Psychiatry exam
1/48
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
49 Terms
1. Disturbances in perception
Abnormalities in how a person perceives/experiences sensory stimuli. These can involve any of the five senses and may include hallucinations & illusions. They can vary in intensity, being hyper- or hypoesthesia
1. Types of disturbances in perception
Quantitative disturbances
Illusions
Hallucinations
Pseudohallucinations
Depersonalisation and derealisation
1+2. Principles of assessment
Anamnesis, past psychiatric and medical history and treatment, personal history and premorbid personality, family history, presenting complaints
Mental status examination: appearance and behaviour, speech, mood, thoughts, perception, cognition and insight
Rule out organic causes
Risk assessment, substance use (toxicology screening) and physical examination
Clinical disorders according to ICD-10
F20-F29 → schizophrenia and delusional disorders
F30-F39 → mood (affective) disorders
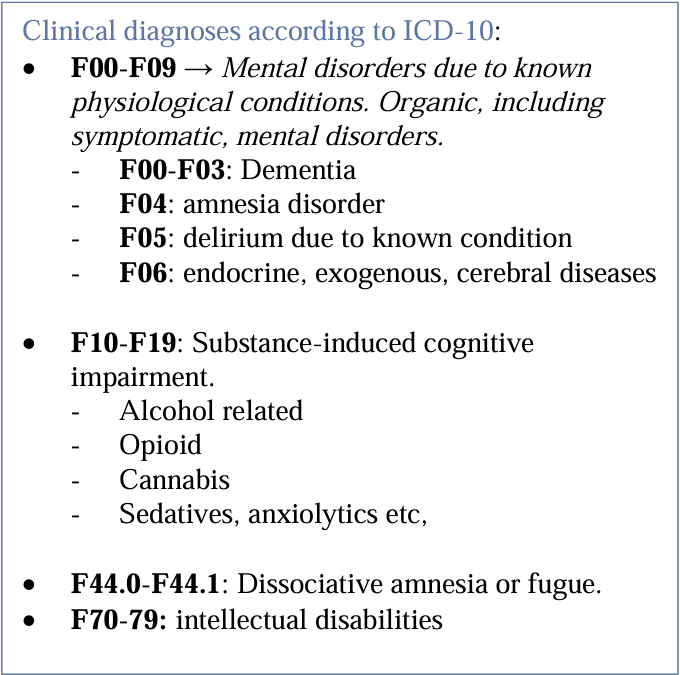
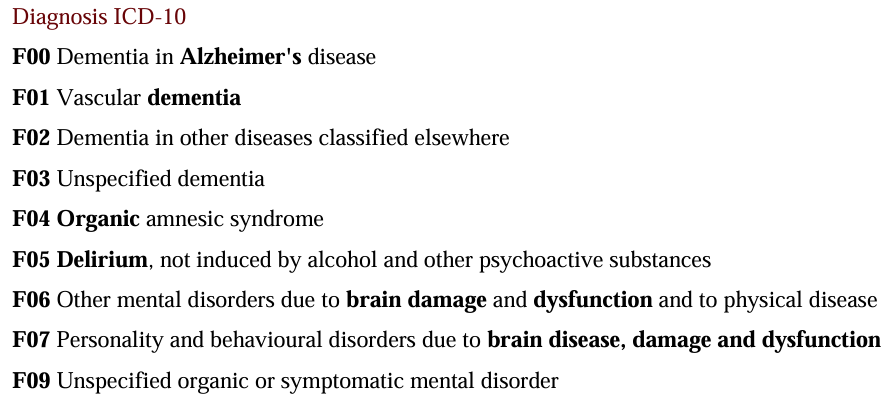
F00-F09 → organic, including symptomatic, mental disorders
1+2. Indications for emergency hospitalisation
Risk to themselves/others
Severe mood disturbances
Substance-related
Acute psychosis
Severe eating disorders
Inability to care for basic needs
Lack of insight
Hallucinations are demanding
Suspected organic cause or delirium
1-3. Risk management in the work with patients
Safe environment and room set up (exits)
Clinical risk assessment - suicide ideation, substance abuse can escalate unpredictable behaviour
Avoid unnecessary physical contact, communicate in a neutral and positive manner
Emergency protocols and stabilisation (pharmacological management) of the patient
Monitor regularly
Understand circumstances on how they came to the clinic - violence, etc.
Disturbances of thinking
Abnormalities in the process, form, or content of thought. impairs communication, decision-making, and perceiving reality
Types of disturbances in thinking
Disturbances in form and flow:
slow/accelerated, thought blocking
word salad
tangentiality
echolalia
stereotypy
connectivity
Disturbances in content:
overvalued ideas
delusions
ideas of references
Disturbances in thought control
thought insertion
thought withdrawal
thought broadcasting
Clinical disorders according to ICD-10
F20-F29 → schizophrenia and delusional disorders
F30-F39 → mood (affective) disorders
F00-F09 → organic, including symptomatic, mental disorders
3. Disturbances in mood
Pathological and persistent changes in a persons emotional state that are disproportionate to their actual circumstances and significantly impair their ability to function
Affect - emotional state at any given period
Mood - emotional stage during longer period
3. Types of disturbances in mood
Depressive: Sadness, hopelessness, or anhedonia.
Manic: Elevated or irritable mood, increased energy, and grandiosity.
Hypomanic: Similar to mania but less severe and without psychotic features or significant functional impairment
Elated: euphoria, elation, exaltation, ecstasy
Bipolar
Anxiety: Excessive worry or tension. Generalized, mutism.
Trait anxiety: anxiety as a feature of temperament
Panic, phobias: irrational fear. Ex. Agoraphobia (public or crowded place)
Dysphoric: combination of anxiety, depression, and irritability.
3. Principles of assessment
PHQ9
HAM-D,YMRS, GDS
Anamnesis, past psychiatric and medical history and treatment, personal history and premorbid personality, family history, presenting complaints
Mental status examination: appearance and behaviour, speech, mood, thoughts, perception, cognition and insight
Rule out organic causes
Risk assessment, substance use (toxicology screening) and physical examination
3. Clinical disorders according to ICD-10
F30-F39 → mood (affective) disorders
F00-F09 → organic, including symptomatic, mental disorders
3. Indications for emergency hospitalisation
Suicidal ideation, plans or attempts
Severe mania
Lack of insight
Psychotic symptoms
Risk of self harm or to others
4. Symptoms of anxiety
Divided into 4 types:
Physical: tachycardia, hyperventilation, sweating, shaking, nausea, dizziness, dry mouth, fatigue
Cognitive: excessive worry, difficulty concentrating, catastrophic thinking
Emotional: irritability, restlessness, panic
Behavioural: avoidance of situation, unable to leave house, compulsiveness
Principles of assessment
Anamnesis, Psychiatric history, medical history and treatment, family history, presenting complaints.
Mental status examination: Appearance, behaviour, speech, mood, thoughts, perception, cognition, insight.
Risk assessment, substance use, physical examination
With focus on:
nature and intensity of anxiety, duration and course, triggering situations, impact on daily life, suicidal risk/harm to others risk
4. Clinical disorders according to ICD-10
F40-F48 - Anxiety, dissociative, stress-related, somatoform and other nonpsychotic mental disorders
Generalized anxiety disorders (F41.1) Panic disorder (F41.0) Phobic anxiety disorders (F40)
Mood (affective) disorders (F30-F39)
Psychotic disorders (F20-F29)
Substance related or withdrawal state (F10-F19)
Organic mental disorders (F00-F09)
5. Cognitive symptoms
Cognitive symptoms involve impairments or abnormalities in mental processes, such as memory, attention, language, executive function, and visuospatial abilities.
Disturbances in consciousness - clouding, delirium, stupor
Memory impairment in retention, recall, registration
Attention and concentration - reduced attention span, high distractibility
Executive function and thinking - slow thinking, impaired planning, poor judgement’
Language and perception - aphasia, apraxia
Orientation - time, place, person
Confusion
5. Principles of assessment
Anamnesis, past psychiatric and medical history and treatment, personal history and premorbid personality, family history, presenting complaints
Mental status examination: appearance and behaviour, speech, mood, thoughts, perception, cognition and insight
Rule out organic causes
Risk assessment, substance use (toxicology screening) and physical examination (blood tests, EEG, brain imaging (CT,MRI))
GCS + Montreal cognitive assessment
5. Clinical disorders according to ICD-10
6. Aetiology and pathogenesis of schizophrenia
Exact cause unknown.
Combination of genetics (genes susceptible: dysbindin, COMT), neurological factors (dopamine dysregulation, hyper + hypo-activity in mesolimbic system) and external factors (perinatal, life events, substance abuse)
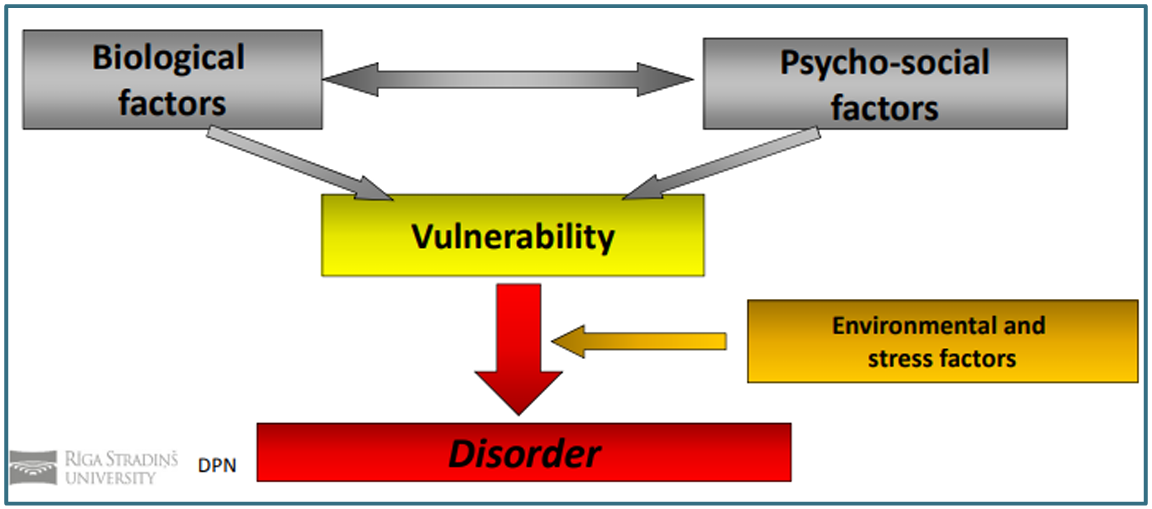
6. Vulnerability model of mental disorders
Process where schizophrenia manifests when a biological or psychological vulnerability (diathesis) interacts with stressful events in life. Explains variability in onset, course & relapse
6. Positive and negative symptoms of schizophrenia
Positive - “what the disease adds”
Hallucinations
Delusions
Thought control: insertion/withdrawal/broadcast
Catatonic behaviour
Disorganised thought and speech
Negative - “what the disease takes away” 5 A’s
Affective flattening (emotion)
Alogia
Avolition
Social withdrawal (Asociality, Anhedonia)
formal though disorders, abstract
+cognitive symptoms
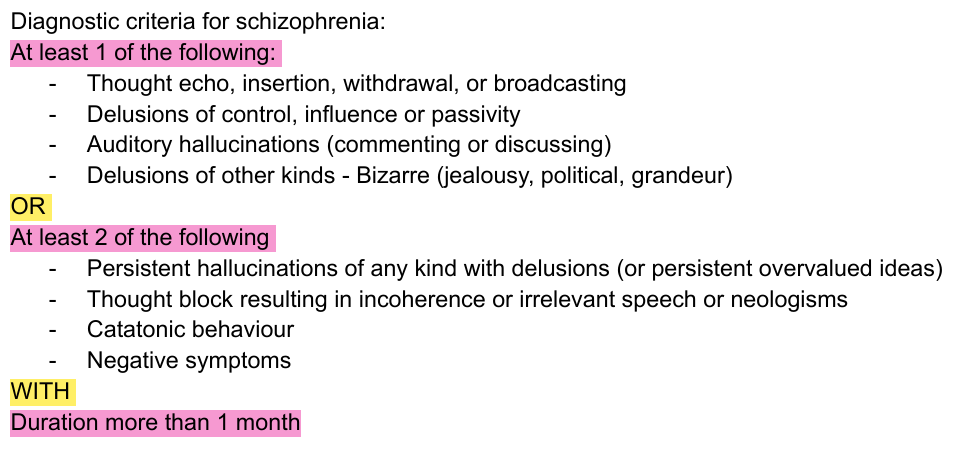
7. Prevalence and diagnostic criteria for schizophrenia (F20) according to ICD-10
Lifetime prevelance: 1% of world population
Incidence: 15-30/100,00/per year
Onset: earlier in men (adolescence), later in women
Male: female ration 1.4:1
7-9. Management strategy and recommendations, for patients with acute psychotic symptoms
Hospitalise patient
Ensure safety: patient and health care workers.
Create a low stimulus environment
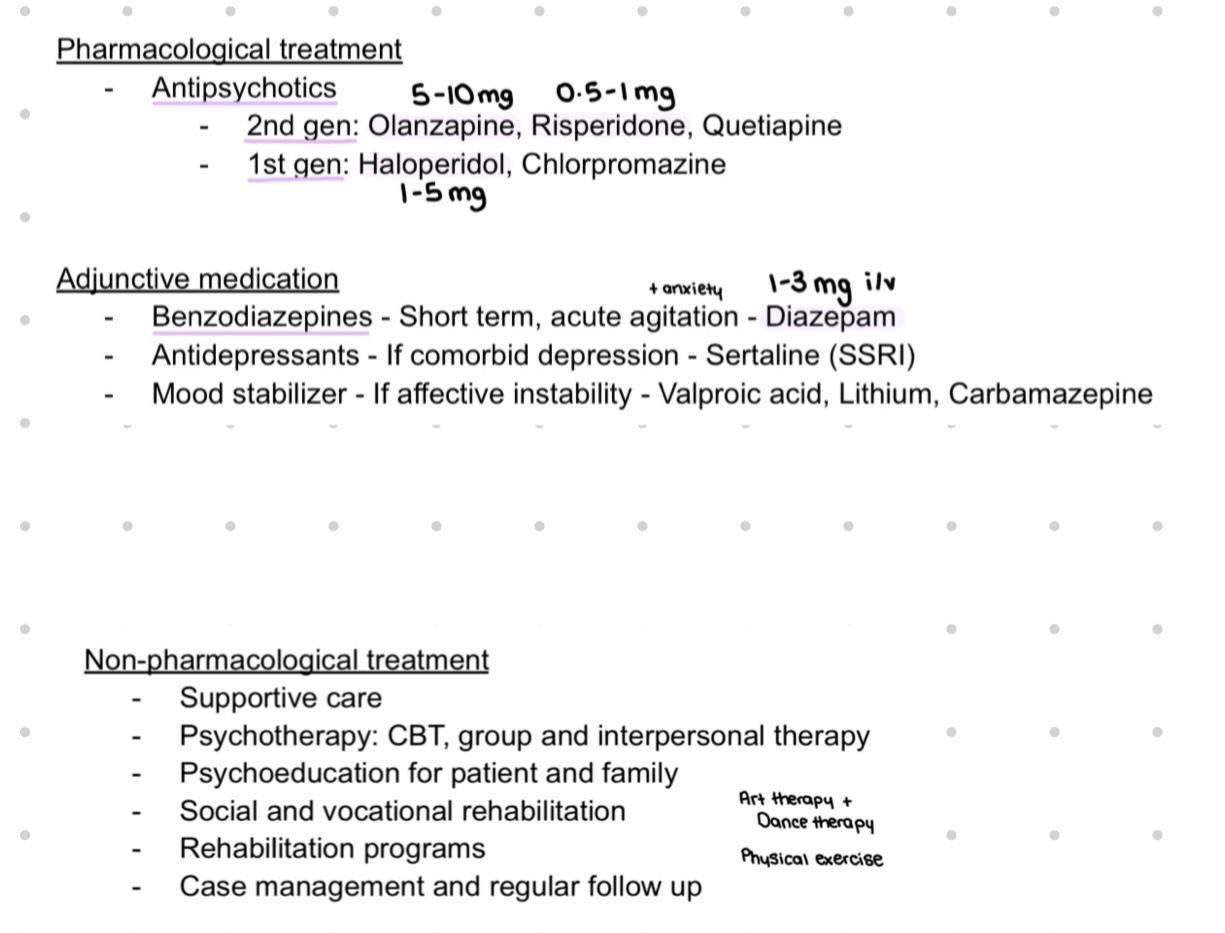
Pharmacological treatment: Benzodiazepines: Diazepam 1–3 mg iv only if needed (agitation, anxiety). Antipsychotics: olanzapine 5-10mg or haloperidol 1-5 mg
Non pharmacological interventions: CBT, psychoeducation, social support, family involvement, social skills training, family therapy
Monitoring
8. Epidemiology, clinical features and basic diagnostic criteria for Acute and transient psychotic (F23) and Schizoaffective (F25) disorders according to ICD-10
Acute and transient psychotic (F23)
Epidemiology
4 per 100,000 per year. 6% of all first-episode psychoses
More common in young adults, women > men
Clinical Features and Diagnostic criteria
Presence of psychotic symptoms (hallucinations, delusions, disorganized thinking, grossly disorganized or abnormal motor behaviour)
Absence of mood symptoms
Acute onset of psychotic symptoms
Duration - At least 1 day, less than 1 month. Abrupt onset and resolution - Usually self-limiting or remitting course.
Spontaneous relief within weeks-months - Complete recovery within 1-3 months
Symptoms may be Polymorphic, Schizophrenia-like
No evidence of organic or substance use
Does not meet criteria for schizophrenia (duration too short)
Schizoaffective Disorder (F25)
Epidemiology
0.5-0.8% of population, women > men
Prevalence: later onset in women than men
Clinical Features and Diagnostic criteria
Psychotic symptoms (period of at least 2 weeks) - hallucinations, delusions, disorganized thinking, Negative symptoms: diminished emotional expression, reduced motivation, social withdrawal, impaired cognitive functioning.
Mood symptoms (one affective disorder) - depressive symptoms, manic symptoms
Both present simultaneously or separate (with days in between) for a substantial period
Criteria of schizophrenia and mood disorder must be met
Exclusion of organic mental disorder (F00-F09) Or substance induced causes (F10-F19)
9. Basic biopsychosocial treatment and rehabilitation principles of Schizophrenia
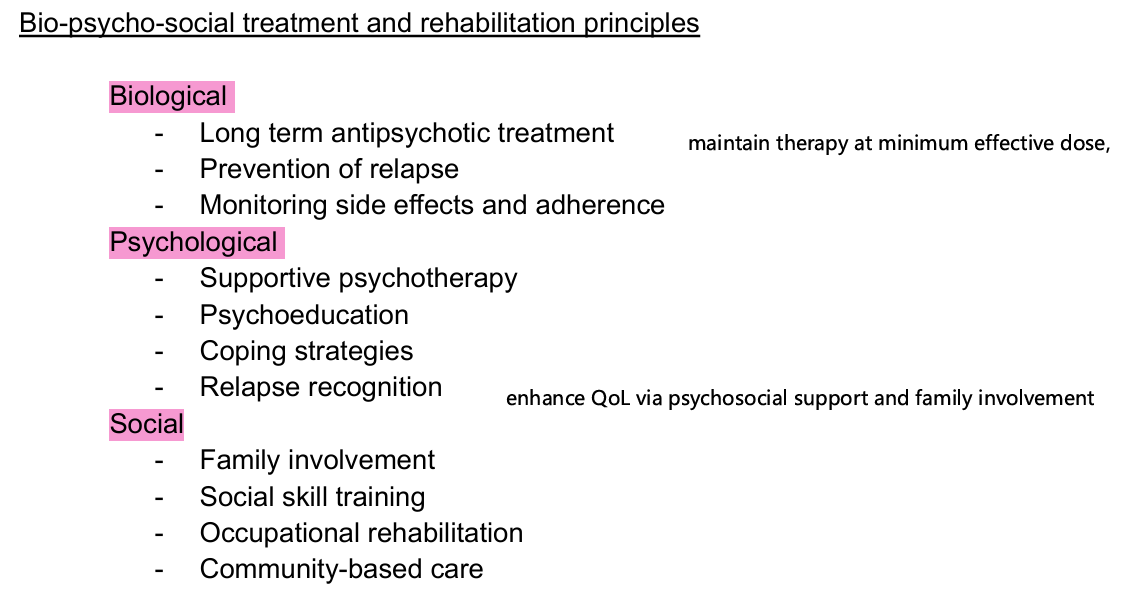
9. Pharmacological and non pharmacological treatment possibilities (schizophrenia)
9.Types of extrapyramidal side effects of antipsychotic medication and their management
Acute dystonia
Parkinsonism
Akathisia
Bradykinesia
Management: Trihexyphenidyl (centralM-cholinoblocker) & Benzodiazepines for spasms and tremor
10. Essence of organic and symptomatic mental disorders
Organic and symptomatic mental disorders (F00-F09) are psychiatric syndromes caused by identifiable brain damage, disease or systemic illness affecting brain function. Where the mental disorder is a direct consequence of the underlying condition
10. Most common clinical features and diagnosis according to ICD-10.
Cognitive impairment : Memory loss, impaired attention, executive function, disoriented
Reduced level of consciousness
Emotional liability
Behavioural changes
Psychotic symptoms: hallucinations, delusions
Personality changes: irritability, apathy, emotional
Fluctuating course
Seizures
Delirium
10. Causes of organic brain disorders
Primary CNS causes
Neurodegenerative
Cerebrovascular disease
Brain tumours
Traumatic brain epilepsy
Epilepsy
CNS infections (HIV, HSV, meningitis, encephalitis … )
Secondary - Systemic causes
Metabolic disorders: hypoglycaemia, electrolyte balance
Endocrine disorders: E.g. Thyroid disease
Hypoxia
Vitamin deficiencies: B1, B9, B12
Toxic or medication effects
Severe systemic illnesses
10. Diagnostic assessments, differential diagnoses
Based on clinical and objective evidence
History of organic disease or medical condition
Psychiatric assessment and mental status examination
Neurological examination
Cognitive testing - Neuropsychological testing (MMSE, MoCA)
Laboratory investigations - Imaging - CT/MRI - EEG - If indicated
Temporal relationship between brain and disease and psychiatric symptoms
Improvement of mental symptoms when underlying cause is treated
11. General description of dementia, reversible and non-reversible causes
Chronic brain syndrome. Its main feature is memory impairment without impaired consciousness. Dementia arises from an organic disease, known aetiology. Impairment of multiple higher cortical functions, including memory, thinking, orientation, comprehension, calculation, learning capacity, language and judgment.
Reversible causes
Depression
Metabolic: Vit B9/B12 deficiency, hypothyroidism, other metabolic disorders
Pressure: Normal pressure hydrocephalus, subdural hematoma, brain tumours
Infections: neurosyphilis, HIV, meningitis, encephalitis
Toxic: alcohol-related, heavy metal poisoning
Medication: side effects (anticholinergics, sedatives)
Non-reversible
Neurodegenerative: alzheimer’s (50%), Lewy body dementia, huntington’s
Frontotemporal dementia
Vascular dementia (20-25%): strokes, ischemia
Parkinson’s dementia
Prion disease: Creutzfeldt-Jakob disease
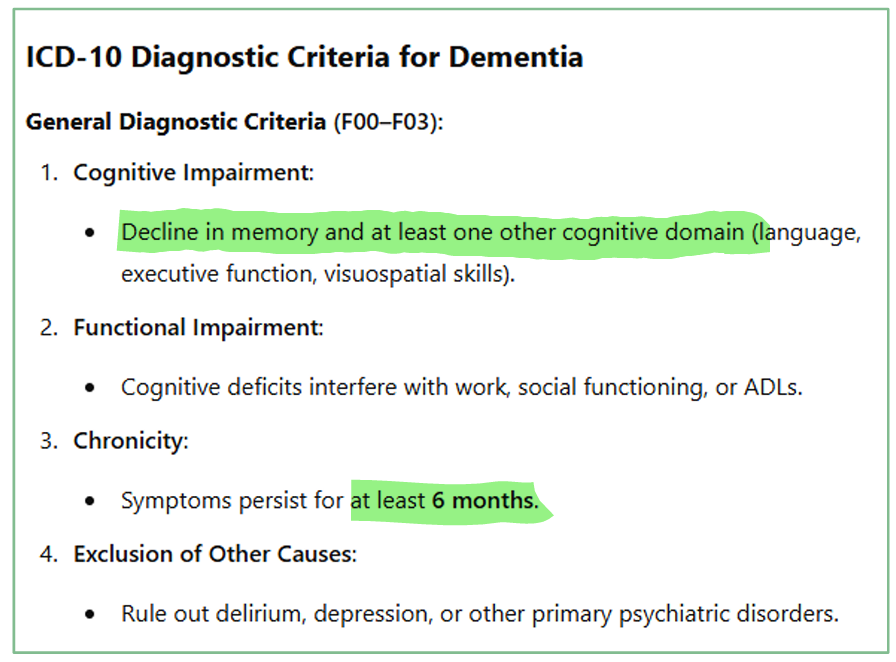
11. Clinical features of dementia, general diagnostic criteria according to ICD-10
Decline in recent memory, thinking and judgement, orientation, language,
Impairment in abstract thinking
Patients often appear apathetic or disinterested, but may appear alert and appropriate despite poor memory,
Decline in everyday functioning (dressing, washing, cooking),
Personality change: Loss of emotional control, patients may be easily upset, tearful or irritable.
Common in older patients, very rare in youth or middle age
11. Differential diagnoses of Dementia, basic principles of treatment and care
Treatment and care
Treat reversible cause!
Start with non pharmacological treatment
Non pharmacological treatment focusing on maintaining QoL.
Orientation aids - routine, calendar, clock, pictures, notes
Regular exercise, nutritional support, safety interventions: restrictions on oven and doors, carpet
Social day care, environmental (quiet, well-lit room, calm clean)
Memory therapy
Psychomotor therapies - dance, drama, singing, sport, music art
Cognitive stimulation therapy
Pharmacological treatment when appropriate
Dementia medication: Donzepil 5-10mg x1, Rivastigmine 6-12mg x2, Memantine 20-30mg x1
Psychotic events: Olanzapine 2.5mg (short term only)
Depression: Sertraline 50mg/day
11-15. Management strategy and recommendations, if patient has a delirium !!
12. Epidemiology, aetiology, risk factors of Alzheimer’s disease
Epidemiology: 50-70% of dementia cases and 5-8% of patients >65 years. 20% above 80 years.
Aetiology is multifactorial. Genetics in early cases, sporadic in late onset, neurobiological mechanism, environmental factors and lifestyle (comorbidities and socioeconomic status → AH, DM, hyperlipidemia, obesity, head trauma, low education, smoking, poor diet, physical inactivity.
Risk factors
Age >65y, increasing age
female
Risk is 4-5x higher if relative suffered from AD: familial. Autosomal dominant mutation
Traumatic brain injury
Alcohol misuse
2 copies of either of these genes alleles: apoE4, apoE2, apoE3.
Poor education
Sleep disorders
Lifestyle factors
Depression
12. Possible pathophysiological mechanisms of AD
Amyloid-beta plaque and tau deposition extracellular
Neurofibrially tangles
Progressive neural and synaptic loss and brain atrophy (neuronal loss)
Predominant involvement - Hippocampus - Memory, spatial navigation, learning. Temporal and Parietal lobes
Cholinergic deficit → Reduced acetylcholine (ACTH) transmission
12. Clinical features and prognosis of dementia in Alzheimer's disease (F00)
Prognosis: the cognitive decline is progressive and non-reversal but can be slowed with medication (no curative treatment). Death is usually between 5-8 years of onset. Neurological signs and psychotic episodes have worse prognosis.
Clinical Features + Diagnostic criteria according to ICD-10 (Q13) :
Development of multiple cognitive deficits >6 months
1) Memory impairment (impaired ability to learn new information or to recall previously learned information).
2) One (or more) of the following cognitive disturbances: a. Aphasia (language disturbance) b. Apraxia (impaired ability to carry out motor activities despite intact motor function) c. Agnosia (failure to recognise or identify objects despite intact sensory function) d. Disturbance in executive functioning (i.e. planning, organising, sequencing, abstracting)
Personality changes
The cognitive deficits cause significant impairment in social or occupational functioning and represent a significant decline from a previous level of functioning. The course is characterised by gradual onset and continuing cognitive decline.
Exclusion of other possible causes of dementia
Absence of disturbances in consciousness
13. Clinical features, diagnostic criteria and differential diagnosis of dementia in Alzheimer's disease (F00) according to ICD-10
‘‘ (answered in Q12)
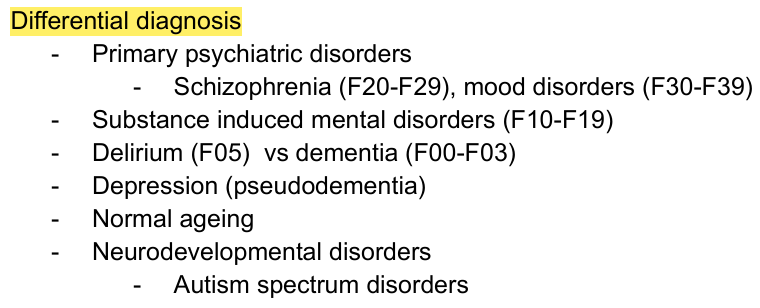
Differential diagnosis
Vascular dementia (F01)
Delirium (F05)
Depression (pseudodementia)
Dementia with lewy-bodies
Normal aging
Medication or substance side effects
Mild cognitive impairment
Metabolic disorders
Structural brain abnormalities
Neurodegenerative disorders
10-13. Pharmacological and non-pharmacological treatment possibilities for AD
Non pharmacological treatment focusing maintaining QoL.
Orientation aids - routine, calendar, clock, pictures, notes
Regular exercise, nutritional support, safety interventions: restrictions on oven and doors, carpet
Social day care, environmental (quiet, well-lit room, calm clean)
Memory therapy
Psychomotor therapies - dance, drama, singing, sport, music art
Cognitive stimulation therapy
Pharmacological treatment when appropriate
Dementia medication: Donzepil 5-10mg x1, Rivastigmine 6-12mg x2, Memantine 20-30mg x1
Psychotic events: Olanzapine 2.5mg (short term only)
Depression: Sertraline 50mg/day
141-14. Epidemiology, aetiology, prophylaxis of Vascular dementia (F01)
Epidemiology: Vascular dementia is the 2nd most common cause of dementia after Alzheimer's disease. It accounts for approximately 10-20% of all dementia cases. It's more common in older age groups. More common in Men, typical onset after 65