Disorders of the Adrenal Gland
1/74
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
75 Terms
What does the zona glomerulosa secrete?
Mineralocorticoids (Aldosterone)
What does the zona fasciculata secrete?
Glucocorticoids (Cortisol)
What does the zona reticularis secrete?
Gonadocorticoids (DHEA)
What is the significance of DHEA in females?
It is a major source of androgens, contributing to 40-75% of testosterone production.
What does the adrenal medulla secrete?
catecholamines (epinephrine and norepinephrine)
What is the function of aldosterone?
Controls body fluid volume, electrolyte balance, and vascular resistance.
What is the role of cortisol?
Regulates metabolism, protects against hypoglycemia, and suppresses the immune response.
What is the HPA axis?
The hypothalamic-pituitary-adrenal axis, which regulates the stress response.
How is ACTH produced?
Produced by the pituitary gland and stimulates production of cortisol with diurnal variation (AM > PM)
What is the purpose of the Plasma ACTH test?
Collected with serum cortisol to differentiate the source of adrenal insufficiency from primary (adrenal), secondary (pituitary), and tertiary (hypothalamic)
What is a 24 hour urine free cortisol test used for?
Measures quantity of free cortisol collected; Ideal for suspected hypercortisolism
What is the ACTH Stimulation test used for?
utilizes cosyntropin to differentiate source of adrenal insufficiency
What result of an ACTH stimulation test indicates adrenal insufficiency?
a subnormal response of cortisol level
What is the Dexamethasone suppression test used for?
To confirm abnormal excess production of cortisol.
What result of a Dexamethasone suppression test indicates a functioning adrenal gland?
suppressed cortisol level
What is the most common cause of Cushing Syndrome (Hypercortisolism)?
Long term high-dose glucocorticoid use (Exogenous/iatrogenic)
What are endogenous causes of Cushing Syndrome?
Pituitary adenoma (MC endogenous cause; AKA Cushing Disease), Ectopic ACTH-producing tumor, and Adrenal Tumor
What falls under the classification of ACTH- dependent hyperfunction?
Cushing disease (pituitary adenoma), Ectopic ACTH, and administration of exogenous ACTH
What falls under the classification of ACTH- independent hyperfunction?
Therapeutic administration of corticosteroids and adrenal tumors (adrenal adenoma or carcinoma)
What are common clinical manifestations of Cushing syndrome?
Weight gain, fatigue, proximal muscle weakness, hypertension, insulin resistance, and purple abdominal striae >1cm wide
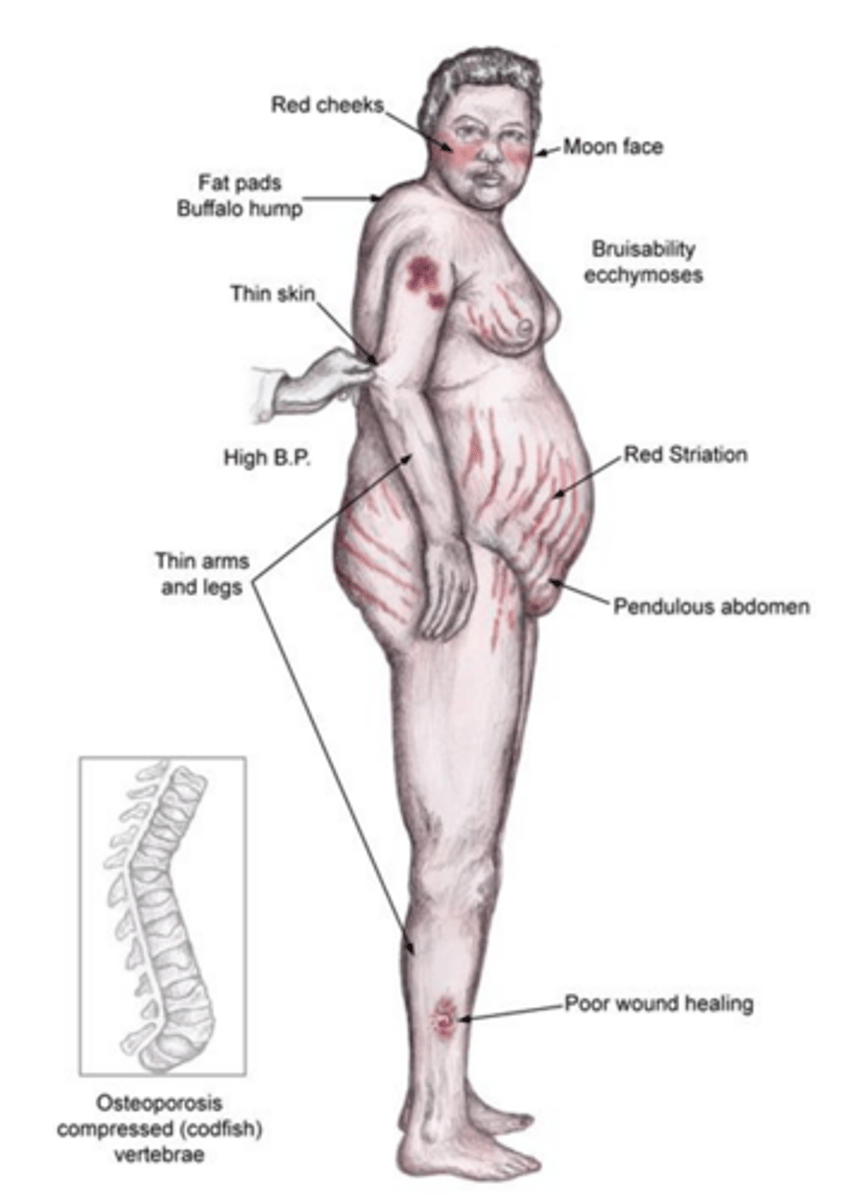
What are the manifestations of weight gain in Cushing Syndrome?
Truncal obesity, moon face, supraclavicular fat pad, and cervical fat pad (buffalo hump)
What are the other systemic symptoms of Cushing Syndrome?
Hirsutism, amenorrhea, osteoporosis, thin skin, acanthosis nigricans, impaired wound healing, depression, and paranoia
What should be done if you have clinical suspicion of Cushing Syndrome?
Exclude exogenous glucocorticoids
What laboratory evaluations are used in diagnosing Cushing Syndrome?
CBC (leukocytosis), CMP (hyperglycemia), and lipid panel.
What screening tests are used for Cushing Syndrome?
- 24-hr urinary free cortisol: + if elevated (most specific with 2 measurements)
- Nighttime salivary cortisol: + if elevated on 2 separate nights
- Low dose Dexamethasone Suppression test: + if no change in cortisol
What is the only screening test that determines an endogenous cause?
Low dose Dexamethasone Suppression test
What secondary testing is used in Cushing Syndrome?
Baseline plasma ACTH + High-dose Dexamethasone suppression test
What does a baseline plasma ACTH level <10 suggest?
It suggests an adrenal tumor (high cortisol with low ACTH)
What does a baseline plasma ACTH level >20 at 8am suggest?
Pituitary adenoma (Low Cortisol, High ACTH) or Ectopic tumor (High Cortisol and ACTH)
What imaging is used for suspected Cushing disease?
Pituitary MRI with and without contrast (Cushing disease), Abdominal CT (adrenal tumor), CXR and pelvic ultrasound (Ectopic ACTH)
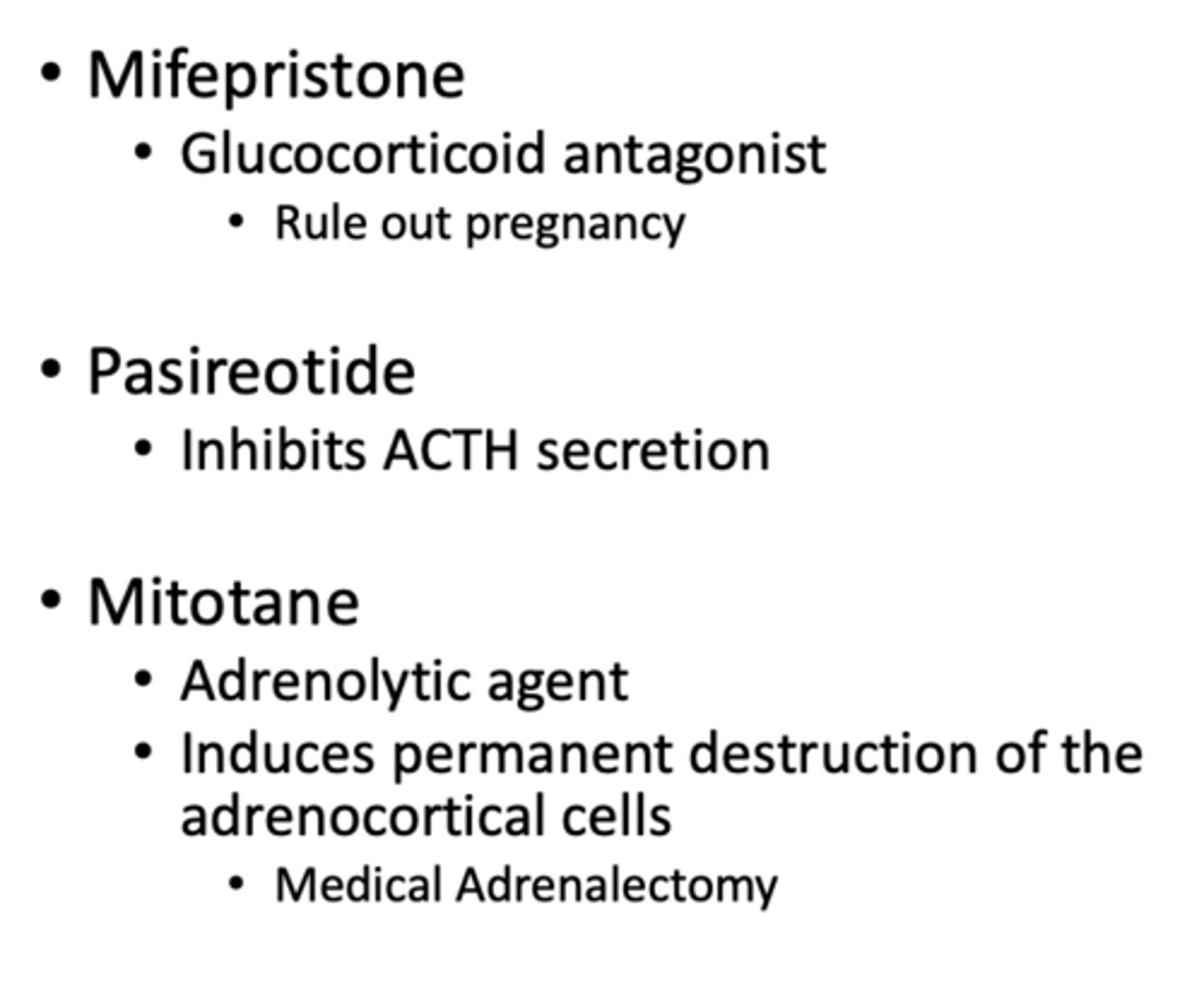
What is the treatment for Cushing disease or pituitary adenoma?
1. Pasireotide + Mifepristone
2. Transsphenoidal resection + Mifepristone
What is the treatment for Adrenal Tumor?
Tumor resection; Potential for iatrogenic adrenal insufficiency needing replacement therapy
What is the treatment for Ectopic ACTH production?
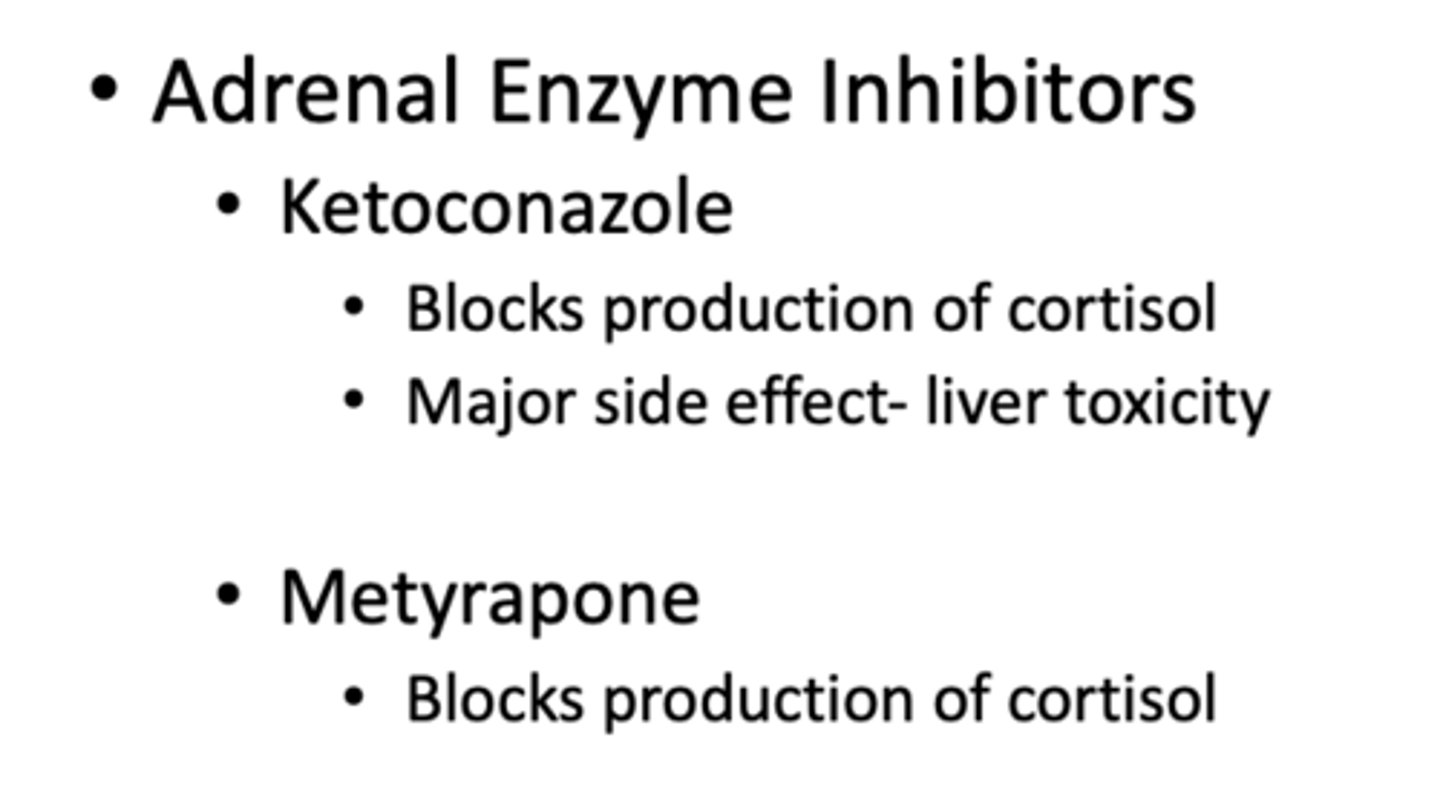
Resect tumor if possible otherwise try Ketoconazole or Metyrapone
What is the most common causes of primary adrenal insufficiency?
Addison disease (US) or Tuberculosis (worldwide)
What medication can cause adrenal insufficiency?
Ketoconazole, Rifampin, Phenytoin, Barbiturates
What are the causes of secondary adrenal insufficiency?
Exogenous glucocorticoid use (MC), Pituitary failure of ACTH secretion, and Hypopituitarism
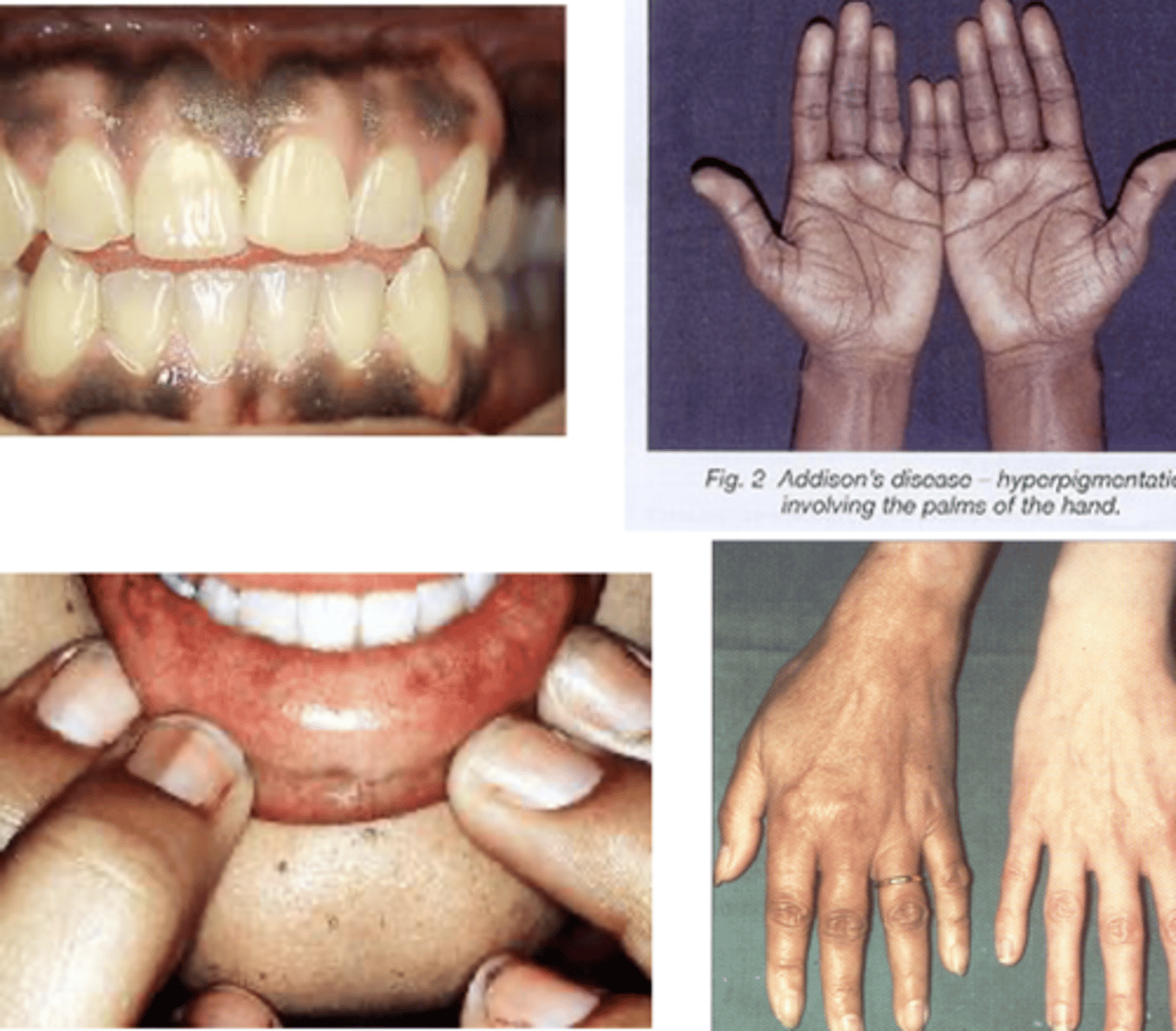
What are the hallmark symptoms of adrenal insufficiency?
Weakness/fatigue, weight loss/anorexia, hyperpigmentation (most characteristic), and hypotension.
What does hyperpigmentation in adrenal insufficiency indicate?
It is driven by elevated ACTH levels (POMC precursor and MSH) leading to darkening of non-sun exposed areas (skin creases, pressure areas, and mucous membranes)
What are more systemic symptoms of adrenal insufficiency?
HA, salt cravings, low libido, amenorrhea, loss of axillary pubic hair
What laboratory findings are indicative of adrenal insufficiency?
Hyperkalemia, hyponatremia, and fasting hypoglycemia.
What does a low serum cortisol level (<3 mg/dL) indicate?
very likely that the patient has adrenal insufficiency
What does an ACTH stimulation test result of less than 18 mcg/dL indicate?
It indicates adrenal insufficiency
What is the treatment for primary adrenal insufficiency?
Glucocorticoid replacement (Hydrocortisone 5-10mg BID or TID) and mineralocorticoid replacement (Fludrocortisone 0.1-0.2 mg daily)
What is the treatment for secondary adrenal insufficiency?
Only needs glucocorticoids
What is an adrenal crisis?
an emergency state due to extremely low levels of cortisol often precipitated by a "stressful" event
What are the most common causes of adrenal crisis?
Abrupt withdrawal from glucocorticoids without tapering (MC), Sheehan syndrome (postpartum pituary necrosis), and Waterhouse-Fredrichsen Syndrome
What are common clinical manifestations of adrenal crisis?
Shock, acute abdominal/low back pain, N/V/D, fever, dehydration, and altered mental status.
What is the treatment for adrenal crisis?
Immediate administration of isotonic IV fluids (D5N5 or normal saline over 1-2 hours) and glucocorticoids (IV Hydrocortisone 100mg injected over 30 seconds, repeated 6-8hrs)
What is managed after stabilization of adrenal crisis with fluids and glucocorticoids?
Reversal of electrolyte disorders and Fludrocortisone
What are the most common causes of primary hyperaldosteronism?
Adrenal cortical hyperplasia (MC) and Adrenocortical adenoma (Conn's Syndrome)
What is the pathophysiology of primary hyperaldosteronism?
sodium retention and renal potassium & hydrogen ion wasting
What are the clinical exam findings of primary hyperaldosteronism?
Proximal muscle weakness, polyuria, polydipsia, ↓ DTR, HA, facial flushing, and blurred vision
What triad of findings is associated with primary hyperaldosteronism?
Hypertension, hypokalemia, and metabolic alkalosis.
What is the best initial screening test for primary hyperaldosteronism?
Plasma renin and plasma aldosterone levels (ARR > 20:1)
What are the confirmatory tests for primary hyperaldosteronism?
Oral sodium loading test, saline infusion test (>10ng/dL), Fludrocortisone suppression test, and Captopril challenge test
What imaging is used in primary hyperaldosteronism after confirmatory test?
CT or MRI to look for mass followed by adrenal venous sampling
What is the treatment of primary hyperaldosteronism?
Spironolactone +/- Surgical removal of adenoma, antihypertensive agents
What is a pheochromocytoma?
A rare tumor arising from chromaffin cells that secretes catecholamines.
What are the risk factors for pheochromocytoma?
MEN 2 and neurofibromatosis
What are the classic symptoms of pheochromocytoma?
Hypertension, palpitations, headache, and excessive sweating.
What are some precipitating factors of pheochromocytoma "attacks"?
palpation of tumor, posture change, abdomen compression, anesthesia, emotional trauma, pregnancy, caffeine
What is the initial study of choice for diagnosing pheochromocytoma?
Biochemical testing for metanephrines (catecholamine metabolite) using a 24 hour urine screen or plasma metanephrine
What imaging is used in pheochromocytoma diagnosis?
- MRI or noncontrast CT of abdomen and pelvis
- Metaiodobenzylguanidine (MIBG) scintigraphy
What is the order of management for pheochromocytoma?
1) Nonselective alpha blocker (Phenoxybenzamine or Phentolamine)
2) Beta Blocker or CCB
3) Surgical resection once stabilized (1-3 weeks of medical therapy
What is an adrenal incidentaloma?
A mass lesion greater than 1 cm discovered incidentally by radiologic examination.
What are the risk factors of adrenal incidentaloma?
Obesity, Hypertension, and diabetic
What is the MRI presentation of a benign adrenal incidentaloma?
Homogenous, unilateral, <4cm, lipid-rich, rapid contrast wash out, isointensity compared to liver on T1 and T2
What is the MRI presentation of an adrenal incidentaloma carcinoma?
Inhomogeneous with central necrosis, Unilateral, >4cm, Calcifications, Delayed wash out, Hypointensity on T1, High signal intensity on T2
What is the MRI presentation of an adrenal incidentaloma metastases?
Inhomogeneous, irregular shape, bilateral, low lipids, delayed wash out, Isointensity on T1, Intermediate signal intensity on T2
What is the first step in the workup of an adrenal incidentaloma?
Measure serum cortisol, ACTH, DHEA, and aldosterone.
When is a FNA with biopsy indicated for adrenal incidentaloma?
Known primary malignancy elsewhere
When is a FNA with biopsy NOT indicated for adrenal incidentaloma?
Biochemical evidence of pheochromocytoma and known widespread metastatic disease
What is the managment for a documented pheochromocytoma or carcinoma?
Surgical intervention
What is the typical management for a benign adrenal incidentaloma > 2 cm?
Consider resection; Repeat Dexamethasone suppression test annually for 4 years
What is the typical management for a benign adrenal incidentaloma < 2 cm?
Repeat imaging in 6 months; consider additional imaging at 12 and 24 months with repeat dexamethasone suppression test x 4 years