UNIT 2 EXAM
1/26
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
27 Terms
What are “locus” and “focus” and why are they important?
Two treatment approaches
Restore lost fx: Involves an effortful swallow or the Masako maneuver, which involves moving the tongue all the way forward past the teeth and swallowing your saliva. This is meant to strengthen the muscles in the throat and improve swallowing functions.
Compensate for lost fx: Effortful swallow, altered consistencies based on the IDDSi scale, and a secondary swallow to clear residue.
Functional etiology: what is muscle tension dysphonia?
• Strained vocal quality
resulting from increased
laryngeal muscle tension
-can be psychological and caused by stress
Vocal misuse leads to what?
a. Nodules-growths that are formed on the vocal cords (not cancerous) BREATHINESS AND LOWER PITCH
b. Cysts-hardened growth on the vocal cords containing fluid (benign)
c. Edema-swollen vocal folds causing a deeper or raspy voice, thick and heavy vocal folds cause by misuse or acid reflux. (benign) LOWERED PITCH
d. Polyps-damage to the labia propria of the VFs that can be sessile or pedunculated. It can look like a blister on the vocal folds. Can be hemorrhagic, translucent, or fibrotic. BREATHINESS AND LOWER PITCH
e. Hyperemia-inflammation of the vocal folds which can appear red
Hemorrhage of Vocal Folds (VFs)
Organic: what are some neurogenic voice disorders?
Caused by damage to the nervous system.
○ Vocal Fold Bowing
■ Parkinson’s Disease (primary) MONOPITCH
■ (non-neurogenic: age-related)
○ Paresis / Paralysis of VF (unilateral or bilateral)
■ Nerve damage (CN X)
■ Amyotrophic Lateral Sclerosis
■ Primary Lateral Sclerosis
○ Paresis / Paralysis of Velum
■ Nerve damage (CN IX)
■ Amyotrophic Lateral Sclerosis
■ Primary Lateral Sclerosis
○ Spasmodic Dysphonia VOCAL STRAIN/STRUGGLE
■ Adductor Spasmodic Dysphonia
■ Abductor Spasmodic Dysphonia
What is a neoplasm?
Laryngeal neoplasms are cancer located in the vocal cords and involve growths in the vocal cords.
What are the parts of an assessment?
Subjective Assessment: entails listening
and observing the patient while they
are speaking. (how does it effect them?)
Includes:
• Voice History Form (a.k.a. Intake or
Case History) -possible things that stress them out or an event that happened, divorce,etc.)
• Voice-Related Quality of Life Scale
(Likert Scale)
• Voice Quality Rating (e.g., GRBASI
Scale)
• Observation of Body Movements
• posture
• Objective Measurements using Voice Analysis Software (e.g., PRAAT)
• Jitter: amount of variation from average F0 (in Hz)
• Shimmer: amount of variation from average amplitude (in dB)
• CPP (Cepstral Peak Prominence): variation from average frequency
• Vizualization of Vocal Anatomy
• Indirect and Direct Laryngoscopy
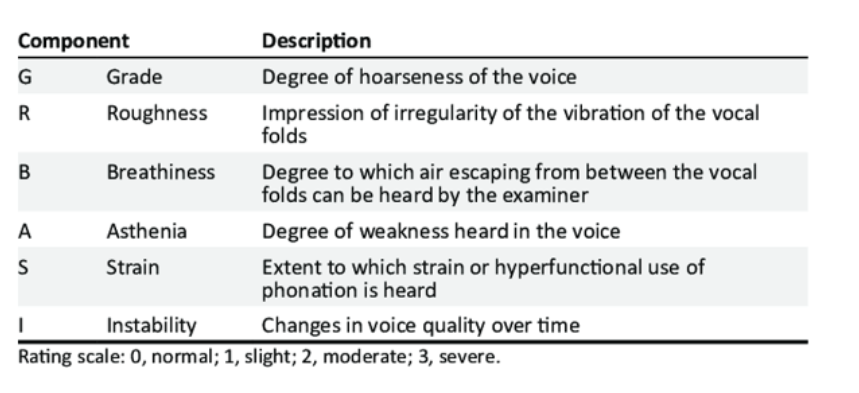
What is the GRBASI scale?
Stands for grade, roughness, breathiness, asthenia, strain, and instability. REFER TO IMAGE FOR EXPLANANTION
Diagnosis What are some symptoms?
-breathiness, lowered pitch,
-monopitch and reduced loudness
-hoarseness, strain/struggle
Treatment: What are some treatment options for vocal disorders?
Forms of direct therapy
LSVT (Lee Silverman voice treatment): Involves intensive effort to increase loudness. Common for Parkinsons. Patients increase loudness in order to help others understand what they’re saying and create stronger communication.
SOVT (Semi-occluded vocal tract exercises): Increase back pressure by obstructing the vocal tract, which helps the vocal cords vibrate more efficiently. (straw exercise)
-Narrowing the mouth builds positive air pressure
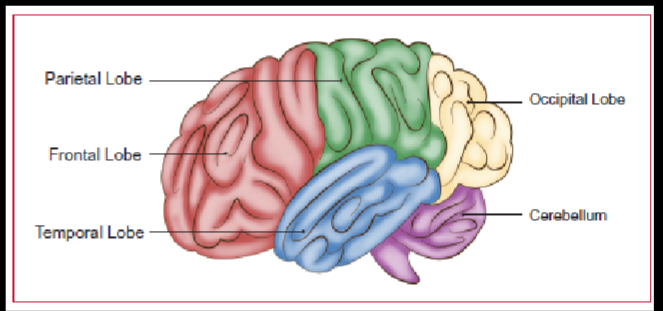
Parts of the brain
• Nervous System: central and peripheral
• Frontal Lobes: important in the planning of
physical movement.
Broca’s Area: speech production
• Temporal Lobes: important for perception
Wernicke’s Area: speech comprehension
Heschl’s gyrus: primary auditory center
• Parietal Lobes: process incoming sensory
information.
• Occipital Lobes: process of incoming visual
information.
Brodmanns areas for Broca and Wernicke’s area
-44-45 Brocas area
-22 Wernickes area
What are the fluent types of aphasia? Symptoms and etiologies?
1. Wernicke’s: Very wordy speech, and from a distance it may seem okay, but once you come closer, the speech doesn’t make sense. Sentences have no meaning, and words can be made up. Sounds like a sentence, but there’s no content. ETIOLOGY: damage to Wernicke’s area of the brain due to possible accidents such as a TBI and stroke (CVA)
2. Anomic: Difficulty naming words, patients tend to produce grammatically correct yet empty speech, and language comprehension tends to be preserved. ETIOLOGY: stroke (CVA) or a traumatic injury
3. Conduction: Difficulty repeating words or phrases back to someone but doesn’t affect the ability to understand others.
ETIOLOGY: stroke
What are some non fluent aphasia types?
1. Broca’s: Broken speech and may struggle to say words and form a sentence. Omit small words such as “is” “and” “the”. Can be easily frustrated by it due to being aware. ETIOLOGY: damage to brocas area of the brain, TBI or a stroke
2. Global: May be nonverbal or use facial expressions/gestures to communicate. May understand some words. ETIOLOGY: stroke, TBI, or tumor.
What are some right hemisphere disorder symptoms?
Damage to the right side of the brain and includes:
Word retrieval difficulty, sometimes using the incorrect word.
Poor topic maintenance during a conversation, including turn-taking.
Difficulty understanding and appreciating word-based humor.
Misinterpretation of sarcasm.
Flat affect or inappropriate emotional expression
Flat/monotonous prosody (aprosodia)
Poor nonverbal communication, such as facial expression or body language.
Problems recognizing faces (prosopagnosia), leading to awkward
communication exchanges.
Visuospatial difficulties affecting reading and writing.
Problem solving difficulties.
Decreased awareness or insight of their communication difficulties.
Why is it important to get a baseline function?
It determines the patients speech abilities and evaluates their skills such as speech sounds. It helps measure progress and helps the slp know their notes and goals
What is Boston Diagnostic Aphasia Exam?
Boston Diagnostic Aphasia Exam-Diagnoses aphasia and looks for specific symptoms
1. Word-naming (tests for Anomia)
2. Repetition
3. Expressive Language (morphological and sentence structure)
4. Receptive Language (comprehension)
Differential diagnosis between apraxia and dysarthria
How are they different?
Dysarthria involves an effect on muscle tone or function, while apraxia affects the individual’s neural control of those muscles. Dysarthria is NEUROMUSCULAR, and apraxia is NEUROLOGIC.
Dysarthria-
Etiologies: Parkinsons disease, multiple sclerosis, and amyotrophic lateral sclerosis.
Symptoms: Slurred or slow speech
Apraxia-brain doesn't communicate properly with muscles
Etilogies: stroke, TBI, (childhood: genetic or neurological impairment)
Symptoms: pauses and unclear vowels/consonants. Sound substitutions and sound additions.
Treatment: sound sequencing and Dynamic temporal and tactile cueing, and prompt.
What are some ways we can assess to determine if it is apraxia, for example
1. Varied utterance length (looking for more errors in longer utterances)
2. Look for inconsistent errors
-rule out muscle weakness or language comprehension problems
What are the types of dysarthria?
Hyperkinetic (e.g., Huntington’s Disease & Tardive Dyskinesia)
a. Basal ganglia damage
SYMPTOMS: problems with involuntary movement and unpredictable speech/variation of loudness.
TREATMENT: LSVT LOUD
2. Hypokinetic (e.g., Parkinson’s Disease)
a. Substantia nigra – dopamine production
SYMPTOMS: Monotone speech pattern or quiet
TREATMENT: Motor learning intensive practice
3. Spastic (e.g., Cerebral Palsy)
a. Upper motor neuron damage
SYMPTOMS: Problems with executing fine motor movements and slowed or strained speech.
TREATMENT: LSVT LOUD
4. Flaccid (e.g., Guillain-Barre Syndrome)
a. Lower motor neuron damage
SYMPTOMS: Problems with vocal fold movement (paralysis) involve breathiness and hypernasality.
TREATMENT: Motor learning intensive practice
5. Ataxic (e.g., Friedrich’s Ataxia)
a. Cerebellar damage
SYMPTOMS: Problems with regulating force, timing, rhythm, speed, and overall coordination of movement. Slurred speech and trouble swallowing.
TREATMENT: Motor learning intensive practice
6. Mixed
a. E.g., Mixed Spastic-Flaccid (e.g., ALS, a.k.a. “Motor Neuron Disease” –
why?)
SYMPTOMS: Associated with motor degenerative diseases such as Lou Gehrig's disease. Strained vocals and slurred speech
TREATMENT: Motor learning intensive practice
What are the anatomical parts related to swallow and their function?
i. Cricopharyngeal muscle and the UES:
ii. Epiglottis:
iii. Anterior faucial pillars (what muscles are these?): The palatoglossus and the palatopharyngeus. The palatopharyngeal arch raises the back of the tongue, while the palatoglossal arch helps raise the larynx and pharynx.
What are the phases of the swallow?
1.Oral Phase
Food/drink enters oral cavity
Manipulation of lips, jaw, tongue
Mastication (chewing)
Manipulation of food to grinding
surface (jaw, cheeks, tongue, and teeth)
-Oral transport: bolus forms and mastication stops
-tongue dorsum lowers
2. Pharyngeal Phase
Bolus makes contact with anterior faucial pillars
Involuntary initiation of pharyngeal swallow (automatic)
Velum elevates (levator veli palatini)
Tongue activity continues to propel
bolus toward pharynx and
esophagus
3. Esophageal Phase
UES is sealed after bolus passes
through
Peristaltic movement of bolus
toward LES, muscles of LES then
relax to allow bolus to move into
the stomach.
What is penetration and aspiration? Compare them
Penetration is when the bolus enters the airway but not below the true vocal folds. (can be cleared by a cough). Aspiration is when the bolus passes through below the true vocal folds and enters the breathing airway.
What is VFSS/MBSS? What can you see and how is it performed?
What is FEES What can you see and how is it performed?
What are some compensatory strategies?
i. Effortful Swallow
ii. Thickening thin liquids
What are some rehabilitative/restorative stratgesis?
i. Masako maneuver