatment options:
- R-CHOP chemotherapy +/- Radiotherapy
- Combination therapy with antibody + chemotherapy
- Effector cells therapies
- Bispecific Antibodies, CD3xCD20 engagers
- CAR (Chemeric Antigen Receptor) -T cell therapy
.
Rx: combination chemotherapy (e.g. CHOP-R)
- Complete remission rates: 70-80%
- Approximately 60% curable
- CAR T-cell or bispecific antibodies in relapse setting
.
CAR T-cell therapy is a revolutionary immunotherapy that engineers a patient’s own T cells to recognize and kill cancer cells. It involves extracting immune cells, modifying them in a lab to target specific cancer proteins, and re-infusing them to treat diseases like lymphoma, leukemia, and myeloma
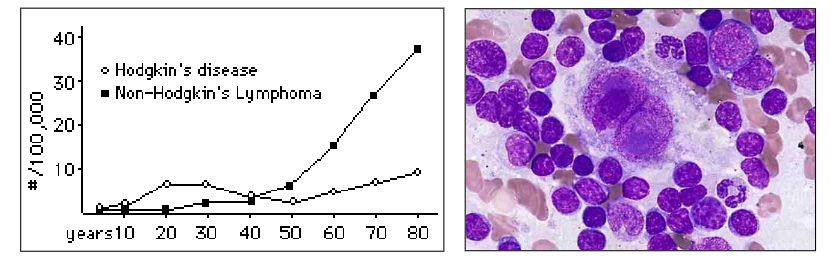
B. Hodgkin Lymphoma
- Thomas Hodgkin 1798-1866
.
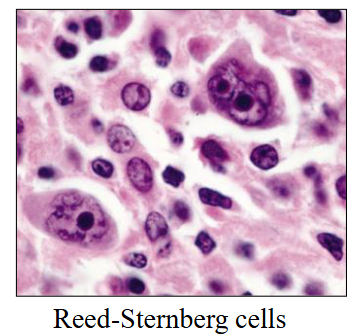
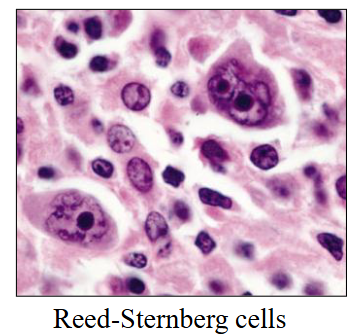
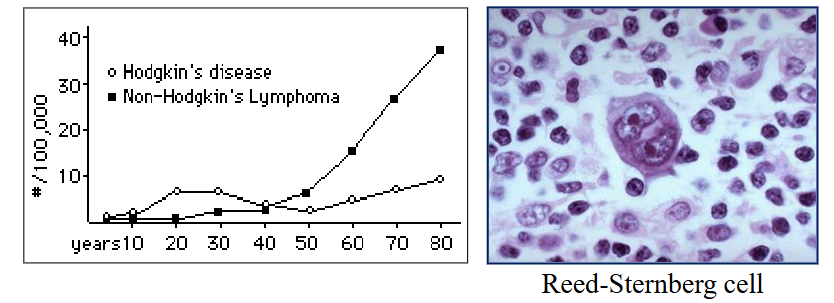
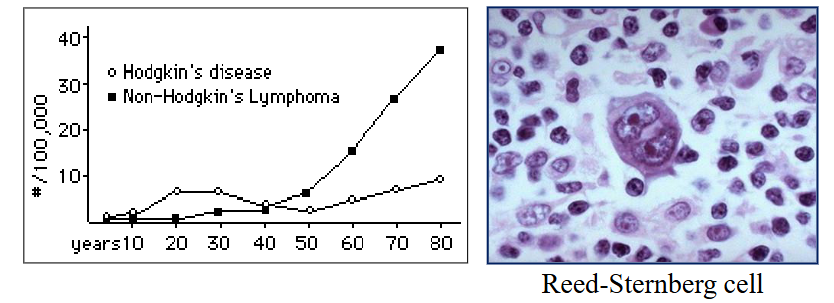
Hodgkin lymphoma (Hodgkin's disease) is characterised by the Reed-Sternberg cell:
- Minor cell component with an inflammatory cell background
.
Bimodal age incidence:
- Young adults (20-30 yrs) and > 50 yrs
Hodgkin Lymphoma: Clinical Features
Painless, non-tender, rubbery lymph nodes
- Cervical: 60-70%
- Axillary: 10-15%
- May become painful after drinking alcohol
.
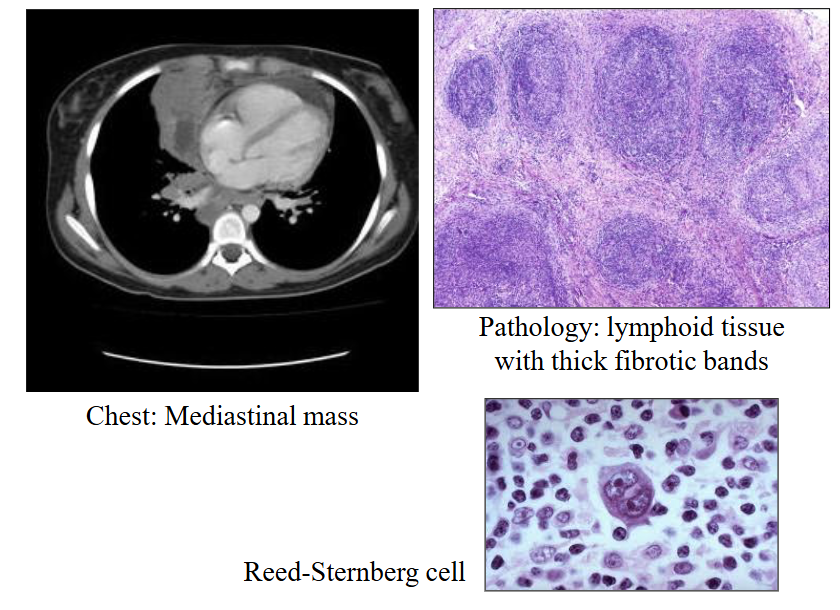
- Shortness of breath with mediastinal involvement: especially young patients
- Splenomegaly: rare at presentation
.
Constitutional symptoms ("B symptoms"):
- Fever (30%; cyclic), pruritis (itch), weight loss
Hodgkin Lymphoma: Other features
FBC: reactive blood count and film features
- Normochromic normocytic anaemia
- Leucocytosis: mild neutrophilia; eosinophilia
.
Bone marrow: usually reactive changes
- May be performed as staging procedure
- Rarely involved at presentation
.
Reduced cell mediated immunity:
- Loss of immunologically competent T cells
Diagnostic Investigations
DIAGRAM ON SLIDE 26
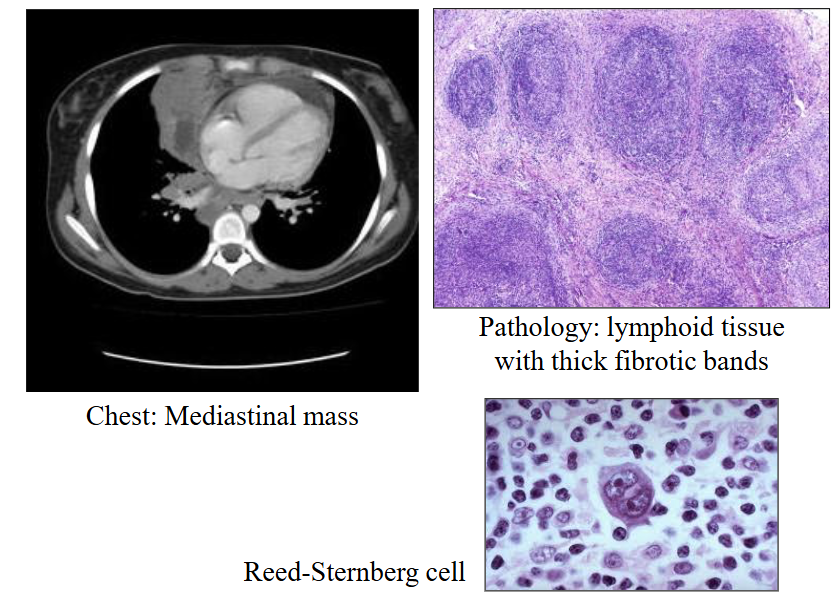
Hodgkin Lymphoma: Pathology
Diagnosis on histology of lymph node or tissue:
- Reed-Sternberg cell: Large, bi- or multi-nucleate; prominent nucleoli ("owl eye"), Pathognomonic = indicative; characteristic of Hodgkin
- Inflammatory cells: lymphocytes, histiocytes, plasmacells, eosinophils
- Variable fibrosis
.
Sub-types based on histology:
- Classified by Pathologist
- Not of major clinical significance
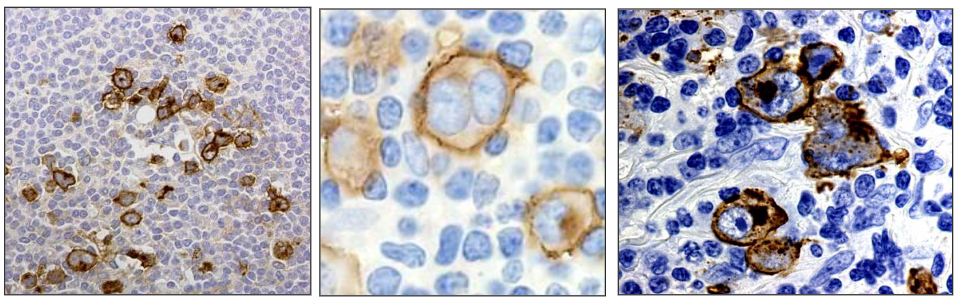
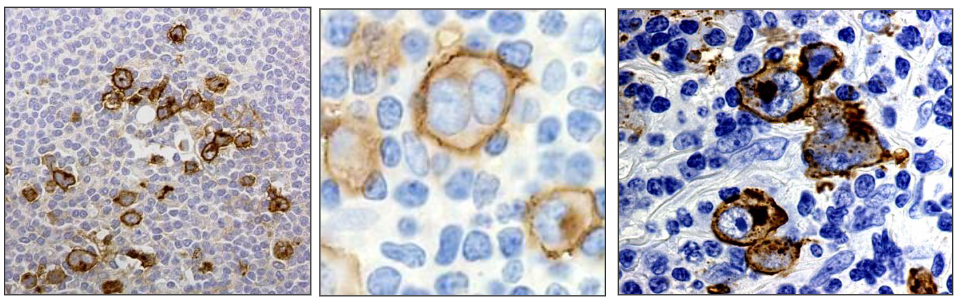
Ancillary Pathology Studies
Immunophenotyping:
- Reed-Sternberg cells express CD15 and CD30 antigens and are CD45 negative
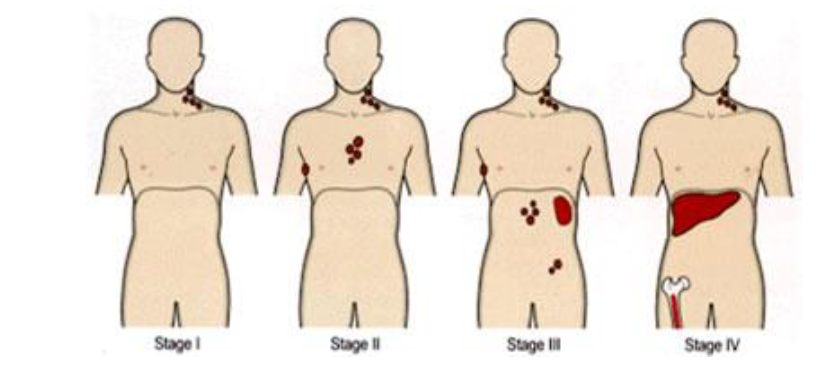
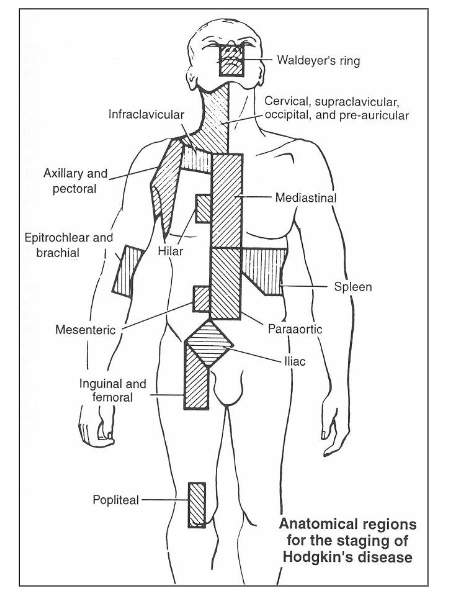
Hodgkin Lymphoma: Staging
- Clinical staging: PET/CT
A: No B (systemic) symptoms
B. "B symptoms" (fever, night sweats, weight loss)
Treatment of Hodgkin Lymphoma
- Potentially curable
.
Early stage favourable: Stage 1 and 2
- Combined modality or chemotherapy only: BV-AVD: Brentuximab, doxorubicin, vinblastine and dacarbazine, Involved field radiotherapy
.
Advanced disease: stage 3 and 4
- ABVD: doxorubicin, bleomycin, vinblastine and dacarbazine
- More intensive combined chemotherapy
Late Effects of Therapy
Second malignancies:
- 10% at 10 years
- 25% at 30 years
.
- Lung cancer (from radiotherapy): most common
- AML (from cumulative dose of akylating agents)
- Breast cancer (radiotherapy to mediastinum / axilla) (Adolescent or young women, Dose-response relation exists)
- Skin cancers
Hodgkin Lymphoma: Prognosis
- Hodgkin lymphoma is a curable malignancy
- Overall cure rate approximately 80%
- Prognosis based on staging and bulk of disease
- Infections: reduced cell-mediated immunity
.
Relapsed disease: can be treated
- Autologous bone marrow transplant
- Second malignancies can occur 5%
Hodgkin Lymphoma: summary
- A specific type of lymphoma
- Affects young adults and >50yrs
- Classical pathology: Reed-Sternberg cell
- Potentially curable (>80% cases)
- Chemotherapy, radiotherapy, transplant
- Risk of second cancer: 5%
Summary - Learning Outcomes
DIAGRAM ON SLIDE 34