EXAM 2 - Cranial Nerves & Head Structures
1/119
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
120 Terms
Cranial Nerves
The brain's way to communicate with the rest of the
body
all 12 cranial nerves arise from what and exit the cranium via what?
base of the brain and the foramina
all 12 cranial nerves lead mostly to
Lead mostly to sense organs and muscles in the head and neck 1 exception: vagus n - to the whole body
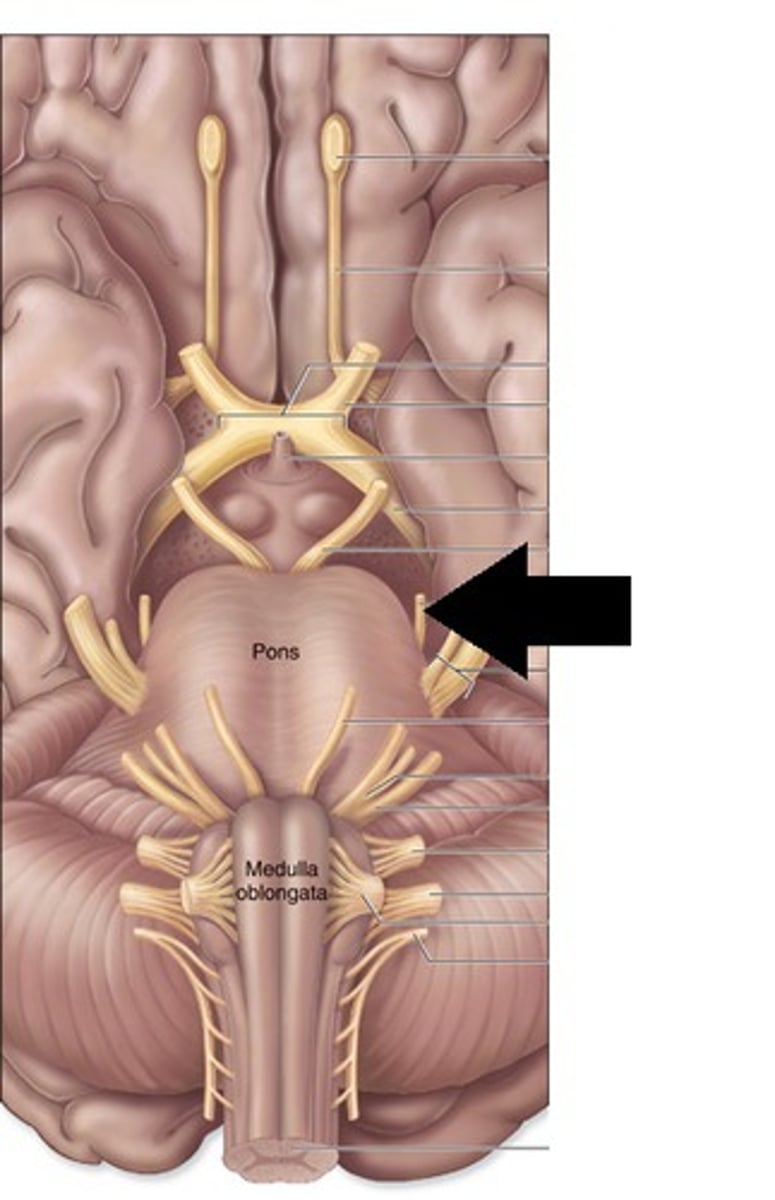
Cranial Nerve Pathways
Many begin in nuclei of the brainstem
⚫ Sensory fibers begin in receptors located mainly in
head and neck and lead mainly to the brainstem
⚫ Most cranial nerves carry fibers between brainstem
and ipsilateral receptors and effectors
Lesion on the L side of the brain stem causes a defect in what side of the body?
left (same side) - Most cranial nerves carry fibers between brainstem and ipsilateral receptors and effectors
Exceptions to cranial nerves carrying fibers between brainstem and ipsilateral receptors and effectors
1. optic nerve - 1/2 (nasal) fibers cross (partial decussation)
2. trochlear nerve - all contralateral
Sensory CN
I, II, VIII
1,2,8
Motor CN
III, IV, VI, XI, XII
3,4,6,11,12
Mixed CN
V, VII, IX, X
5,7,9,10
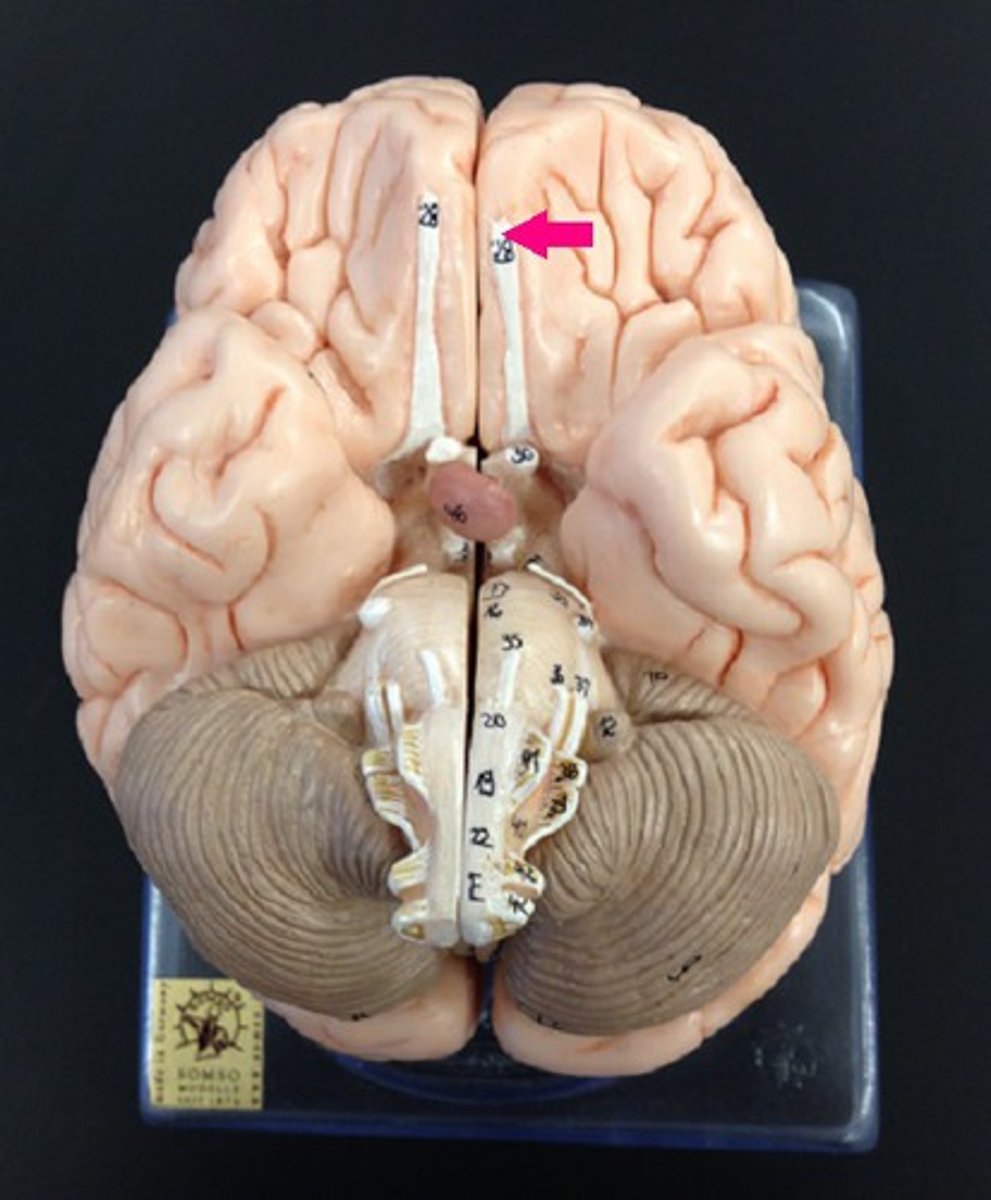
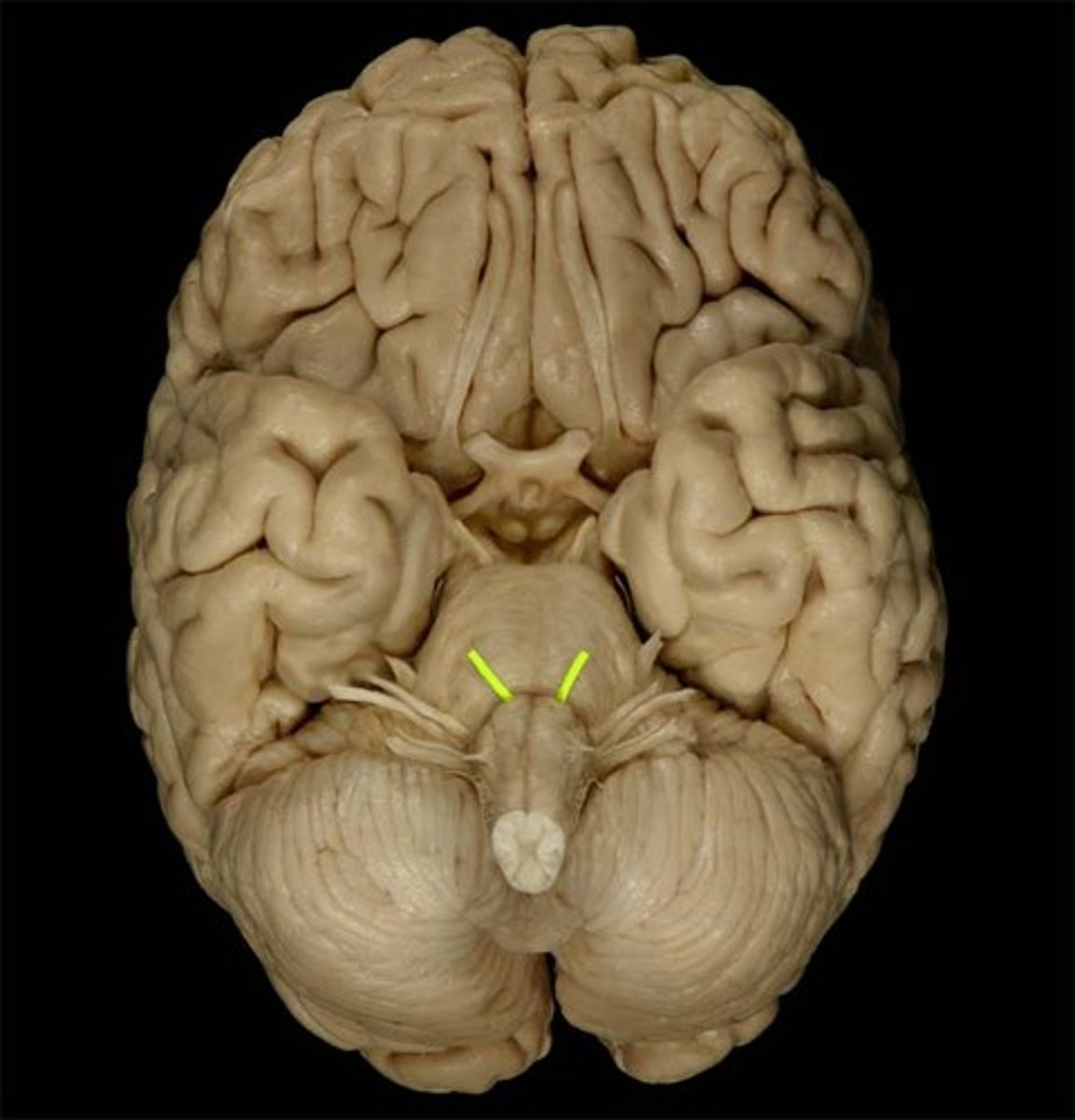
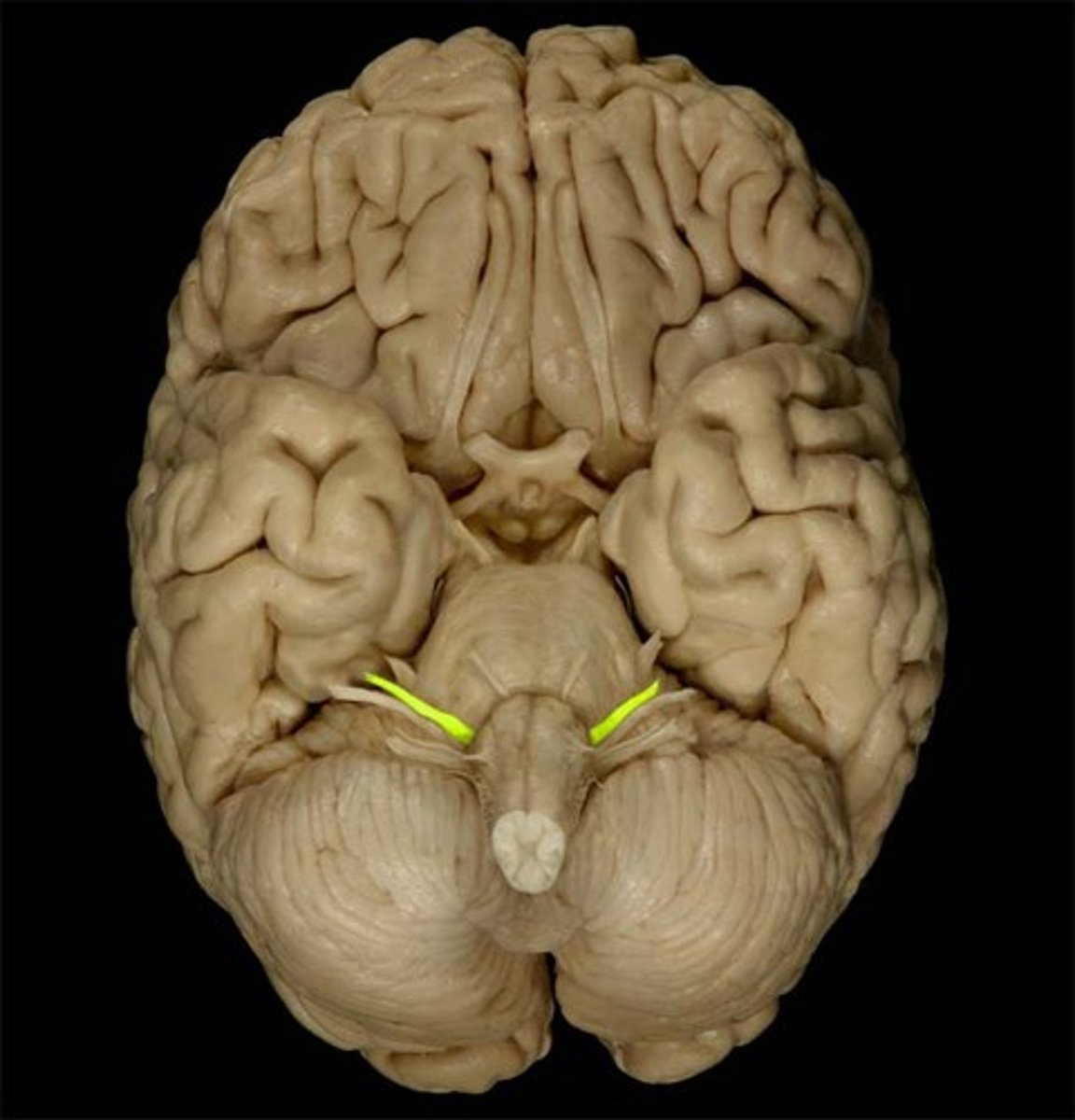
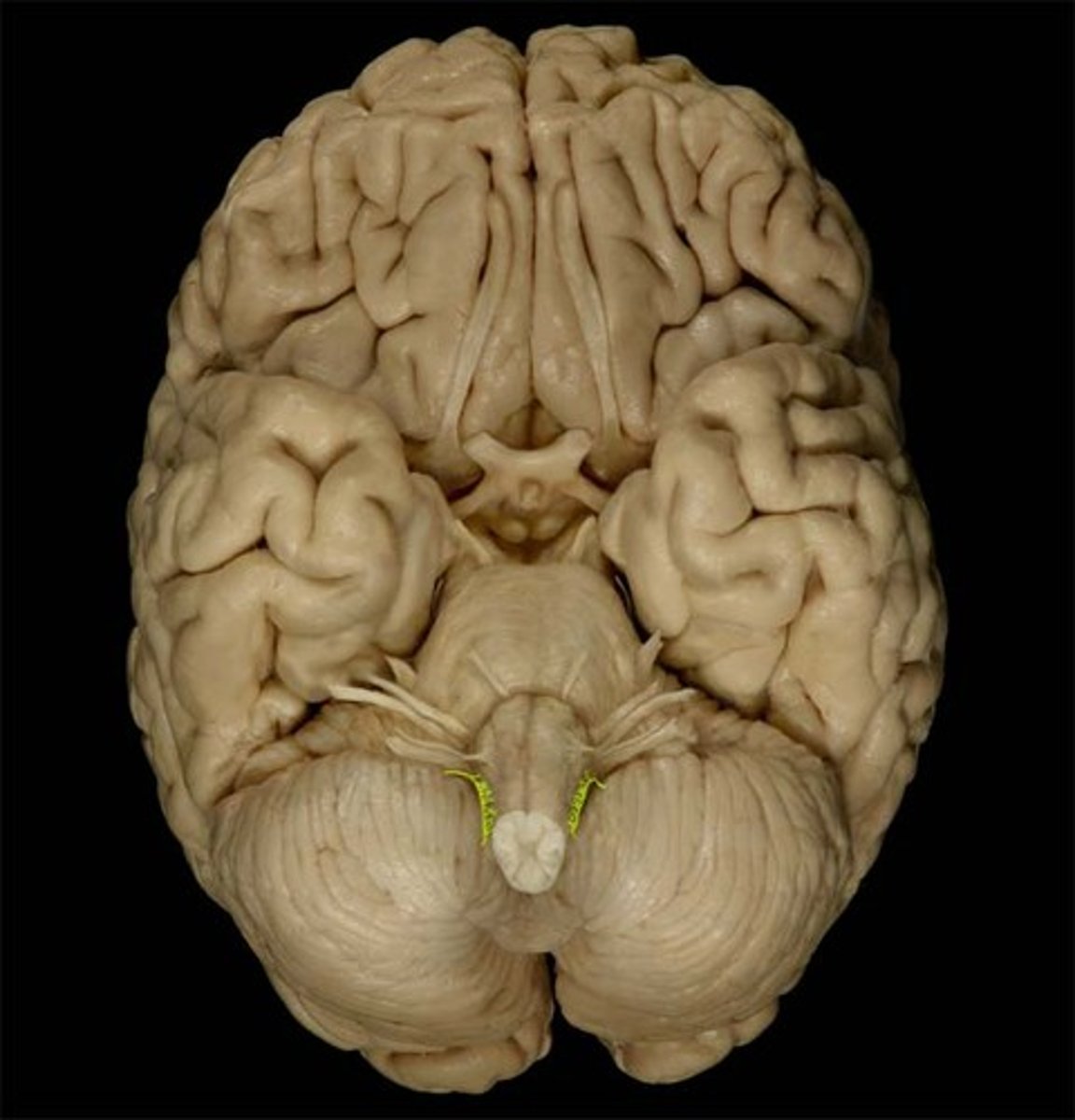
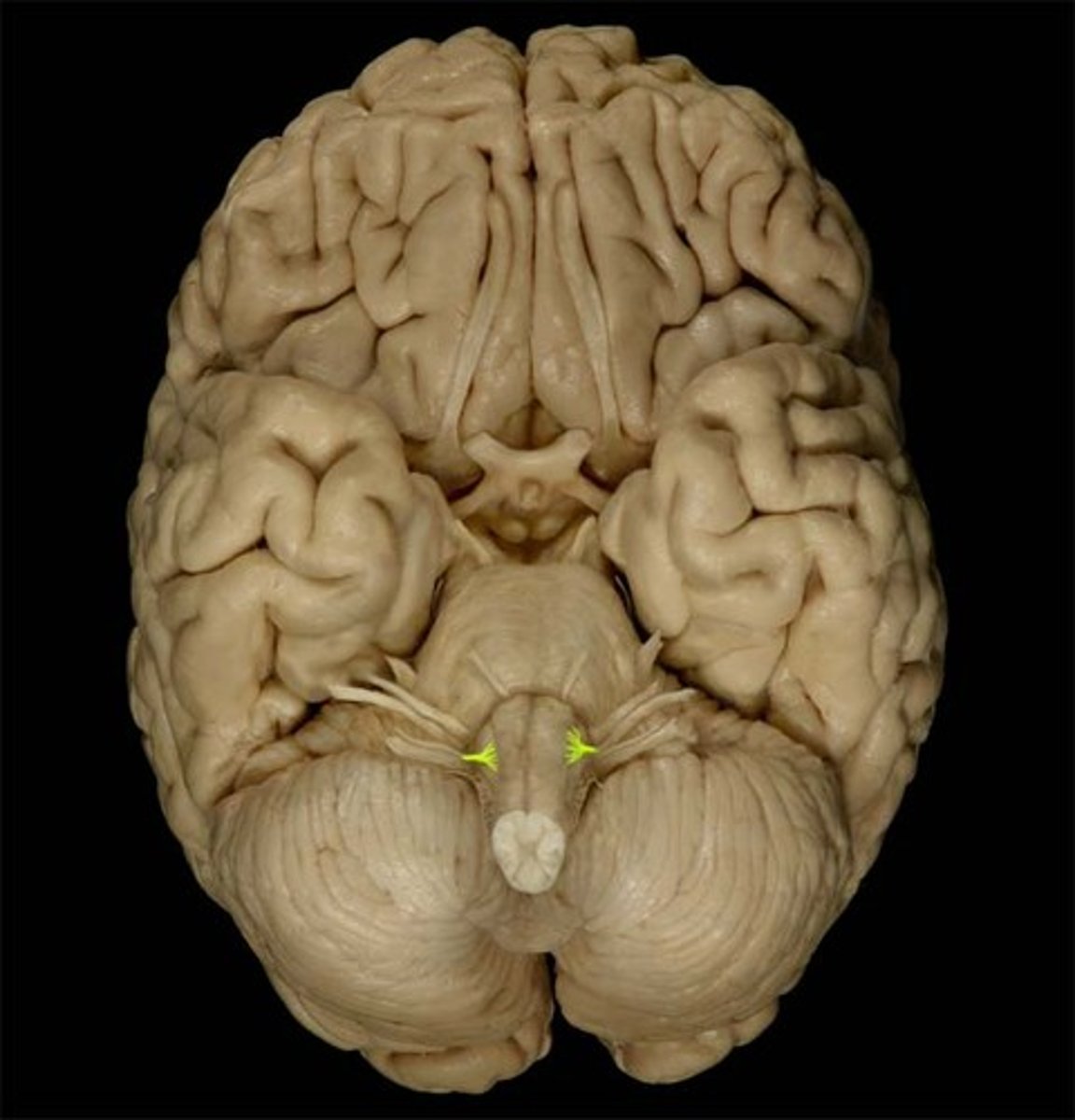
CN1
olfactory nerve
Sensory Nerve - for SMELL only. Originates in the nasal mucosa as fascicles of the olfactory n. Passes thru foramina in the cribriform plate of the ethmoid bone. Ends at the olfactory bulb.
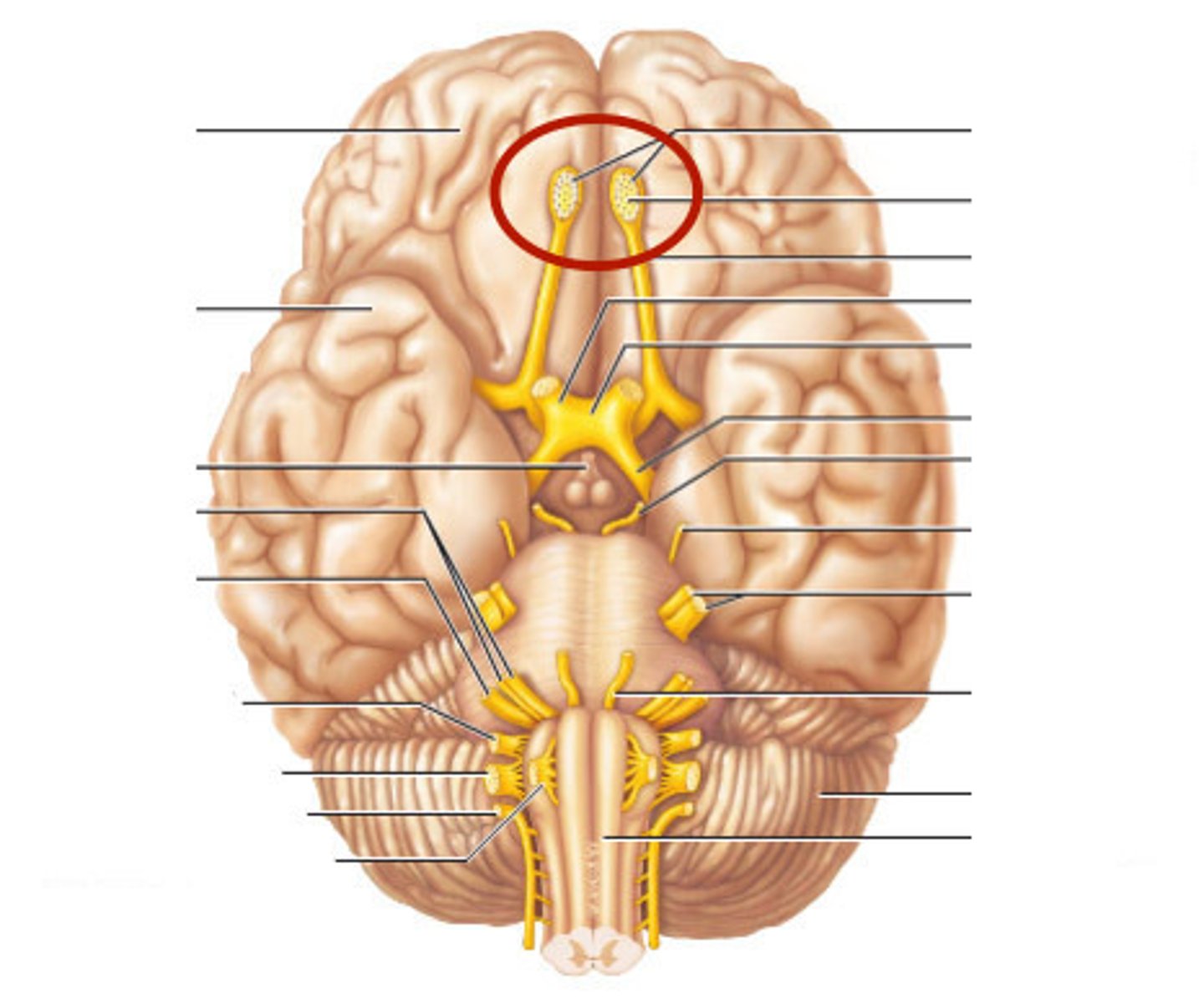
olfactory tract
the path along which the olfactory receptors send their electrical messages to the brain.
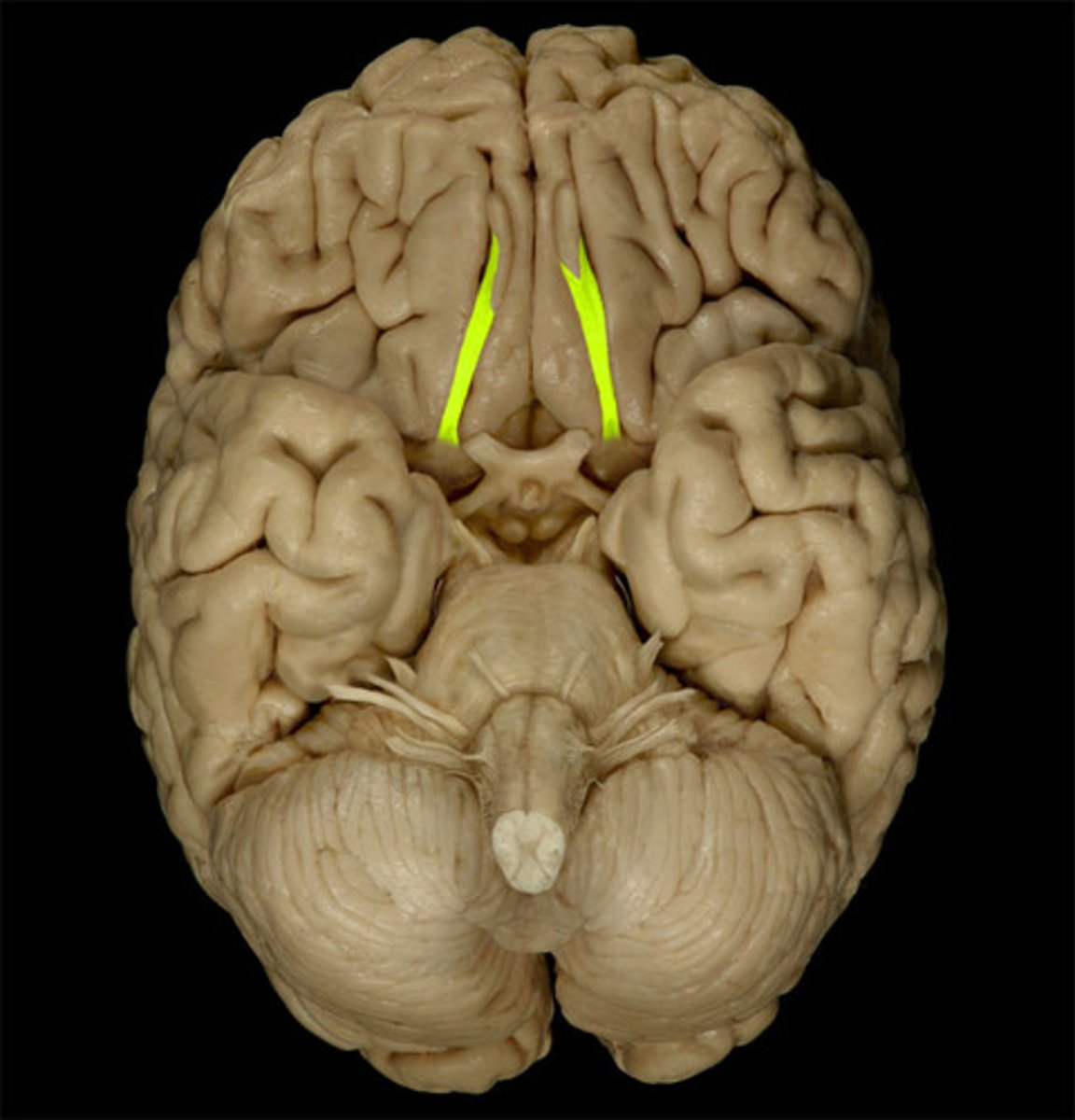
olfactory bulb
a brain structure located above the nasal cavity beneath the frontal lobes
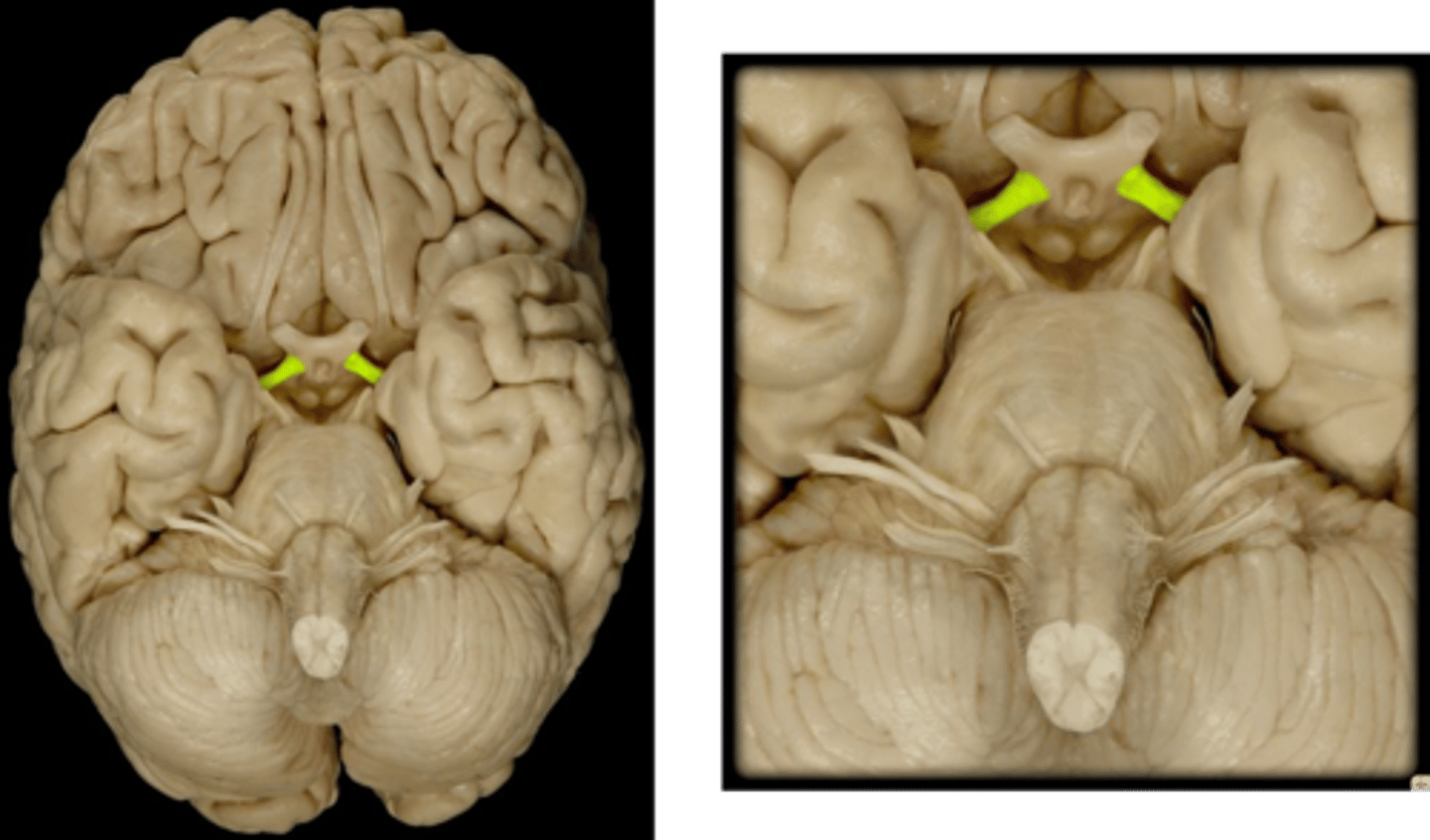
CNII
Optic Nerve
Sensory for VISION only
partial decussation at the optic chiasm
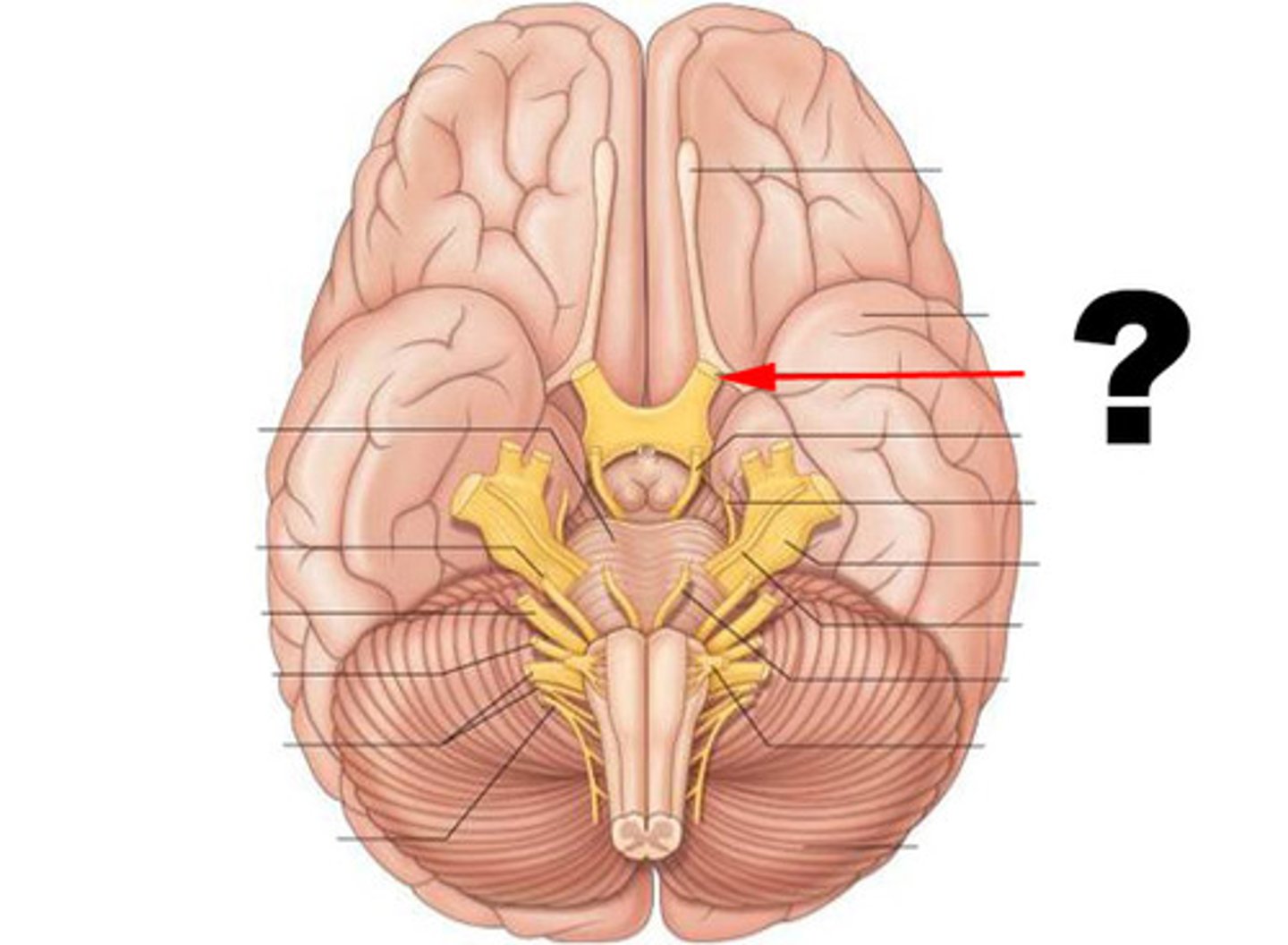
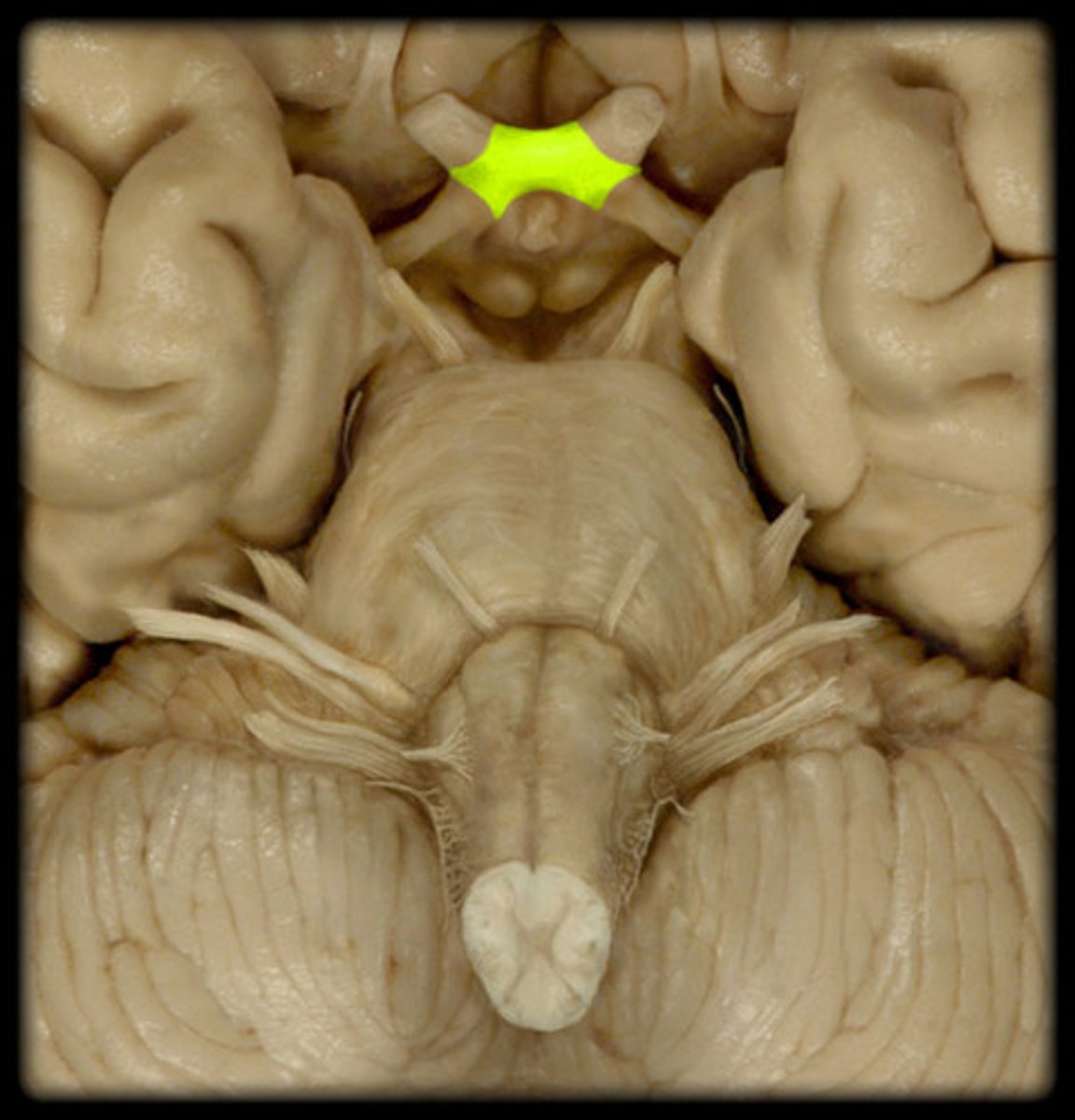
optic chiasm
point at which optic nerve fibers cross in the brain
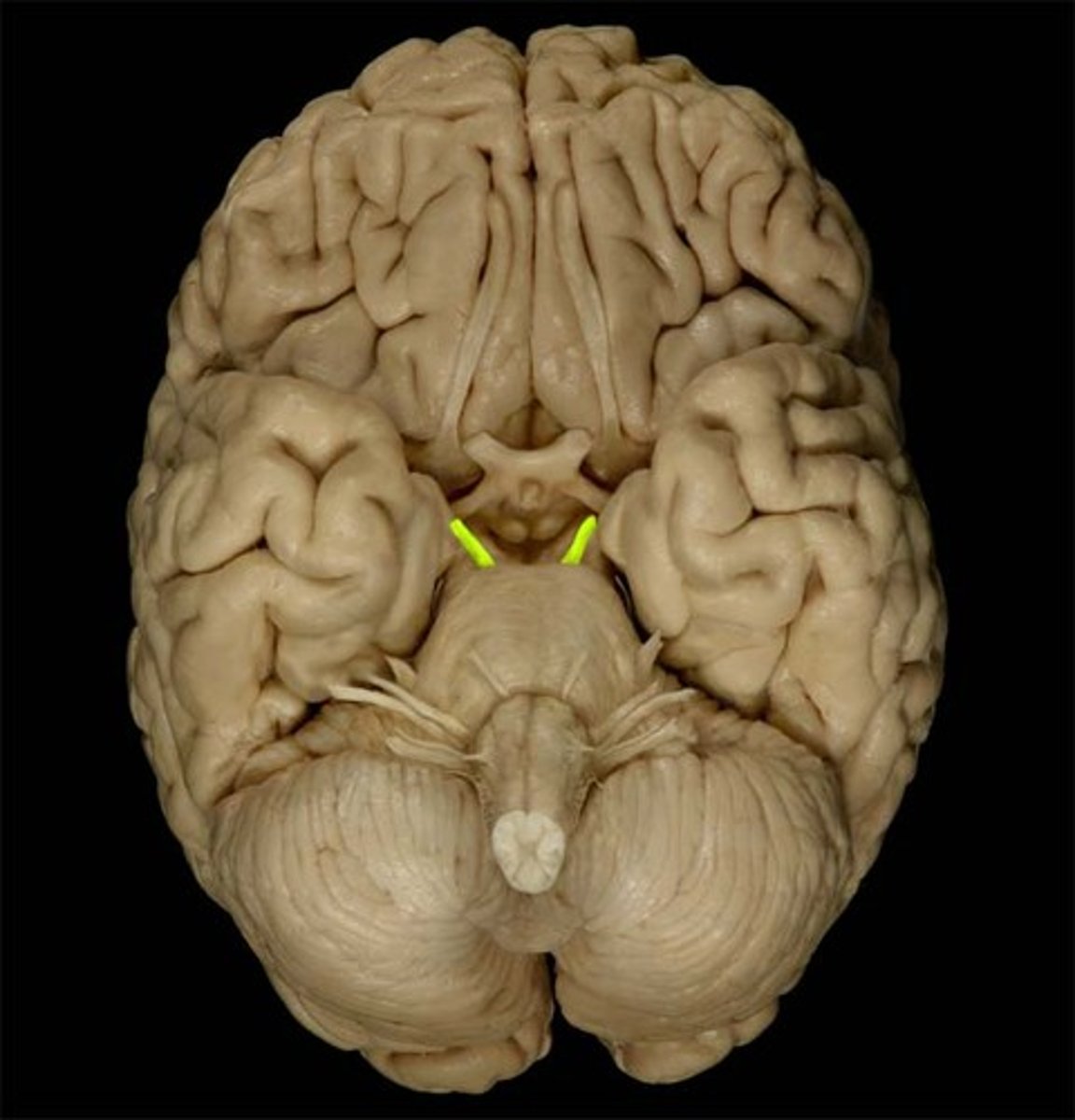
optic tract
How information from the optic nerve travels to the thalamus.
mixed fibers medially and laterally
CN III
Oculomotor Nerve
motor only
Innervates extraocular muscles (Superior Rectus, Medial Rectus, Inferior Rectus, Inferior Oblique).
Action: move eyeball up, down, and medially
control iris, lens, and upper eyelid
injury to CN III
-drooping eyelid (ptosis), pupil dilation, in ability to move eye in certain directions
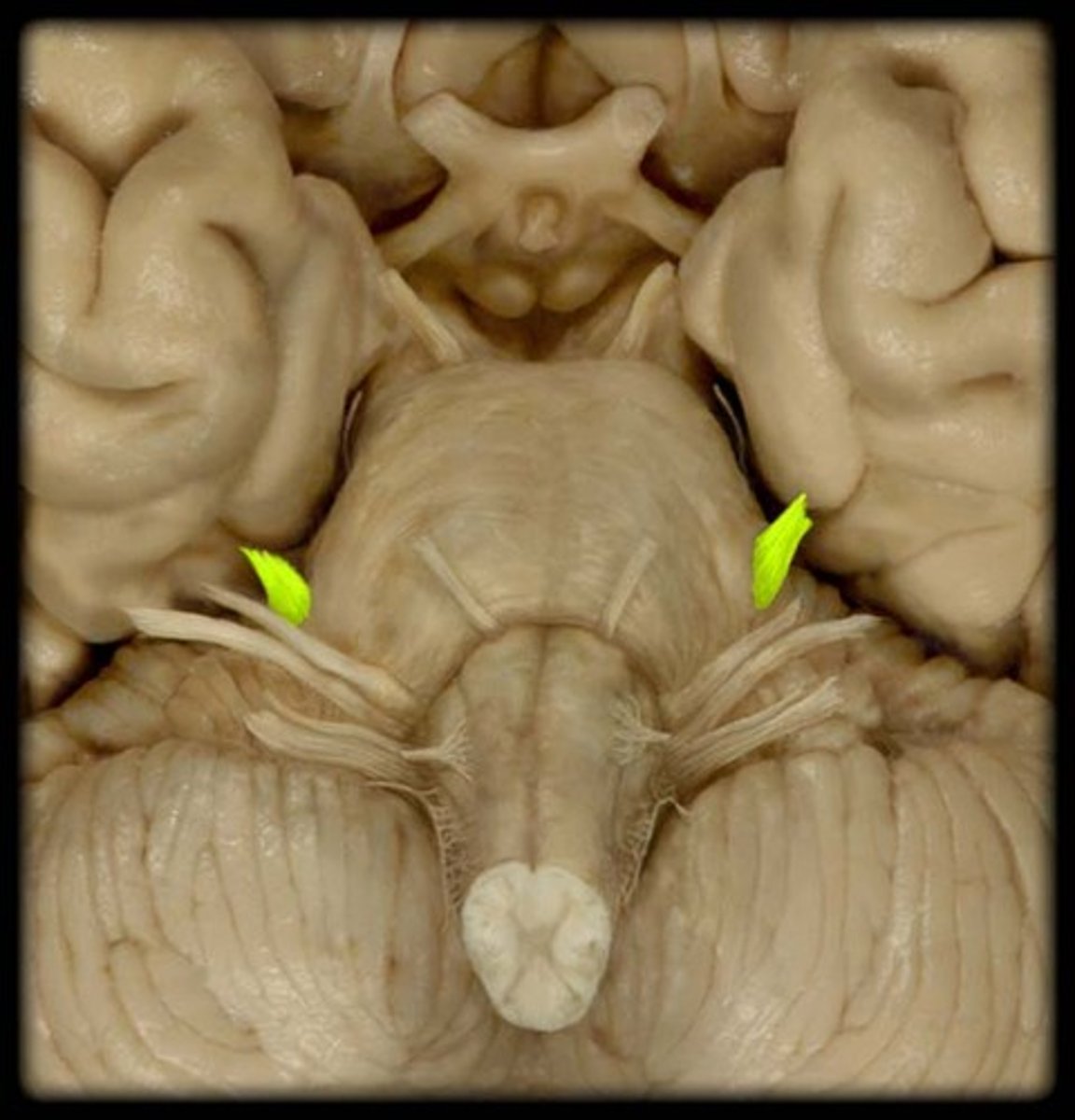
CN IV
Trochlear Nerve
motor only
innervates contralateral superior oblique muscle
Motor: abducts, depress, and inferiomedially moves eye (intorsion)
injury to the trochlear nerve
effects are CONTRALATERAL
-paralysis of superior oblique
-impaired ability to turn the affected eyeball inferomedially (leads to extorsion)
- diplopia (double vision)
- Clinically: inability to look down when eye is adducted
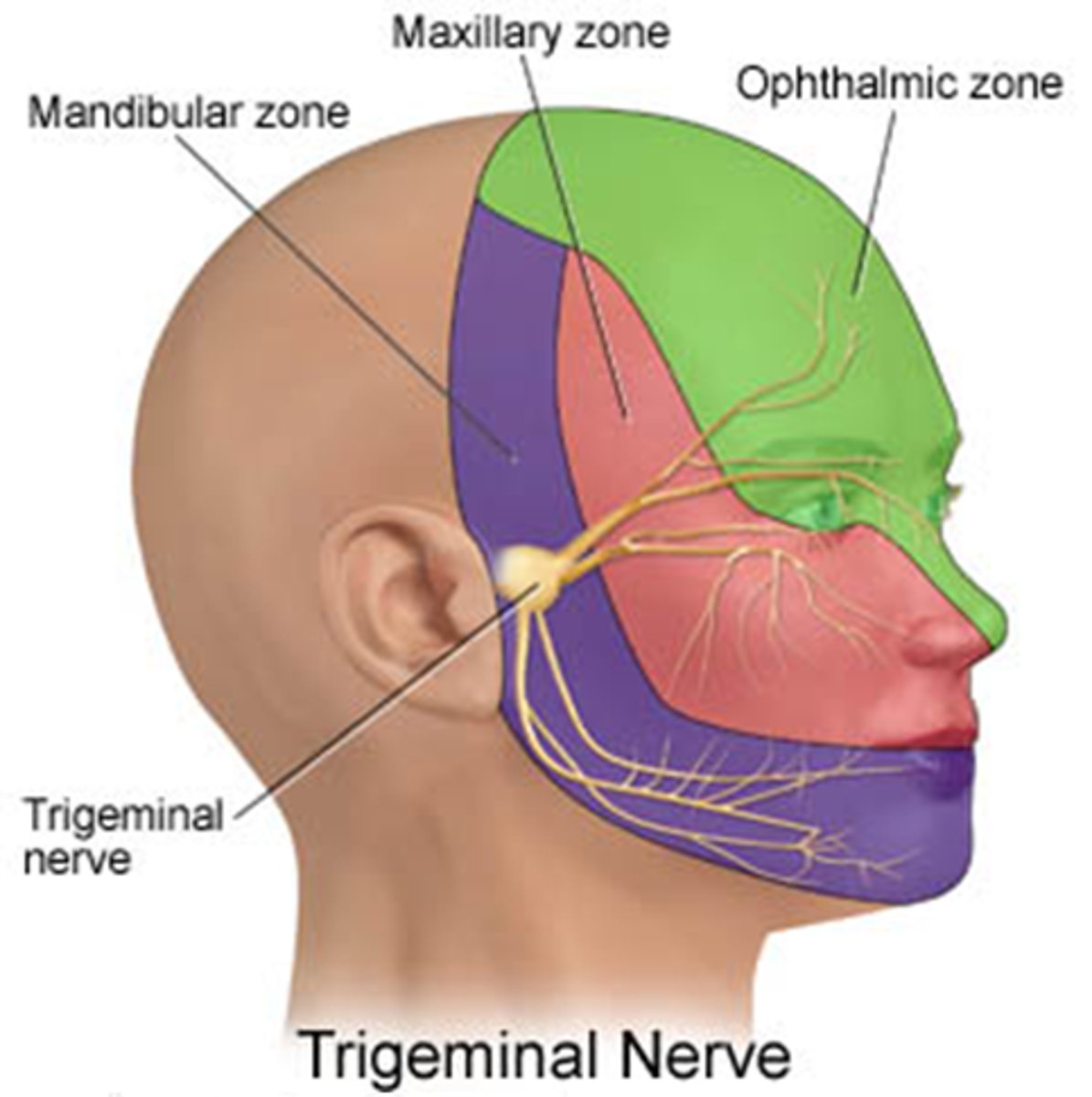
CN V
Trigeminal Nerve largest of the CN with a wide sensory distribution to the face and scalp via three branches
"great sensory nerve"
MOST IMPORTANT SENSORY N OF FACE (this is the dentist nerve)
mixed(sensory and motor)
Trigeminal (CN V)
⚫ 3 branches (V1, V2, V3)
Sensory: forehead, face, jaws (V1, V2, V3)
⚫ Supply dermatomes of face (Posterior region of the head via dorsal roots of cervical spinal nerves)
Motor: (V3) for motor outflow to the muscles of
mastication (chewing)
"Oh My Molars"
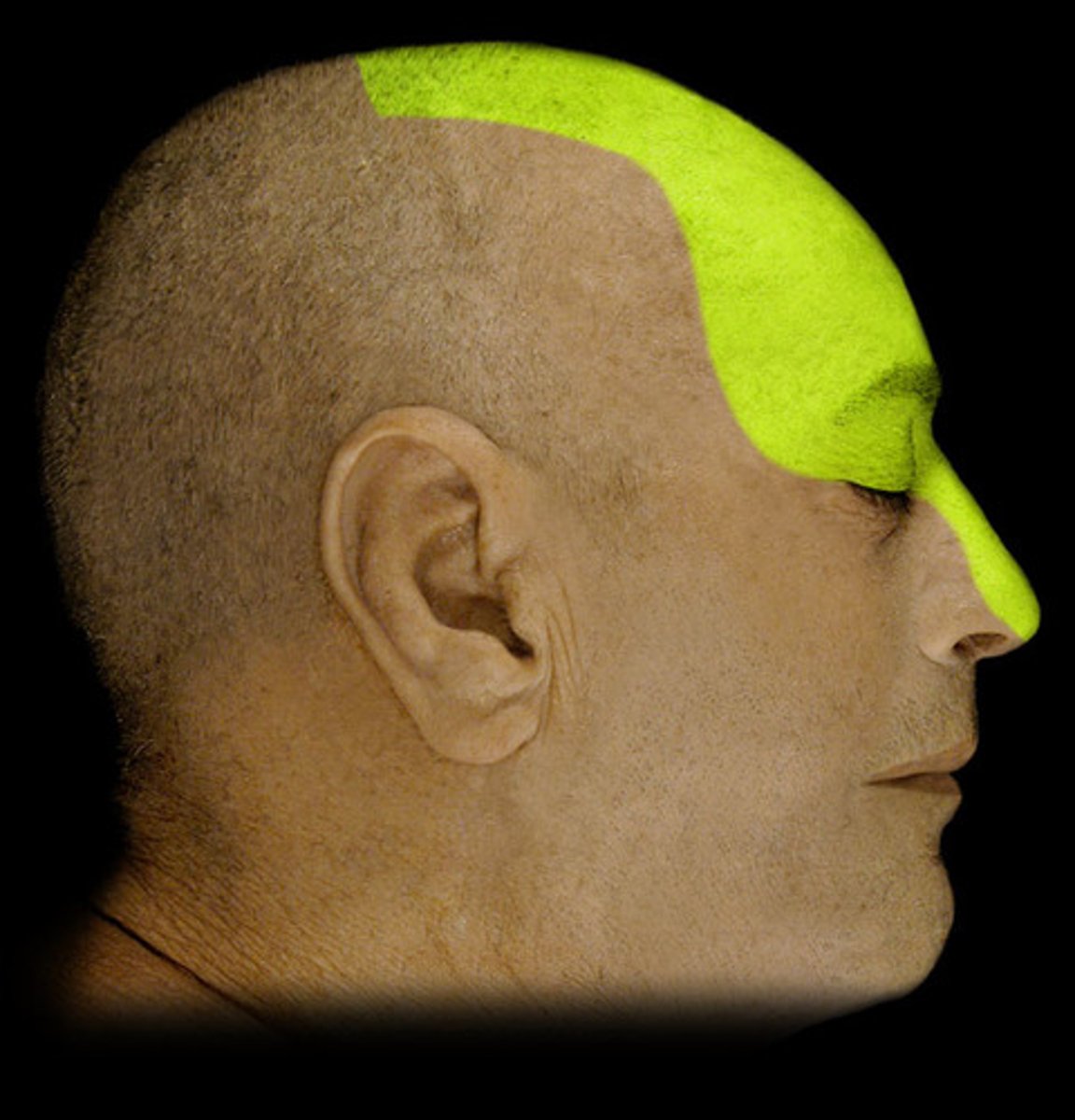
V1 (Ophthalmic nerve) Fxn
general sensory in forehead region
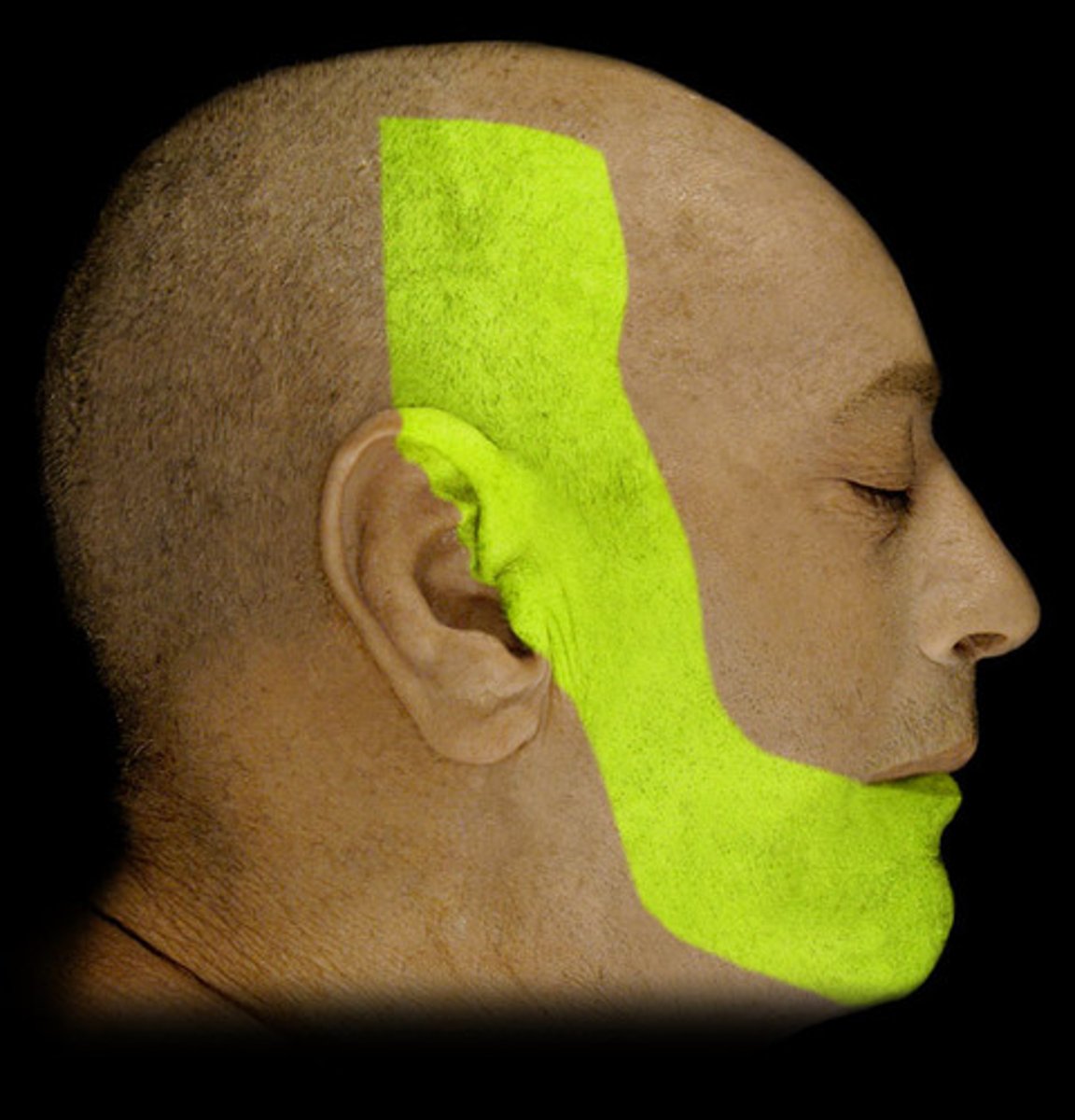
V2 (Maxillary nerve) Fxn:
general sensory below the eye

V3 (Mandibular nerve) 2 Fxn's
1. Sensory for the lower jaw/mandible and tongue
2. motor innervation of muscles of mastication
Clinical Application - sinus infections
most commonly in the maxillary sinus
-common complaint is a aching of molar teeth because the V2 branches (superior alveolar nerve) innervates the sockets/alveoli of the teeth and mucous membranes of sinuses
- pressure in the sinuses can radiate into the teeth and cause horrible tooth ache in molars because of this overlapping innervation
Trigeminal Nerve-3 Divisions
Cranial Nerve V
1. Ophthalmic
2. Maxillary
3. Mandibular
Clinical Highlight
⚫ Trigeminal Neuralgia (tic douloureux)
Recurring Episodes of intense stabbing pain where CNV innervates (mouth, nose)
Even small stimuli/triggered by:
- light touch
- drink Hot/cold water
- washing face
overactive nerve leads to intense pain to the point of severing the nerve
CN VI
Abducens Nerve
motor only
Innervates the lateral rectus muscle
action: moves the eye laterally
Injury in CN VI
results in an inability to the move the eye laterally, eye appears to move medially
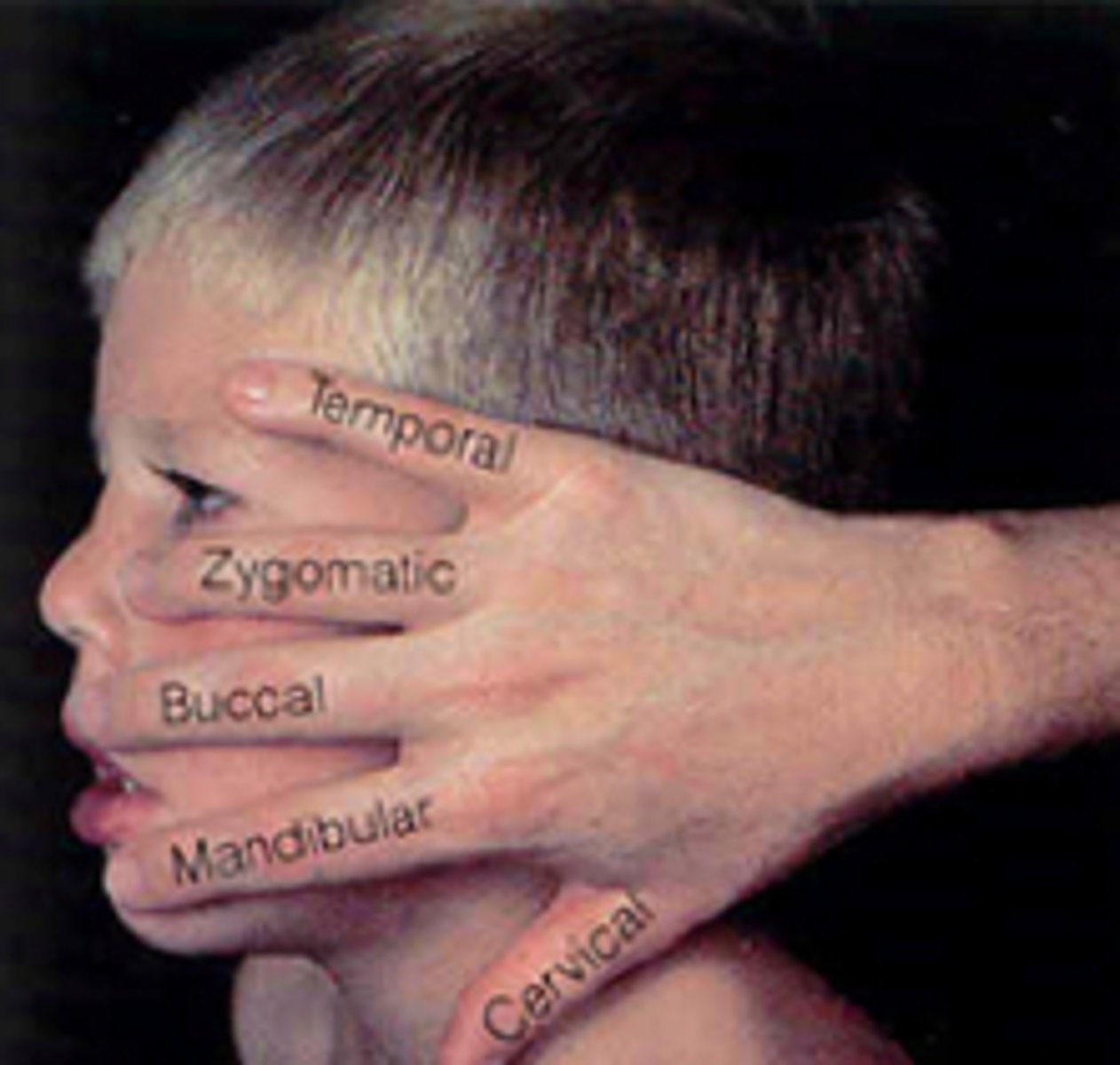
CN VII
Facial Nerve
"Great motor nerve"
- special motor outflow to facial muscles (muscles of facial expressions)
- special sensory to the taste on anterior 2/3 of tongue
5 Main branches of the N
5 main branches of CN VII
branch division occurs deep to the R/L parotid gland
Temporal
Zygomatic
Buccal
Mandibular
Cervical
"those zany biologists memorize cranial nerves"
Injury to the CN VII
lose taste of anterior 2/3 tongue, lose ability to move facial muscle
how to test motor function of CN VII
Ask pt. to wrinkle forehead. Have pt. shut eyes tightly while I try to open them. Raise eyebrows. frown. puff out cheeks. Ask pt. to smile. See if pt. can do these and if there is asymmetry.
Bell's Palsy
paralysis of facial n
- cause: stroke, aneurysm, virus (stress reactivates virus leading to inflammation around facial nerve and paralysis)
Can be pregnancy induced (but cant treat while pregnant)
- drooping of the face on one side
- painful onset
- lost sense of taste (sweet and salty)
- everything is bitter
- problems closing eye, mouth (sipping straw, mouthwash, brushing teeth
- within a year of onset, what has not been repaired is most likely gone
-treatment with painkillers, steroids, antivirals
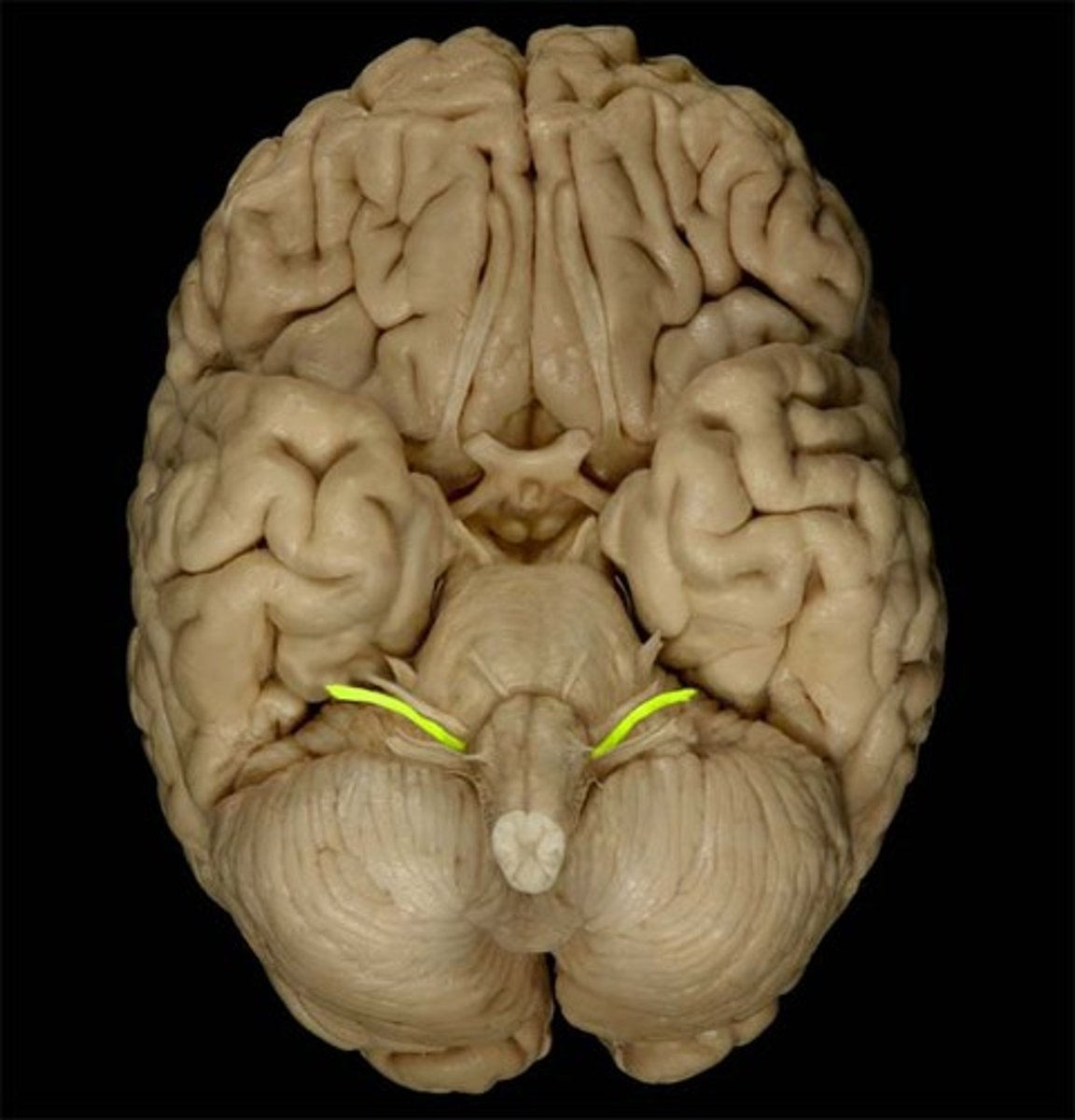
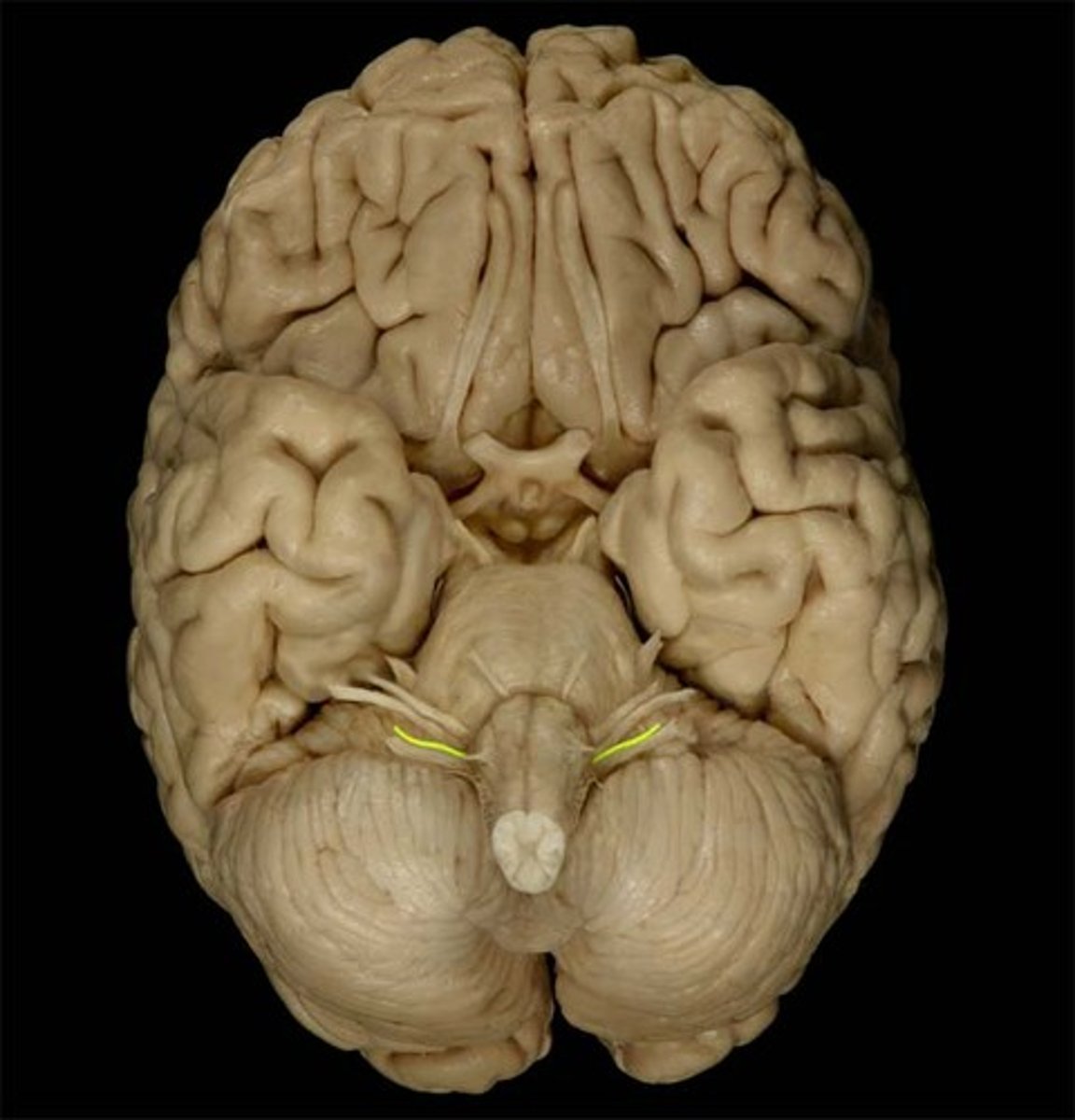
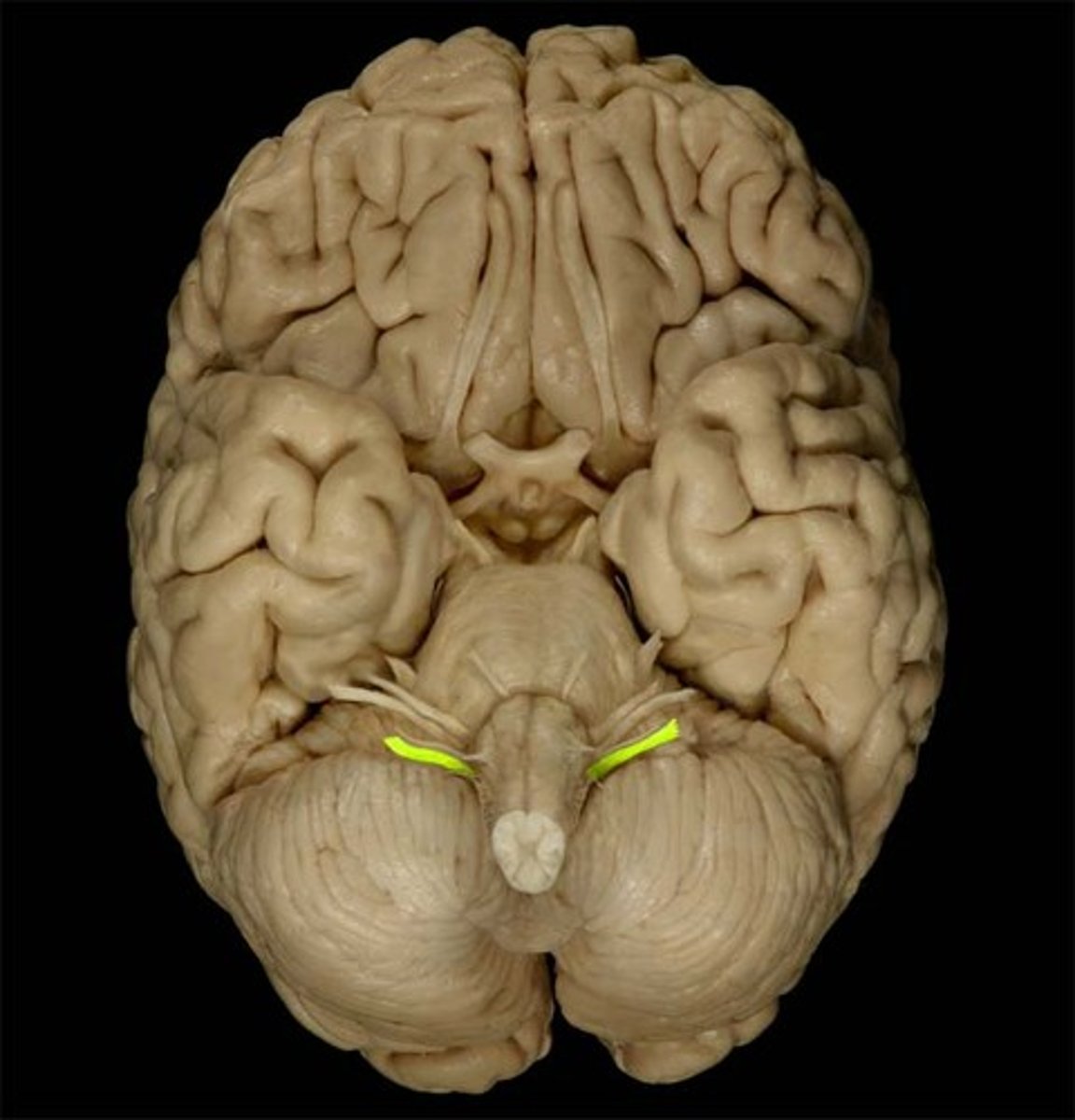
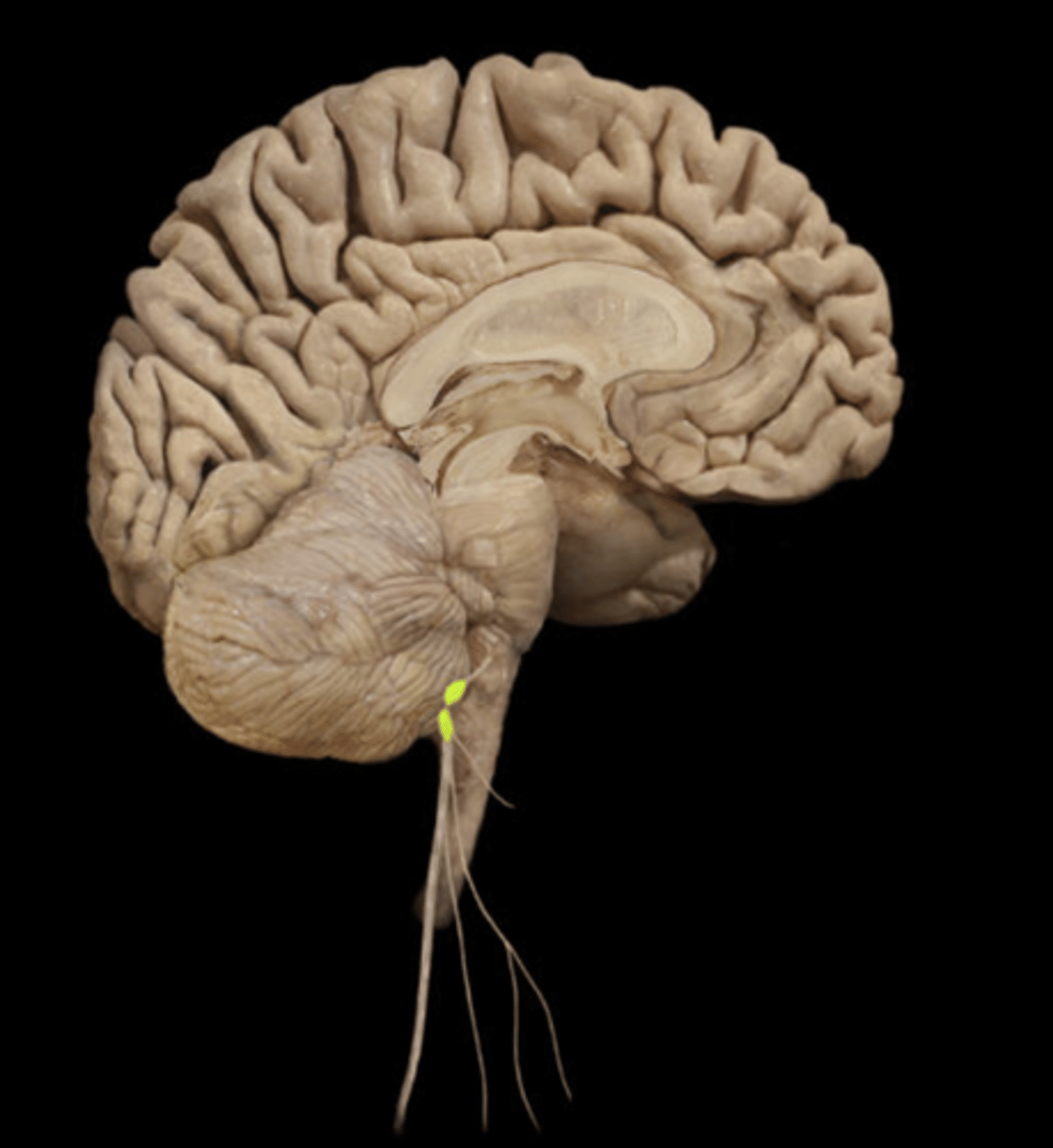
CN VIII
Vestibulocochlear Nerve
sensory (only) cranial nerve within the labyrinth that consists of two branches, the vestibular nerve (for balance) and the cochlear nerve (for hearing)
injury to CN VIII
nystagmus, deafness, and others
CN IX
Glossopharyngeal Nerve
mixed (sensory and motor)
Sensory: taste for posterior 1/3 of the tongue (bitter)
Motor: control of swallowing, salivation, gag reflex, controls BP and respiration
Injury to CN IX
Loss of bitter taste, impaired swallowing, impaired ability to regulate BP and respiration, impaired gag reflex
CN X
Vagus Nerve
mixed nerve (sensory and motor)
Wondering Nerve
- leaves the head and neck
HUGE Distribution
- cardiac
-respiratory
- GI
- reproductive
- spleen
- urinary
-etc
Injury to 1 and/or both of CN X
1 - impaired swallowing, hoarse voice, and issues with everything it innervates
Damage to both Vagus N's = DEATH
vagal ganglion
CN XI
Accessory Nerve
Motor: muscles move head, neck and shoulder
Goes down to major muscle: TRAPEZIUS and sternocleidomastoid
testing CN XI
shrug shoulders, turn head
testing the muscles allows to test nervous system (CN XI)
Injury to CN XI
impaired muscle movements (movement of head and neck)
head will turn towards one side
Hypoglossal Nerve CN XII
Motor: tongue movement for speech sound articulation, swallowing, and food manipulation
ipsilateral atrophy of CN XII
damage on one side leads to tongue deviation to that injured side
damage to both means can't stick out tongue at all
Scalp
Continuous with the skin of the neck
- Spans: from occipital bone to frontal bone, from temporal to zygomatic arch
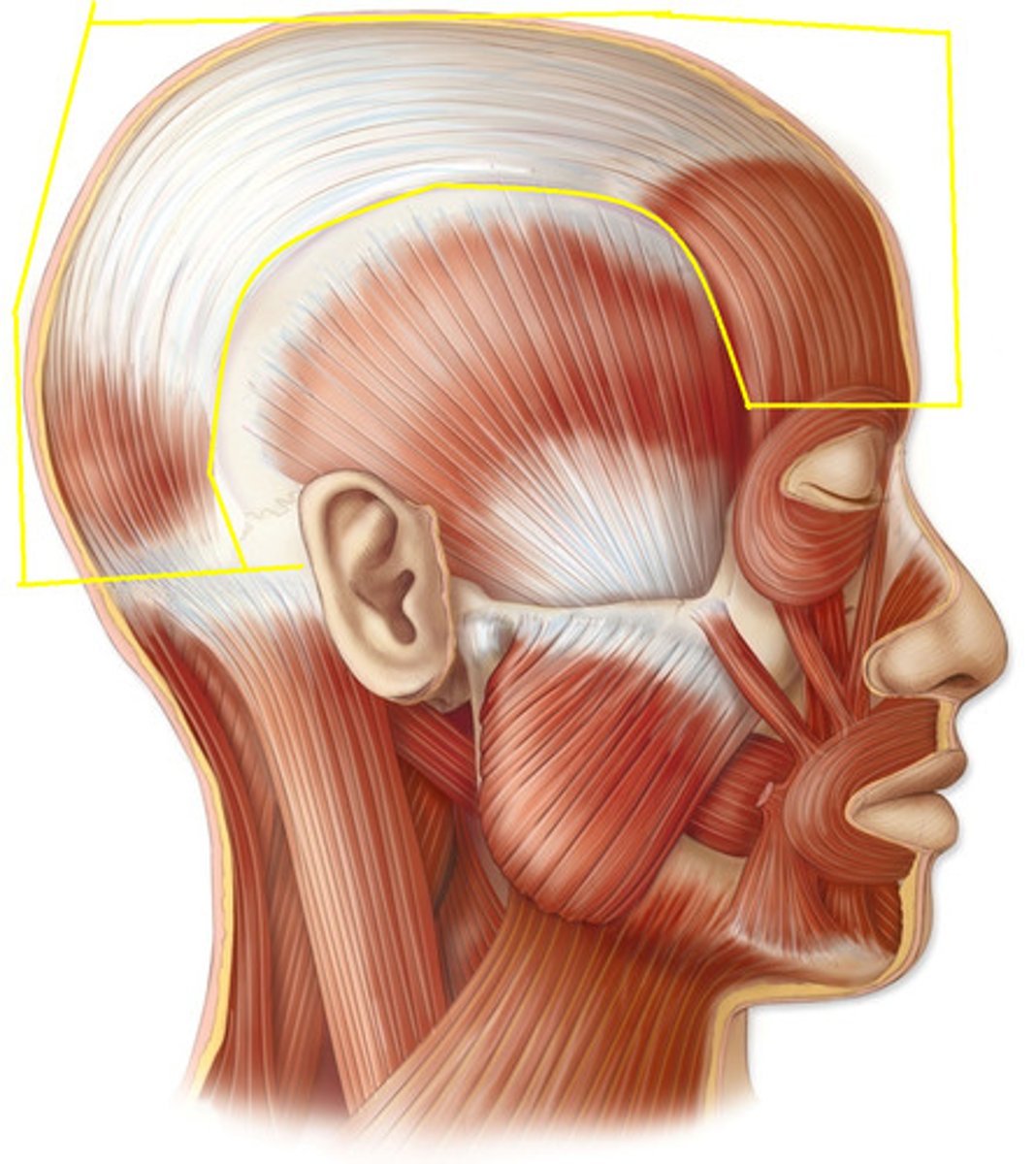
5 layers of scalp
Skin
Connective tissue
Aponeurosis
Loose areolar tissue
Pericranium
skin of scalp
thin
highly vascularized
(sebaceous glads)
connective tissue of scalp
thick and dense
dense connective tissue
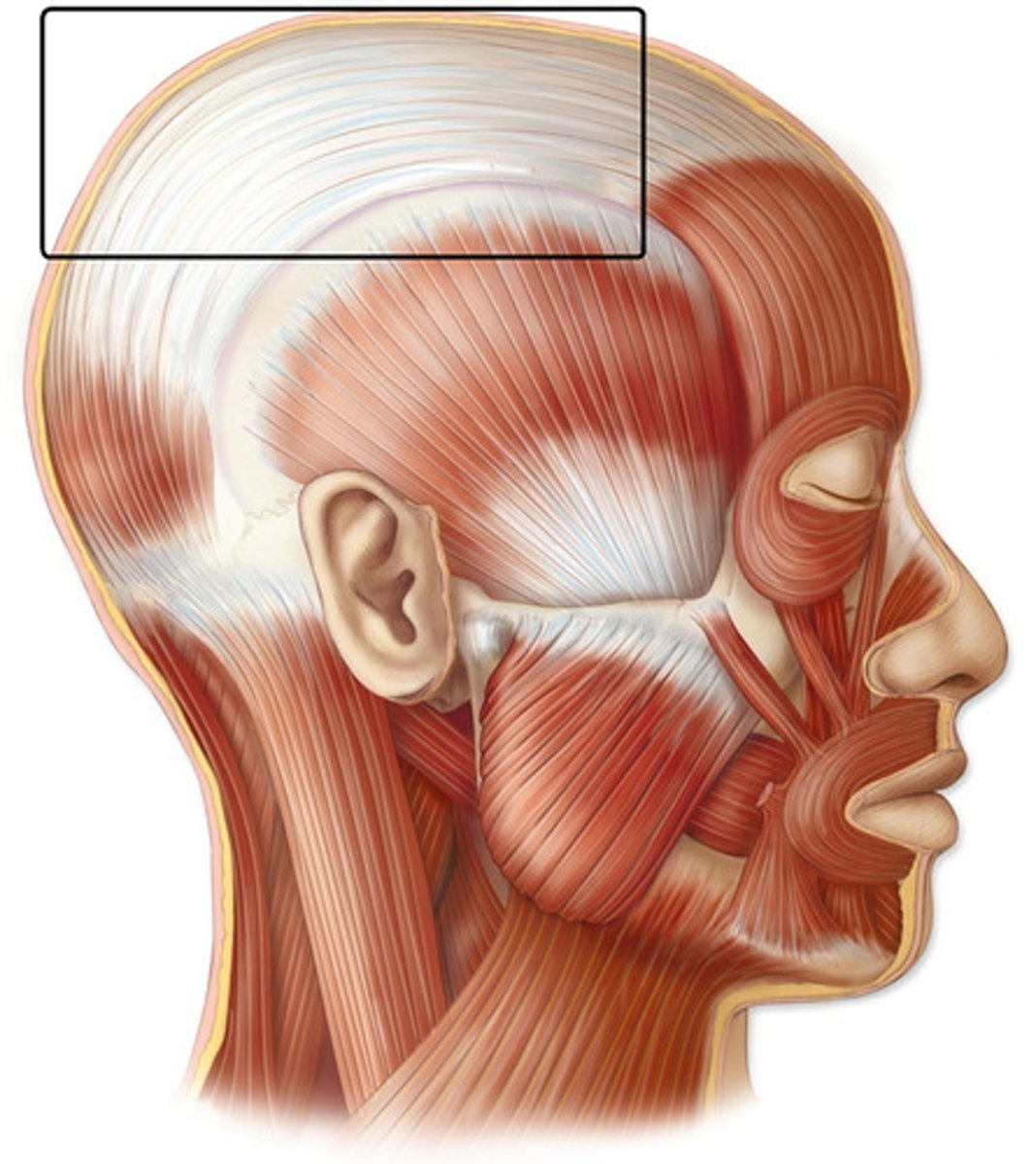
Aponeurosis of scalp
epicranial aponeurosis
thickening of connective tissue, flattened tendon/fascia sheath
Loose areolar tissue of scalp
loose and allows for free movement of skin on scalp
Pericranium of scalp
Attached to bone itself (periosteum)
Temporomandibular (TMJ) Joint
Modified hinge—synovial
Mandibular elevation
Mandibular depression
Mandibular protrusion/retrusion
Mandibular dislocation
what is the articulation of the TMJ
condyloid process of the mandible articulates with the mandibular fossa of the temporal bone
Elevation TMJ Muscles
this is closing mouth:
temporalis
masseter
med. pterygoid
Depression TMJ muscles
this is opening mouth:
lateral pterygoids
infrahyoid
mylohyoid
GRAVITY is primary mover (sleeping in car and mouth drops open)
protrusion TMJ muscles
masseter
med and lat pterygoids
retrusion TMJ muscles
temporalis-main one
masseter
lateral movements TMJ muscles
temporalis of the same side
pterygoid of the opposite side
Vascular Supply of the face
supra/infra orbital
facial
maxillary
lingual
temporal
occipital
what is special about the vasculature of the nasal cavity
highly vascular nature of the nasal cavity
Venous Drainage and arteries of face
supra/infra orbital
facial
maxillary
lingual
temporal
occipital
Facial veins drainage
-the primary drainage of the face
-joins with the retromandibular v (anterior division) to
empty into the internal jugular v in the neck
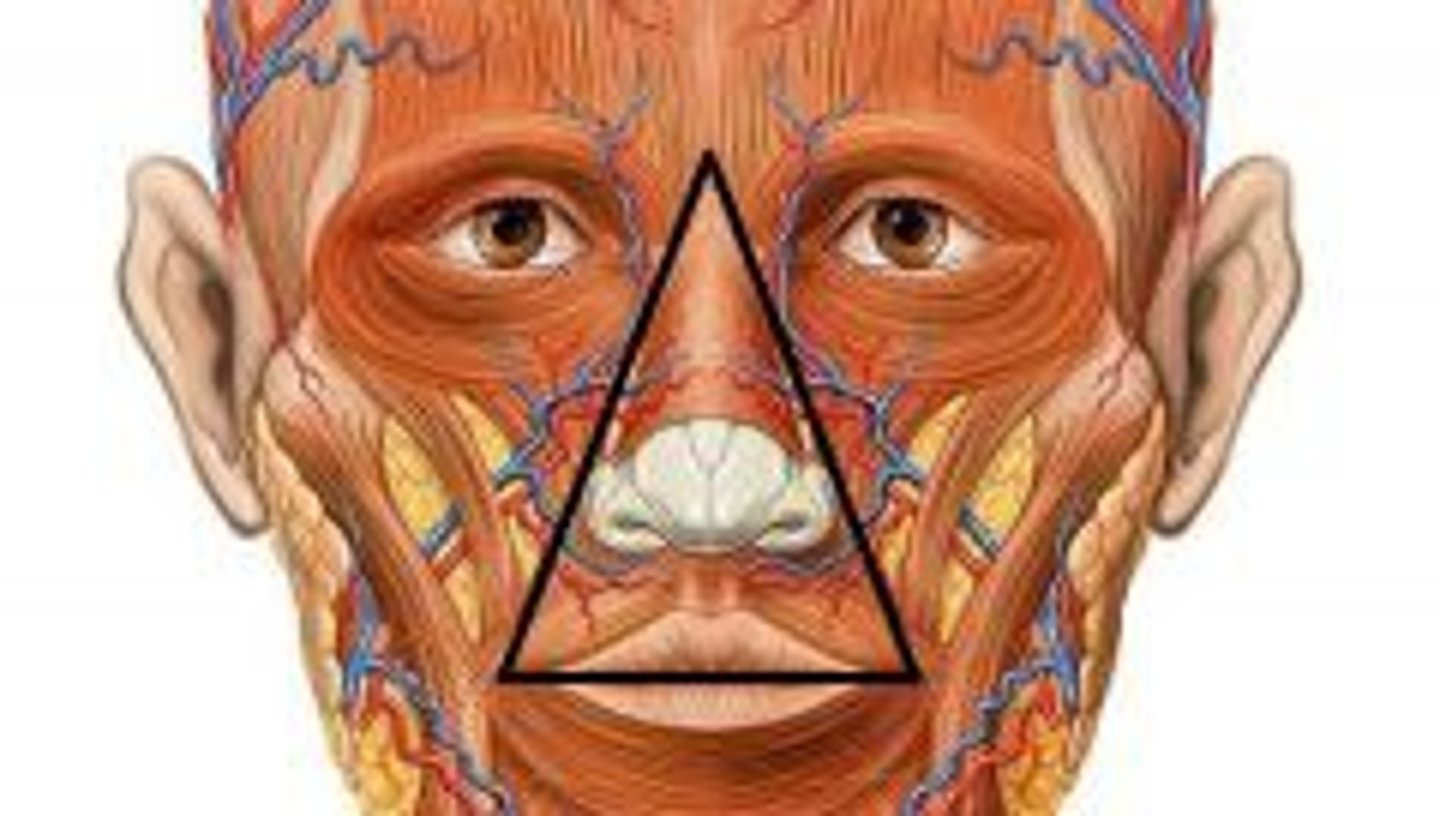
Danger Triangle
⚫ Margins:
⚫ Why "Danger"???
bridge of nose to upper lip
highly vascular supply meaning easier to spread infection
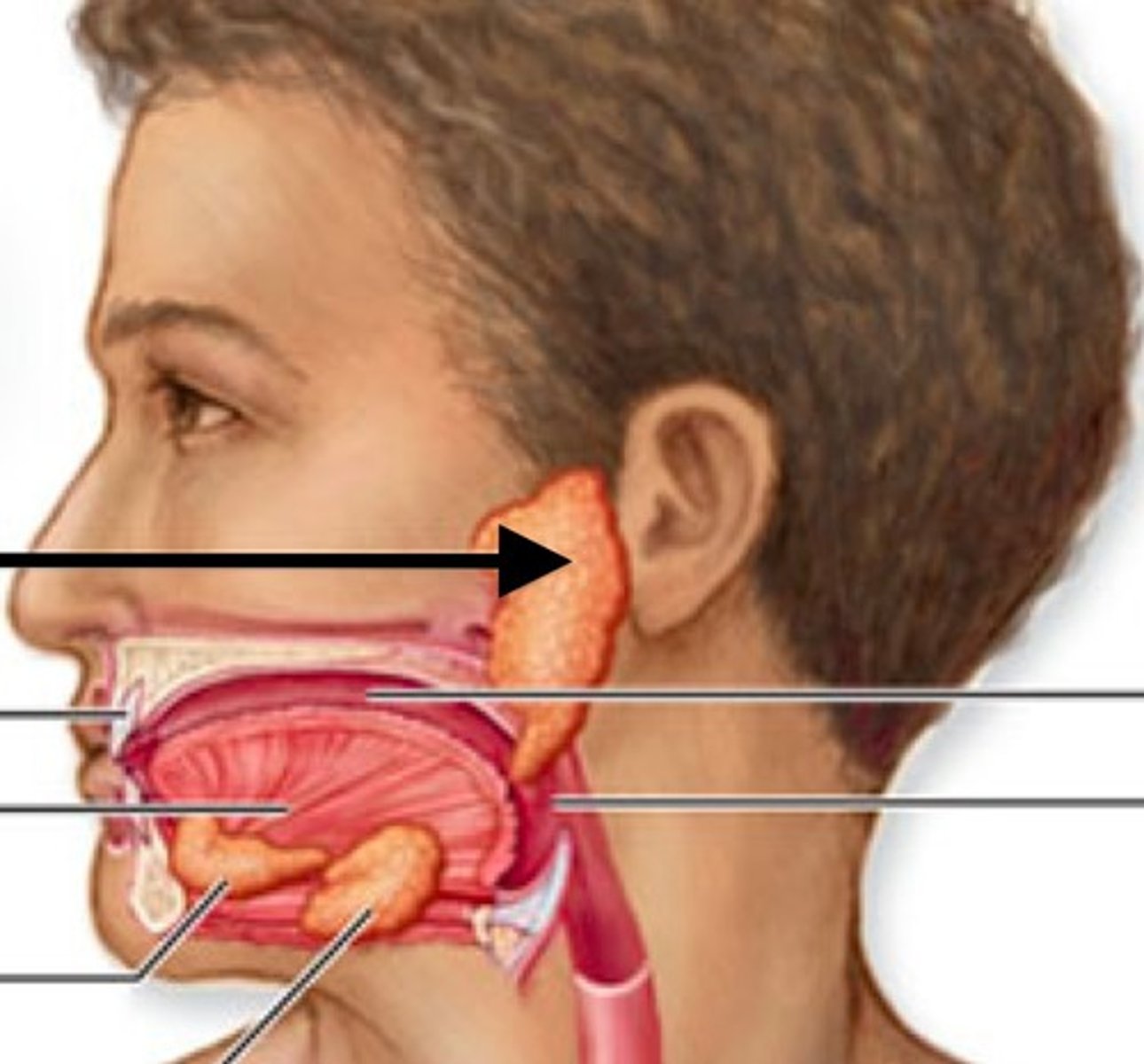
Salivary Glands
3 paired:
parotid, sublingual, and submandibular glands
Parotid Gland
Largest
Clinically important: many structures pass through or are associated with it
- ex. Facial nerve branches all pierce it
Location - "sandwiched" between: mandibular rami and the mastoid process of temporal bone
Childhood Disease with parotid gland
mumps
- unilateral or bilateral

Muscles of Facial Expression innervation
All innervated by the facial nerve (CN VII)
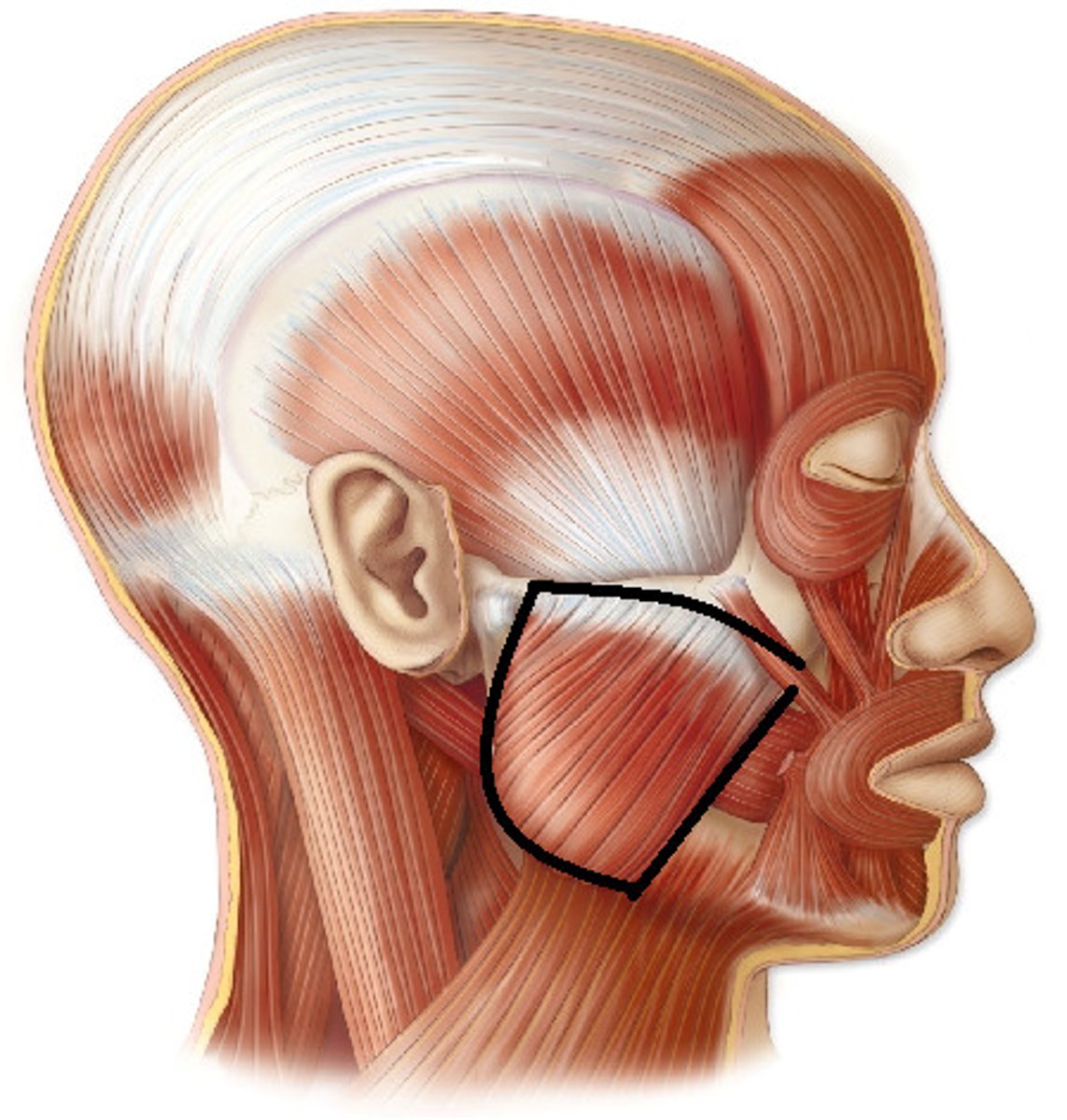
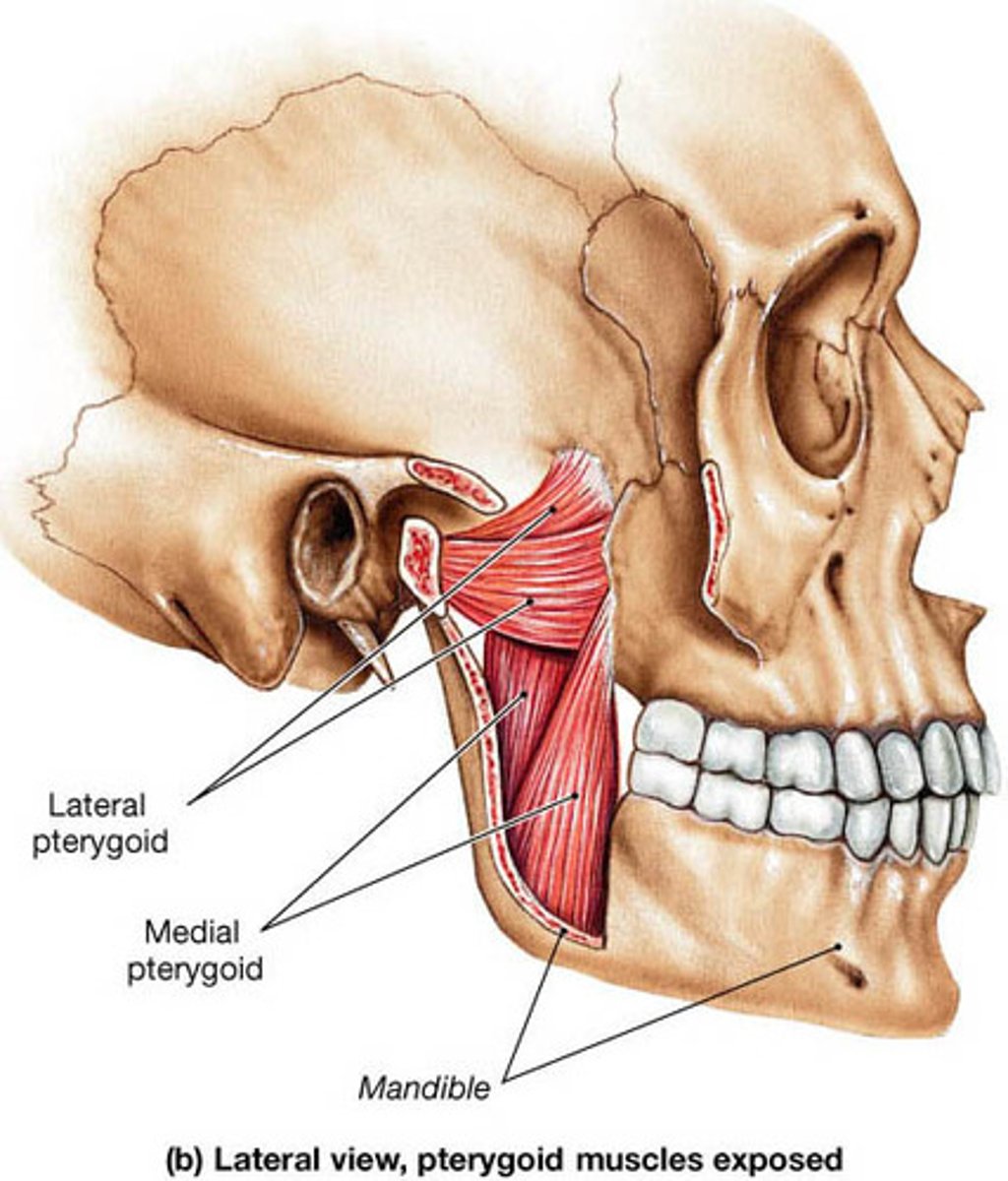
muscles of mastication
masseter, temporalis, medial and lateral pterygoids
Origin and insertion of masseter
Origin: zygomatic arch
Insertion: mandible
action: elevate, protract, and retract mandible
innervation: trigeminal, V3
Origin and insertion of temporalis
origin: temporal fossa
insertion: mandible
action: elevate and retract mandible
innervation: All trigeminal, V3

Origin and insertion of medial pterygoid
origin: pterygoid plate
insertion: mandible
action: elevate and protract mandible, and lateral movement of opposite side of mandible
innervation: All trigeminal, V3
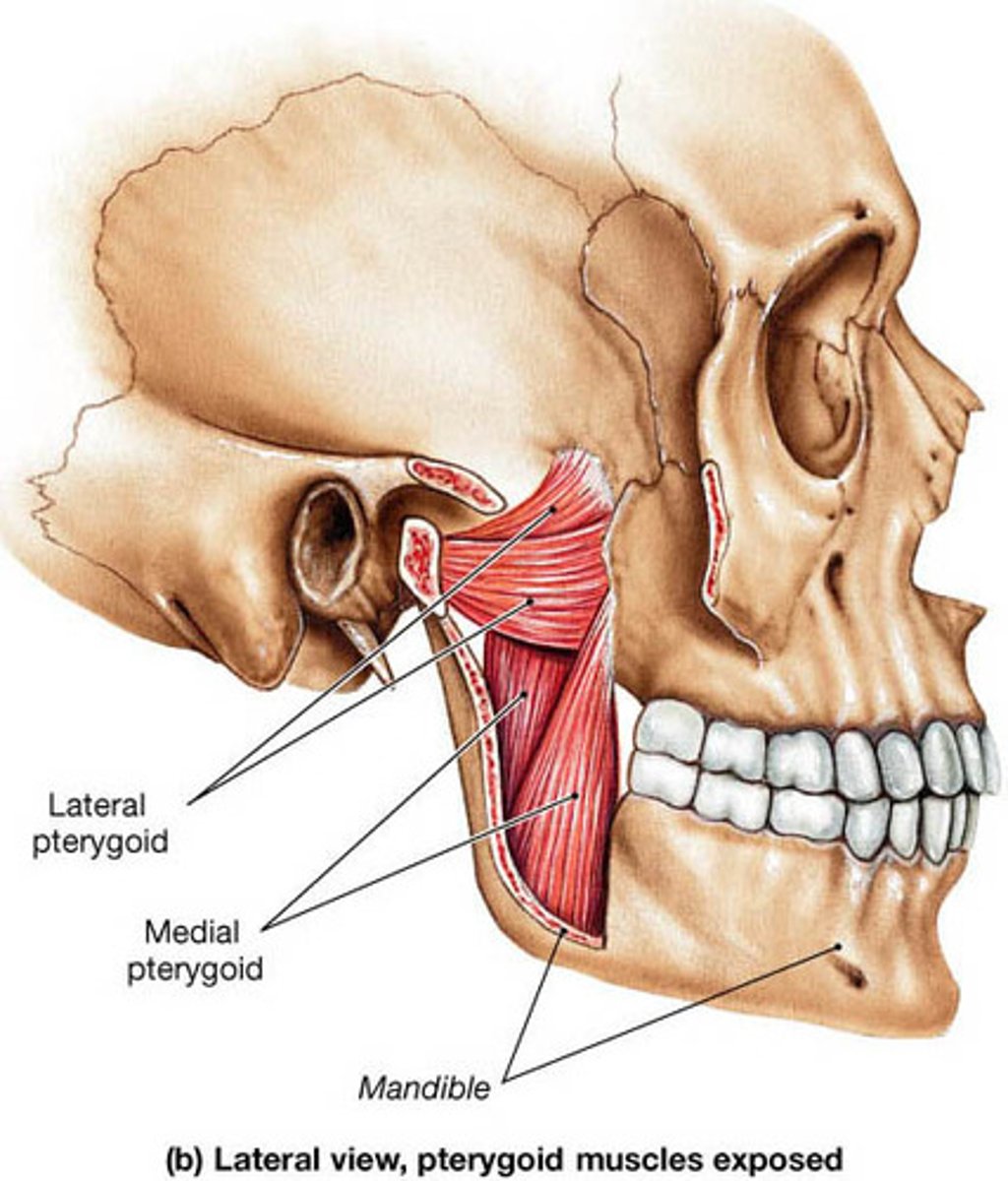
Origin and insertion of lateral pterygoid
origin: pterygoid plate
insertion: mandible
action: depress and protract mandible, and lateral movement of opposite side of mandible
innervation: All trigeminal, V3
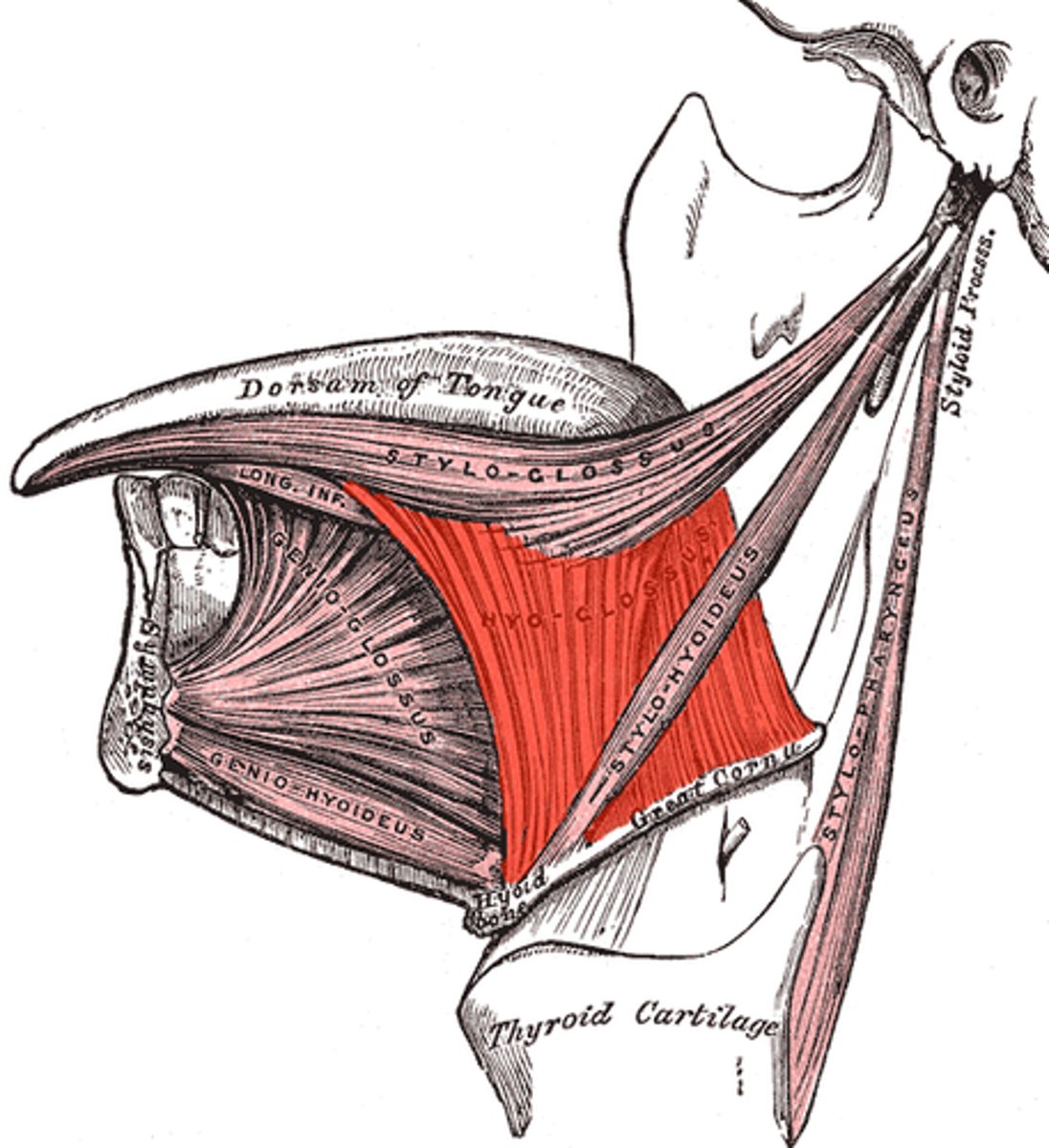
extrinsic muscles of tongue
Genioglossus
Hyoglossus
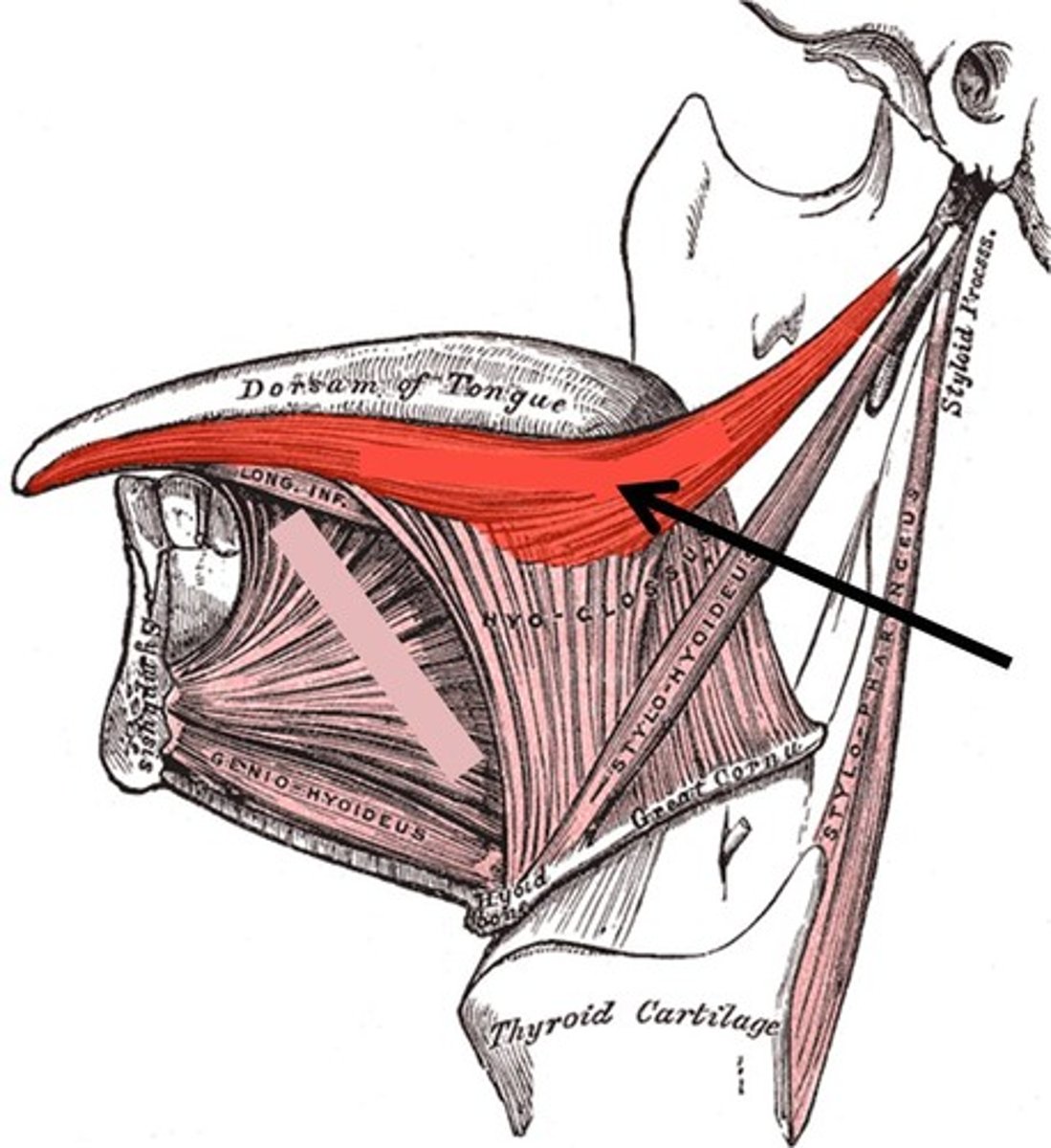
Styloglossus
Palatoglossus
action of genioglossus
action: depresses and protrudes tongue
innervation: CN XII (hypoglossal)
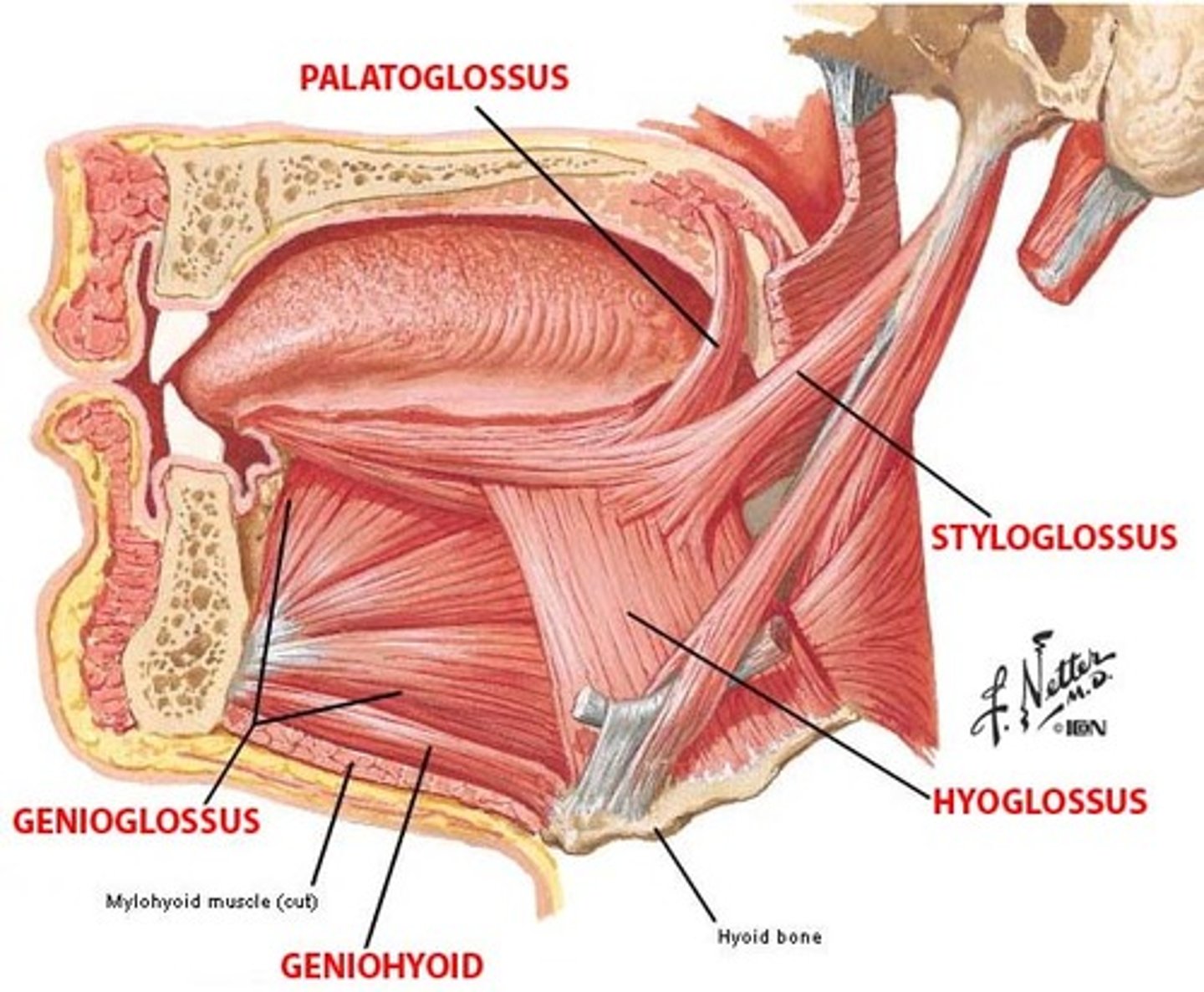
action of hyoglossus/hyoglossal
depresses tongue
innervation: CN XII (hypoglossal)
action of styloglossus/styloglossal
retrude and curls the tongue
innervation: CN XII (hypoglossal)
action of palatoglossus/palatoglossal
elevates posterior tongue to palate
innervation: CN X (Vagus)
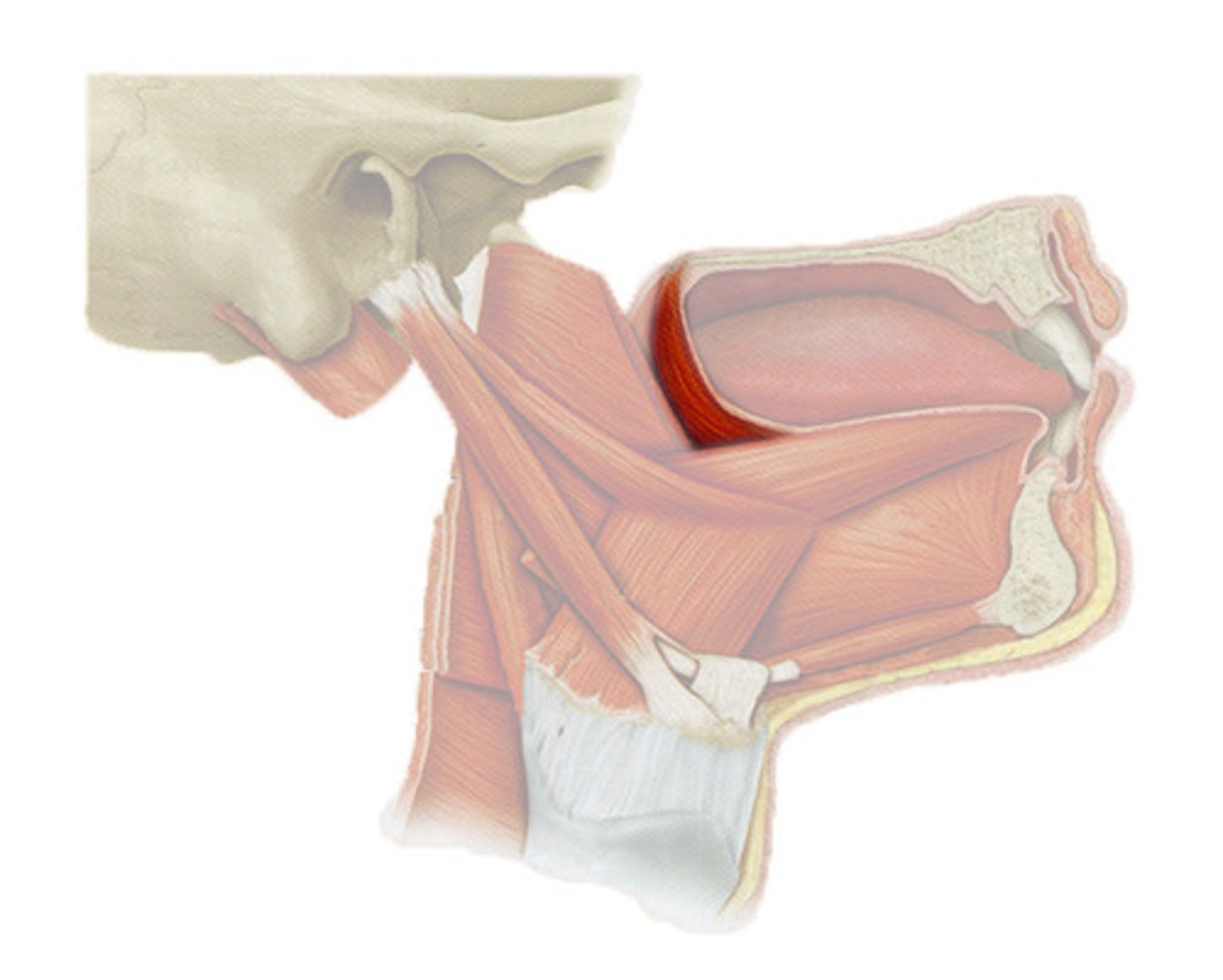
intrinsic & extrinsic tongue muscles
Extrinsic - originate outside of the tongue and insert on the tongue
intrinsic = Origin and insert within tongue
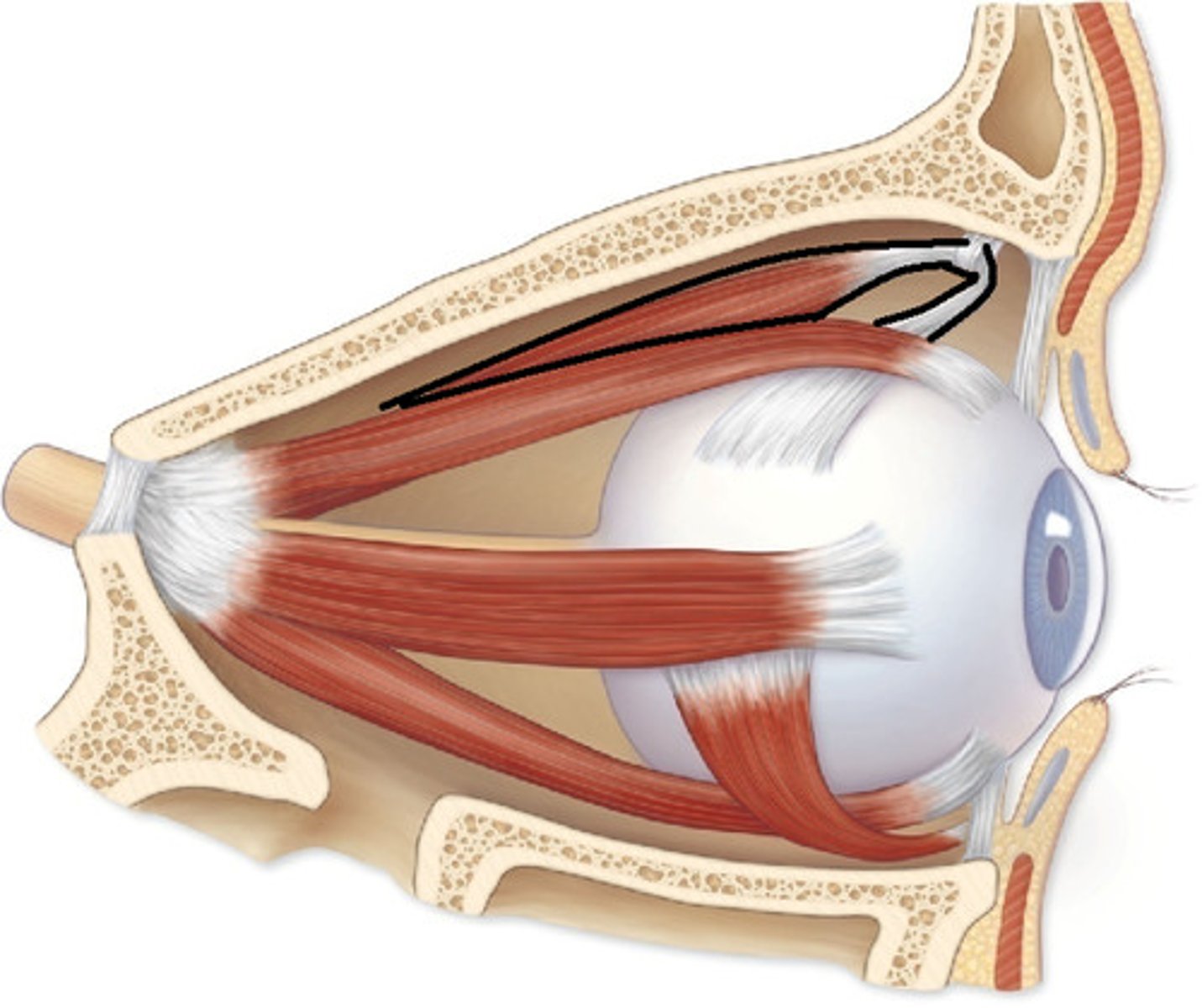
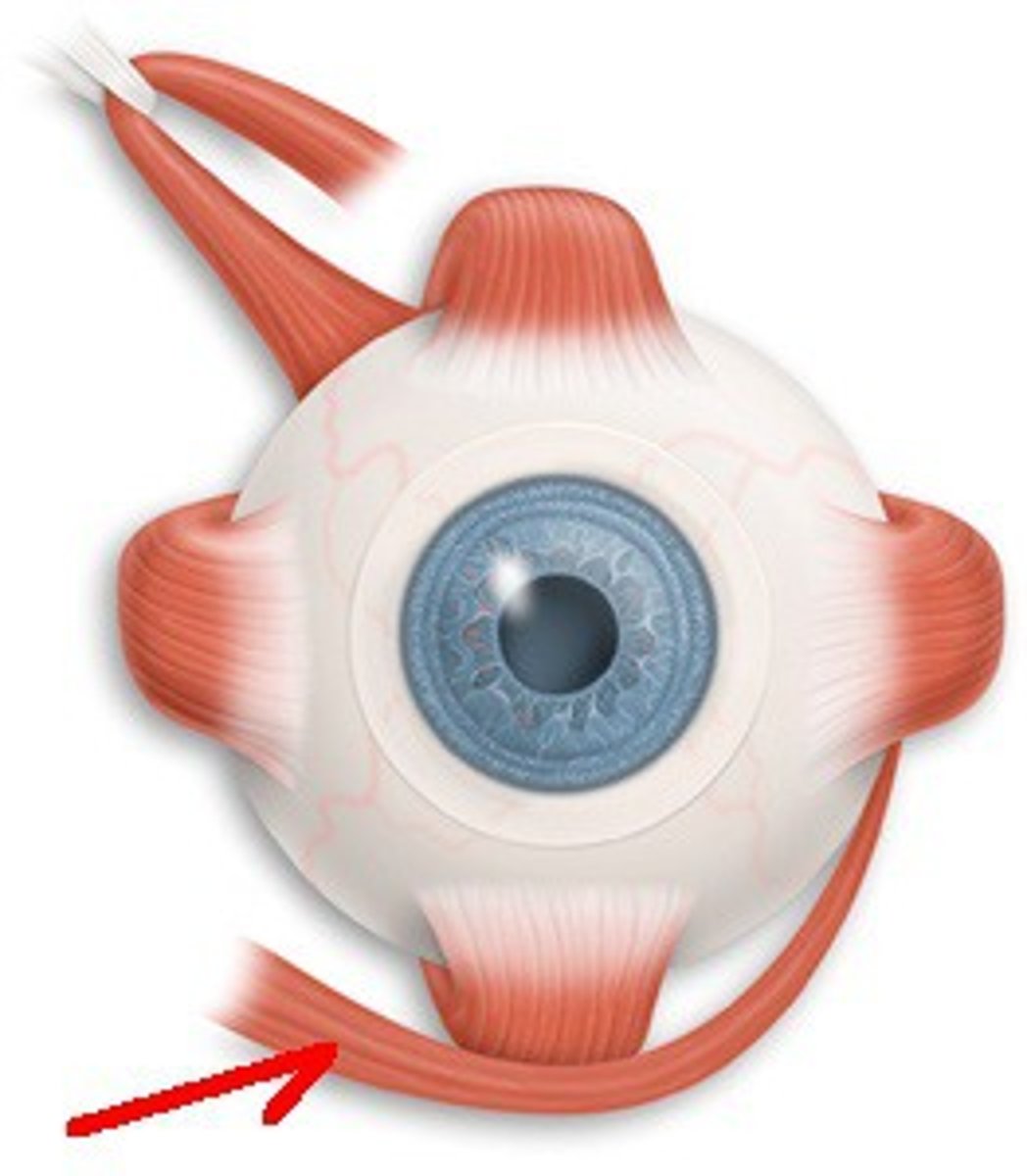
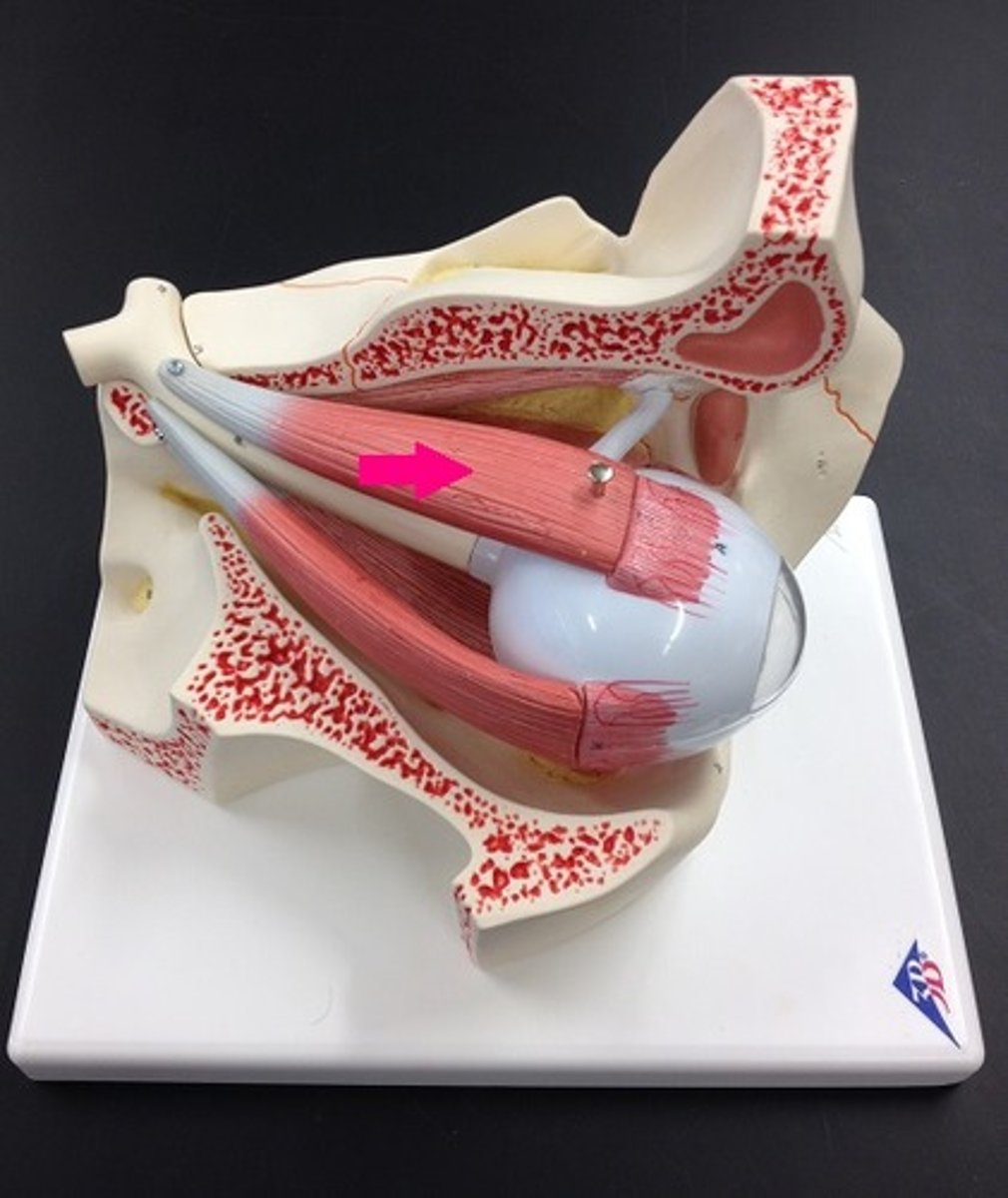
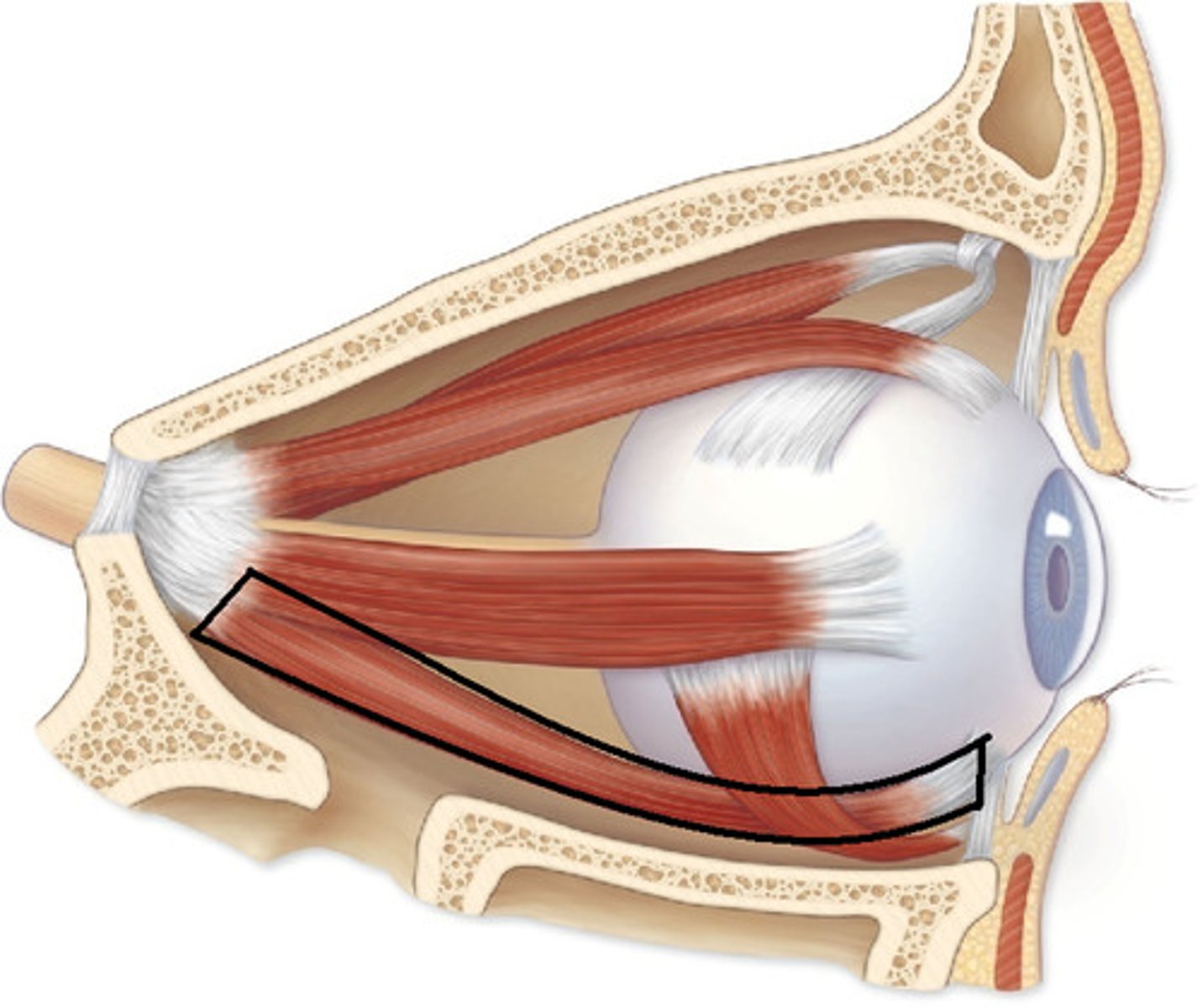
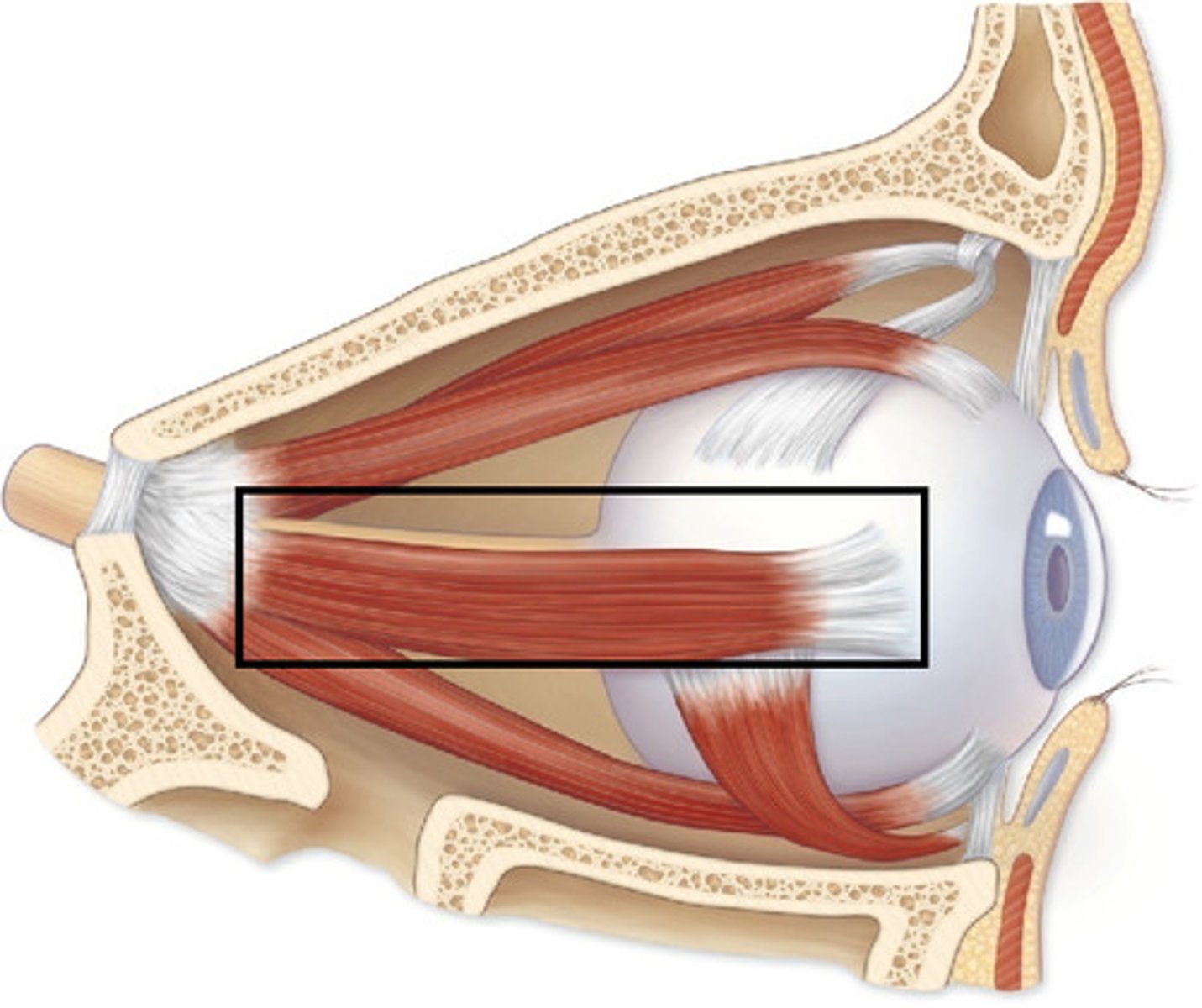
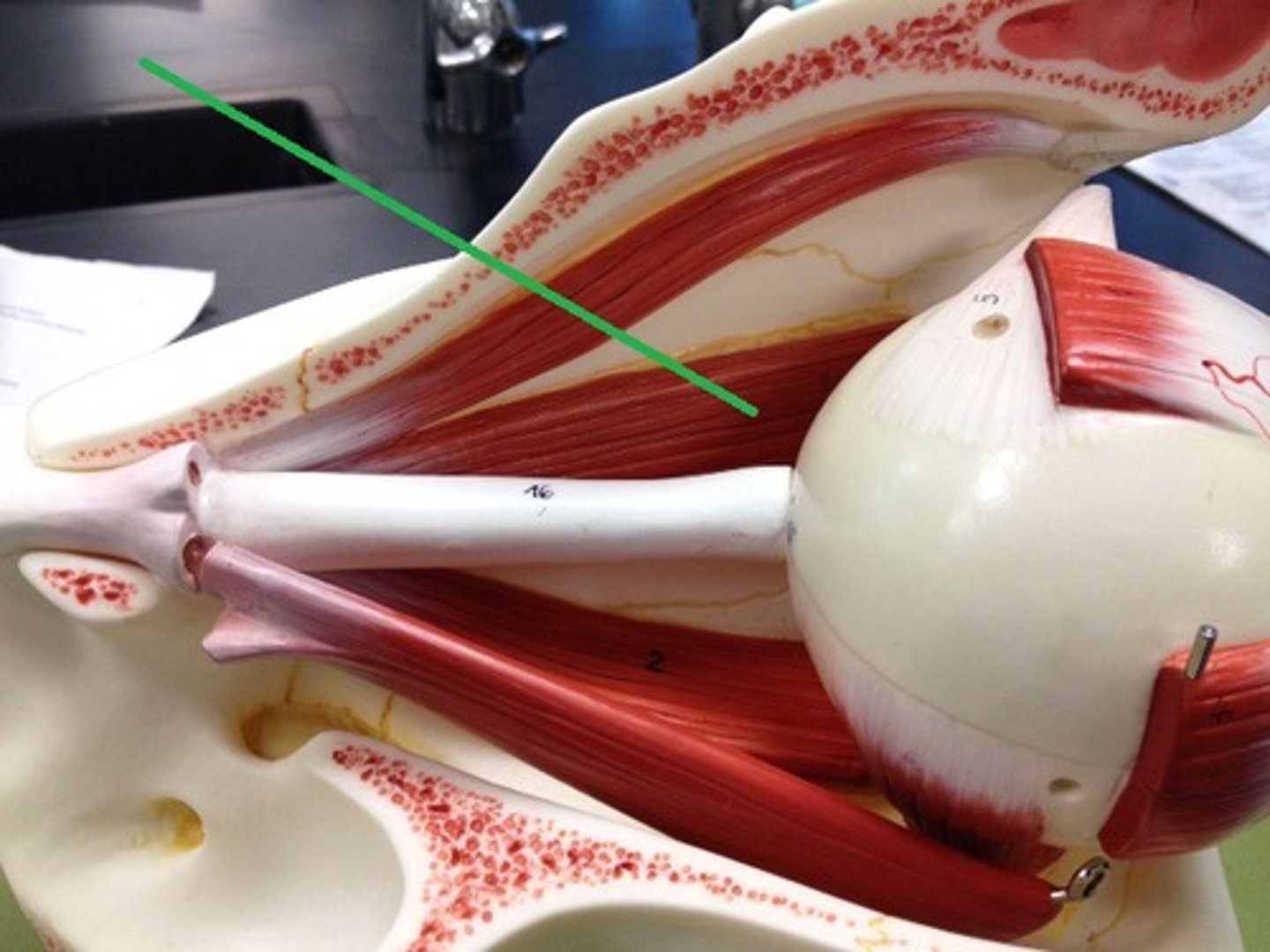
Extraocular Eye Muscles
superior rectus, inferior rectus, lateral rectus, medial rectus, superior oblique, inferior oblique
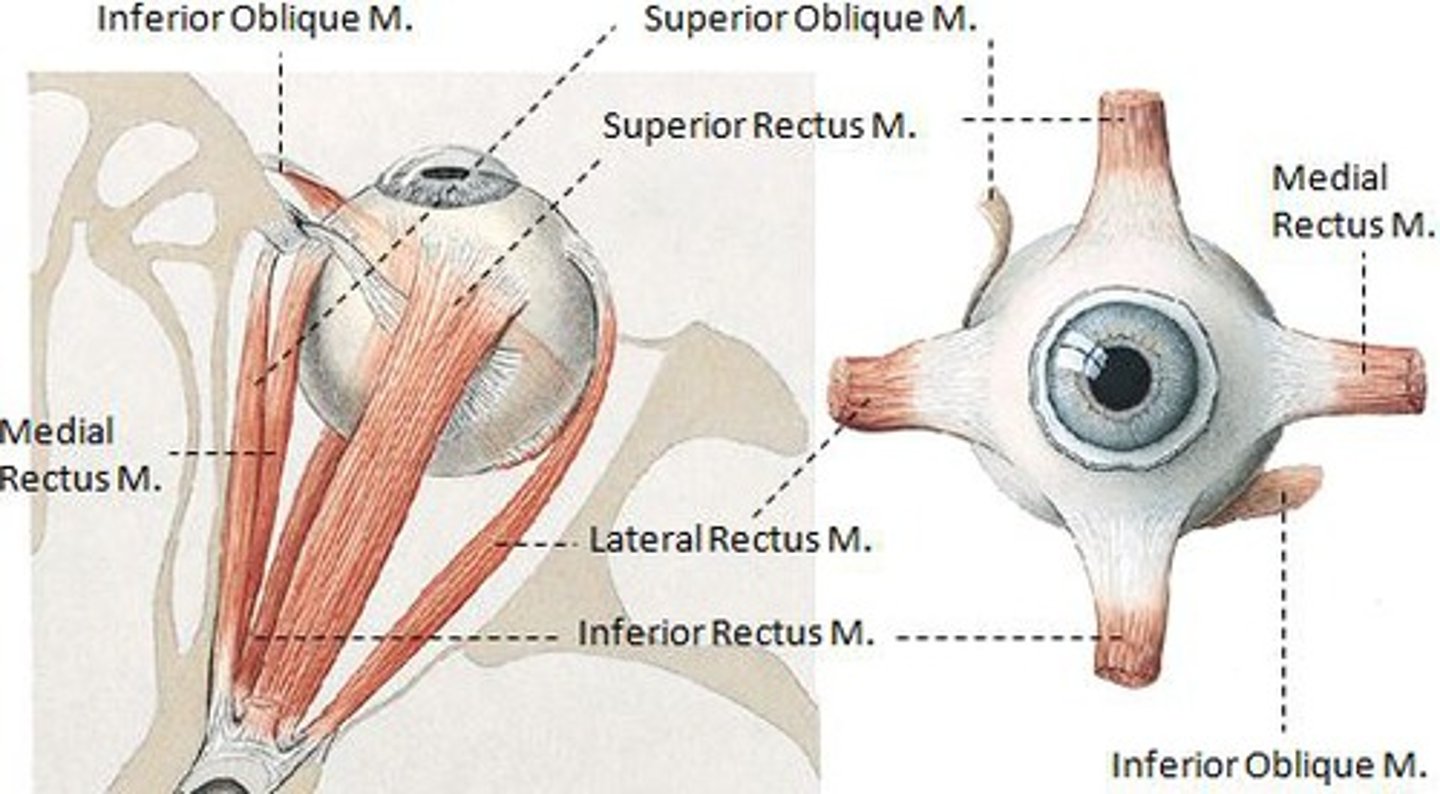
Innervation of EOM
[LR6(SO4)]3
![<p>[LR6(SO4)]3</p>](https://knowt-user-attachments.s3.amazonaws.com/2b55e03c-31de-475b-a0cc-743bce8dfcf1.jpg)
Superior oblique
Depresses eye and turns it laterally
CN IV (trochlear)
Inferior oblique
Elevates eye and turns it laterally
III (oculomotor)
Superior rectus
elevates eye; III oculomotor
inferior rectus
depresses eye; III oculomotor
lateral rectus
moves eye laterally (VI abducens)
medial rectus
moves eye medially (III oculomotor)
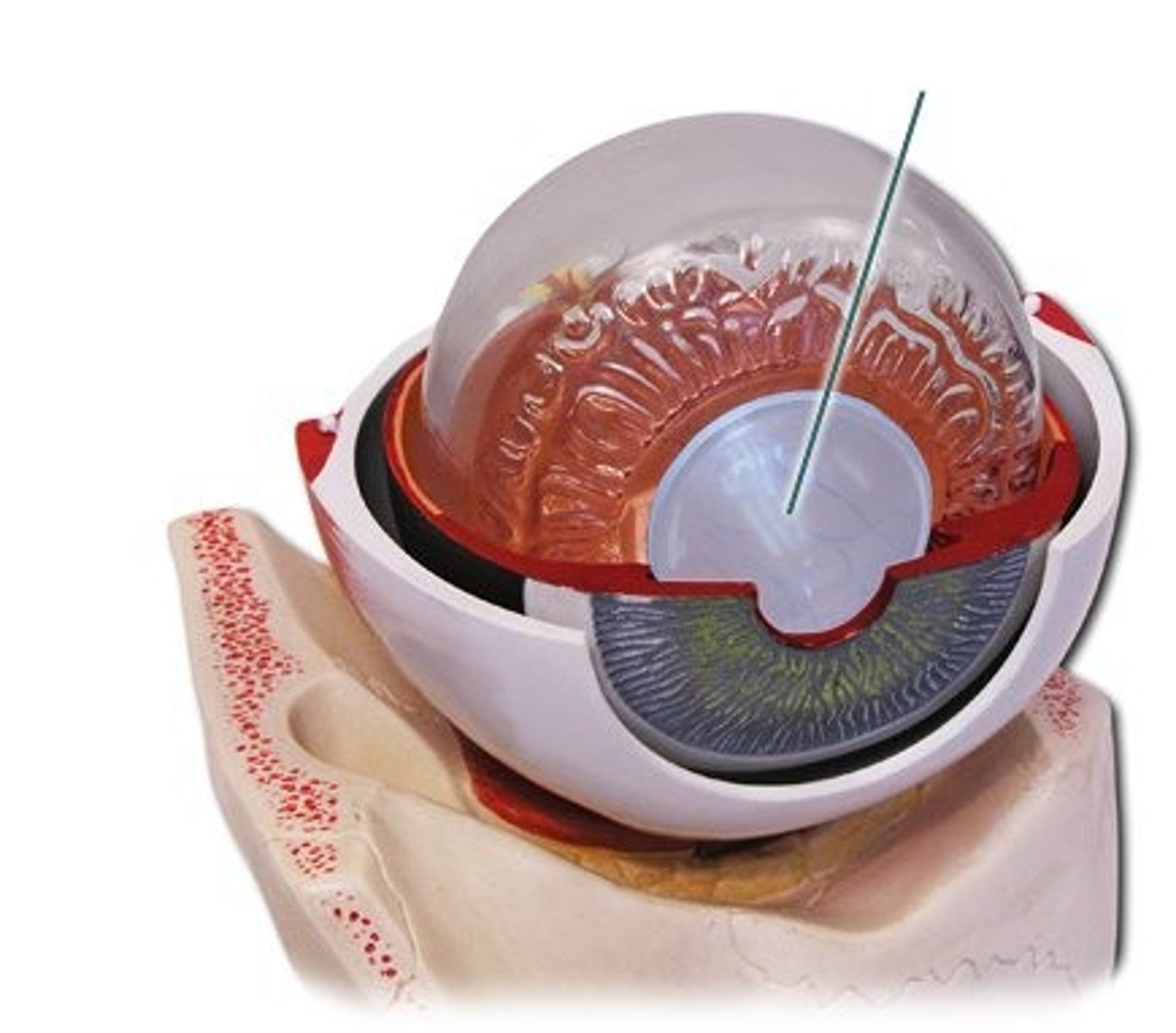
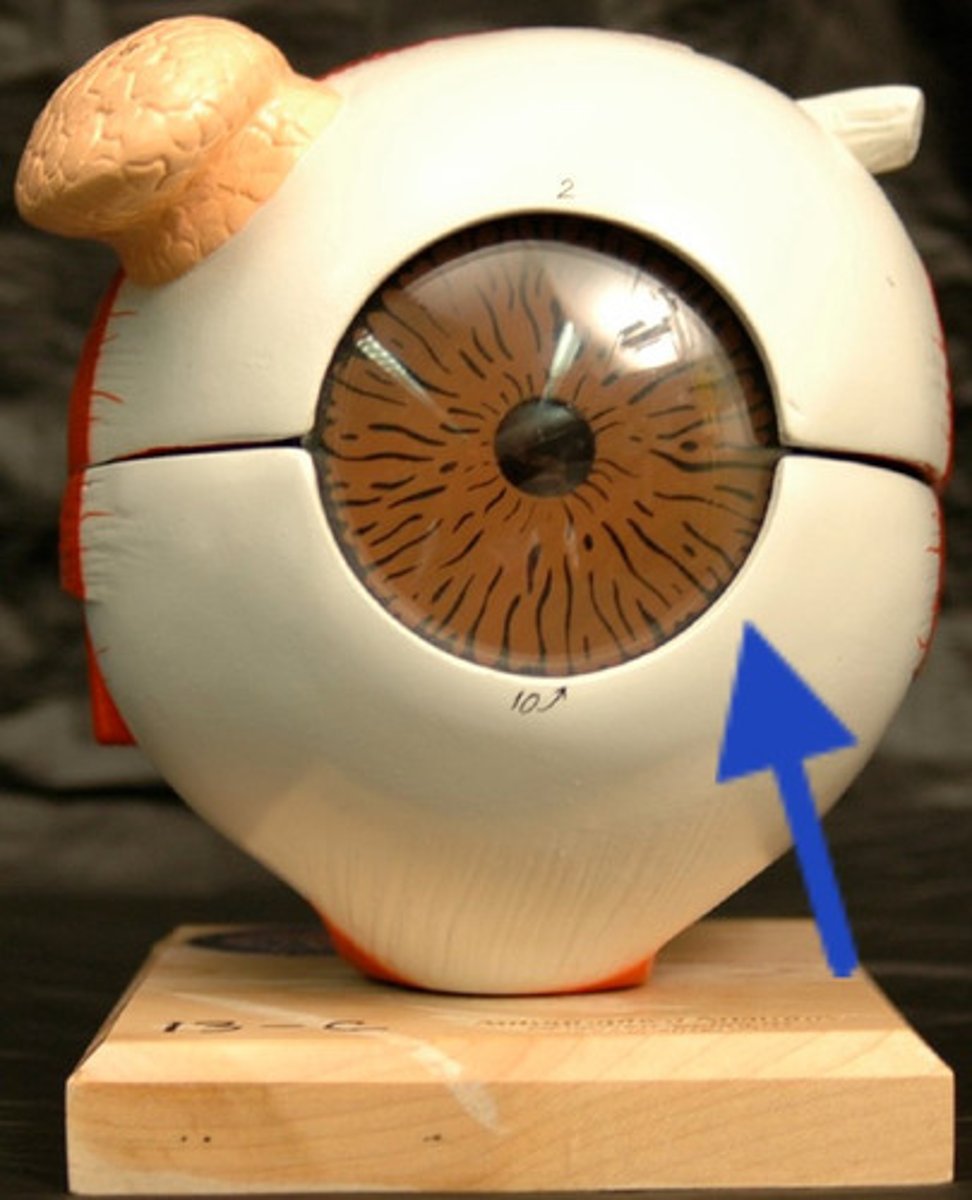
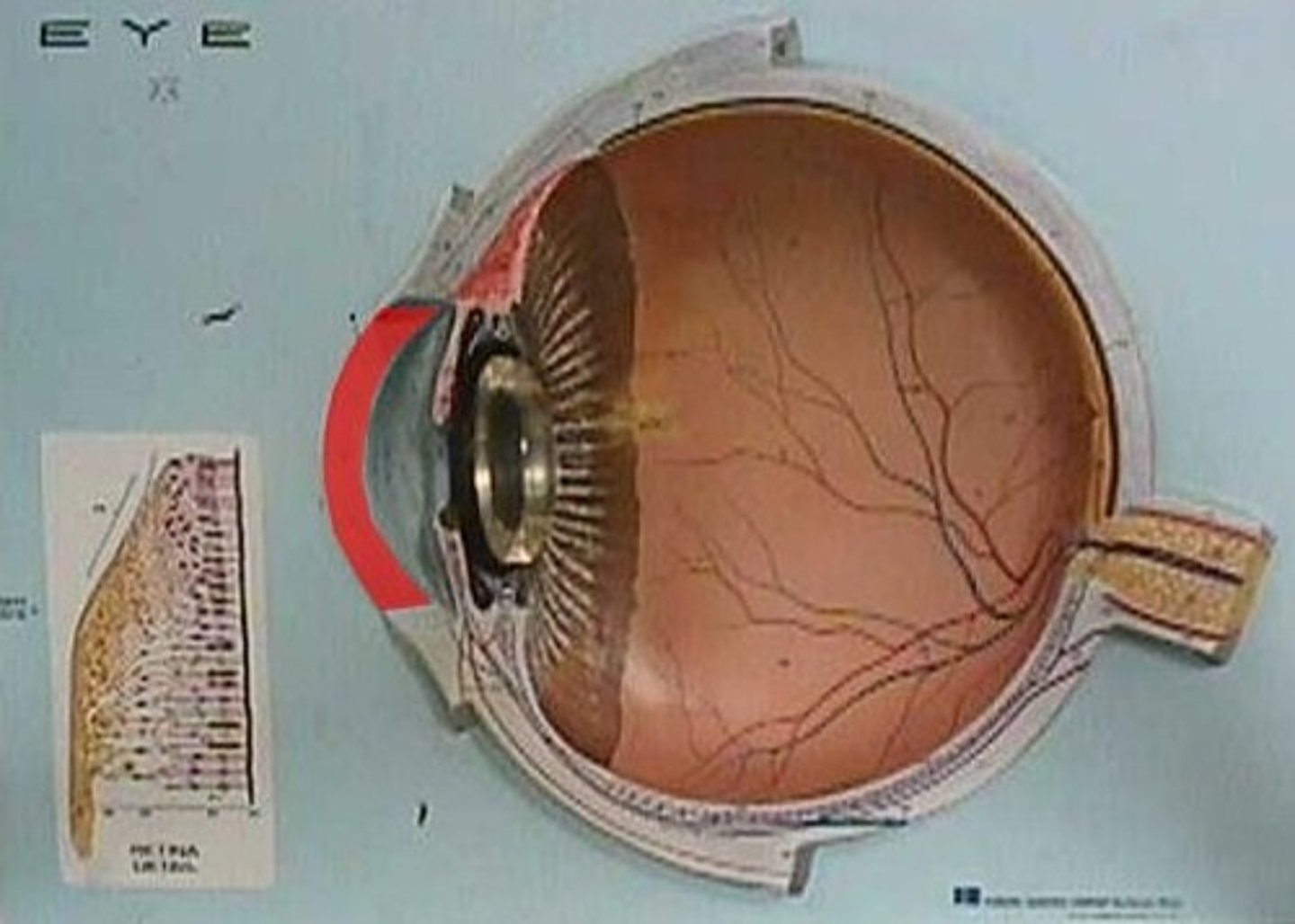
Sclera
white of the eye
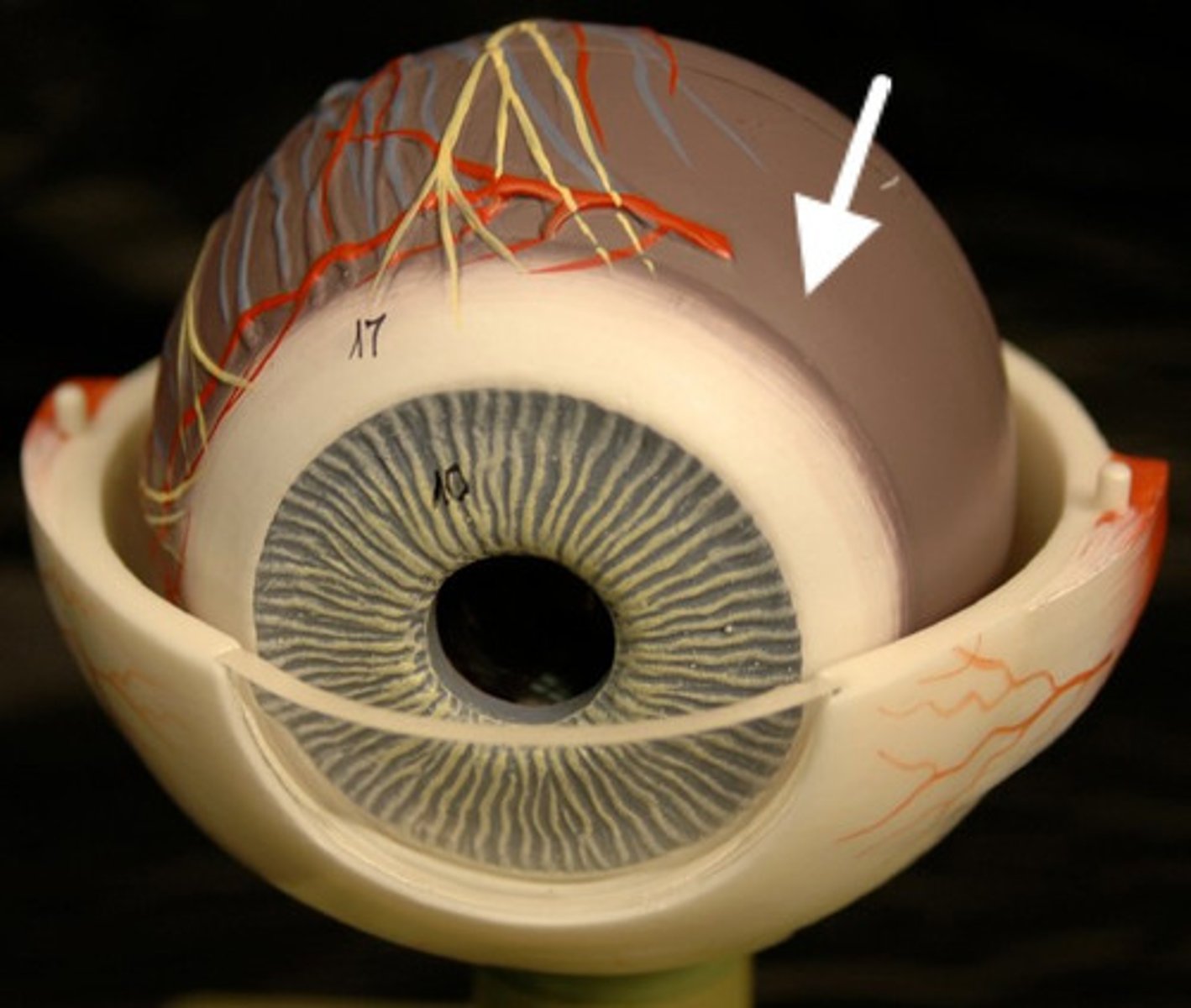
choroid
middle, vascular layer of the eye, between the retina and the sclera
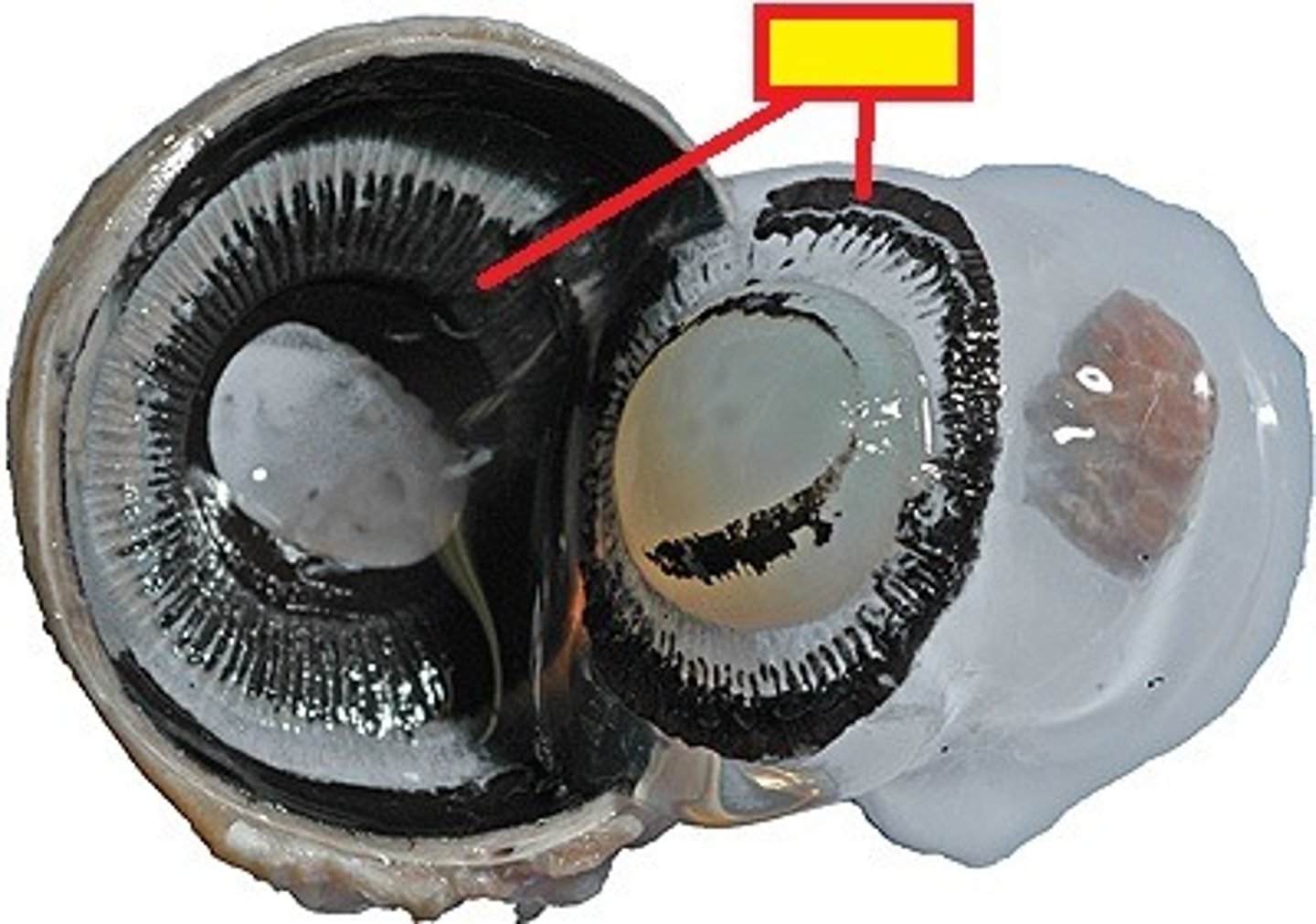
retina
the light-sensitive inner surface of the eye, containing the receptor rods and cones plus layers of neurons that begin the processing of visual information
macula lutea
a yellowish central area of the retina that is rich in cones and that mediates clear detailed vision
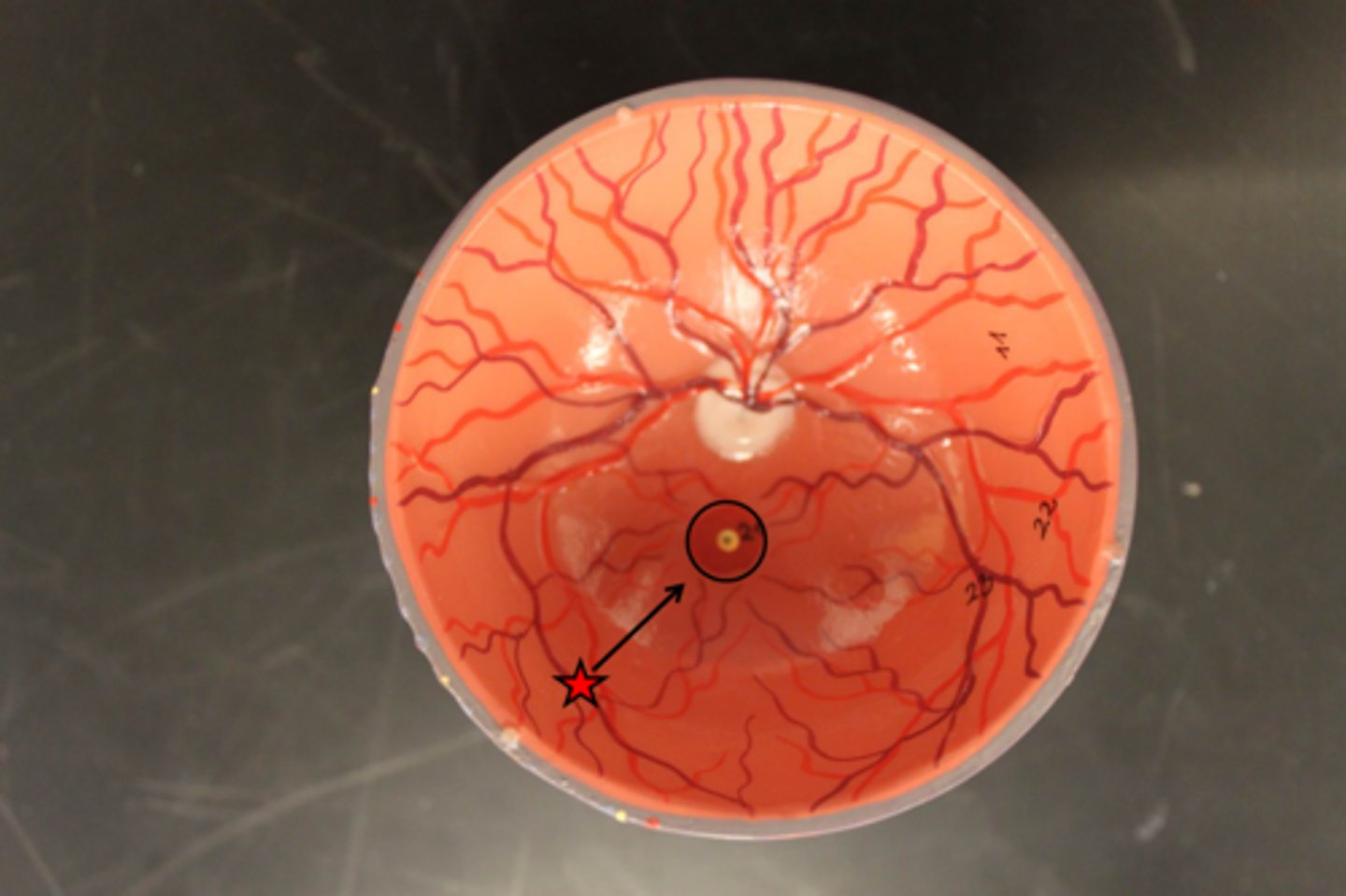
fovea centralis
tiny pit or depression in the retina that is the region of clearest vision
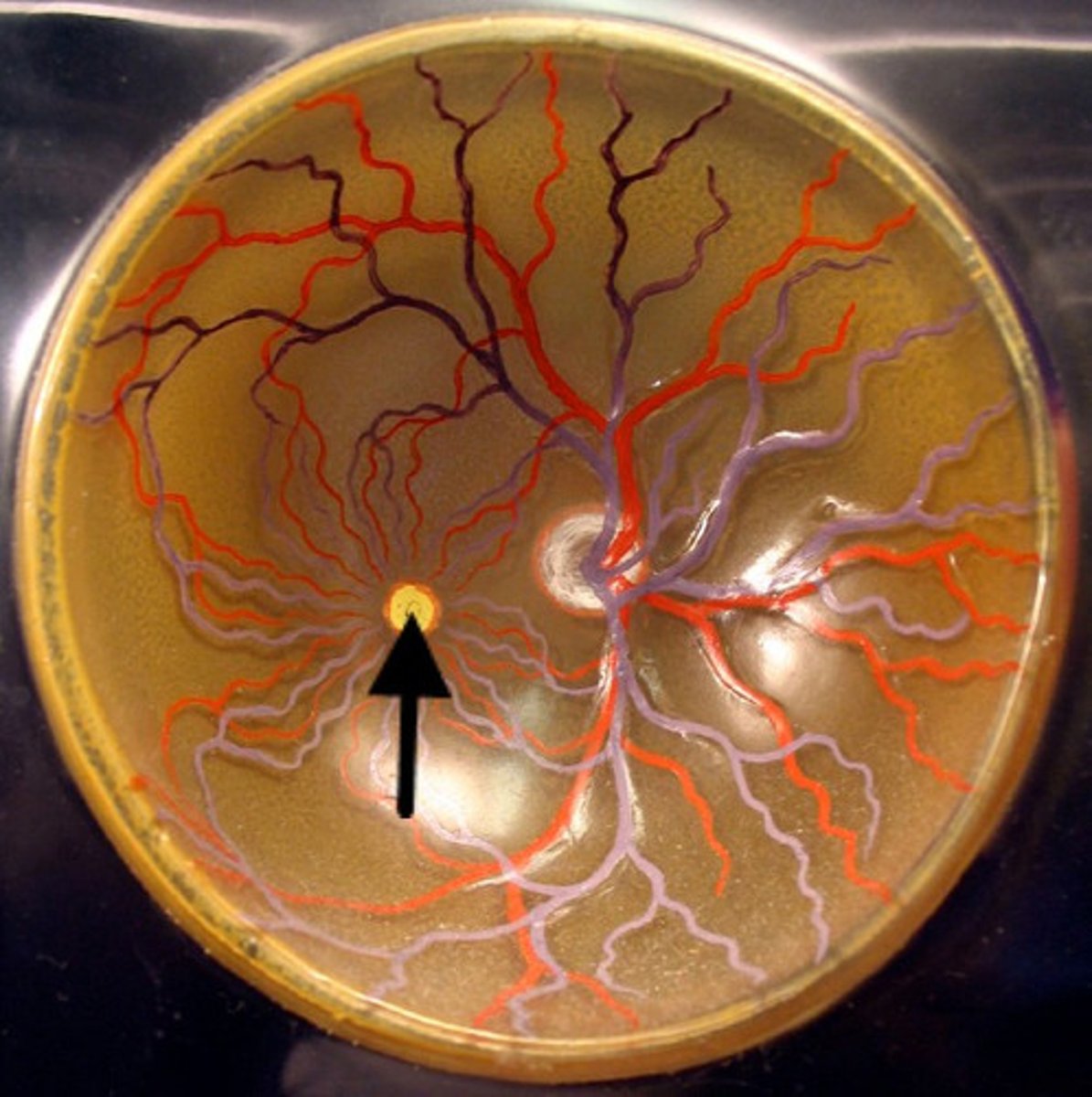
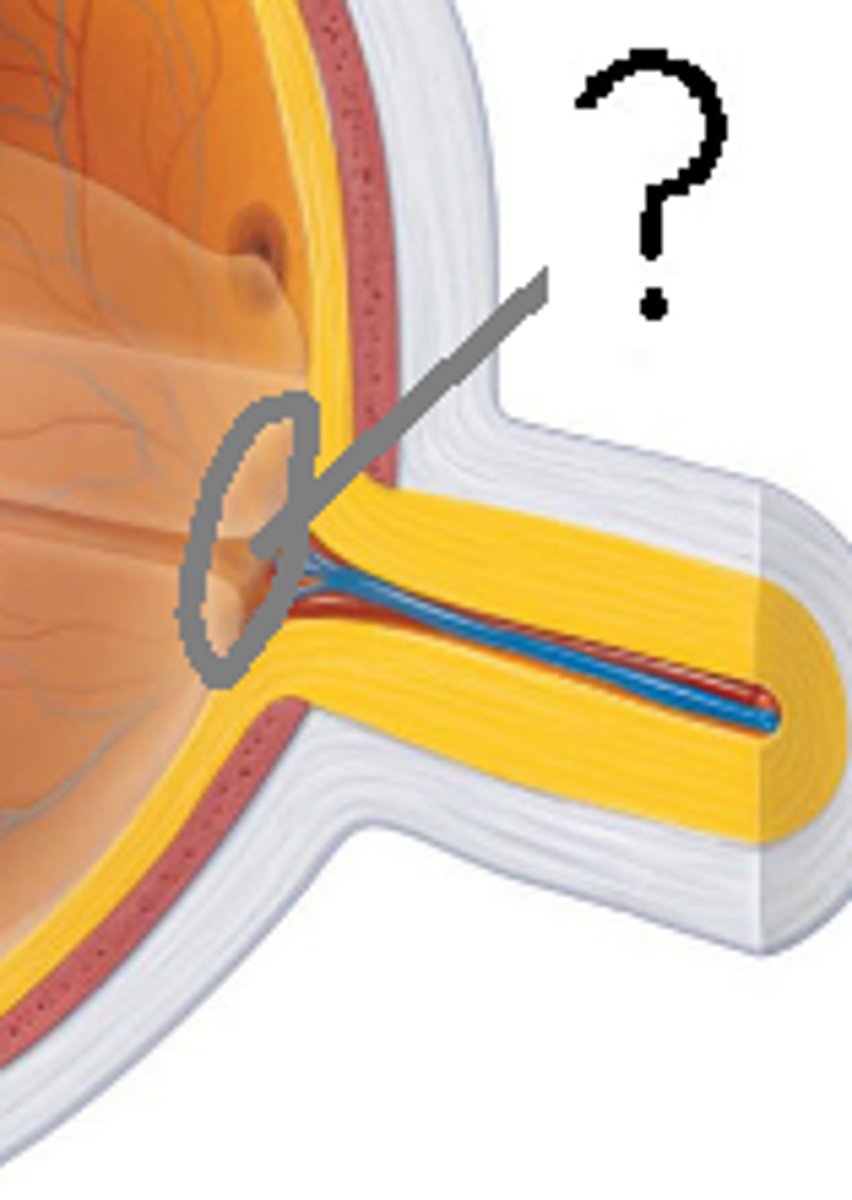
optic disc
Region at the back of the eye where the optic nerve meets the retina. It is the blind spot of the eye because it contains only nerve fibers, no rods or cones, and is thus insensitive to light.
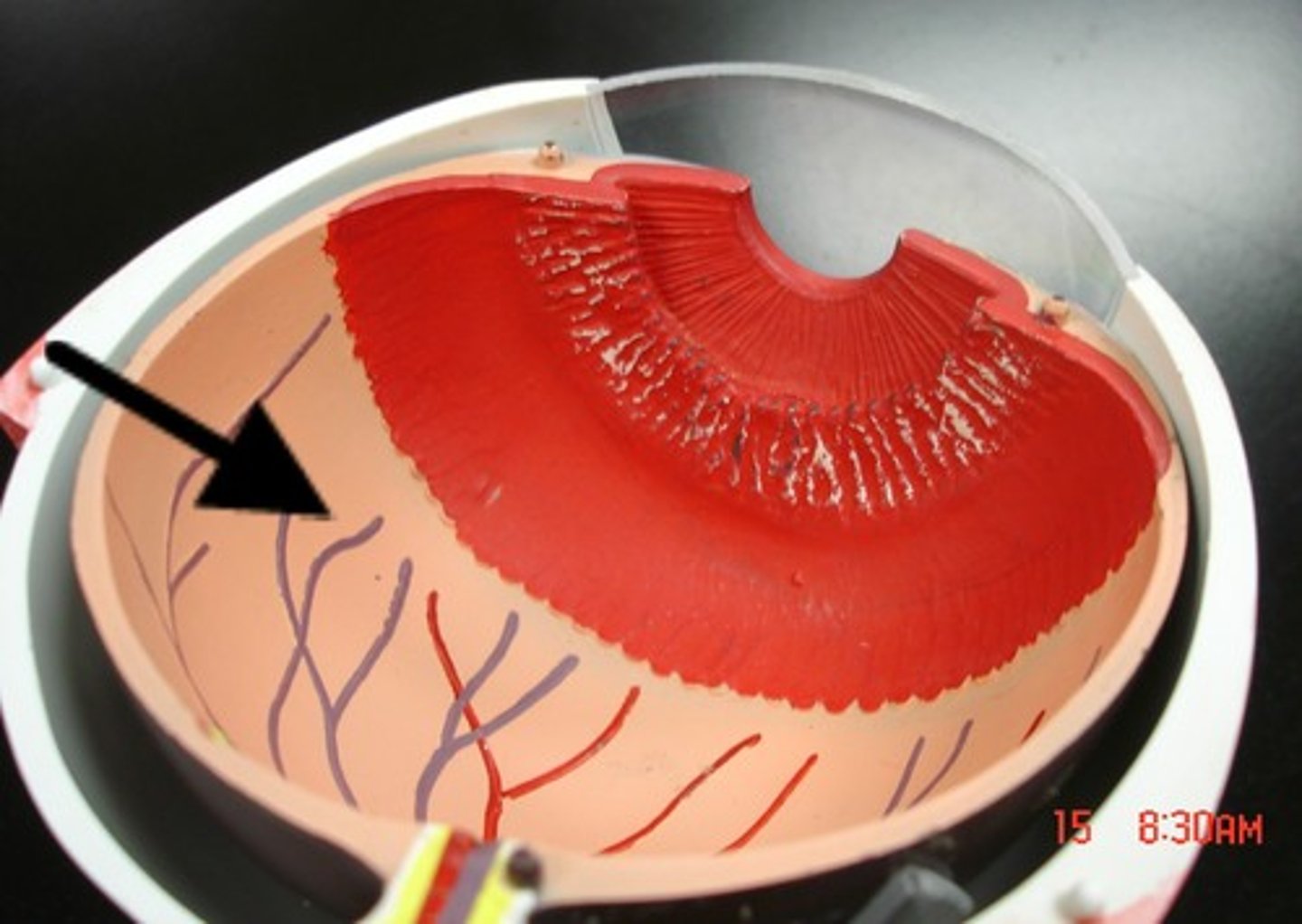
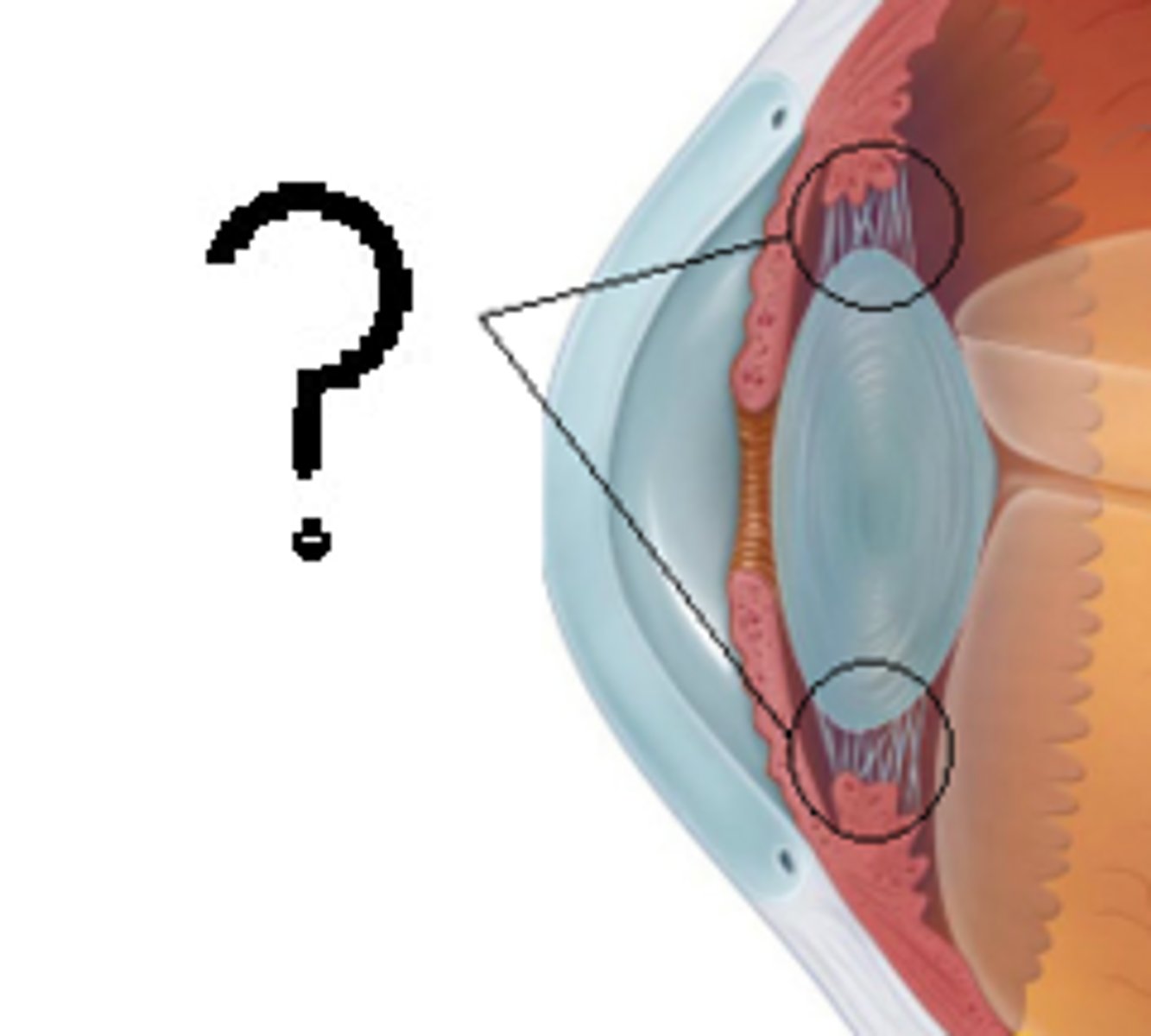
ciliary body
ring of tissue behind the peripheral iris that is composed of ciliary muscle and ciliary processes
suspensory ligaments
hold the lens in place
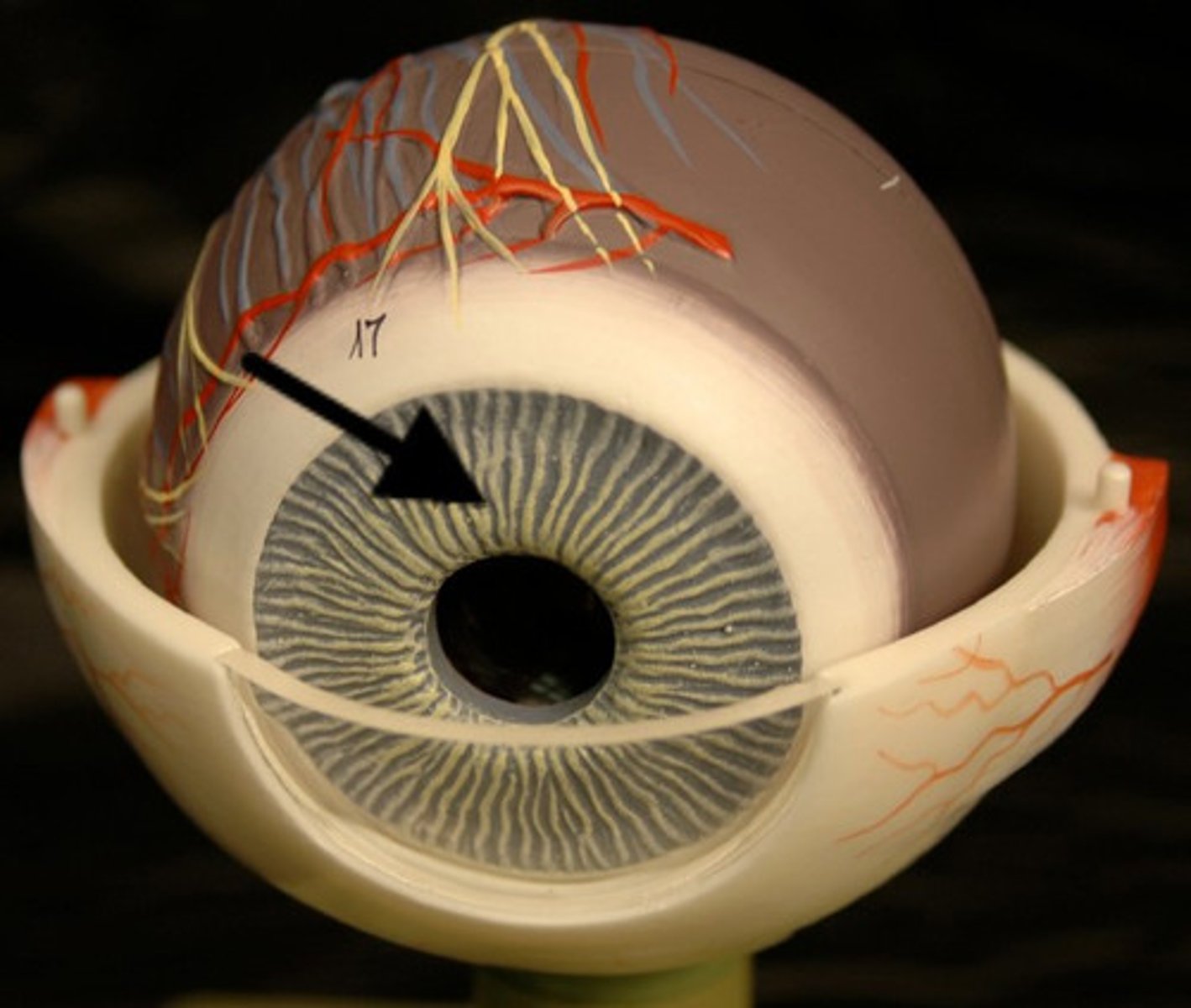
iris
a ring of muscle tissue that forms the colored portion of the eye around the pupil and controls the size of the pupil opening
cornea
The clear tissue that covers the front of the eye
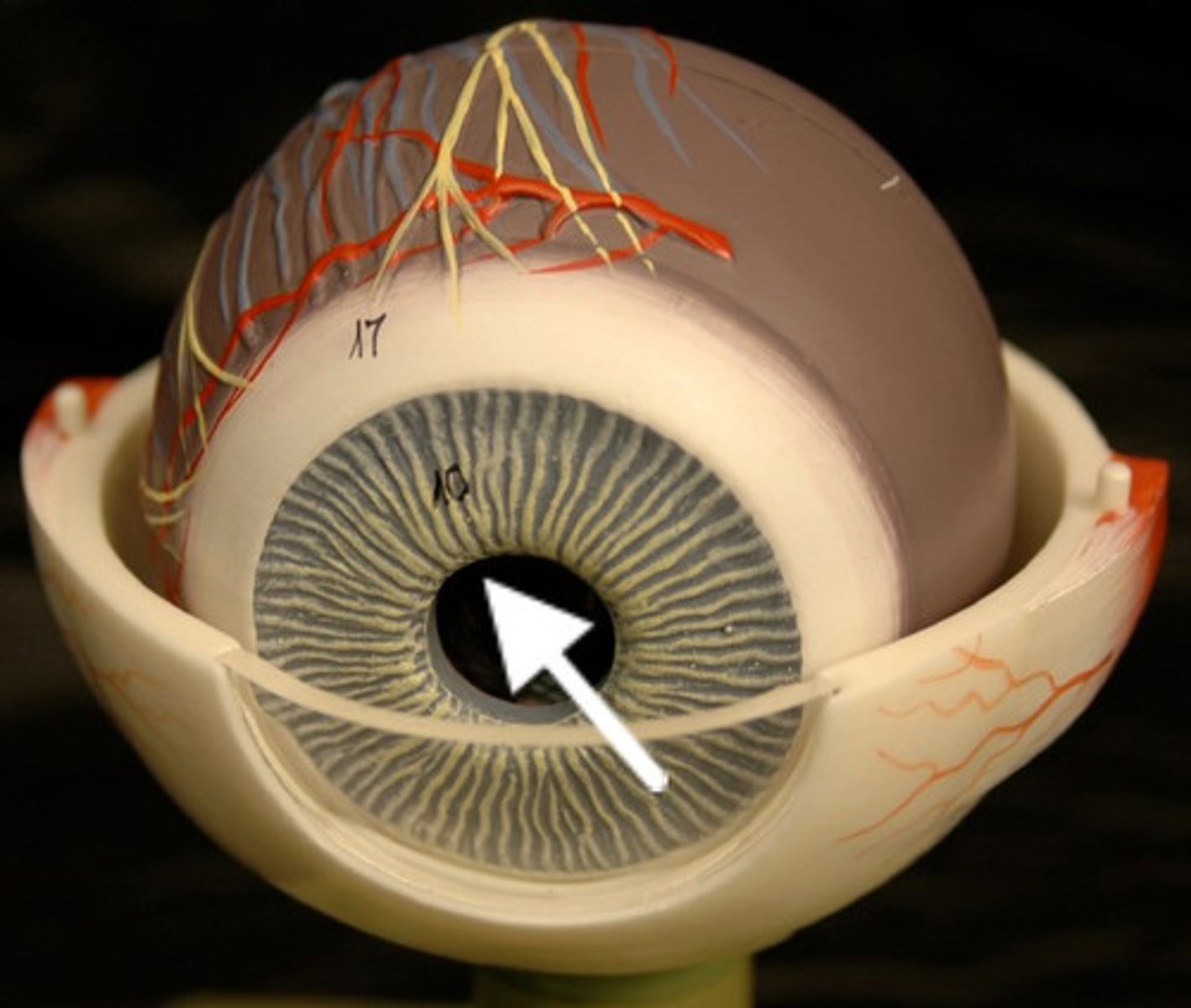
pupil
the adjustable opening in the center of the eye through which light enters
lens
the transparent structure behind the pupil that changes shape to help focus images on the retina