Pharm
1/305
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
306 Terms
Inflammation
This is a protective response that the body does when stimulated by some sort of injury to the tissues. The purpose is to destroys, dilutes, or walls off that agent that caused injury so that it does not go to the rest of the body.
Inflammation symptoms
pain, fever, swelling, loss of function, redness – and result from arterial venous and capillary dilation, enhanced blood flow and vascular permeability.
inflammation
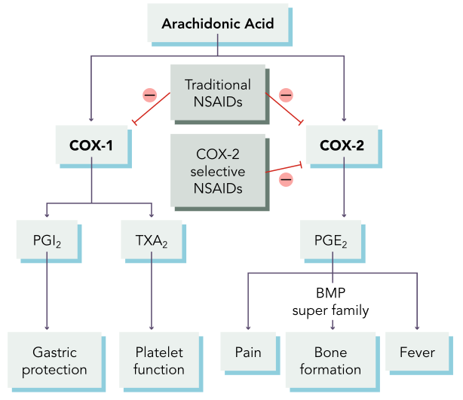
Its meaded by a lot of compounds in the body including histamines, bradykinin, leukotrienes and prostaglandins. It all meadted by the arachidonic acid pathway. This is the acid that you body releases in response to an injury. It is convered to the enzyme cycoloxinatase which you will see abbreviated as COX-2 into various prostaglandins. Protoglandind then cause inflammation and it breaks down into two different pathways. There is both traditional ones and also selective ones to the cox-2 pathway because they cause fewer side effects.
NSAIDS
•1st: ibuprofen (Motrin), aspirin (Ecotrin) – cox 1 and 2 inhbitors
•2nd: celecoxib (Celebrex) – cox 2 inhibitor to just stop the pain, fever, and inflammation
MOA for ibuprofen
•1st generation: Inhibits COX-1 (when inhibited it results in GI irritation, ulceration and bleeding) and COX-2 (prostaglandins are going to decrease which reduces the response that would result in pain, inflammation and fever)
MOA Celecoxib
•2nd generation: Inhibit COX-2 to decrease inflammatory response
NSAIDS contraindications/ precautions
•1st: GI bleed or ulcers (make them worse, can take meds to protect the GI mucosa to cause less damage), pregnancy (tetrogenic), CABG, hyperkalemia, renal and hepatic impairment , children, blood coagulopathy disorders (they already increase the risk of bleeding)
•Older adults, smokers, cardiovascular disease, alcohol misuse (use cautiously)
side effects of ibuprofen
•GI effects, increased risk of bleeding
•Kidney problems (they are excreted in the kidneys), hypertension, tinnitus, skin reactions, MI, stroke, heart failure, hyperkalemia
•Aspirin: Reye’s syndrome (especially if they have a viral illness swelling of the brain and liver damage in kids
Celecoxib side effects
•2nd – can cause cardiovascular and cerebral vascular events (MI, stroke, HF – black box warning)
NCAIDS Interactions
Glucocorticoids, anticoagulants (also increase the risk of bleeding), antiplatelets, ACE inhibitors, ARBs, digoxin, lithium, alcohol
Nursing implications for NCAIDS
•Assess: pain, fever, CBC, I&O (potential for HF and fluid retention), LFTs (risk for hepatic impairment)
•Educate: take with food or fluid, stop prior to procedures (usually a week to reduce the risk of GI bleeding).
MO of NSAIDS
Relief of pain, swelling, fever
Glucorticoids
•Prednisone (Deltasone) – steroid
Prednisone MOA and indications
•Suppress inflammatory cytokines (this includes the Cox 2 and prostaglandins) to reduce inflammation and immune response
•They block the whole arachidonic pathway and prostaglandins and they block the leukotrienes pathway. That is why use see so many other side effects and suppresses your immune system.
Indications: Inflammation, pain, swelling
Prednisone contraindications
•Active infection, adrenal suppression (which causes electrolyte changes because steroids also cause electrolyte changes: like hypokalemia), immunosuppression, liver disease, psychiatric conditions (exsasterbate them: depression, anxiety, sycosis), PUD, hypertension, heart failure, DM, renal disease, pregnancy
Prednisone no side/adverse effects
Side effects: Hyperglycemia (affect glucose metabolism – watch closely in diabetic patients), GI upset and bleeding when taken with NCEDS, increased appetite, weight gain, restlessness, insomnia, dizziness, headache, risk of infection
adverse: Muscle wasting, lipodystrophy (uneven distributions of fat and Cushing symptoms), depression, anxiety, psychosis, irritability, interrupted sleep (because it excites those neurons), hypernatremia, hypokalemia
Predisone interactions
Indications: NSAIDs, live vaccines, anticoagulants, antihyperglycemics, loop diuretics (cause changes in potassium), digoxin (causes changes in potassium), immunosuppressants (they already cause immune suppression), grapefruit juice
Prednisone nursing implications and MO
Nursing implications:
•Educate: don’t abruptly stop taking (can cause adrenal crisis), take with food (minimize GI upset)
•Assess: height, weight, BP, BS, electrolytes
MO: reduced inflammation and pain
Gout
Gout is a really painful, it's an arthritic inflammatory disease that develops when you have high levels of uric acid in the blood, or hyperuricemia. And that occurs due to increased intake of purines, or an overproduction of that uric acid, or really your body's inability to get rid of that uric acid. And that causes the development of crystals, urate crystals, that resemble sharp needles in a lot of your joints.
A common area to see this is your big toe. The deposits of the crystal
Antihyperuricemics
•Allopurinol (Zyloprim)
Allopurinol MOA and indications
MOA: Reduces production of uric acid to treat gout. Helps improve pain and inflammation.
Indications: gout
Allopurinol contraindications and MO
Contraindications: Renal or liver impairment (exacerbate them), dehydration (can cause dehydration), pregnant, breastfeeding, bone marrow depression.
MO: improved inflammation and pain
Allopurinol side effects/ adverse effects and interactions
side effects: N/V, diarrhea, drowsiness, headaches, dizziness
adverse effects: Hepatic and renal impairment, agranulocytosis (monitor CBC)
Interactions: Warfarin, penicillin antibiotics, chemotherapy – can cause toxicity of them
Allopurinol nursing implications
•Assess: uric acid( you want it to be less than 6 milligrams per deciliter), pain (and inflammation at the specific joint), CBC, kidney function, LFTs
•Educate: dietary changes (have a low purine diet because it produces uric acid. They should avoid red meats, sea food, alcohol and caffeine), drink at least 3000 ml
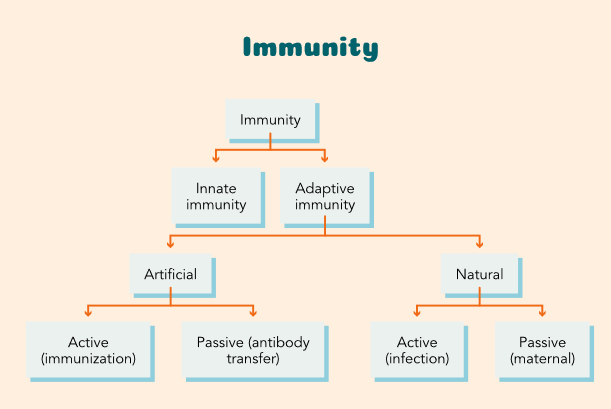
Innate immunity
Innate immunity is that body's primary defense to block pathogens from the body. So, example, the skin. The cornea, the mouth, your nares, the cilia in their lungs, GI and the GU tract.
Addapitive immunity
The adaptive immune system is what happens once those pathogens get inside the body, if the innate immune system isn't able to stop them from entering. The adaptive immune system is what produces the specific antibodies against specific microbes or chemicals.
artificial immunity
that's where your vaccines come into play. That refers to when a person is intentionally given small disease antigen so that their body can develop immunity and develop antibodies to fight it off should their body be introduced to it in the future.
active immunity
active immunity is when an individual is exposed to a pathogen, and their own immune system produces antibodies, in response to that pathogen.. So, when the body is developing the antibodies, they hang on to it longer.
Passive immunity
this is When an individual gets antibodies or antitoxins from an outside source, and it's temporary. the person is actually given the antibodies. Say someone gets a snake bite, and they need an antitoxin to prevent death from the snake bite, that is passive immunity, where you're giving them the antibodies they need right now.
active natural vs passive natural immunity
Active Natural immunity - Natural immunity develops when antibodies are naturally produced in the body in response to an infection.
Passive Natural immunity – antibodies are transferred to the fetus either through the placenta or by breast milk.
immune response (2)
antibodies (immunoglobinlins)
cellular response (cell meated immune response)
antibodies (immunoglobulins)
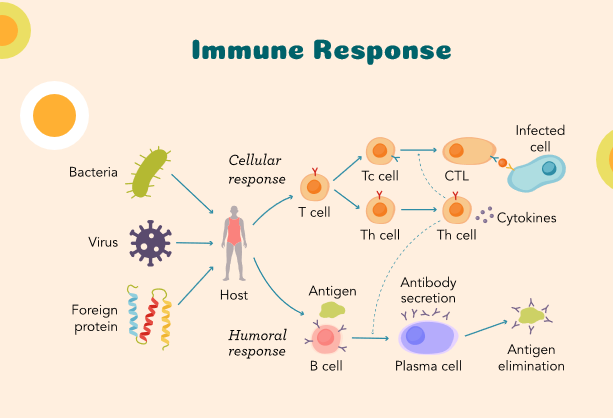
they are specific proteins that are used by B-cell in response to the antigens produced by the host or the bodies immune system. The humoral response (b-cells) produces the antibody. These antibodies can then go on and destroy what ever invaded the body.
Cellular response (cell mediated response)
this occurs by the activation of cells like macrophages and natural killer cells and the release of cytokines which are one of those inflammatory chemicals in the body. that response is important to destroy viruses, wall off that virus, bacteria. (anti-inflammatory drugs)
Vaccines
•Live-attenuated: MMR, varicella
•Inactivated: hepatitis A, B, inactivated poliovirus, HPV, haemophiles influenzae (HIB), DTAP
•mRNA: COVID-19, rotavirus
Vaccines MOA
•Live-attenuated (weakened): contain weakened forms of virus or bacteria to prompt an immune response from the body
•Inactivated: use viral or bacterial antigen without active pathogen to trigger immune system to develop antibodies
• mRNA: synthetic mRNA matches spike proteins on the surface of the target virus which triggers the immune system to develop antibodies
Vaccines indications and MO
Indications: Recommended by age (childhood vaccination schedule), health status, and risk factors for diseases, older adults have more too.
MO: Provide protection from pathogens
Vaccines contradictions and interactions:
Contradictions: Immunocompromised, Guillain-Barre syndrome, encephalopathy, some in pregnancy (potential risk to fetus), history of reactions (allergic reactions)
Interactions: Vaccines should not be mixed in same syringe with other vaccines, but multiple can be given in at the same time in the same spot.
Vaccine side/adverse effects
•Localized injection-site reactions (soreness, redness, swelling, inflammation), fever - Could get an immune response
•Allergic reaction (anaphylaxis's), seizures, intussusception (twisting of the bowel and could cause bowel rupture)
Vaccines Nursing implications
•Educate: Inactivated vaccines require multiple doses over time (series vaccines have follow ups)
•Administration: vaccines schedules, route & site
•Administration is different for each vaccine. So, like, in kids, vastus lateralis is the most common injection site, whereas in adult, deltoid is the most common injection site.
Educate patients that are vaccine hesedency (respect there thoughts). You just advise them and they make the decisions.
live vaccines
it is unable to cause serious disease in people but it allows the body then to develop an immune response to that. It allows for more of a robust and long-term protection against what ever they are being vaccinated for. MMR ( a two series and then your done)
Inactivated vaccines
but this requires multiple doses over time to maintain that ongoing immunity. You are going to need the boosters of inactivated vaccines.
mRNA vaccines
These vaccines can be produced more quickly, and they're considered generally safe, even in immunocompromised people. This technology has been out for a long time. They have spike proteins on the cells that the vaccines can bind to and cause that immune response and produces antibodies that attach to it and mark that cell for distruction.
Hypertention is?
Hypertension is the pressure of blood against the walls of the arteries when the pressure is to high.
Blood pressure is systemic vascular resistance (SVR) x cardiac output
factors that affect BP
SVR - Systemic Vascular Resistance
CO - cardiac output
Meds
Fluid volume
Sympathetic Nervous system
vascular changes and Rass system
Systemic Vascular Resistance (SVR)
○How tight blood vessels are → higher SVR = higher BP. How tightly the vessels are clammed down. How hard does the heart have to work to pump against those. If the blood vessesl are really constricted your going to have a higher SVR.
Cardiac output and meds
○Cardiac Output (CO): Blood ejected by left ventricle/min (normal 4–8 L). Main pumping chamber of the heart in one min.
○A lot of the meds affect Co or SVR as their mechanism of action.
Fluid volume and SNS
○Fluid volume: Diuretics reduce circulating volume.
○Sympathetic Nervous System: Fight or flight → increases HR & BP. – some medications work to block that response
vascular changes and RASS system
Vascular changes: can also cause hypertension, over time the vessels might thicken or loose elasticity. They get stiffen and this leads to higher blood pressure.
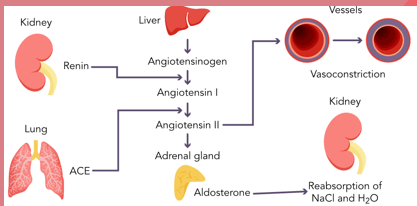
Rass system – is any important system that plays a role in the regulation of hypertension by managing BV and vascular resistance. When the blood volume is low your kidneys release renen and this causes a change reaction which leads to the formation of angiotensin one and then to angiotensin
This conversion in the Rass system happens because of the enzyme:
This conversion happens because of the enzyme called ACE. This system mainly uses ACE inhibitors and ARB’s.
■Renin → Angiotensin I → Angiotensin II (via ACE enzyme).
■Angiotensin II = vasoconstrictor. (potent) and also stimulates the release of aldosterone from the adrenal glands.
■Aldosterone = sodium & water retention → ↑ blood volume → ↑ BP. It makes you retain sodium and hold onto water in your kidneys.
what can also influence hypertension
Sodium and fluid retention can also influence hypertension. High sodium and impaired kidney functioning can lead to fluid retention and increase your total blood volume leading to higher blood pressure. Drug therpys’s can help with these.
genetic and environmental factors
●Family history (genetic predisposition), diet, exercise, stress, smoking, alcohol, prioritize sleep. These can increase your risks of getting hypertension. Life style changes is the first intervention before medications.
symptoms of hypertention
●Symptoms (usually when severe): its starts asymptomatic till the person has really high blood pressure or significant damage has occurred in the BV.
●Chest pain, headaches, dizziness, shortness of breath, nosebleeds, vision changes. – usually only occur when BP is really high
complications of hypertension
●Complications if unmanaged: if it is not managed properly it can lead to complications like: Heart attack, heart failure, stroke, aneurysms, chronic kidney disease, kidney failure, cardiovascular disease. Retina damage and visual disturbances.
●Hyperetion is defined as consistent reading that are greater than 130/80. Treatment goal is aimed at reducing that blood pressure.
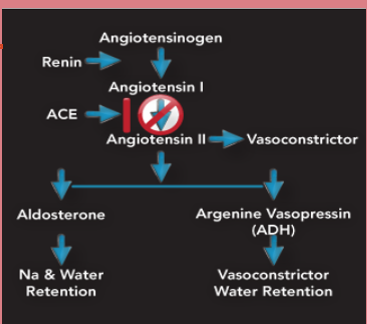
Angiotensin-Converting Enzyme (ACE) Inhibitors
•Captopril (Capoten)
Captopril MOA and MO
MOA: Block angiotensin-converting enzyme which reduces angiotensin II. They stop the conversion of angiotensin one to angiotensin 2 (this takes place in the lungs). causing excretion of excess sodium and water (because we do not have the release of aldosterone) and vasodilation which decreases BP (no vasoconstriction)
MO: Reduce BP, protect kidney function
Captopril indications and contradictions
Indications: Hypertension, heart failure, MI, kidney disease( can help protect the kidneys), DM (helps with the BV)
Contraindications:
•Pregnancy, breastfeeding, angioedema (important to remember, sever facial swelling around the eyes lips and tongue, this is a medical emergency. They usually need to be intibated) it could take years for them to have this reaction to it.)
•Hypotension, older adults, heart disease, hyperkalemia, hyponatremia – ace inhibitors can both cause hyperkalemia and hypernatremia so its important to monitor their electrolights.
Captopril side effects/ adverse
Side effects: Dry cough (nonproductive), rash, taste changes(metallic taste), dizziness, syncope (fainting), kidney function could be affected too.
Adverse: Angioedema, hyperkalemia, neutropenia, renal impairment, severe hypotension, hyponatremia, worsening heart failure 9rare)
Captopril interactions and nursing implications
Interactions: NSAIDs (an increase the risk of lithium toxicity), potassium sparing diuretics, potassium supplements, antihypertensives, lithium
Nursing implications: Assess: BP, P, electrolytes – get BP before you give them the medication and also teach them how to monitor there BP at home as well.
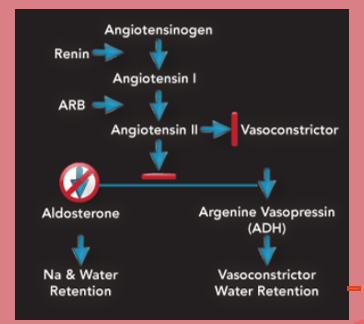
Angiotensin II Receptor Blockers (ARBS)
•Losartan (Cozaar)
Angiotensin receptor blockers are going to block that. It can’t bind to the cells and it can’t cause vasoconstriction. They also can’t release aldosterone and antidiuretic hormone which also helps lower the blood pressure.
Losartan MOA and indications
MOA: Bind to and block angiotensin II receptors which leads to vasodilation
Indications: Hypertension, heart failure, kidney problems due to DM (have some protective properties on the kidneys too).
Losartan contraindications and interactions
Contraindications: Pregnancy, renal artery stenosis, hepatic impairment (they can exacerbate those conditions which is also why you monitor renal and liver functions), kidney impairment
Interactions: Potassium-sparing diuretics, potassium supplements (increase that risk of hyperkalemia), NSAIDs (can interact with the MOA), antihypertensives (additive effects)
Losartan side/ adverse effects
•(think of they symptoms that you will have when your blood pressure Is low). Dizziness, fatigue, anemia, hypoglycemia, UTI, chest pain, nausea
•Angioedema (lower than with ace inhibitors but it is still there), hyperkalemia (monitor the electrolytes), renal impairment, severe hypotension
Losartan nursing implications and MO
Nursing implications:
•Assess: BP, P, electrolytes, renal & liver function
•Educate: lifestyle
MO: Reduce BP, prevents thickening of heart, protect kidney function
Calcium Channel Blockers (CCB)
•Nifedipine (Procardia)
•Diltiazem (Cardizem)
Nifedipine MOA and indications
MOA: They play a role once they get into the cells. They block calciums entrance into the cells causing slowed heart rate and BP, it decreased myocardial contractility
Indications: Hypertension, some fast dysrhythmias (because it can lower the pulse)
Nifedipine contraindications and side effects/adverse
Contraindications: Heart block, severe hypotension, left ventricular dysfunction
Side effects: Fatigue, hypotension, edema, bradycardia (because they affect the heart rate)
adverse effects: Heart failure – can exacerbate it
Nifedipine interactions and nursing implications
Interactions: Cyclosporine, grapefruit juice
Nursing implications:
•Assess: BP, P, cardiovascular assessment (including the assessment of the heart rhythm)
•Educate: lifestyle
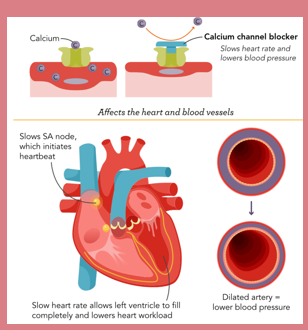
Nifedipine MO
•Reduce BP, improve angina, slow heart rate
vasodilators
•Hydralazine hydrochloride (Apresoline)
Hydralazine hydrochloride MOA and indications
MOA: •Relax smooth muscles in arteries which lowers BP, causes vasodilation and open up the blood vessels and this enhances blood flow to the different organs.
Indications: Hypertension, eclampsia, heart failure – other medical emergencies that also have high blood pressure involved.
•Hydralazine hydrochloride contraindications and interactions
Contraindications:
•CAD, aortic dissection, CHF, severe renal and liver impairment
•Breastfeeding – use cautiously
Interactions: •Antihypertensives (additive effects), NSAIDs (can cause electrolight imbalances), alcohol
•Hydralazine hydrochloride side effects/adverse
•Tachycardia, dizziness, weakness, fatigue, headache, fluid retention, hypotension
•Immune-effects (like drug included lupis), hemolytic anemia, liver injury
•They can also cause fluid retention and swelling which is why it is important to do skin assessments with these meds.
•Hydralazine hydrochloride nursing implications and MO
Nursing implications:
•Educate: abrupt discontinuation can cause hypertensive emergency or heart failure; rise slowly. Tell them to change positions slowly because of the risk of orthostatic hypotension.
•Assess: weight (because of the possible fluid retention), BP, P, skin, kidney function, LFTs, electrolytes – to monitor how the client is responding to treatment.
MO: reduce BP
Alpha1 Blockers
•Doxazosin (Cardura)
Doxazosin MOA and indications
•Block alpha1 receptors in blood vessels causing vasodilation, it relaxes them.
• The alfa 1 cause the smooth muscle contractions in the BV
•They work in the sympathetic system
Indications: Hypertension, BPH (the alpha receptors in the prostrate and bladder are blocked causesing the muscle to relax and help improve the urine flow in males that have problems).
Doxazosin contraindications and MO
contraindications:
•Pregnancy, orthostatic hypotension(history of it because it can cause it), severe liver impairment (because it is metabolized in the liver)
•Older adults, cataract surgery (interoperative floppy iris syndrome)
MO: Reduce BP, improved BPH symptoms
Doxazosin side effects/ adverse
side effects: Tiredness, headache, tachycardia, weakness, swelling, nasal congestion, URI, breathing issues, dizziness, fatigue, orthostatic hypotension (with dose increases or when they are just started)
adverse: Syncope, hypotension, intraoperative floppy iris syndrome
Doxazosin interactions and nursing implications
interactions: Antihypertensive meds, PDE-5 inhibitors (Viagra which also causes vasodilation), nitrates (cause vaso), NSAIDs (reduce effectiveness), alcohol (also metabolized in the liver)
Nursing implications:
•Assess: BP, P, rhythm
•Educate: avoid driving until they know how med affects them, lifestyle (exercise, diet, low-sodium diet), don’t stop abruptly 9can cause rebound hypertension) – because of all the side effects
Centrally Acting Alpha2 Agonists
•Clonidine (Catapres)
clonidine MOA and indications
MOA: Stimulates alpha2 receptors in the brain, which reduces the release of norepinephrine and lowers the activity of the SNS to decrease BP and HR
Indications: hypertension
clonidine contraindications and MO
contraindications:
•Severe bradycardia, hypotension, CAD, renal impairment
•Recent MI, syncope, depression
MO: reduce BP, HR
clonidine side effects
•Nausea, headaches, hypotension, fatigue, mood changes (irritability), constipation/diarrhea (GI effects), dry mouth, drowsiness
•Angioedema, depression, heart block, syncope
Clonidine interactions and nursing implications
Interactions: Antihypertensive, CNS depressants, antidepressants, digoxin (can cause excessive bradycardia), MAOIs
Nursing implications:
•Educate: don’t stop abruptly (rebound hypertension), lifestyle
•Assess: BP, P - watch for signs of hypertension and bradycardia
beta blockers
•Metoprolol (Lopressor) – cardio selective so you will not have the reparatory side effects.
•Carvedilol (Coreg) – nonselective affects the lungs and would not be helpful in patients that have lung conditions. They block beta 1 and 2 and also alpha 1 receptors.
Metoprolol MOA
•Block beta receptors to reduce impact of SNS which causes reduced BP, heart rate, myocardial contractility, and cardiac output
•They are different in how they work because some of them are cardio selective - Meaning that they mainly block the beta 1 receptors In the heart. The nonselective ones are going to bind to the beta one and beta 2 recepotrs which are also located in the lungs)
metoprolol indications and contraindications
Indications: Hypertension, angina, arrhythmias, heart failure
Contraindication:
•Severe hypotension, heart block, severe bradycardia, decompensation heart failure, liver impairment
•Respiratory disorders
metoprolol side effects/ adverse
side effects: Tiredness, dizziness, bradycardia, hypotension, headaches, nausea, sexual issues (impotence), bronchospasm (usued cautiously in people with repiratory disorders)
Adverse effects: Heart block, worsening heart failure, mask hypoglycemia
Metoprolol interactions
•Digoxin, diltiazem, verapamil, antihypertensives – all three of these lower the heart rate
• alcohol (hypotensive effects can be increased whtn taken with these), beta agonists – they are trying to produce that response and they would directly fight with each other.
metoprolol nursing implications
•Educate: don’t abruptly stop – can cause serious heart problems.
•Assess: BP, P, cardiovascular assessment, blood glucose, LFTs
metoprolol MO
reduce BP and angina
other antihypertensive medications
Direct Renin Inhibitors Aliskiren
diuretics
Aldosterone antagonists Eplerenone (Inspra)
Direct Renin inhibitors
Those interfere with the RAAS system activation and prevent that conversion of angiotensin I to 2.
Diuretics
can also lower blood pressure.
Thiazide diuretics: hydrochlorothiazide
Loop diuretics: furosemide (lasixs)
Potassium-sparing diuretics: spironolactone (Aldactone)
Osmotic diuretics: mannitol
Aldosterone antagonists
block the effects of aldosterone and leads to reduced blood volume and blood pressure
Nitrates
vasodilator that can lower blood pressure
antilipidemic
These medications are used to lower fat in the blood or lower cholesterol