Sleep disorders
1/54
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
55 Terms
What are the two important phases of sleep?
Slow-wave sleep
Rapid eye movement (REM)
Slow-wave sleep
The body-restorative sleep, which is what makes your body heal up and feel rested
Early in the night, you get lots of slow wave sleep. But, as you get closer and closer to the morning, you get more REM sleep
Dreaming does occur during slow-wave sleep, but is much more common during REM
REM Sleep
You memorize and consolidate stuff better during REM sleep
It’s also impossible to restrict REM sleep, because if you decrease it, then it will take over your slow-wave sleep
If you’re greatly sleep deprived, your eyes may begin to twitch and you slip into REM sleep
How does sleep effect other disorders?
Anxiety, mood, and psychotic disorders have sleep issues—it’s usually best to treat insomnia before stuff like depression, as the insomnia is more likely to cause the depression—sleep orders cause and/or precipitate these disorders
Gender prevalence for insomnia, hypersomnolence, and narcolepsy
Insomnia—about doubly common in women
Hypersomnolence disorder—seems to be equal between men and women, but extremely little research has been done on it
Narcolepsy—slightly more common in men
How long do you need to have sleep issues in order to have insomnia
For three nights a week for three months
Three DSM Criteria and definition of Insomnia
A predominant complaint of dissatisfaction with sleep quantity or quality, with at least 1 of the following:
Difficulty initiating sleep
Difficulty maintaining sleep
Early-morning awakening with inability to return to sleep
Three sub types of insomnia
Having all of the criteria, but they only last for:
Episodic—having the disorder for one month but less than three
Persistent—more than three months
Recurrent—two episodes in a year
Six etiological factors of insomnia
Delayed body temperature rhythm
Drug use
Hyperthyroidism
Environmental issues, recurrent napping
Association between bed and wakefulness cues
Dysfunctional beliefs regarding sleep
Delayed body temperature rhythm
Our bodies naturally get cool at night, but for some people, their body temperature doesn’t cool down
If you exercise before bed, that warms your body, so you can’t sleep
Eating a big meal cools your extremities down, which is why it appears that turkey makes you sleepy
Drug use
Long-term weed smoking tends to make things worse regarding sleep—it only appears to help in the short-term
Hyperthyroidism
Too much thyroid hormone
Environmental issues
i.e. Your sleep hygiene. Do you have bright lights in your room? Is your roommate noisy? Usually, most people address this before seeking therapy, and
Association between bed and wakefulness cues
Napping greatly screws up your sleep schedule; if you have insomnia, you’re not allowed to nap (but if you don’t have the disorder, it can be okay).
Blue light doesn’t have near as prominent of an effect, as the problems existed way before the blue light.
Three key treatment methods for insomnia
Sleeping pills
Melatonin
Antithyroid medications
NOTE: white noise machines don’t seem to help
Sleeping pills
Classically, benzodiazepines were commonly use as sleeping pills, but now, AmBien is much more common.
AmBien is okay for the short term, such as for flying, but in the long term, you get addicted to them, and you get rebound insomnia when you go off them.
It can have nasty side effects, such as causing you to hook up with your ex.
Melatonin
Melatonin levels are low when you wake up in the morning after a good sleep. As the day progresses, melatonin levels increase
For persistent long-lasting insomnia, melatonin does little
Anti-thyroid medications
Extremely rare
Three treatment methods for insomnia
Elimination of environmental issues/naps
Behavioural therapy for extinction of wakefulness cues
Cognitive therapy for beliefs
Behavioural therapy for extinction of cues
Try to eliminate cues that are associated with being awake, such as not making a phone call in bed, or reading in bed before night
Very effective
For people in hospitals that have to be in bed, they are supposed to talk and visit and on the right side of the bed, and sleep on the left side, and the body can make the distinction
What does idiopathic mean?
We don’t know the cause of whatever disorder
Ex. Idiopathic hypersomnia means they don’t know why you can’t sleep
Hypersomnia definition
Sleep dysfunction involving an excessive amount of sleep that disrupts normal routines
Hypersomnia Three DSM Criteria
Recurrent periods of sleep or lapses into sleep in the same day
Prolonged sleep of more than 9 hours that is unrefreshing
Difficulty being fully awake after abrupt awakening
Prolonged sleep of more than 9 hours that is unrefreshing
9 and a half hours is the regular amount of sleeping time for someone with this disorder, and you are still tired after it
Are naps refreshing for people with hypersomnia?
No, people with hypersomnia tend not to wake up refreshed by naps either
Three subtypes of hypersomnolence
Acute—less than 1 month
Subacute is 1-3 months
Persistent is 3 months or more
Narcolepsy
Sleep disorder involving sudden and irresistible sleep attacks
Three DSM criteria for narcolepsy
Episodes of cataplexy
Hypocretin/orexin deficiency
Nocturnal REM sleep latency less than 15 minutes, or a mean sleep latency test of less than 8 minutes and two or more sleep onset REM periods
Episodes of cataplexy
A sudden loss of muscle tone but you maintain consciousness
Usually triggered by extremely intense emotions, such as anger or sadness
We all have cataplexy during REM sleep, which is why we don’t act out our dream
Nocturnal REM sleep latency less than 15 minutes, or a mean sleep latency test of less than 8 minutes and two or more sleep onset REM periods
These individuals have a whole bunch of REM at night and they have REM during the day
So, it’s a disorder characterized by too much REM
Other features of narcolepsy that AREN’T criteria
Sleep paralysis (the old hag)
Hypnagogic hallucinations
Restorative naps
Sleep paralysis
Sleep paralysis is when you wake up in the night but you are paralyzed. This is because you are in REM sleep
Hypnagogic hallucinations
Hypnagogic hallucinations are not real hallucinations. They are characterized by waking up during a super intense dream that you think the dream actually happened when you woke up
The dream feels like a memory
There is actually a connection between people who think they’re abducted by aliens and narcolepsy because of the hypnagogic hallucinations
Development of narcolepsy
If it onsents earlier, it tends to be more problematic (15-25 age vs 30-35). Some kids develop narcolsepy before puberty, but it’s super duper rare.
Narcolepsy and hyposomnia etiological factors
Genetics
Orexin deficiency
Hyperactivity of the histamine system
Hypothyroidism
Orexin deficiency
Only for narcolepsy
This is because there are cells in the hypothalamus that produce orexin, but a genetic auto-immune mutation causes you to not have those cells, thus you have the deficiency
Histamine system
Benadryl hits the histamine system way too hard for hyposomnia people, making the system too active
Treatment for hypersomnia/narcolepsy
Modafinil (Provigil) and amphetamines
Antidepressants for cataplexy
Thyroid medications
Modafinil (Provigil)
Modafinil (Provigil) work like an amphetamine, but are NOT amphetamines
The drug promotes wakefulness
Features of amphetamines
One feature of amphetamines that we don’t understand is that their effectiveness is dependent on the day
With women, it may have to do with the menstrual cycle
What is the most likely basis for hyposomnia and narcolepsy?
Both seem biologically based
Alex’s sleep as a coping mechanisms theory
Alex’s sleep used as a coping mechanism theory is that napping is a coping mechanism for anxiety and depression
Treatment for hypersomnia and narcolepsy
Psychoeducation regarding disorder
Development of coping strategies
Adjustment to life circumstances
Psychoeducation regarding disorder
Therapy is usually just used to help you realize that the disorder is part of your life—psychology doesn’t have a huge influence on the disorder, as CBT can’t make you less sleepy
Adjustment to life circumstances
These disorders are super hard to treat, so you have to explain to individuals that they may not be able to complete them
E.g. if you have narcolepsy, you likely won’t be able to be an ER surgeon
Circadian rhythm disorders
Sleep disruption due to alteration of the circadian system, or misalignment between endogenous circadian system and the individual’s required sleep-wake schedule
Circadian rhythm disorders
Delayed sleep type
Advanced sleep type
Non-24-hour type
Shift work type
Jet leg type
Delayed sleep type
Falling asleep later than you want to
Going to bed at 10 but not being able to fall asleep until 12
Advanced sleep type
When you’re falling asleep much earlier than you want to
We see this with seniors.
Non-24 hour type
This is when people’s normal clock is a 25 or 26 hour clock
What happens in this case you go to bed at 9, then the next week 10, and the next week 11, and the next week 12 etc…It slowly moves you around
Shift-work type
When you’re awake at the wrong time, and you’re sleepy at the wrong time
It’s mainly because your work schedule is super unpredictable
Jet lag type
When you fly somewhere and your clock doesn’t match the clock of where you are
Most commonly when you fly west to east
Etiology of circadian rhythm disorders
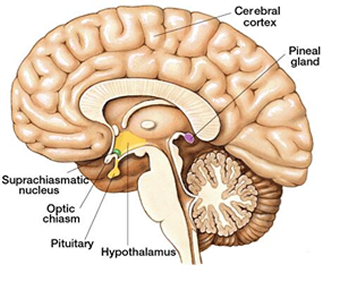
Suprachiasmatic nucleus (SCN)
Melatonin
Changing work schedules
Suprachiasmatic nucleus (SCN)
Part of the hypothalamus and sets your internal clock based on how much light hits your retina
With jet lag, your SCN likely hasn’t had enough light to reset your clock
Treatments for circadian rhythm disorders
Phase delaying—if you’re having trouble sleeping, you delay till the next evening to fall asleep
Exposure to sunlight/bright light therapy
Changing expectations regarding employment—if your SCN is too hard wired to fix, you then go to therapy to learn how to deal with not sleeping well