ch 18 O2 transport and regulation
1/80
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
81 Terms
4 processes of respiration
ventilation
pulmonary gas exchange
gas transport
cellular respiration
ventilation (step of respiration)
step 1 of respiration; Movement of air in and out of lungs (atmosphere O2 → lungs)
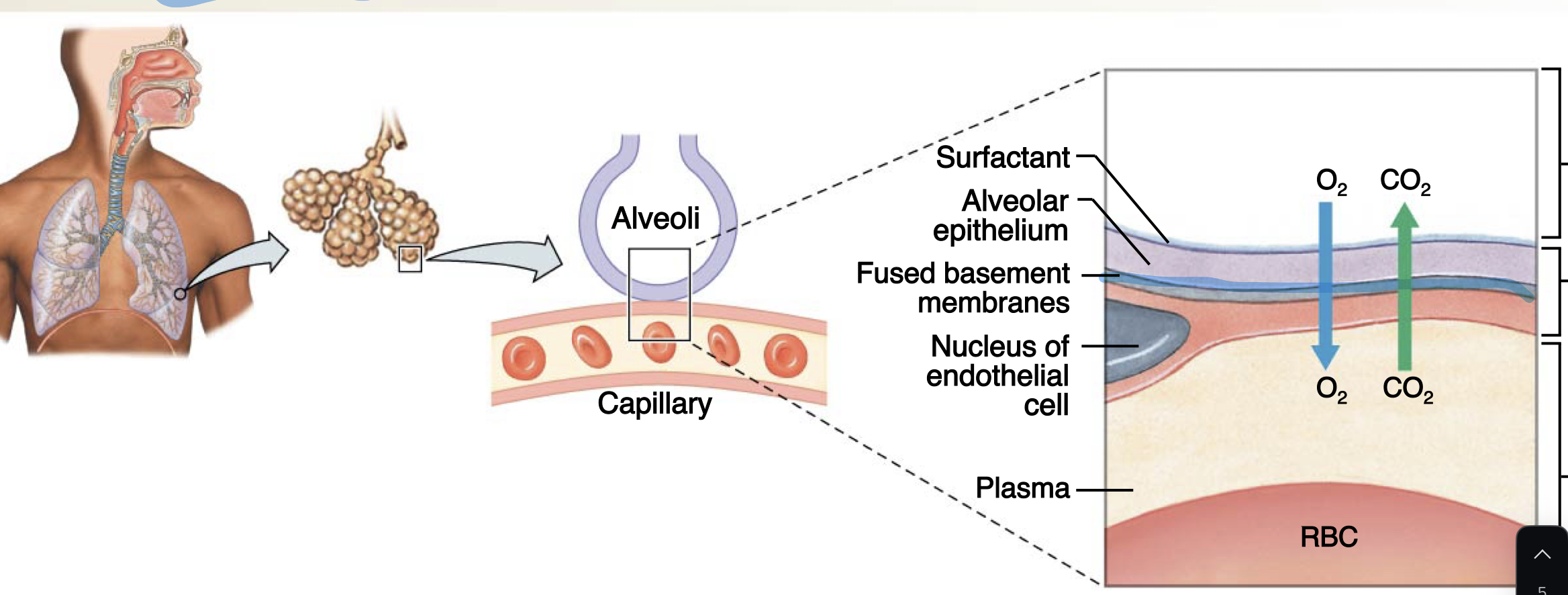
pulmonary gas exchange (step of respiration)
step 2 of respiration;
(O2 in lungs to blood)
O2 enters blood at alveolar-capillary interface, CO2 leaves.
oxygen moves from the lungs to blood, while CO2 moves from the blood to the lungs
Gas Transport (step of respiration)
step 3 of respiration; (blood), blood carries oxygen from the lungs to cells and CO2 from cells to the lungs
Cellular respiration (step of respiration)
step 4 of respiration;
(blood → cells)
oxygen is released to cells and CO2 is picked up from them!
in which direction do gases diffuse?
from areas of higher partial pressure to lower partial pressure
average of PCO2
40 - 46 mmHG
average of PO2
40 - 160 mmHg
diabetes pateints take a super long time to reocver becasue…
bad perfusion damages peripheral nerves; don’t feel the pain
cells form a ________ ______ between lung and blood
diffusion barrier
made of
alveolar air space (with surfactant)
Alveolar epithelium
Fused basement membranes
Endothelial cell nucleus
Plasma
Red Blood Cell (RBC)
hypoxia
dangerous condition where tissues or organs in the body do not receive enough oxygen to function properly.
pathologies causing hypoxia
emphysema
fibrotic lung disease
pulmonary edema
asthma
normal PO2
100 mmHg
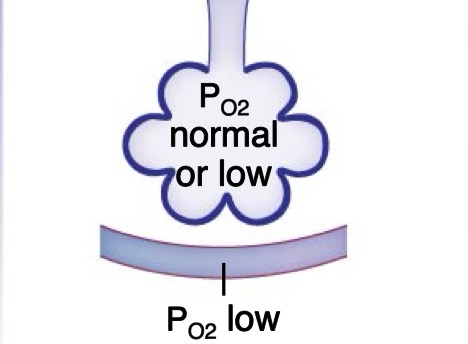
emphysema
Destruction of alveoli → less surface area for gas exchange → low PO2
due to smoking
damages elastic fiber
damaged, inelastic air sacs (alveoli) that trap air, making it hard to breathe
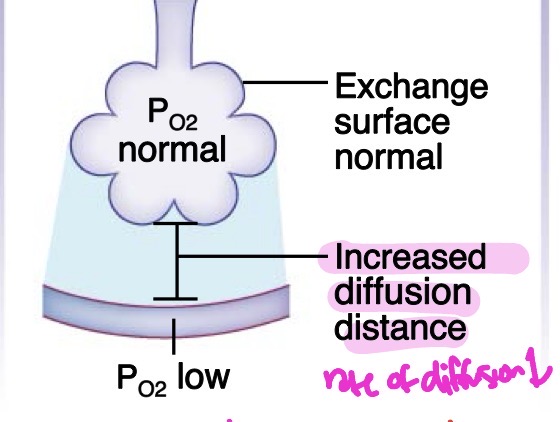
fibrotic lung disease
Thickened alveolar membrane slows gas exchange; loss of lung compliance may decrease alveolar ventilation → low PO2
due to dirty air (ex. working in a minefiled)
lung grows thicker, increasing diffusion distance —- supposed to be simple squamous epithelium
Lung compliance
a measure of the lung's ability to stretch and expand (distensibility) during breathing
pulmonary edema
Fluid in interstitial space increases diffusion distance → low PO2.
arterial PCO2 may be normal due to higher CO2 solubility in water
rate of diffusion decreases
very similar to fibrotic lung disease — both increase diffusion distance
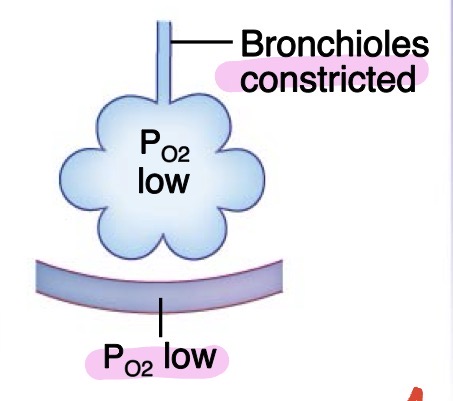
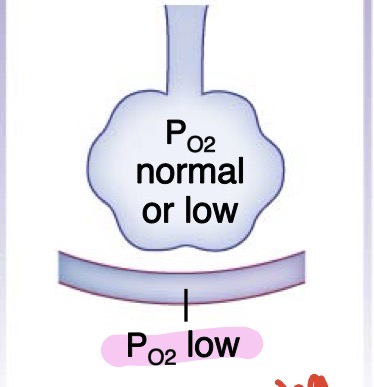
asthma
Increased airway resistance decreases alveolar ventilation → PO2
constricted bronchioles!!
Sequence of Oxygen Movement
Atmospheric O2 → Alveolar O2 → Plasma O2 → HbO2 (hemoglobin O2)
atmospheric O2 affects
all other O2 (alveolar, plasma, and hemoglobin)
Atmospheric O2 is affected by..
altitude, humidity
o2 is low in high altitudes
Alveolar O2 is affected by…
lung compliance (lung’s ability to stretch), airway resistance, rate and depth of breathing
Plasma O2 is affected by…
factors affecting diffusion (distance, surface area, barrier permeability)
alveolar gas exchange is influenced by
O2 reaching the alveoli
gas diffusion between alveoli and blood
adequate perfusion of alveoli
oxygen reaching the alveoli is influenced by
Composition of inspired air (e.g., altitude, humidity).
Alveolar ventilation: Affected by rate and depth of breathing, airway resistance, lung compliance.
alveolar ventiliation is affected by:
rate and depth of breathing
airway reistance
lung compliance
Gas diffusion between alveoli and blood is influenced by:
barrier thickness, amount of fluid, surface area, diffusion distance
when temperature remains constant, the amount of gas that disccolves in a liquid depends on…
the solubility of the gas in the liquid and partial pressure of the gas
oxygen solubility is
LOW;
CO2 solubility is
HIGHER (than O2)
CO2 dissolves in water (plasma) much easier than O2
anemia
not enough red blood cells or dont have healthy RBCS
we need RBCs to carry O2
causes: accelerated RBC loss. hemolytic anemias, decreased RBC production, etc
sickle cell anemia
hereditary disease where they have unhealthy misshapen RBCs — so O2 has difficulty reaching the body
O2 movement is driven by
concentration (pressure)
hematocrit
a test to see if someone has anemia: measures the percentage of your total blood volume that consists of red blood cells (RBCs)
total blood O2 =
O2 dissolved in plasma (PO2) + O2 bound to hemoglobin (HbO2).
hemoglobin’s role in blood
More than 98% of oxygen in blood is bound to hemoglobin in red blood cells; less than 2% is dissolved in plasma!!!
Without hemoglobin, O2 carrying capacity is very low
also carries CO2 and CO (carbon monoxide)
Is most blood dissolved in plasma or bound to hemoglobin?
More than 98% of oxygen in blood is bound to hemoglobin in red blood cells; less than 2% is dissolved in plasma.
how CO2 transports in blood (3)
dissolved CO2: 7%
HbCO2: 23% — CO2 binds to hemoglobin
HCO3- (bicarbonate): 70%
HCO3- (bicarbonate)
stores CO2 in a non-acidic form (buffer) to maintain pH
main buffur
hemoglobin’s role in CO2 transport
it grabs H+ so the blood doesnt get too acidic (backup buffer)
the whole story of CO2 and pH
Cells make CO₂ (waste)
CO₂ enters red blood cells
It turns into carbonic acid (H₂CO₃)
Then breaks into:
H⁺ (acid)
HCO₃⁻ (bicarbonate)
The H⁺ could make blood acidic BUT hemoglobin grabs it → prevents pH from dropping
when CO2 is too high, the pH…
becomes acidic
chloride shift
when bicarbonate leaves the RBC, it loses a negative charge, so chloride must come in to balance the negative charge
the amount of oxygen bound to hemoglobin depends on
plasma O2 and the amount of hemoglobin
hemoglobin increases
oxygen transport
what determins the % saturation of hemoglobin?
plasma O2
what determines the total number of Hb binding sites (calculated from Hb content and number of RBCs?
the amount of hemoglobin
if # of RBCs increase, more _________ is carried to your tissues
oxygen
hemoglobin consists of ___________, centered around a _____ group
4 polypeptides, heme group
hemoglobin can carry up to
4 oxygen molecules
4 polypeptides of hemoglobin
2 alpha and 2 beta
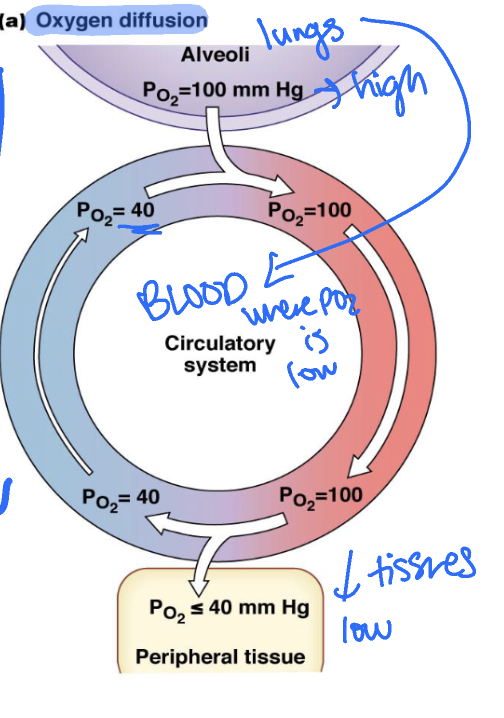
gas exchange: oxygen diffusion
alveoli (lungs) → blood → peripheral tissue
moves from high PO2 in ungs to low PO2 in blood and in peripheral tissue
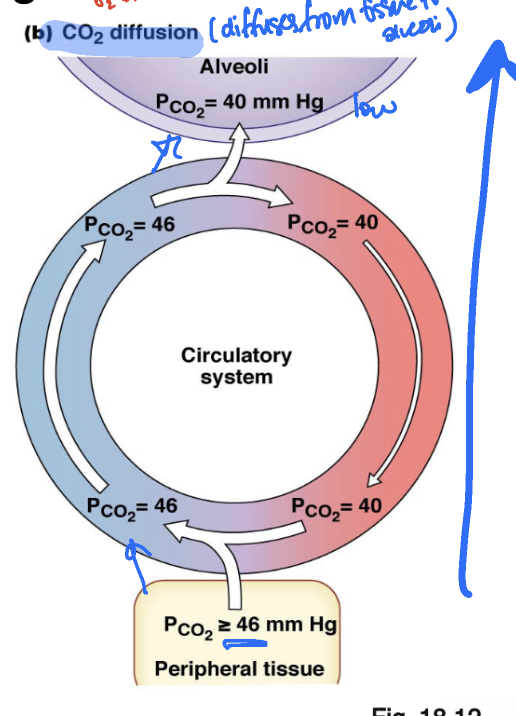
gas exchange: carbon dioxide diffusion
peripheral tissue → blood → alveoli (lungs)
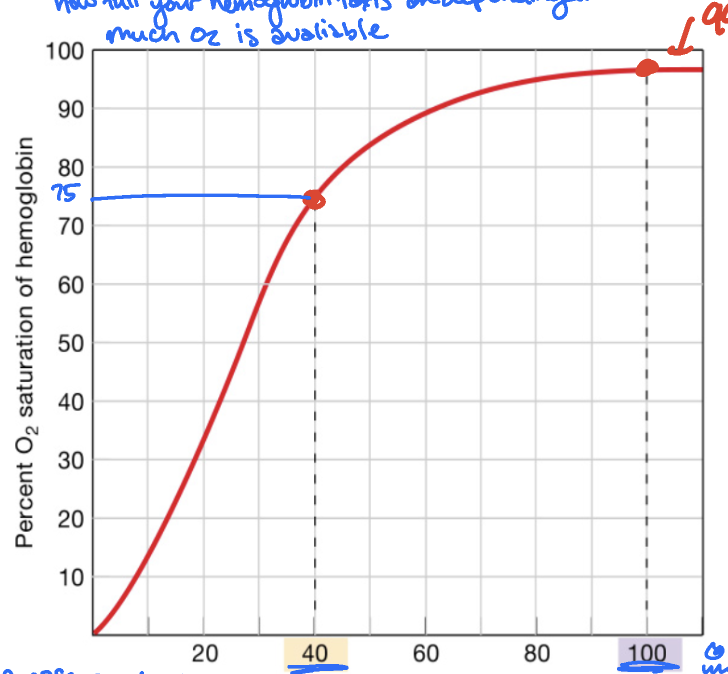
normal HbO2% saturation curve
shows how full your hemoglobin “taxis” are depending on how much O2 is avaliable
in a resting cell (40 mmHg), 75%
in alveoli (100mmHg), 99%
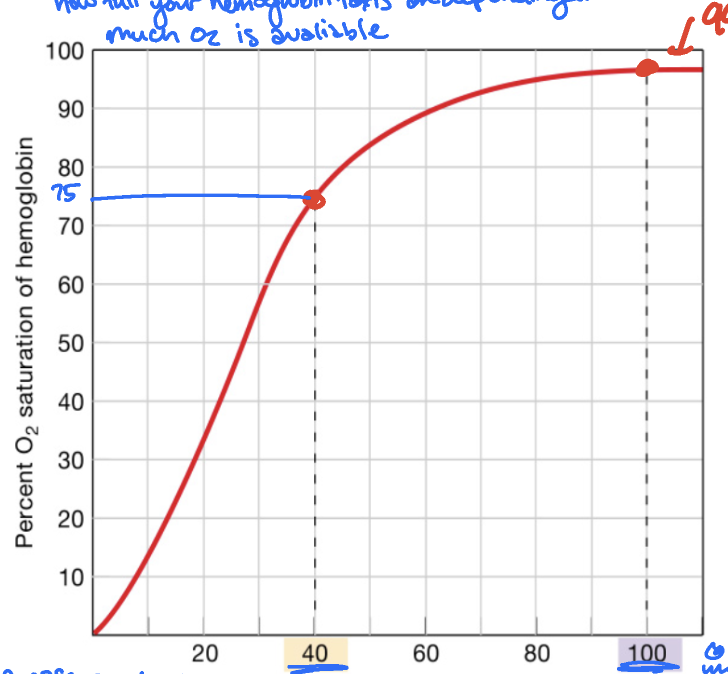
higher pressure on the curve means
hemoglobin is loading up on O2
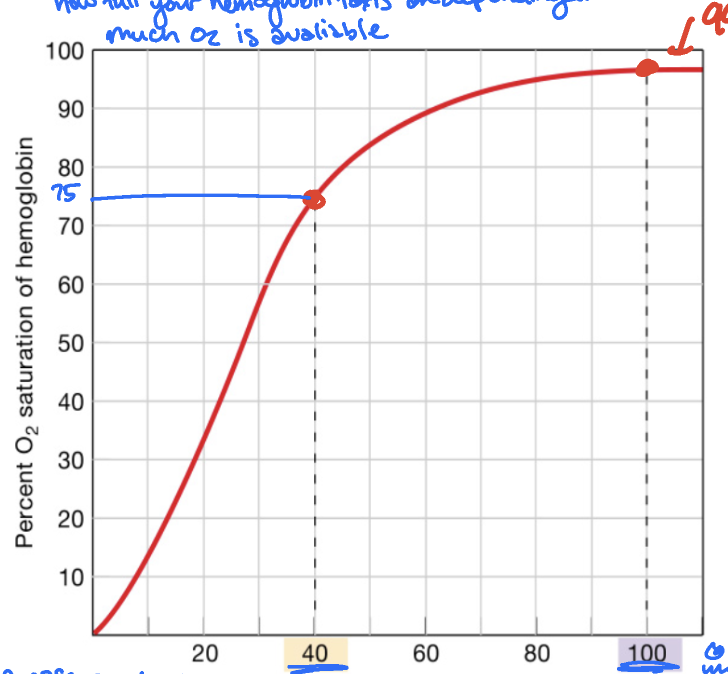
lower pressure on the curve means
hemoglobin is unloading up O2
left shift in Hb curve
Hemoglobin has a higher affinty for O2
grabs O2 easier and is stingier
right shift in Hb curve
Hb has a lower affinity for O2
easier to release O2
results in lower saturation at a certain pressure compared to the normal curve bc of O2 release
factors that decrease affinity of Hb for O2 (right shift)
increased CO2
increased temperature
increased acidity (lower pH)
increased 2,3-DPG
factors that increase affinity of Hb for O2 (left shift)
less acidity (higher pH)
lower temperature
lower PCO2
lower 2,3-DPG
fetal hemoglobin causes a
fetal Hb has a higher affintiy for O2 than adult Hb, becasue it has to steal O2 from its mother’s blood
left shift!!!
Carbon monoxide poisoning
CO binds to Hb on the exact same spot as O2 on Hb, but much mroe strongly, leaving less seats for O2 to bind
treatment for carbon monoxide poisoning
breathing in pure O2 to get ride of the CO
is CO poisoning a right or left shift?
it is am extreme right shift case
decreases affinity for O2
How does the body respond to hypoxia/high altitudes?
increased erythropoitin, a hormone, that travels to the bone marrow and tells it to produce more RBCs
with RBCs, there are more taxis to pick up whatever O2 is avaliable
hypoxia
low oxygen; can be due to higher altitudes
total arterial O2 content
oxygen dissolved in plasma (PO2 of plasma) (2%)
influenced by rate and depth of breathing, airway resitance, and lung compliance, surface area, diffusion distance (membrane thickness)
oxygen bound to Hb (98%)
influenced by % saturation of Hb, total number of binding sites — PCO2, pH, temperature, 2,3-DPG, Hb content per RBC, number of RBCs
neural control of breathing
involuntary
controlled by medulla oblongata & pons
ex. pacemaker for breathing
voluntary
controlled by higher brain centers (cerebral cortex), skeletal
ex. holding your breath or speak
emotions
limbic system
ex. gasping when scared
respiratory control centers
medulla oblongata
pons
dorsal respiratory group (DRG)
ventral respiratory group (VRG)
medulla oblongata
initiates respiration; one of the pacemakers
pons
modulates respiration; acts as the bridge and smooths the transition between inhaling and exhaling; talks between DRG & VRG!
dorsal respiratory group (DRG)
in the medulla; quiet breathing (inspiration)
triggers diaphragm to inhale
ventral respiratory group (VRG)
in medulla: forced breathing (expiration)
ex. when you exercising and need to more air out of your lungs quickly
chemoreceptor response
thermostat for breathing
central (medullary) chemoreceptors
CO2 can cross the BBB but H+ (acid) cannot
when CO2 gets into the cerebrospinal fluid, it turns into H+
brain senses the acid and screams breathe (increased ventilation) to get rid of the CO2
receptors that ONLY detect CO2 levels via H+
when CO2 gets into the cerebrospinal fluid, it turns into
H+
Which can cross the BBB: CO2 or H+?
CO2
it crosses and then turns into H+
peripheral chemoreceptors (neck/heart)
detects CO2, pH, and ocygen
only detects when O2 is at a dangerously LOW levels (below 60mmHg)
what is primary driver for breathing?
CO2 levels detected as H+ in the brain
pre-botzinger complex
pacemaker for cells
fetal hemoglobin
left shift