BB Lab Final Exam (copy)
0.0(0)
Studied by 6 peopleCard Sorting
1/70
Earn XP
Description and Tags
Last updated 10:50 PM on 11/13/22
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
71 Terms
1
New cards
The pipette always needs to be held at the same angle; a vertical angle will result in smaller drops, while a 45° angle will result in larger drops- always be consistent and keep the same angle.
How can you assure consistency of volume dispensed when using controlled drop pipettes?
2
New cards
Place tubes in the centrifuge in the same order they were in the rack. This helps to avoid mixups. Also, don't mix and match patients in the centrifuge. If you have time try to only spin one patient at a time
What technique can you use when centrifuging in blood bank immunofuges to increase technologist speed and avoid mix-ups?
3
New cards
Washing: 60 seconds
Reactions: 20 seconds
Reactions: 20 seconds
What is the centrifugation time (at 3400 rpm) for washing cell suspensions ______________ and reaction tubes _______________?
4
New cards
Mother tubes: Patient name and one other identifier (birthday or MRN)
Reaction tubes: Patient last name first initial and what reaction is in tube (anti-A, etc)
Reaction tubes: Patient last name first initial and what reaction is in tube (anti-A, etc)
What general information should appear on labels of tubes used in blood bank testing (not the tube used to draw the blood). Mother tubes should include______. Reaction tubes should include___________.
5
New cards
Use reagent cells to compare suspensions
How do you judge a 3-5% cells suspension (without measuring precisely)?
6
New cards
This ensures that reactions are performed the same way every time between all techs. Also if you drop dead in the middle of setting up a reaction, someone else could hop right in and know where to continue.
Why is it important to have a specific strategy (that is used consistently) to organize a rack for reaction tubes in blood bank?
7
New cards
1) Never have two lids off at once
2) Never leave uncapped bottles on the table
3) Don't touch tips of the droppers to the reaction tubes
2) Never leave uncapped bottles on the table
3) Don't touch tips of the droppers to the reaction tubes
What are 3 rules for handling bottled reagents (antisera or cells)?
8
New cards
Clear stuff first (antisera, plasma) then cells last. This is because it is easier to visualize that all reagents were dropped into their appropriate reaction tubes
In what order should reagents be added to reaction tubes and why?
9
New cards
Front type--Commercial antisera and patient cells. Looking for antigens on patient cells
Back type--Patient plasma and commercial cells. Looking for antibodies in patient plasma
Back type--Patient plasma and commercial cells. Looking for antibodies in patient plasma
List the two main parts (phases) to a blood type and describe what you are testing for in each part
10
New cards
A person will not make ABYs to antigens they have, this is because the possessed antigens are considered "self". The only exception is autoimmune ABYs to RBC antigens
Describe Landsteiner's Law
11
New cards
For the front type, the patient's cells must be in a 3% solution. From there, it is a 1:1 ratio between patient 3% cell solution and anti-sera (1 drop of each). For the back type, you do a ratio of 2:1, with 2 drops of plasma and 1 drop of commercial A1 or B cells
What volume of anti-sera and patient's cells do you add in the Front Type? How much patient plasma and commercial cells do you add in the back type?
12
New cards
Reactive at 37C. Will cause harm to a patient
Explain what is meant by clinically significant. Are ABO antibodies clinically significant?
13
New cards
We have to use a 3% solution of patient cells to create a "zone of equivalence" between patient AGN and ABY. If the suspension is too light, there will be excess ABY compared to AGN, and create a "prozone" effect. If the suspension is too heavy, it'll create a "post-zone", where there is too much AGN compared to ABY
Why do we use a 3% suspension of patient cells. What do you think could happen if our suspension is too light? Too heavy?
14
New cards
Hemolytic disease of the newborn (HDN), transfusion reactions (HTR), and autoimmune (or drug induced) hemolytic anemias (AIHA/DIHA). A positive DAT result would infer that the patient is making sensitized RBCs to IgG or complement CD3.
What are the 3 situations where a DAT would be appropriate to order? What would a positive result tell you?
15
New cards
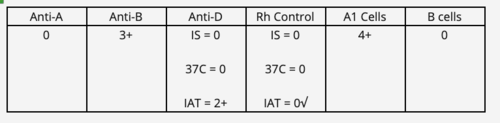
Bpos, weak D pos
The following results were obtained on a patient workup. Interpret the ABO and Rh type
16
New cards
If unbound antibodies are not washed away, they remain in the reaction tube and can bind anti-IgG that should be binding to antibody of the cells. You will get reagent neutralization (of anti-IgG), no agglutination, and a false negative result.
What type of error is caused by insufficient washing of cells in a reaction tube ? Provide a reason why.
17
New cards
Coombs control cells (check cells) are IgG-sensitized or complement coated RBCs that are added to reactions to check that negative results. If it is a true negative, agglutination will occur when Check cells are added, if AHG reagent was forgotten then agglutination will not take place even with check cells
What are Coombs control cells? What are they used for?
18
New cards
A pos DAT invalidates all IAT testing. DAT pos cells will react with the anti-IgG in weak D testing regardless of whether or not D antigen is present. Monoclonal anti-D with a neg Rh control at IS. If you really really wanted to know weak D, genetic testing or elution.
How does a positive DAT affect typing for Weak D? Explain the mechanism behind your answer. How can you get an accurate Rh type on the patient?
19
New cards
O cells--ABO antibody or another blood group.
AC--Auto antibody
AC--Auto antibody
When resolving ABO discrepancies, how would O cells and an autocontrol help you? When would you use them?
20
New cards
Anti-A,B used to distinguish from O from A or B. Also can pick up weak subgroups of A
When resolving ABO discrepancies, when would you use Anti-A,B?
21
New cards
Using Anti-A,B in a discrepancy helps distinguish between Type A/B or O. Not useful if you have strong front type reactions because you use Anti-A,B to make weak reactions stronger. If it's already 4+, A,B won't help. O patient shouldn't have strong front type.
Would using Anti-A,B help you if you have strong reactions with Anti-A and/or Anti-B? Explain your answer
22
New cards
Trust the strongest reactions. NO not always the best approach because sometimes you have evidence of something else going on (patient history, etc). "Cold antibody" can look strong.
What's generally the "first rule" when beginning to troubleshoot a discrepancy? Is this always the best approach?
23
New cards
A2 cells used to distinguish between A or O/B.
A1-lectin pos, A2 cells neg--Type A1
A1-lectin neg, A2 cells neg--Subgroup of A
A1-lectin neg, A2 cells pos--Type O or B
Not react--A or AB
A1-lectin pos, A2 cells neg--Type A1
A1-lectin neg, A2 cells neg--Subgroup of A
A1-lectin neg, A2 cells pos--Type O or B
Not react--A or AB
Describe when you would use A2 cells. What type of patient do you expect to react with A2 cells? Not react?
24
New cards
anti-A,B
What reagent would you use to perform QC on reagent A2 cells?
25
New cards
anti-A1 lectin is used to differentiate A1 individuals from other A subgroups in the ABO grouping system. anti-A1 lectin will react with A1 cells only, whereas other A subgroups will all be non-reacting (0). This could help solve an unexpected reverse type discrepancy.
What is the purpose of anti-A1 lectin? Explain when you would choose to use it and what results you would expect in your scenario. How would it help you in solving a discrepancy?
26
New cards
a. in vivo
DAT detects ______ sensitization of RBCs
a. in vivo
b. in vitro
a. in vivo
b. in vitro
27
New cards
washed patient cells and saline to rule out spontaneous agglutination
what control is used for a DAT?
28
New cards
- increase incubation time, re-spin, and re-read
- add 2 extra drops of serum
- if neither of those work, you can do AC or O cells
- add 2 extra drops of serum
- if neither of those work, you can do AC or O cells
how do you handle missing reactions in the reverse type?
29
New cards
- run AC and O cells
- if both neg, run anti-A1 lectin and A2 cells
- rule out rouleaux
- if both neg, run anti-A1 lectin and A2 cells
- rule out rouleaux
how do you handle unexpected positives in the reverse type?
30
New cards
rule out spontaneous agglutination with DAT
- rule out rouleaux
- double check patient history and diagnosis
- polyagglutination, acquired B, cord blood, etc.
- rule out rouleaux
- double check patient history and diagnosis
- polyagglutination, acquired B, cord blood, etc.
how do you handle unexpected reactions in the forward type?
31
New cards
What cells are used in Antibody Screens?
Commercial single-donor O cells
32
New cards
Clinically significant antibodies react strongest at which phase?
IAT
33
New cards
What is the goal in performing an antibody screen on the patient? Why is this important in transfusions?
Goal is to identify UNEXPECTED, non- ABO antibodies that a patient may have in plasma. It is important to transfuse antigen neg blood to patient with corresponding antibody to avoid transfusion reactions.
34
New cards
Explain at what point in the antibody screen procedure you will add enhancement reagents. How much will you add?
Immediately prior to 37 incubation. Add same drops enhancement as plasma. (2)
35
New cards
Explain why you never stop an antibody screening procedure at IS.
Clinically significant antibodies react at IAT and may not react at IS.
36
New cards
What percent of cell suspensions are used in antibody screening using the gel method? How much volume of cells and plasma are added to the gel card?
0.8%.
50uL cells 25uL plasma.
50uL cells 25uL plasma.
37
New cards
Why is it recommended to wait for the results of E typing before typing for e?
Conservation of anti-e sera due to expenses.
38
New cards
What two requirements must be met for a donor unit of pRBC's selected for transfusion to patients with clinically significant antibodies?
1. crossmatch compatible at IAT
2. antigen negative for antibodies
2. antigen negative for antibodies
39
New cards
What is the importance of antigen testing a patient for antigens to which you think a patient has antibodies to?
Antigen test patient to see if they are capable of making suspected antibodies.
40
New cards
Explain the difference between abbreviated and full crossmatches and what type of patients qualify for each type.
A full crossmatch tests recipient plasma against donor cells using an IAT method. This is commonly for people who have a positive screen and are getting transfusions.
The abbreviated version is for people who test negative during the screen and record review. This version only carries the crossmatch through the immediate spin phase.
The abbreviated version is for people who test negative during the screen and record review. This version only carries the crossmatch through the immediate spin phase.
41
New cards
Compare the procedural differences between PeG and LISS methods for screen/ID.
PeG: there is no 37°C centrifugation step; only IS and IAT.
LISS: Includes IS, 37°C, and IAT phase.
LISS: Includes IS, 37°C, and IAT phase.
42
New cards
Why would a tech choose to use PeG instead of LISS in an antibody workup?
PeG more sensitive at pickup of weak, warm, Kidd antibodies.
43
New cards
In the DAT gel procedure, what is the percent cell suspension used? What is the source of cells? How does the procedure differ from the Antibody Screen done in gel?
A 0.8% cell suspension is taken from packed RBCs. from patient, in both the DAT and screening gel procedures.
- For the DAT, the 0.8% suspension is added into the gel cartridge (which includes anti- C3d and anti- IgG). There is no incubation step that the gel card goes directly to centrifuging step.
- For the ABY screen, a 0.8% is used again. The suspension is added to the anti-IgG cartidge (theres no anti-C3d). The gel card must incubate at 37°C for 15-40 minutes, then centrifuge.
- For the DAT, the 0.8% suspension is added into the gel cartridge (which includes anti- C3d and anti- IgG). There is no incubation step that the gel card goes directly to centrifuging step.
- For the ABY screen, a 0.8% is used again. The suspension is added to the anti-IgG cartidge (theres no anti-C3d). The gel card must incubate at 37°C for 15-40 minutes, then centrifuge.
44
New cards
How would you perform donor reconfirmation on a Bneg unit? What results would you expect?
A Bneg unit would receive confirmation with anti-A, anti-B, and anti-D. You would expect a strong reaction (4+) with anti-B, and a negative (0) reaction with anti-A and anti-D.
45
New cards
Provide 2 reasons why you would get variable reactivity strength on an antibody ID panel
1) multiple antibodies
2) one antibody displaying dosage
2) one antibody displaying dosage
46
New cards
Describe the differences in grading procedures/interpretation between Gel and Solid Phase technologies when performing antibody screens
GEL
- Gels are graded based on where the RBCs fall in terms of the tube. If at the very top, this is a strong positive and is a 4+. When there are some cells at the top, and some in the upper portion, this is a 3+. a 2+ is when the cells and suspended throughout the gel. a 1+ is when the cells are suspended in the lower portion of the gel with a visible button at the bottom. Negative (0) is when all cells are suspended at the bottom. Mf can occur when there is cells at the top and cells at the bottom
SOLID
- a positive reaction (4+) is shown when there is presence of RBC adherence to the monolayer with no visible button. a 3+ is when there is strong degrees of adherence to the monolayer (about 3/4ths), but can still have somewhat of a button in the middle. 2+ reactions resemble a large hole/blister where the RBCs are in the middle. A 1+ looks like a 'fuzzy button' in the middle for the RBCs while only 1/4th RBCs adhere to the monolayer. a negative reaction (0) is shown when there is no RBC adherence
- Gels are graded based on where the RBCs fall in terms of the tube. If at the very top, this is a strong positive and is a 4+. When there are some cells at the top, and some in the upper portion, this is a 3+. a 2+ is when the cells and suspended throughout the gel. a 1+ is when the cells are suspended in the lower portion of the gel with a visible button at the bottom. Negative (0) is when all cells are suspended at the bottom. Mf can occur when there is cells at the top and cells at the bottom
SOLID
- a positive reaction (4+) is shown when there is presence of RBC adherence to the monolayer with no visible button. a 3+ is when there is strong degrees of adherence to the monolayer (about 3/4ths), but can still have somewhat of a button in the middle. 2+ reactions resemble a large hole/blister where the RBCs are in the middle. A 1+ looks like a 'fuzzy button' in the middle for the RBCs while only 1/4th RBCs adhere to the monolayer. a negative reaction (0) is shown when there is no RBC adherence
47
New cards
How would you QC anti-Jkb antisera?
Use a known positive Jkb and a known negative Jkb to run alongside patients once every 24 hours. We use CorQC and Saline in lab.
48
New cards
In your own words, describe the principle of Solid Phase technology
Essentially it seems like we are adding RBC antigens to the bottom of the microtiter plate. Then, we are adding in patient serum/plasma. If there is binding to create an ABY/AGN complex, leftover ABY will washed away. If there is no binding (a neg test), the ABY will be washed away (after the incubation step). After the washing step, we are adding in indicator anti-IgG coated cells. When we centrifuge this, it will bring the IC in contact with the patient serum ABYs (that are attached to the RBC membrane-bound AGNS). In a positive test, the IC will be impeded/stopped bc of the anti-IgG and IgG complexes, this causes the indicator cells to bind to the screening cells at the bottom. In a negative test, the ABY from the patient would have never bound to the AGN on the titer plate, been washed away, and then the indicator cells would have centrifuged to the bottom and created a button without a problem
49
New cards
How do PeG and LISS work?
LISS (low ionic strength solution) works by canceling out the negative zeta potential that RBCs have
PeG works by removing H2O molecules which allows small IgG abs and RBCs to come into contact together
PeG works by removing H2O molecules which allows small IgG abs and RBCs to come into contact together
50
New cards
why do we not spin PeG after the 37° stage?
can cause anomalous precipitation of plasma proteins (spontaneous agglutination)
51
New cards
List the screens in order from the most sensitive to the least
SP/Gel > PeG > LISS > Albumin
52
New cards
unexpected antibodies are found in _____% of the population
0.3-3.0%
53
New cards
Explain why intact RBC's in urine are not indicative of a HTR?
An HTR is an intravascular hemolytic reaction, therefore intact RBCs would not be in the urine (free hgb would be)
54
New cards
provide 2 circumstances where an elution may be performed
1. identify ABYs that are coating cells of a patient with a positive DAT
2. isolate specific antibodies from plasma
2. isolate specific antibodies from plasma
55
New cards
explain the purpose of the last wash in an elution. What do we do with the last wash sample that's collected and why?
The last wash is to assure that the washing was adequate to remove unbound aby . We do this to detach the ABYS from the RBC and then keep the last wash to test it to assure the washing was adequate.
56
New cards
D frequency
85
57
New cards
C frequency
70
58
New cards
E frequency
30
59
New cards
c frequency
80%
60
New cards
e frequency
98%
61
New cards
Jk(a) frequency
77
62
New cards
Kell frequency
9
63
New cards
k frequency
99
64
New cards
Fy(a) frequency
66
65
New cards
Fy(b) frequency
83
66
New cards
A frequency
40
67
New cards
B frequency
11
68
New cards
O frequency
45
69
New cards
AB frequency
4
70
New cards
Major crossmatch
Donor RBC vs recipient serum
71
New cards
Minor Crossmatch
Donor serum vs recipient RBC