Pulmonary Pathophysiology
0.0(0)
Studied by 0 peopleCard Sorting
1/65
Last updated 7:44 PM on 12/6/22
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
66 Terms
1
New cards
What is COPD?
Chronic Obstructive Pulmonary Disease (COPD) describes airflow limitation that is not fully reversible. Emphysema and Chronic Bronchitis both result from damage to the lungs over many years and predominantly affect former and current smokers. They are the most common causes of respiratory failure.
2
New cards
COPD High Risk Populations
All smokers 45 y.o. and older
Past smokers with a 20--pack year hx of smoking
Pt's w/ recurrent or chronic respiratory sx including cough and breathlessness on exertion.
Pt's w/ family hx of COPD
Pt's w/ significant occupational exposure to respiratory irritants.
Past smokers with a 20--pack year hx of smoking
Pt's w/ recurrent or chronic respiratory sx including cough and breathlessness on exertion.
Pt's w/ family hx of COPD
Pt's w/ significant occupational exposure to respiratory irritants.
3
New cards
X-ray findings of COPD
Flattened diaphragm, Increased A-P distance, Vertical heart.
Lungs are large and hyperinflated
Signs of hyperinflation may be seen in emphysema, chronic bronchitis and asthma.
Lungs are large and hyperinflated
Signs of hyperinflation may be seen in emphysema, chronic bronchitis and asthma.
4
New cards
Emphysema Etiology
Abnormal and permanent enlargement of the gas exchange airways. Destructive changes to the alveolar wall, without obvious fibrosis. Obstruction occurs as a result of changes in lung tissue and loss of elastic recoil.
Alveoli collapse during expiration.
Obstructive
Alveoli collapse during expiration.
Obstructive
5
New cards
Emphysema S&Sx
Genetics: Alpha-1 antitrypsin deficiency
Air pollutants
Infection
Cigarette smoking
May be called "pink puffers"
Malnourished
Cachexia: Weakness and wasting of the body due to sever chronic illness.
Air pollutants
Infection
Cigarette smoking
May be called "pink puffers"
Malnourished
Cachexia: Weakness and wasting of the body due to sever chronic illness.
6
New cards
Chronic Bronchitis Etiology
Chronic cough lasting longer than three months for 2 consecutive years.
-Airways become swollen and partially clogged w/ mucous.
-May have mm spasms in the airways.
-Most common cause is smoking.
-Chronic inflammation of the bronchial mucosa. Airway narrowing. Decreased ciliary function.
Obstructive
-Airways become swollen and partially clogged w/ mucous.
-May have mm spasms in the airways.
-Most common cause is smoking.
-Chronic inflammation of the bronchial mucosa. Airway narrowing. Decreased ciliary function.
Obstructive
7
New cards
Chronic Bronchitis S&Sx
Described as "Blue Bloaters"
Spasmodic cough + sputum production
Chronic Bronchitis can lead to emphysema.
High incidence of infection d/t trapped secretions.
Spasmodic cough + sputum production
Chronic Bronchitis can lead to emphysema.
High incidence of infection d/t trapped secretions.
8
New cards
More Emphysema
Pink Puffer
-Low BMI
-Few co-morbidities
-Less mm mass
-Hyperinflation
-Low diffusion capacity for CO
-More dyspnoea
-Decreased exercise capacity
-Worst health status
-Low BMI
-Few co-morbidities
-Less mm mass
-Hyperinflation
-Low diffusion capacity for CO
-More dyspnoea
-Decreased exercise capacity
-Worst health status
9
New cards
Less Emphysema
Blue Bloater
-High BMI
-More co-morbidities
-Cardiac Compromise
-Less hyperinflation
-More chronic bronchitis
-Increased exacerbations
-More normal diffusion capacity
-High BMI
-More co-morbidities
-Cardiac Compromise
-Less hyperinflation
-More chronic bronchitis
-Increased exacerbations
-More normal diffusion capacity
10
New cards
Asthma Etiology
Inflammatory disorder of the airways characterized by periodic attacks of wheezing, SOB, chest tightness and/or coughing
Increased reactivity of the tracheobronchial tree to different stimuli.
Attacks may be relieved with medications and are episodic in nature.
Contributing factors: Environmental, genetic predisposition, diet, respiratory tract infections, ANS imbalance, Mucosal damage
Obstructive
Increased reactivity of the tracheobronchial tree to different stimuli.
Attacks may be relieved with medications and are episodic in nature.
Contributing factors: Environmental, genetic predisposition, diet, respiratory tract infections, ANS imbalance, Mucosal damage
Obstructive
11
New cards
Asthma S&Sx
-Episodes of bronchoconstriction resulting in wheezing and dyspnea.
-Nonproductive cough, prolonged expiration, Increased HR and breathing rate.
-Accessory mm use.
-May have inspiratory and expiratory wheezes.
-X-ray may show hyperinflation
-Nonproductive cough, prolonged expiration, Increased HR and breathing rate.
-Accessory mm use.
-May have inspiratory and expiratory wheezes.
-X-ray may show hyperinflation
12
New cards
Asthma Tx
Identification and avoidance of triggers
Sx Management
-Bronchodilator medication
-Anti-inflammatory meds
Sx Management
-Bronchodilator medication
-Anti-inflammatory meds
13
New cards
Bronchiectasis Etiology
Defined as permanent pathologic enlargement of airways (normal diameter > 2mm)
Results in fibrosis and ulceration of bronchioles, chronically retained secretions, atelectasis and infection.
Obstructive.
Results in fibrosis and ulceration of bronchioles, chronically retained secretions, atelectasis and infection.
Obstructive.
14
New cards
Bronchiectasis Mechanism: Bronchial wall injury/structural weakness of bronchial walls
Can occur following infection or inhalation accidents.
May be from genetic condition causing structural defects of the airway or abnormal mucociliary clearance.
Exaggerated immune response disorders.
May be from genetic condition causing structural defects of the airway or abnormal mucociliary clearance.
Exaggerated immune response disorders.
15
New cards
Bronchiectasis Mechanism: Traction froma adjacent lung fibrosis
Ex: Sarcoidosis or interstitial fibrosis
Airway pulled outward by local retractile forces resulting in fixed dilation of airways.
Airway pulled outward by local retractile forces resulting in fixed dilation of airways.
16
New cards
Bronchiectasis Mechanism: Bronchial Lumen Obstruction
Related to slow-growing tumors in airway. Could be due to fibrotic structures related to prior infection (TB).
Can develop pna or atelectasis distal to these obstructions.
Can develop pna or atelectasis distal to these obstructions.
17
New cards
Cylindrical Bronchiectasis
Smooth parallel bronchial walls that end squarely and abruptly, commonly seen after pna
18
New cards
Saccular Bronchiectasis
Bronchial dilation progressively increasing toward the periphery, may form honeycomb pattern, most severe.
19
New cards
Varicose Bronchectasis
Bronchi distorted and bulging
20
New cards
Bronchiectasis S&Sx
-May have recurrent URI's and copious secretions.
-Dyspne, fatigue, hypoxia
-Dec VC and expiratory flow rates
-Possible hemoptysis secondary to erosion of bronchial wall
-Auscultation: crackles over involved lobes. Rhonchi during periods of mucous retention. May have wheezing.
-Shallow breathing pattern common to avoid coughing. May caused diminished breath sounds
-Dyspne, fatigue, hypoxia
-Dec VC and expiratory flow rates
-Possible hemoptysis secondary to erosion of bronchial wall
-Auscultation: crackles over involved lobes. Rhonchi during periods of mucous retention. May have wheezing.
-Shallow breathing pattern common to avoid coughing. May caused diminished breath sounds
21
New cards
COPD Stage 1
Very Mild.
With a FEV1 about 80% or more of normal. Commonly, in this stage, COPD causes slight airflow limitation.
With a FEV1 about 80% or more of normal. Commonly, in this stage, COPD causes slight airflow limitation.
22
New cards
COPD Stage 2
Moderate.
With a FEV1 btwn 50-80% of normal. Usually, during this stage, most people seek help for COPD sx of coughing, wheezing and shortness of breath.
With a FEV1 btwn 50-80% of normal. Usually, during this stage, most people seek help for COPD sx of coughing, wheezing and shortness of breath.
23
New cards
COPD Stage 3
Severe.
Emphysema with FEV1 between 30-50% of normal. Typically, in this stage, COPD sx worsen, causing decreased quality of life.
Emphysema with FEV1 between 30-50% of normal. Typically, in this stage, COPD sx worsen, causing decreased quality of life.
24
New cards
COPD Stage 4
Very Severe.
With a lower FEV1 than Stage 3, or those with Stage 3 FEV1 and low blood oxygen levels. End stage COPD, meaning the disease has progressed, lung function has deteriorated and flare-ups could be life threatening.
With a lower FEV1 than Stage 3, or those with Stage 3 FEV1 and low blood oxygen levels. End stage COPD, meaning the disease has progressed, lung function has deteriorated and flare-ups could be life threatening.
25
New cards
BODE Index for COPD Survival Prediction
(B) BMI
(O) Airway Obstruction (FEV1)
(D) Dyspnea
(E) Exercise Tolerance (6MWT)
(O) Airway Obstruction (FEV1)
(D) Dyspnea
(E) Exercise Tolerance (6MWT)
26
New cards
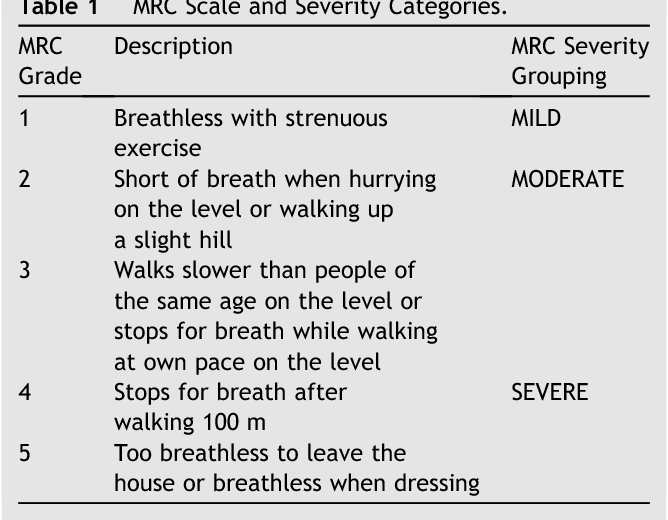
Dyspnea scale
27
New cards
Are there negative effects cognitively for COPD?
Memory Loss
Poor attention
Visual processing
Poor attention
Visual processing
28
New cards
Restrictive Lung Dysfunction
An abnormal reduction in pulmonary ventilation caused by the restriction of expansion by the chest wall or the lungs.
Lung expansion restricted, therefore volume of air moving in and out is decreased.
Lung expansion restricted, therefore volume of air moving in and out is decreased.
29
New cards
Atelectasis Etiology
Partial or total collapse of the alveoli, lung segments or lobes.
Commonly results from hypoventilation and decreased secretion clearance.
Restrictive
Commonly results from hypoventilation and decreased secretion clearance.
Restrictive
30
New cards
Causes and conditions that may contribute to atelectasis
Common Causes:
-Hypoventilation
-Compression
-Airway obstruction
-Adhesions
Conditions:
Inactivity
-Upper abdominal/thoracic incisional pain
-Compression of lung tissue
-Pneumonia
-Diaphragmatic Restriction
-Presence of a foreign body
-Hypoventilation
-Compression
-Airway obstruction
-Adhesions
Conditions:
Inactivity
-Upper abdominal/thoracic incisional pain
-Compression of lung tissue
-Pneumonia
-Diaphragmatic Restriction
-Presence of a foreign body
31
New cards
Pneumonia
Multi-staged inflammatory reaction of the distal airways. Typically begins with infection of the lower resp tract.
-Bacteria
-Viruses
-Foreign substances
-Gastric contents
-Fungi, mycoplasms
-Radiation therapy
-Pollutants/irritants
-Bacteria
-Viruses
-Foreign substances
-Gastric contents
-Fungi, mycoplasms
-Radiation therapy
-Pollutants/irritants
32
New cards
What are the four categories of Pneumonia?
Community Acquired
Healthcare Associated
Hospital Acquired (nosocomial)
Ventilator Associated (nosocomial)
Healthcare Associated
Hospital Acquired (nosocomial)
Ventilator Associated (nosocomial)
33
New cards
Pneumonia Presentation
-Dec lung volumes, Dec lung compliance, dec gas exchange, Inc work of breathing
-Dec PaO2, may have dec PaCO2 if hyperventilating.
-May have bronchial sounds above lobnar pna, absent breath sounds over pna and dull to mediate percussion.
-May have bubbling rales, rhonchi, dec or absent sounds, egophony, whispering pectoriloquy
-Dec PaO2, may have dec PaCO2 if hyperventilating.
-May have bronchial sounds above lobnar pna, absent breath sounds over pna and dull to mediate percussion.
-May have bubbling rales, rhonchi, dec or absent sounds, egophony, whispering pectoriloquy
34
New cards
Pneumonia S&Sx
Bacterial
-high fever, chills, dyspnea, Inc RR, productive cough, pleuritic pain
Viral
-Moderate fever, dyspnea, Inc RR, nonproductive cough, myalgias
-high fever, chills, dyspnea, Inc RR, productive cough, pleuritic pain
Viral
-Moderate fever, dyspnea, Inc RR, nonproductive cough, myalgias
35
New cards
Viral vs Bacterial Pneumonia
Viral:
More likely to impact healthy people with strong immune systems. Antibiotics don't work. Can be fatal.
Bacterial:
More likely to affect someone with a lowered immune system, or someone who is recovering from a respiratory infection. Antibiotics work. More aggressive and difficult to treat.
More likely to impact healthy people with strong immune systems. Antibiotics don't work. Can be fatal.
Bacterial:
More likely to affect someone with a lowered immune system, or someone who is recovering from a respiratory infection. Antibiotics work. More aggressive and difficult to treat.
36
New cards
Aspiration PNA
Foreign substance (food, secretions, environmental compound) enters the lung and causes inflammation. Severity of injury directly related to amount of substance aspirated.
May be found in:
-Dysphagia
-Fused cervical extension
-Intoxication
-Impaired consciousness
-Neuromuscular disease
-Recent anesthesia
May be found in:
-Dysphagia
-Fused cervical extension
-Intoxication
-Impaired consciousness
-Neuromuscular disease
-Recent anesthesia
37
New cards
Aspiration PNA
Cough progresses from dry to productive
Dyspnea
Cyanosis
Tachypnea
Wheezes with crackles, decreased breath sounds
Fever
Hypoxemia
CXR shows pneumonitis
Dyspnea
Cyanosis
Tachypnea
Wheezes with crackles, decreased breath sounds
Fever
Hypoxemia
CXR shows pneumonitis
38
New cards
PNA 0-3 days
Alveolar edema and exudate formation
39
New cards
PNA 2-4 days
Alveolar infiltration w/ bacterial colonization, RBC, WBC, and macrophages
40
New cards
PNA 4-8 days
Alveolar infiltration & consolidation w/ dead bacteria, WBC and fibrin
41
New cards
PNA >8 days
Resolution w/ expectoration or enzymatic digestion of infiltrative cells.
42
New cards
PNA up to 6 wks
Complete clearance of pna. Increased time with older age, + smoking, poor nutritional status, previous pna or coexisting illness.
43
New cards
Acute Respiratory Distress Syndrome/Acute Lung Injury
Result of disease that causes inflammation. Pulm VC can contribute to RHF --> resp failure
3 Stages:
-Exudative: capillary leak cause alveoli to fill with neutrophilic exudate and edema.
-Proliferative
-Fibrotic
Inflammation debris causes issues with diffusion, V/Q mismatch and decreased compliance. Thrombi may cause dead space.
3 Stages:
-Exudative: capillary leak cause alveoli to fill with neutrophilic exudate and edema.
-Proliferative
-Fibrotic
Inflammation debris causes issues with diffusion, V/Q mismatch and decreased compliance. Thrombi may cause dead space.
44
New cards
Interstitial Lung Diseae
General term for destruction of the respiratory membranes in multiple lung regions. Inflammation --> Fibrosis --> Alveolar Scarring.
Causes:
Occupational and environmental factors
Infections
Autoimmune disease
Radiation
Genetics
Idiopathic
Medications
-Antibiotics
-Chemotherapy
-Psych meds
Causes:
Occupational and environmental factors
Infections
Autoimmune disease
Radiation
Genetics
Idiopathic
Medications
-Antibiotics
-Chemotherapy
-Psych meds
45
New cards
Interstitial Lung Disease Sx
Dyspnea
DOE
Dry cough
Fatigue
Decreased exercise tolerance
Crackles.rales on auscultation
Possible: Cyanosis/clubbing if hypoxia
DOE
Dry cough
Fatigue
Decreased exercise tolerance
Crackles.rales on auscultation
Possible: Cyanosis/clubbing if hypoxia
46
New cards
Pulmonary Fibrosis
Progressive interstitial inflammation and fibrosis.
Excessive amount of fibrous or connective tissue in the lung. Marked decrease in compliance, lungs stiff.
May be idiopathic (IPF)
Poor prognosis
Excessive amount of fibrous or connective tissue in the lung. Marked decrease in compliance, lungs stiff.
May be idiopathic (IPF)
Poor prognosis
47
New cards
Sarcoidosis
Idiopathic, granulimatous inflammatory disorder, multi-system disease
Lungs: alveolitis
Granuloma, mass or nodule formations in the affected organs. Develop a progressive, restrictive lung disease.
SOB, cough chest discomfort
Lungs: alveolitis
Granuloma, mass or nodule formations in the affected organs. Develop a progressive, restrictive lung disease.
SOB, cough chest discomfort
48
New cards
Scleroderma
Progressive system sclerosis: progressive fibrosing disorder that causes degenerative changes.
-skin, small blood vessels esophagus, intestines, lung, heart, kidneys
interstitial pulm fibrosis.
No cure.
-skin, small blood vessels esophagus, intestines, lung, heart, kidneys
interstitial pulm fibrosis.
No cure.
49
New cards
Coal Worker's Pneumoconiosis (CWP)
Accumulation of coal dust in lungs and subsequent reaction of surrounding tissue.
Coal macules: local collection of coal dust
Pleural space appears black – used be called “Black Lung” disease
Coal macules: local collection of coal dust
Pleural space appears black – used be called “Black Lung” disease
50
New cards
Body Habitus: Obesity
Increased body mass = extra tissue that requires additional O2 from the lungs.
Decreased chest wall compliance, Increased WOB, Diaphragm in a higher resting position
Decreased lung expansion, early closure of the small airways and alveoli (may result in hypoxemia)
Decreased chest wall compliance, Increased WOB, Diaphragm in a higher resting position
Decreased lung expansion, early closure of the small airways and alveoli (may result in hypoxemia)
51
New cards
Body Habitus: Pregnancy
During the 3rd trimester, ventilation in dependent regions of the lungs is impaired by growth of the fetus.
Decreased chest wall compliance. ERV decreased. WOB increased.
Increased levels of progesterone→increased ventilator drive→ increased TV and respiratory rate → increased minute ventilation.
Decreased chest wall compliance. ERV decreased. WOB increased.
Increased levels of progesterone→increased ventilator drive→ increased TV and respiratory rate → increased minute ventilation.
52
New cards
Body Habitus: Kyphoscoliosis
If severe, lungs are compressed, alveoli are restricted from full expansion
• Causing hypoventilation and atelectasis. Decreased chest wall
compliance.
Sx’s: DOE, decreased exer. Tolerance, mm spasms, accessory mm use.
• Causing hypoventilation and atelectasis. Decreased chest wall
compliance.
Sx’s: DOE, decreased exer. Tolerance, mm spasms, accessory mm use.
53
New cards
Body Habitus: Ankylosing Spondylitis
Chronic inflammatory disease of the spine.
Marked decreased compliance of the chest wall.
Ventilation becomes dependent upon diaphragmatic movement.
• Sx’s: DOE, pleuritic chest pain, progressive dyspnea, may have LBP, weight loss and anorexia
Marked decreased compliance of the chest wall.
Ventilation becomes dependent upon diaphragmatic movement.
• Sx’s: DOE, pleuritic chest pain, progressive dyspnea, may have LBP, weight loss and anorexia
54
New cards
Empyema
Infected pleural effusion = anaerobic bacterial pus in pleural space
• Complication of URI: Pna, lung abscess
-Infec crosses the visceral pleura or chest wall & parietal
pleura penetration from trauma, sx or CT placement
May have cyanosis, fever, tachycardia, cough and pleural pain
• Complication of URI: Pna, lung abscess
-Infec crosses the visceral pleura or chest wall & parietal
pleura penetration from trauma, sx or CT placement
May have cyanosis, fever, tachycardia, cough and pleural pain
55
New cards
Tuberculosis
• Infection caused by Mycobacterium tuberculosis
Transmitted via airborne droplets
Bacteria lodge in lungs, primarily upper lobes.
Associated with:
• Immuno-compromised pts
• Homelessness
• Alcoholism
• Health care workers
• Poor socioeconomic status
Transmitted via airborne droplets
Bacteria lodge in lungs, primarily upper lobes.
Associated with:
• Immuno-compromised pts
• Homelessness
• Alcoholism
• Health care workers
• Poor socioeconomic status
56
New cards
Tuberculosis S/Sx
May be asymptomatic. Otherwise, sx’s may develop
gradually
• Fatigue
• Wt. loss
• Lethargy
• Anorexia
• Low-grade fever
• Cough that produces purulent sputum
• Night sweats
gradually
• Fatigue
• Wt. loss
• Lethargy
• Anorexia
• Low-grade fever
• Cough that produces purulent sputum
• Night sweats
57
New cards
Lung Cancer Chest Sx
Non-smoker’s cough that persists for more than two weeks
Persistent chest, shoulder, or back pain unrelated to pain from coughing
Change in color of sputum
Increase in volume of sputum
Blood in sputum
Wheezing
Recurrent pneumonia or bronchitis
Difficult or labored breathing
Shortness of breath
Hoarseness
Stridor (a harsh sound with each breath)
Persistent chest, shoulder, or back pain unrelated to pain from coughing
Change in color of sputum
Increase in volume of sputum
Blood in sputum
Wheezing
Recurrent pneumonia or bronchitis
Difficult or labored breathing
Shortness of breath
Hoarseness
Stridor (a harsh sound with each breath)
58
New cards
Lung Cancer other Sx
◼ Loss of appetite
◼ Headache, bone pain, achy joints
◼ Unsteady gait or memory loss
◼ Neck and facial swelling
◼ Unexplained weight loss
◼ Headache, bone pain, achy joints
◼ Unsteady gait or memory loss
◼ Neck and facial swelling
◼ Unexplained weight loss
59
New cards
Surgical Interventions: Pleura
Pleurectomy, excision of portion of pleura.
60
New cards
Surgical Interventions: Rib
Rib resection, excision of rib.
61
New cards
Surgical Interventions: Trachea and Bronchi
Tracheal repair and reconstruction and sleeve reconstruction. Excision of trachea and part of main bronchus.
62
New cards
Surgical Interventions: Lung
Pneumonectomy, lobectomy, wedge resection. Excision of entire lung.
63
New cards
Pulmonary Embolus
SOB/Rapid breathing
Rapid HR
Chest Pain
Other signs/sx:
Low BP
Low O2 sat
Rapid HR
Chest Pain
Other signs/sx:
Low BP
Low O2 sat
64
New cards
Pulmonary HTN
Pulmonary arteries and capillaries become narrowed, blocked or
destroyed.
More difficult for pulmonary circulatory flow therefore raising the
pulmonary artery pressure.
-Normal PA pressure
-PA pressure of a pt w PHTN
Increased pulmonary artery pressure leads to right-sided heart
failure.
Can't be cured
destroyed.
More difficult for pulmonary circulatory flow therefore raising the
pulmonary artery pressure.
-Normal PA pressure
-PA pressure of a pt w PHTN
Increased pulmonary artery pressure leads to right-sided heart
failure.
Can't be cured
65
New cards
Pulmonary HTN S/Sx
• SOB/DOE
• Fatigue
• Syncope
• Chest pressure or pain
• LE edema and ascites
• Cyanosis
• Tachycardia and palpitations
• Fatigue
• Syncope
• Chest pressure or pain
• LE edema and ascites
• Cyanosis
• Tachycardia and palpitations
66
New cards
Cystic Fibrosis
Most common life shortening genetic illness in Caucasian population
Decreased transport of chloride, sodium and water in epithelial cells of
• Respiratory tract
• Pancreas
• GI
• Reproductive tract
• Hepatobiliary tract
Decreased transport of chloride, sodium and water in epithelial cells of
• Respiratory tract
• Pancreas
• GI
• Reproductive tract
• Hepatobiliary tract