SCOM - Principles and Components of Spinal Orthoses - Lumbar and Thoracic
1/59
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
60 Terms
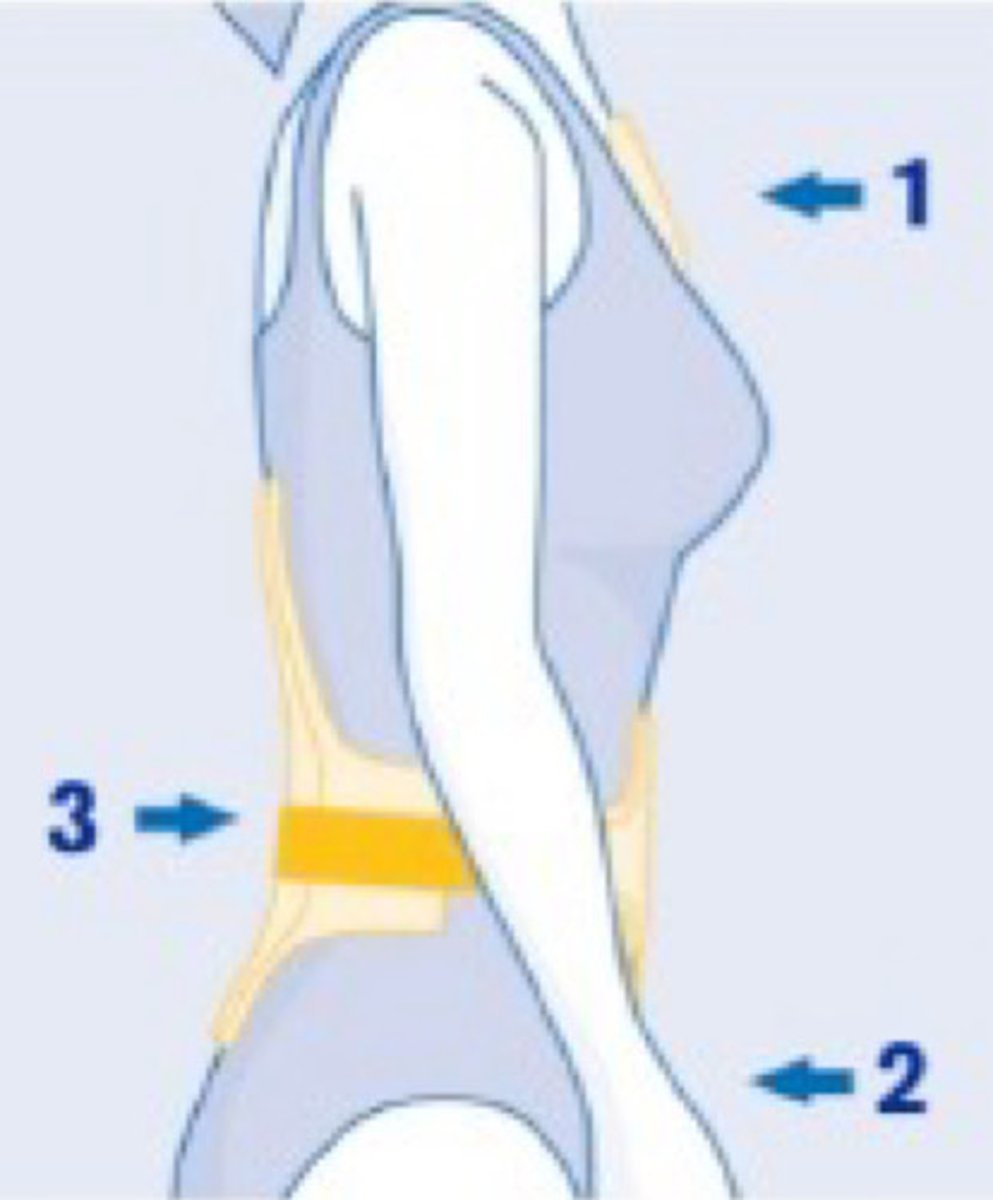
What are the three main principles of biomechanical control for spinal orthoses?
1. 3 point pressure system
2. hydrostatic compression
3. kinesthetic reminder
Abdominal compression may lead to decreased loading on the spinal column.
vertical
Hydrostatic compression is not applicable for the cervical spine. True or false?
true
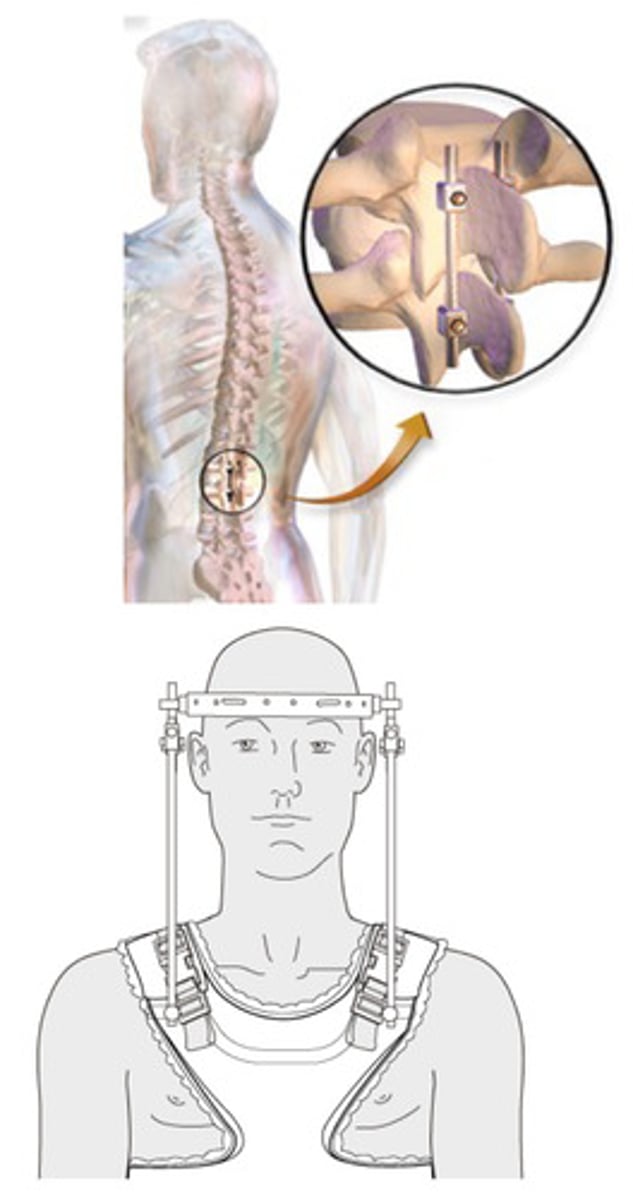
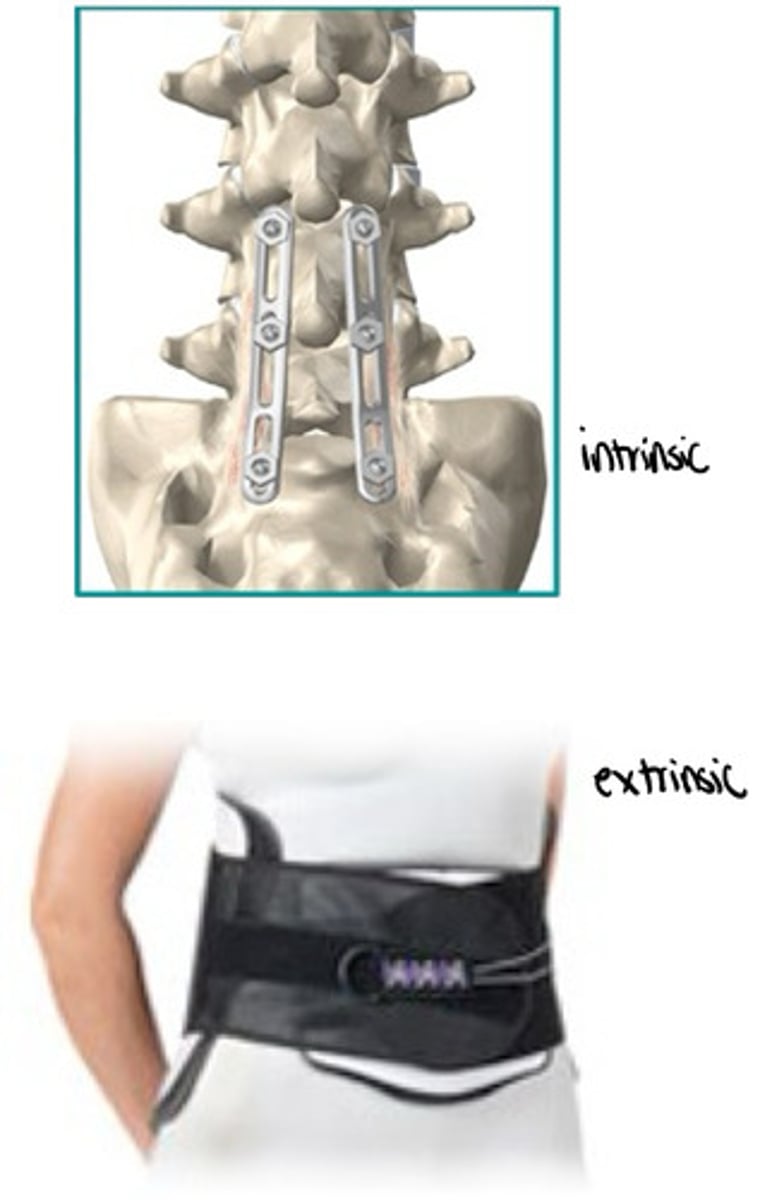
What are the two main principles of spinal surgery?
skeletal fixation
distraction
True distraction of vertebrae is achieved only through surgical intervention or the HALO. True or false?
false - only surgical intervention (HALO is the closest we come, but still not true distraction)
What are possible drawbacks to spinal orthoses?
skin breakdown
localized pressure/pain
psychological dependence
physical dependence (muscular weakening?)
What is the main drawback to any spinal stabilization?
increased motion at immobilization ends
vertebral joints superior and inferior to immobilization have greater demands for motion
How is abdominal compression achieved?
circumferential compression over the waist
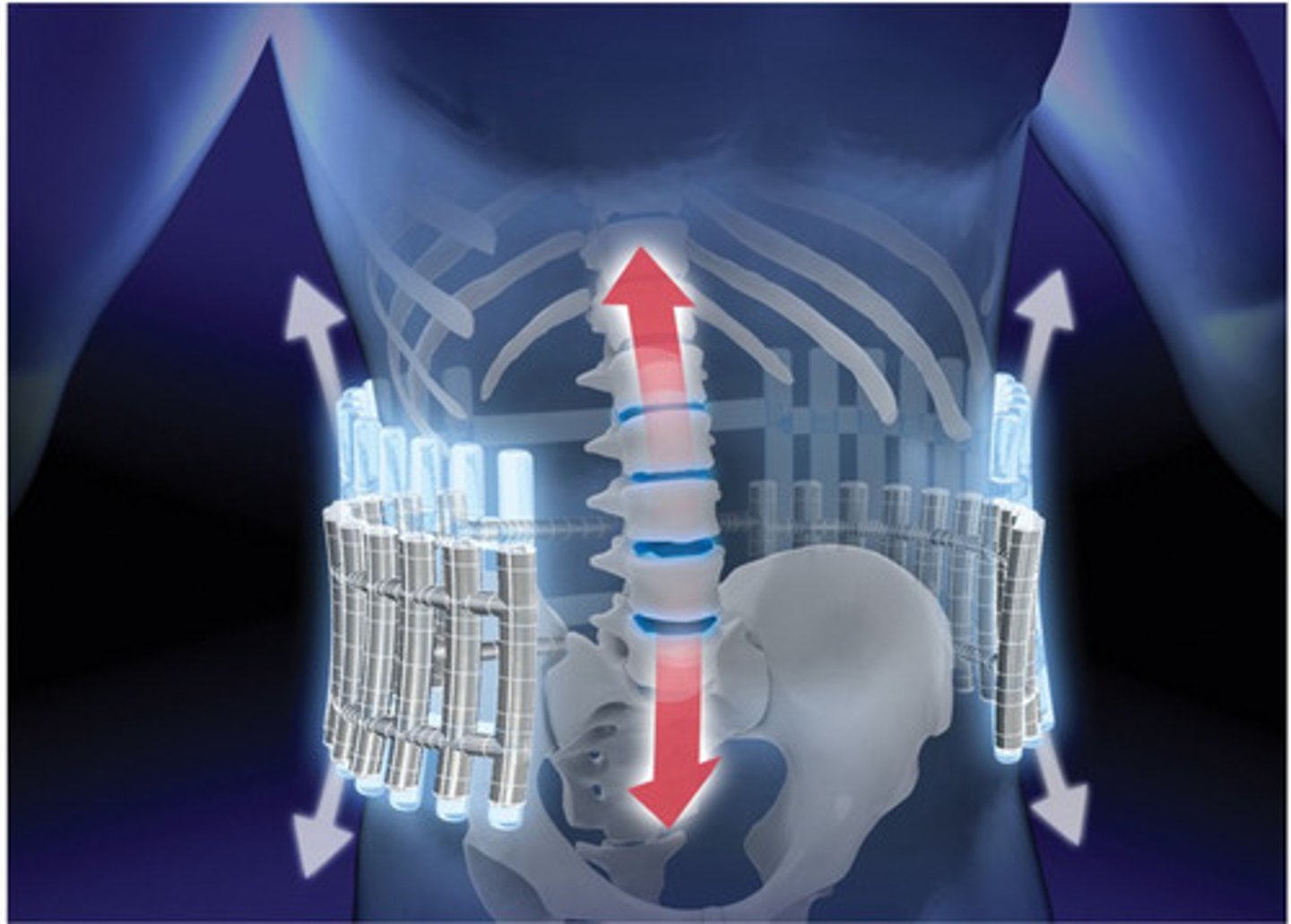
What does abdominal compression achieve?
unloading/distraction of the spine (offloading of internal structures)
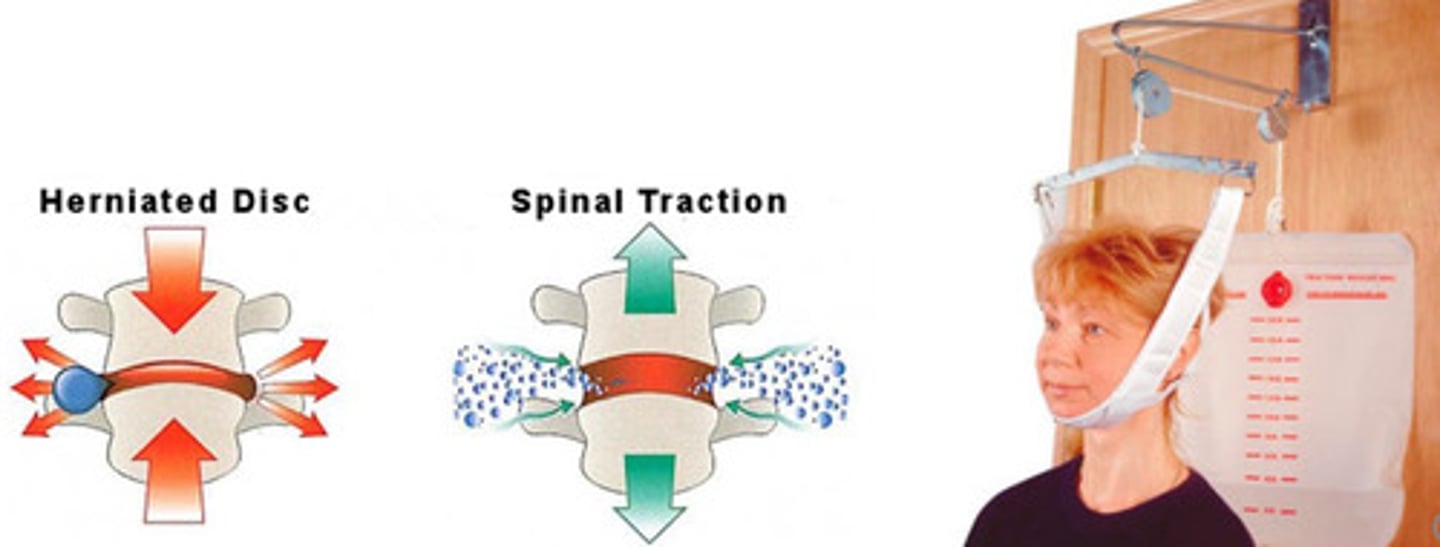
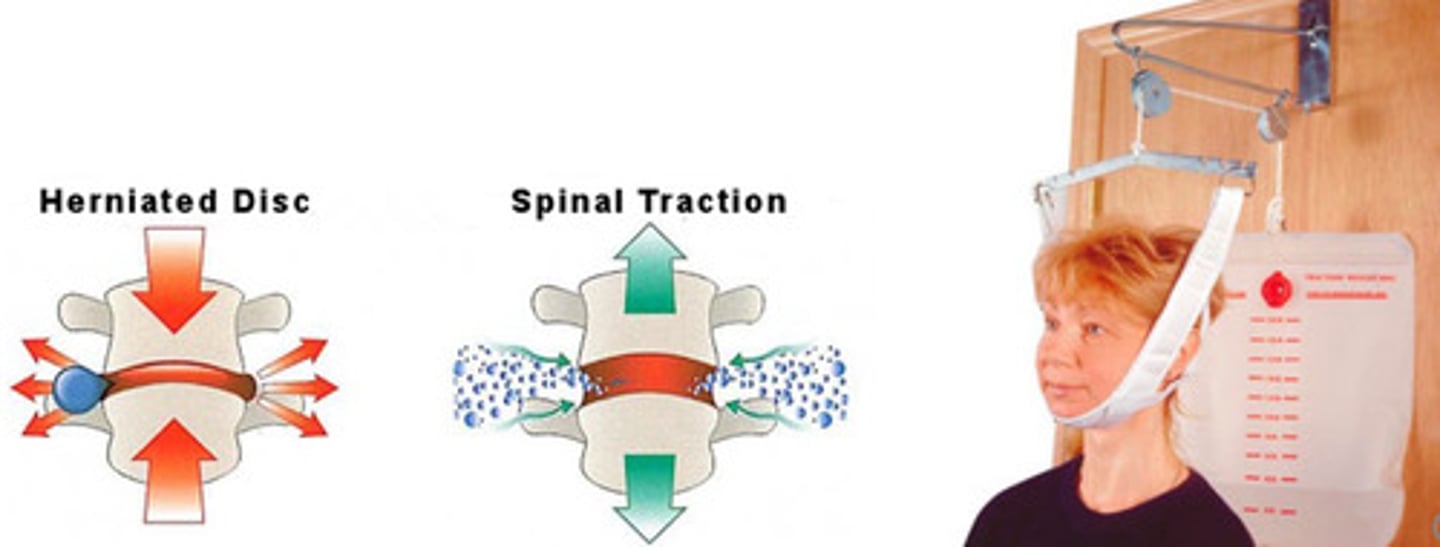
Spinal traction is a form of therapy that relieves pressure on the spine.
decompression therapy
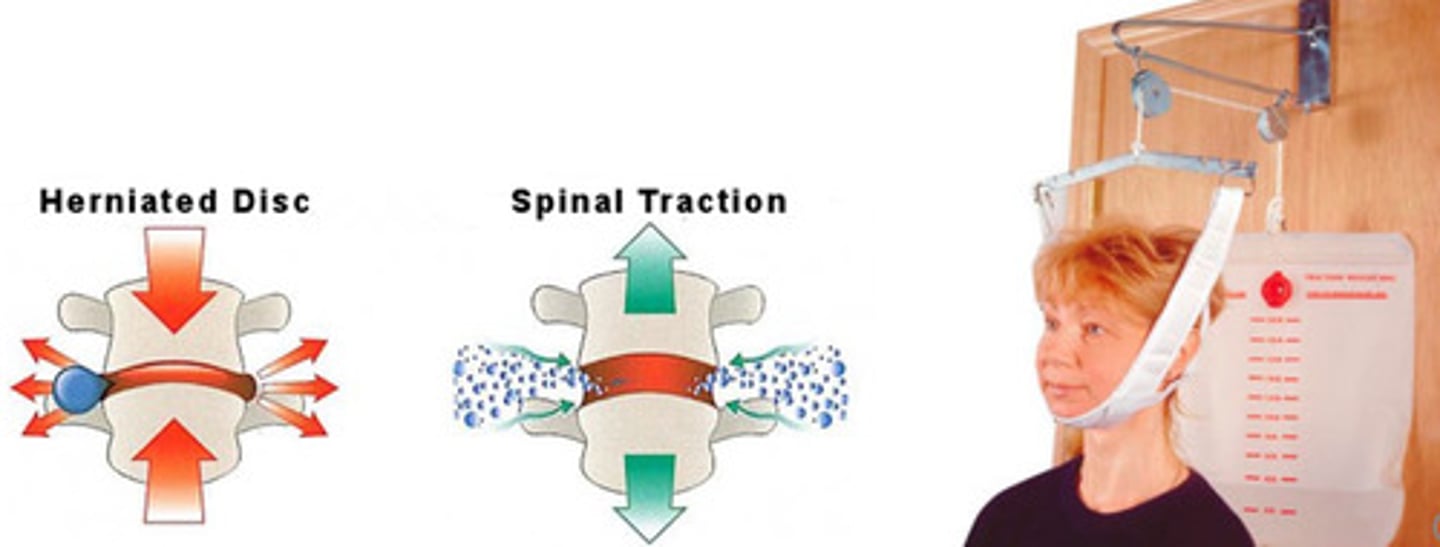
Spinal traction is often used for the thoracic spine. True or false?
false - cervical
What is the primary motion in the lumbar spine?
FL/EXT
The greatest FL/EXT and least bending/rotation occurs at what joint?
L5/S1
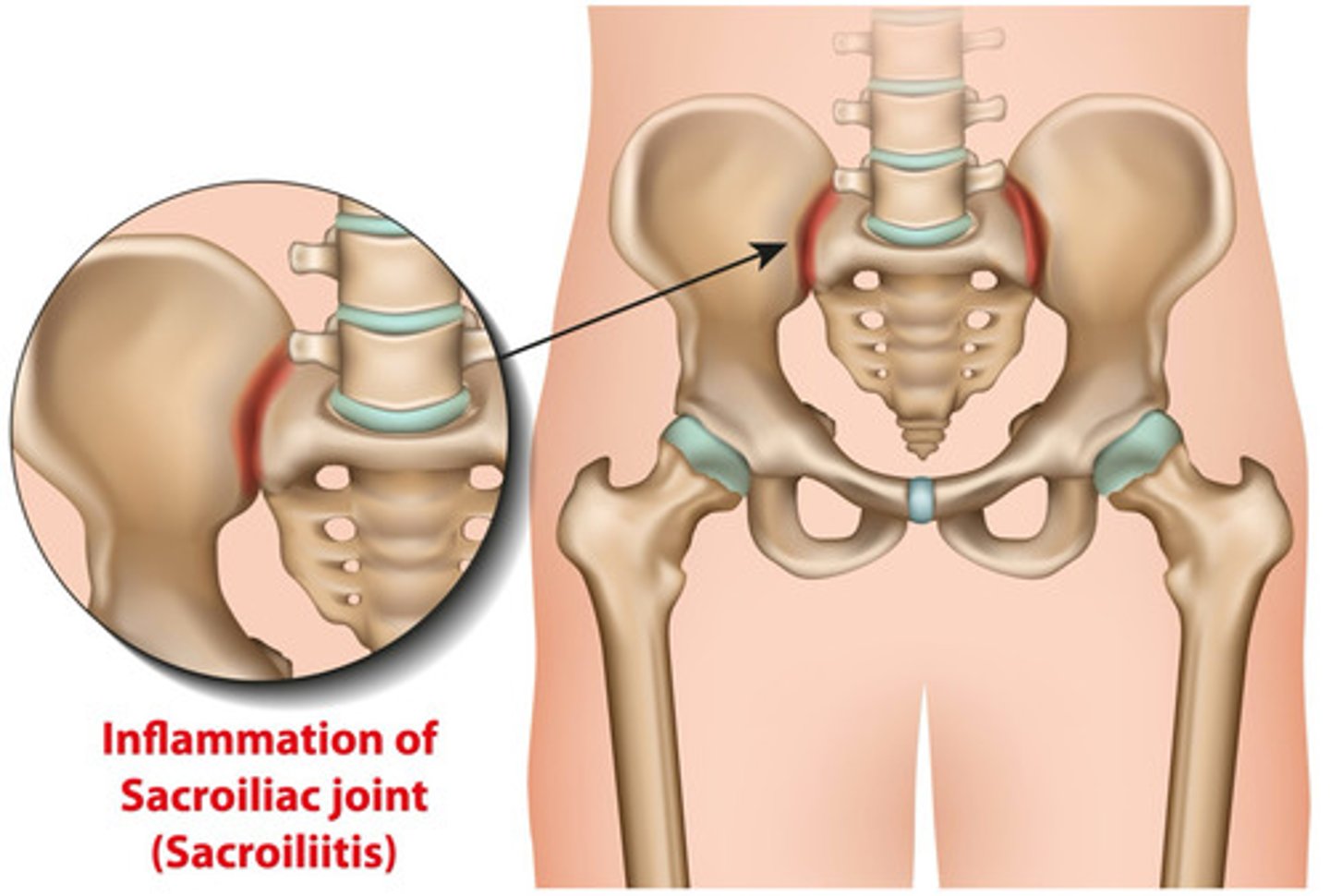
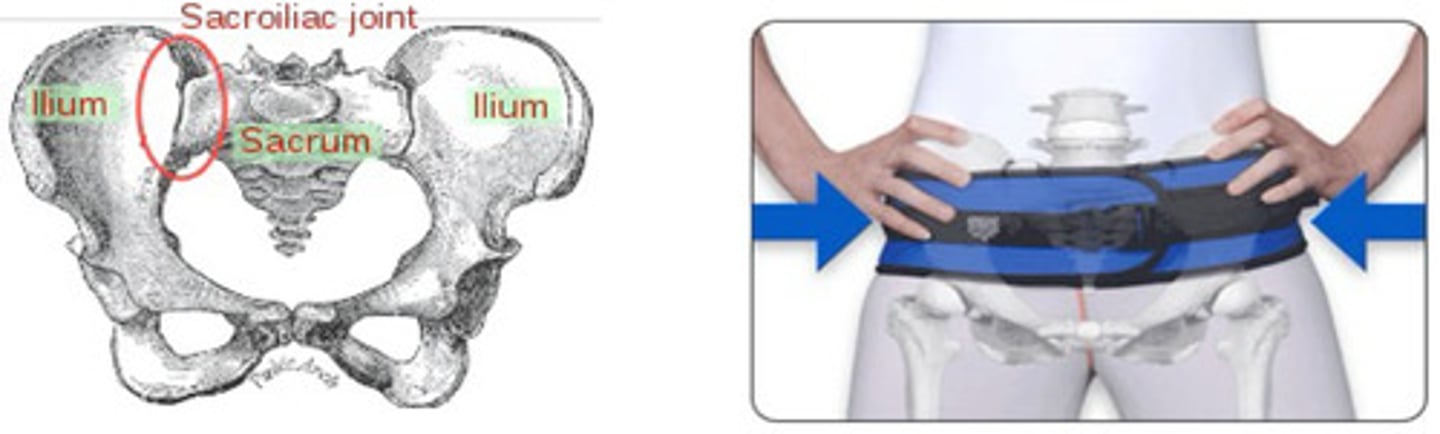
What characterizes the sacroiliac joint?
weight bearing
interlocking
synovial joint
articulation between sacrum and pelvis
What characterizes an elastic abdominal binder?
elastic circumferential wrap
canvas or fabric based
apply by fastening velcro straps anteriorly
intended for lumbar use only

There is a viable CMS code for elastic abdominal binders. True or false?
false - just tell them to get it at CVS
What characterizes a lumbosacral corset?
flexible
removable stays for EXT stop
provides compression
biomechanical capacity
increase hydrostatic compression
support spine and reduce pain
decrease lumbar lordosis/EXT

What characterizes an LSO corset with a rigid panel?
corset with rigid posterior panel (L1-L5)
compression
removable stays
biomechanical capacity
limits lumbar EXT/lordosis
increases intercavitary pressures
cannot immobilize spine

What is the difference between the Chairback vs Knight LSOs?
all are conventional rigid LSOs with corset front
Chairback
horizontal lateral supports
more contoured
rigid lateral and posterior frame
limit EXT and lateral bending
hydrostatic compression
Knight
vertical lateral supports
less contoured
rigid lateral and posterior frame
limit EXT and lateral bending

What characterizes a Williams Flexion LSO?
promotes FL
limits EXT and lateral bending
hydrostatic compression
end point control (good control of lumbar spine)
Which brace provides end point control?
Williams Flexion LSO
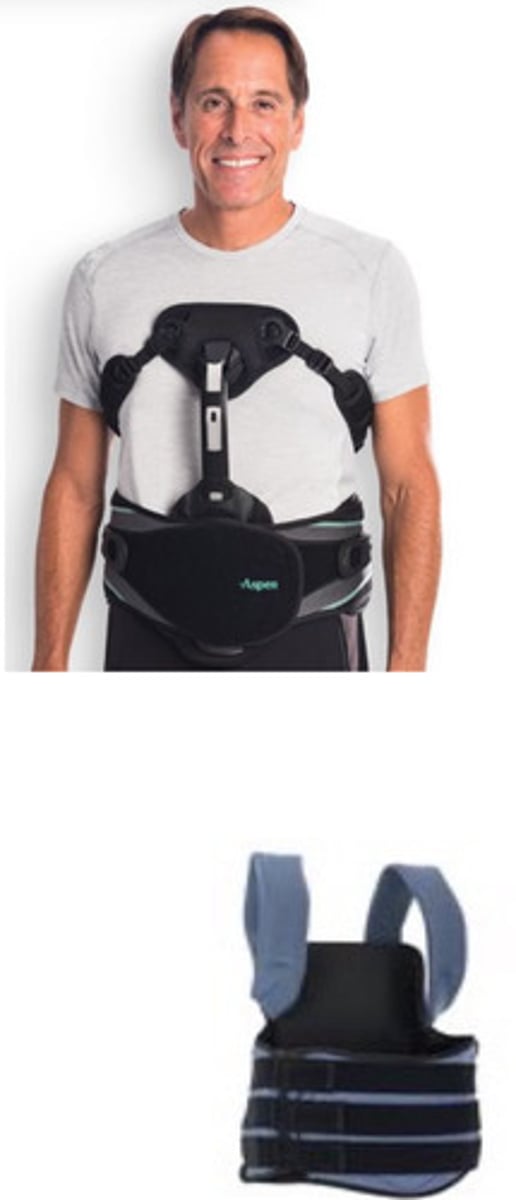
What characterizes a semi-rigid LSO?
circumferential spinal orthosis
T9-sacrococcygeal junction
semi-rigid panels for support
biomechanical capacity
reduces vertical load (hydrostatic compression)
reduces motion in lumbar spine (panels)

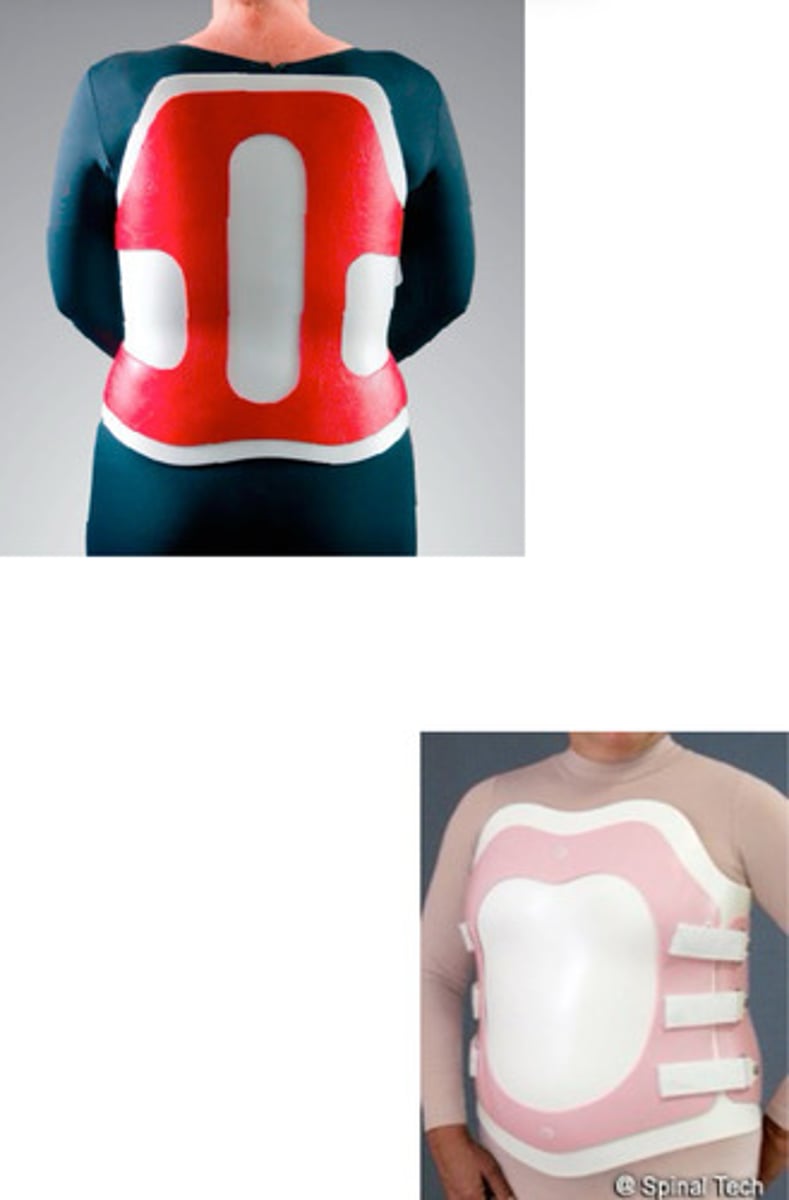
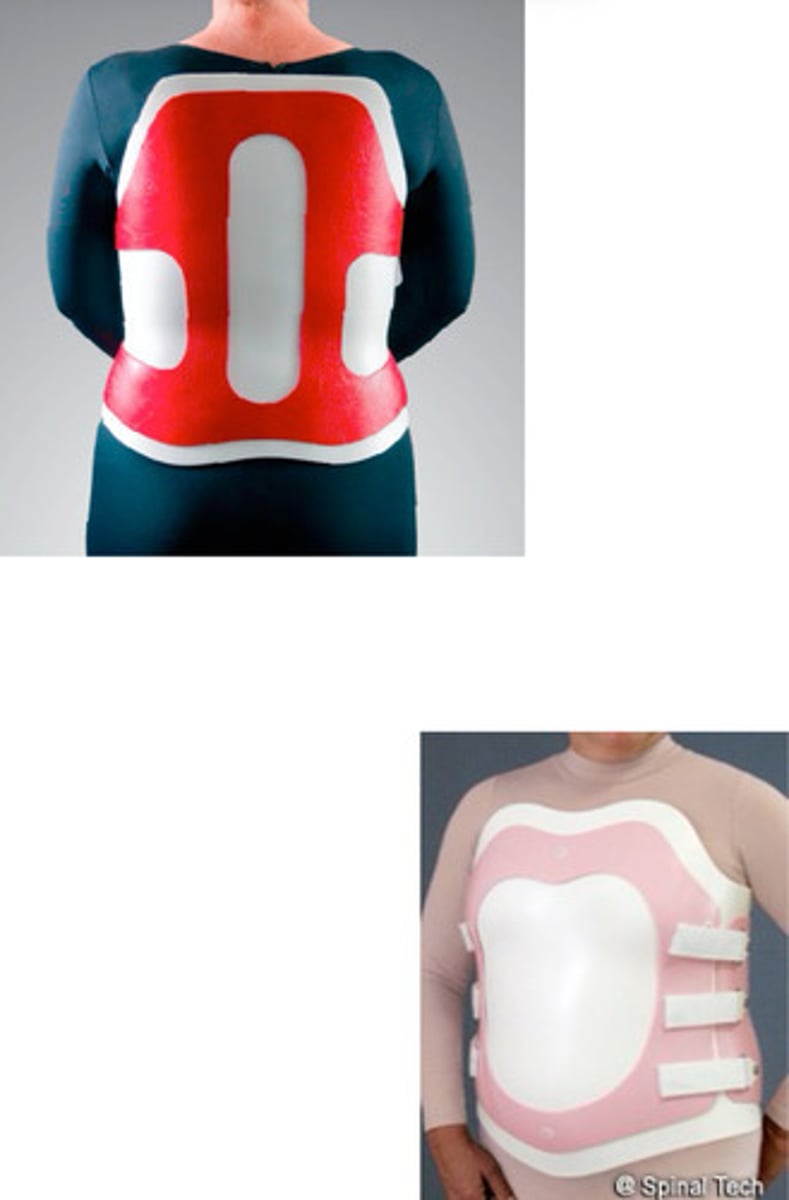
What characterizes a thermoplastic LSO?
prefabricated or custom fabricated
rigid anterior and posterior frames
from T9-sacrococcygeal junction

What are the trimlines for a custom thermoplastic LSO?
anterior/superior: 12mm inferior to xiphoid process, incorporating inferior costal margin
anterior/inferior: 12mm superior to pubic symphysis, inferior to the ASIS with adequate clearance for rectus femoris
posterior/superior: 12mm inferior to inferior angle of scapula (clear scapular wing)
posterior/inferior: sacrococcygeal junction

The custom LSO trimline are based upon the principles of .
endpoint control
What are the biomechanical capacities of a custom molded LSO?
intimate fit
rigid, semi-rigid, or flexible
increase hydrostatic compression
limit FL/EXT/LAT/ROT
does not provide adequate thoracic motion control
trimlines custom for user

Does a custom fabricated LSO provide adequate thoracic motion control?
no
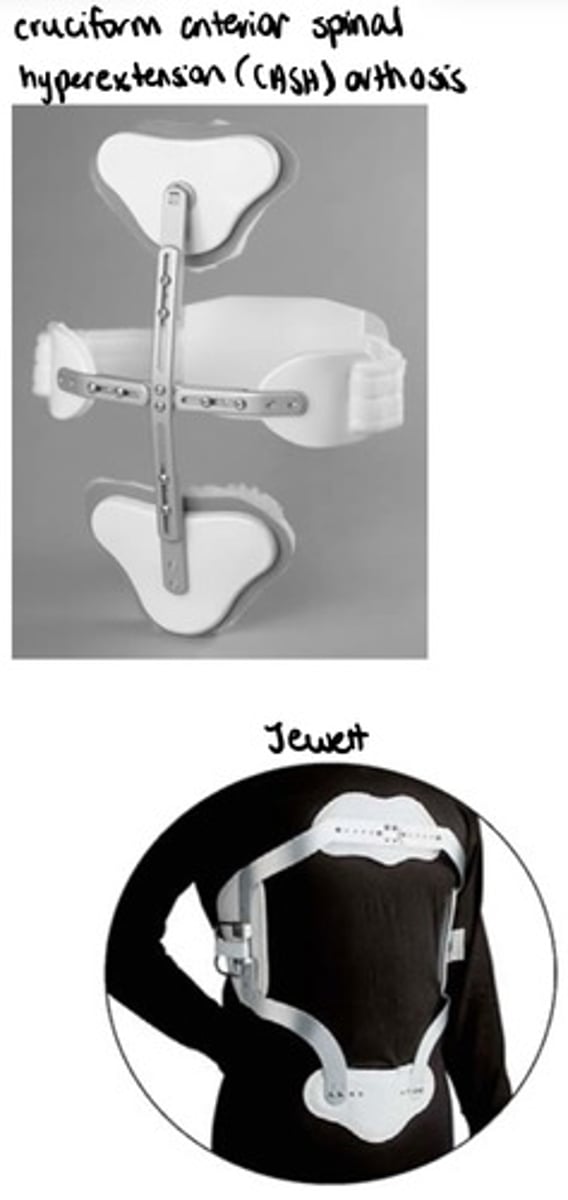
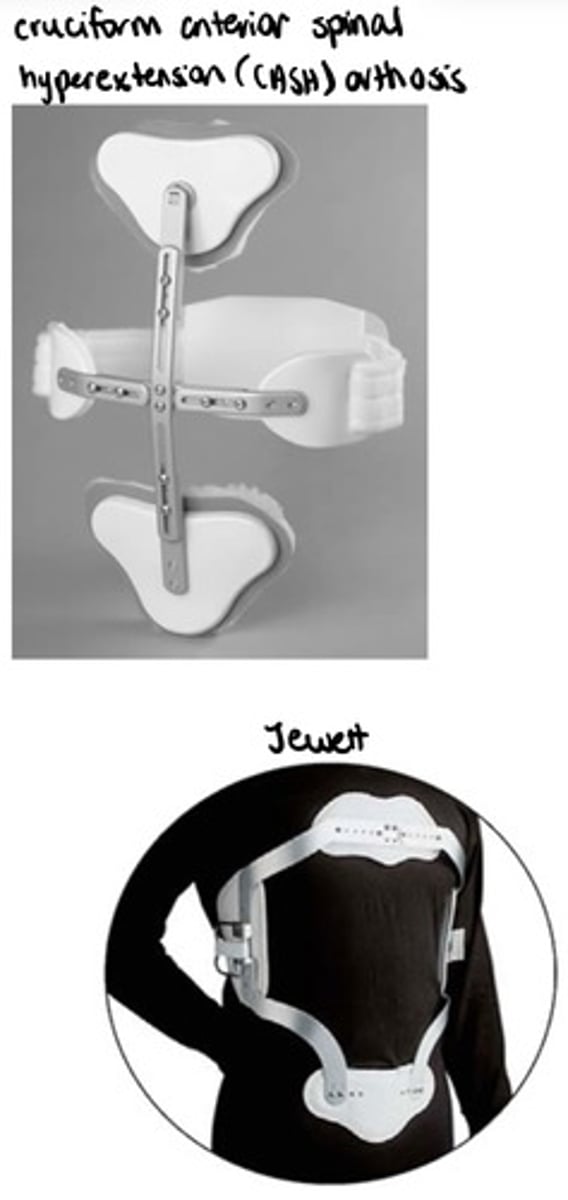
What are two types of hyperextension TLSOs?
1. CASH TLSO
2. Jewett TLSO
What characterizes a thoracolumbar corset?
inelastic
canvas/fabric
circumferential wrap with thoracic extension
rigid stays
shoulder straps
velcro straps/anterior snaps
increases hydrostatic compression

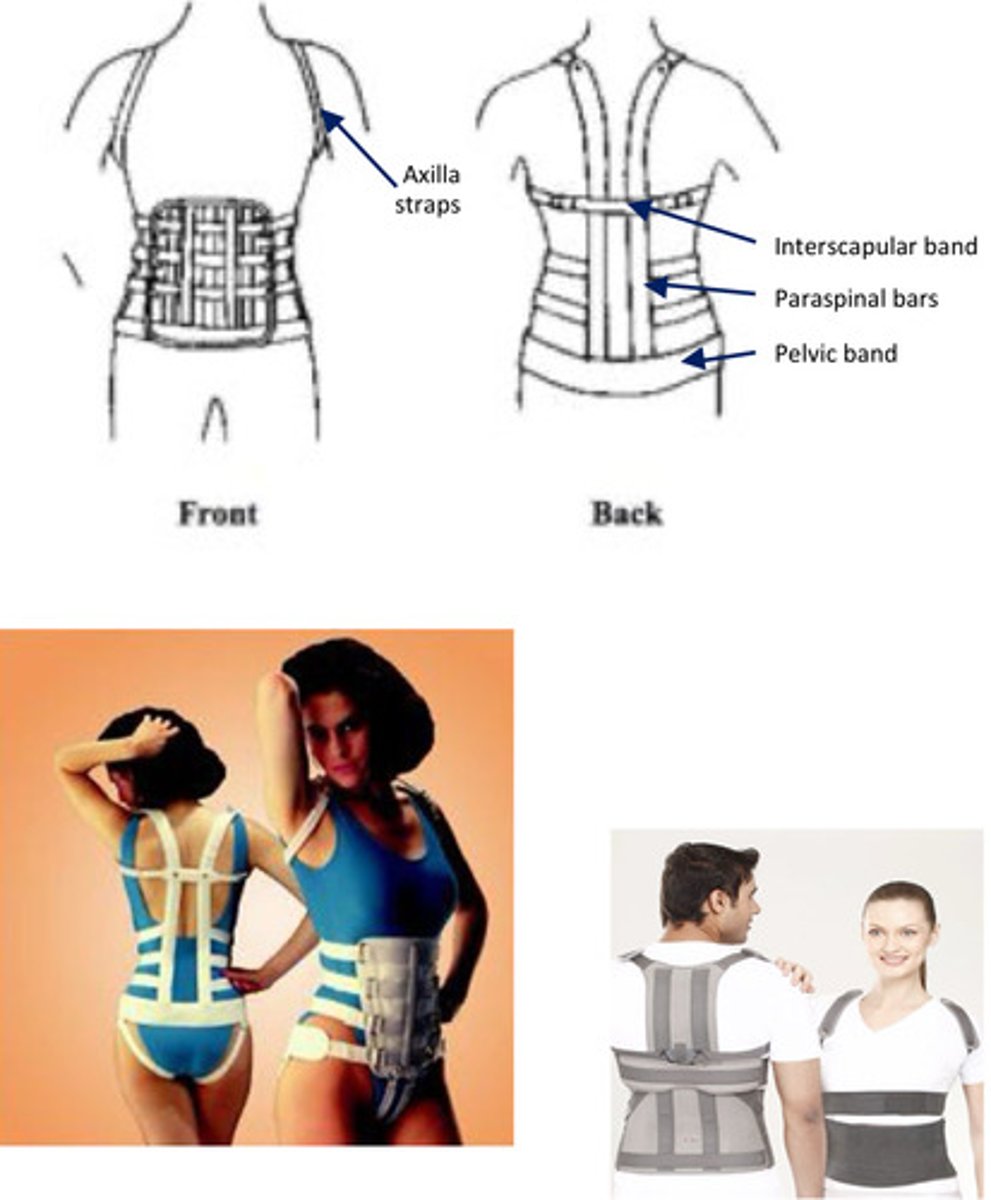
What characterizes the Taylor TLSO?
conventional or thermoplastic TLSO
components: pelvic band, paraspinal bars, interscapular band, axillary straps, corset abdominal support
biomechanical capacity
limit FL/EXT (primarily limit thoracic FL)
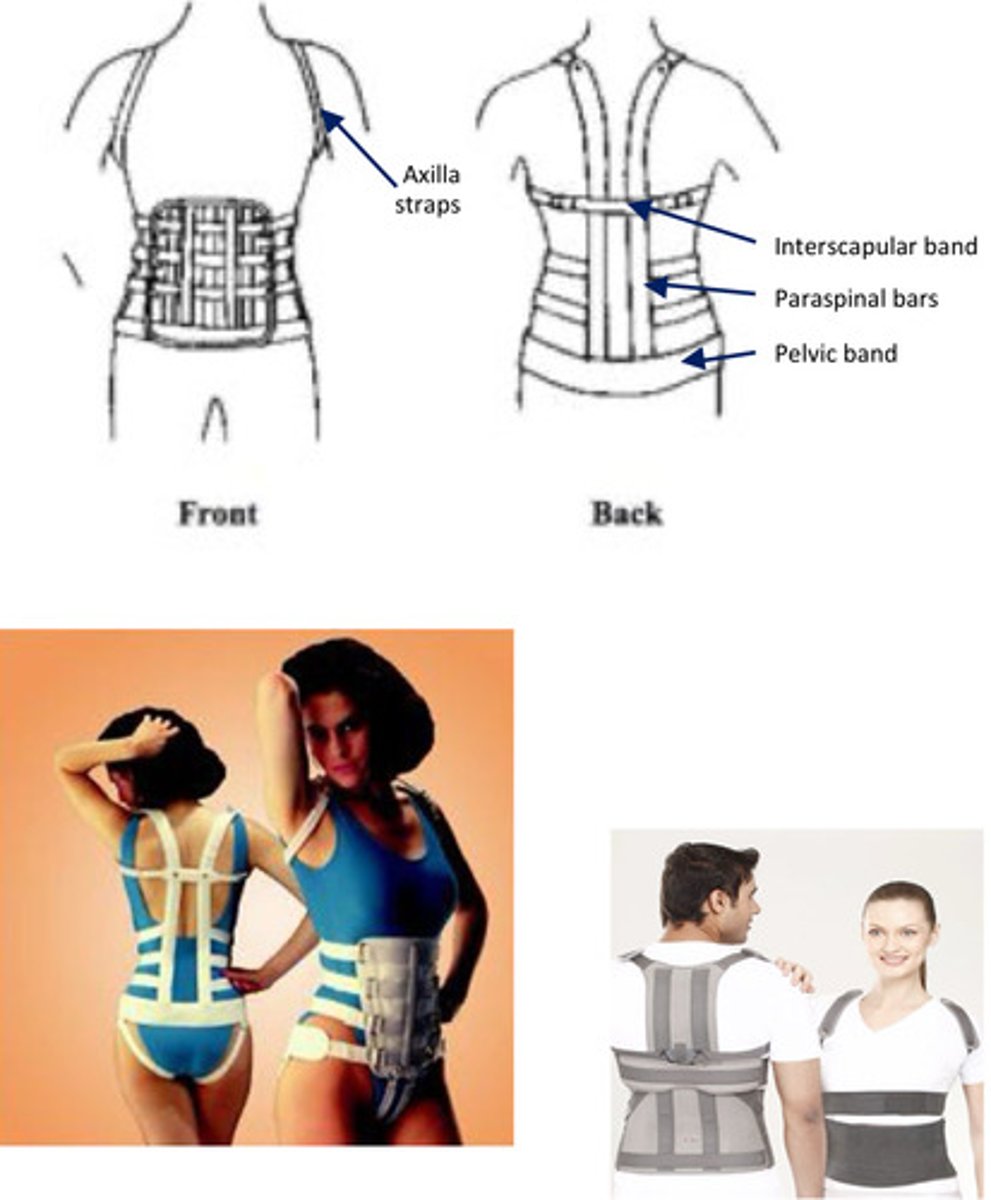
The interscapular band is the primary directed force to limit flexion in the Taylor TLSO.
anteriorly-directed
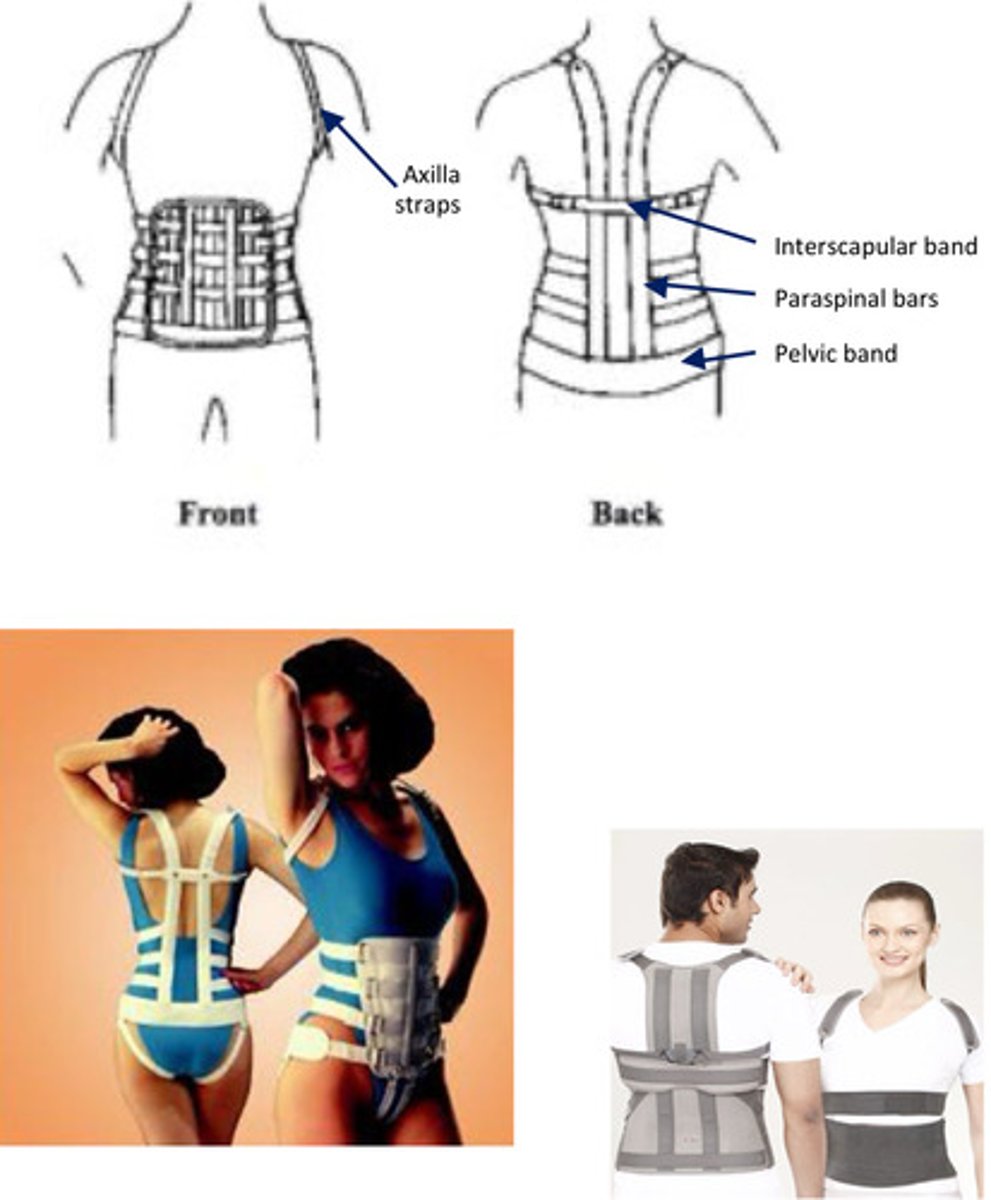
The axillary straps are the primary directed force to limit flexion in the Taylor TLSO.
posteriorly-directed
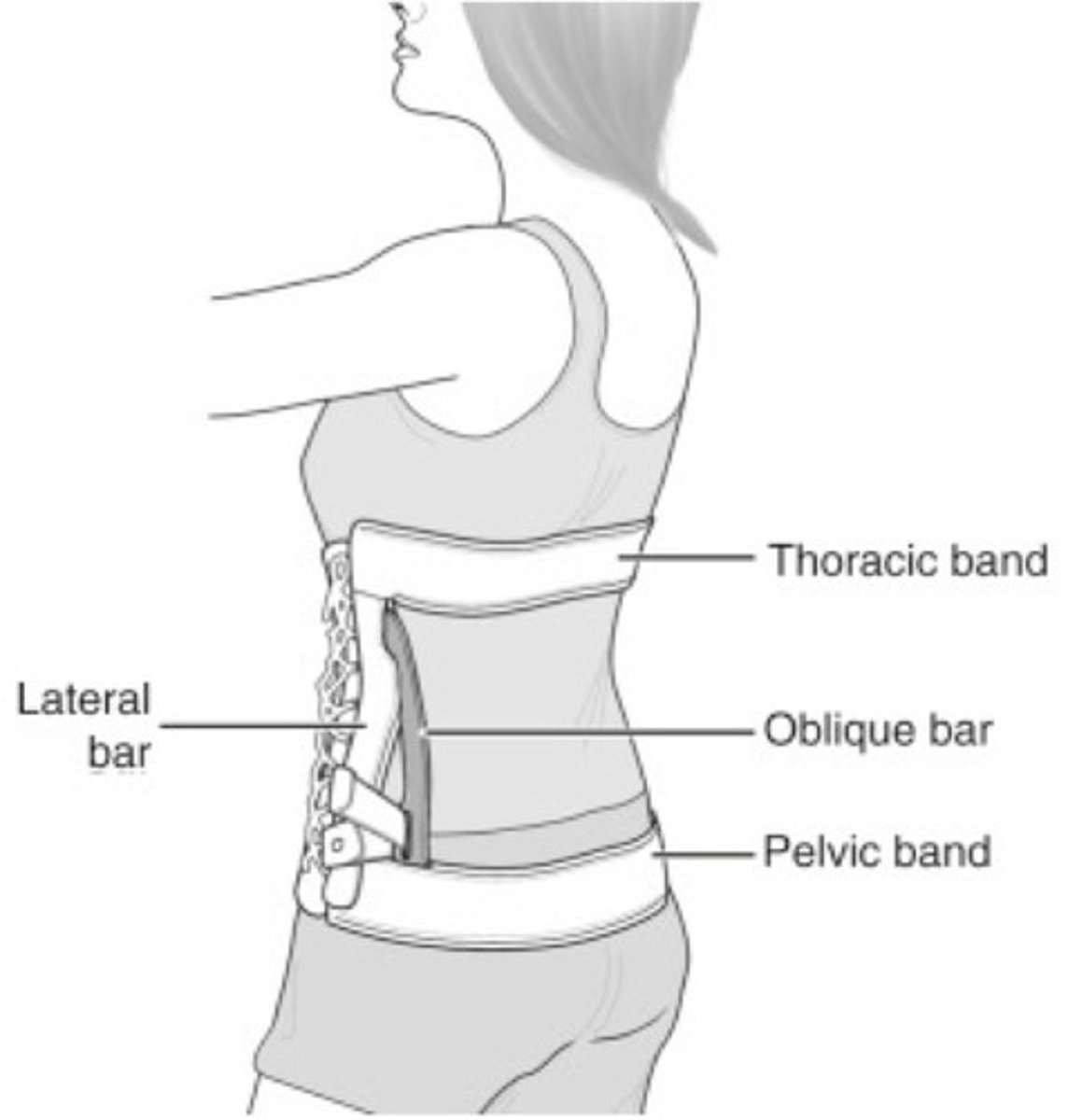
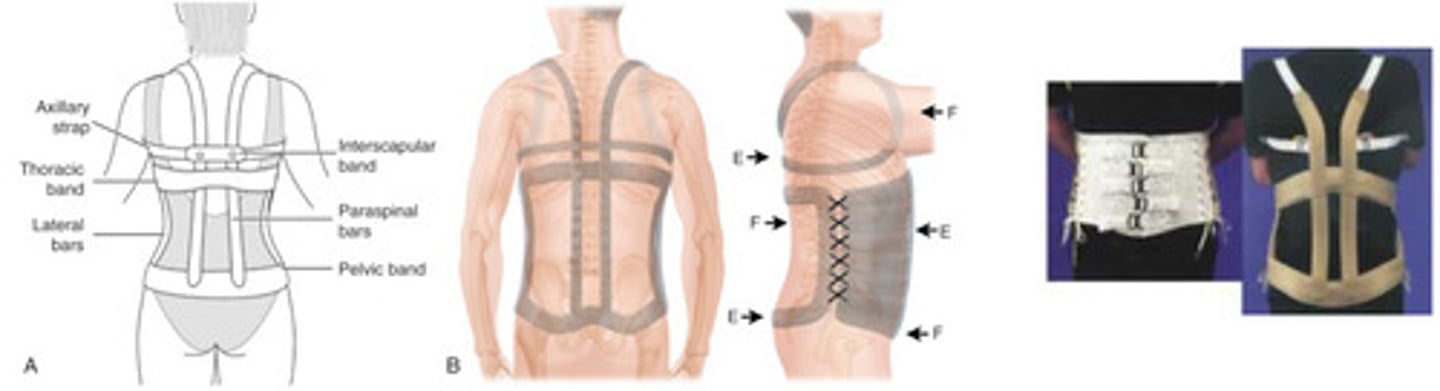
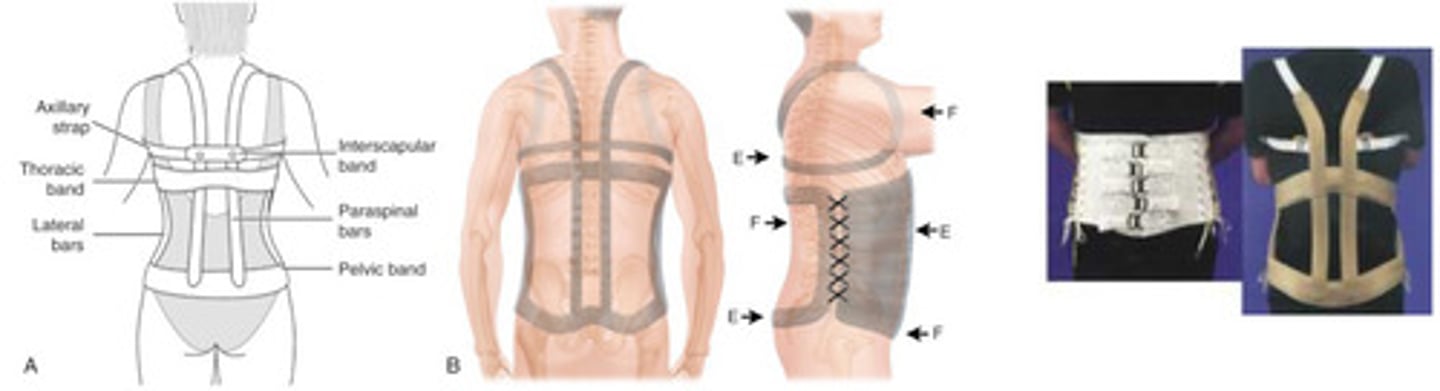
What characterizes the Knight-Taylor TLSO?
conventional TLSO
components: thoracic band, pelvic band, paraspinal bars, lateral bars, interscapular band, axilla straps, corset abdominal support
biomechanical capacity
limit spinal FL/EXT/LAT bending
The Taylor TLSO has lateral bars and the Knight-Taylor TLSO does not. True or false?
false - opposite
What is a hyperextension TLSO?
TLSO that promotes upright position while preventing flexion
often used for anterior compression fracture, Scheuermann's kyphosis, etc.
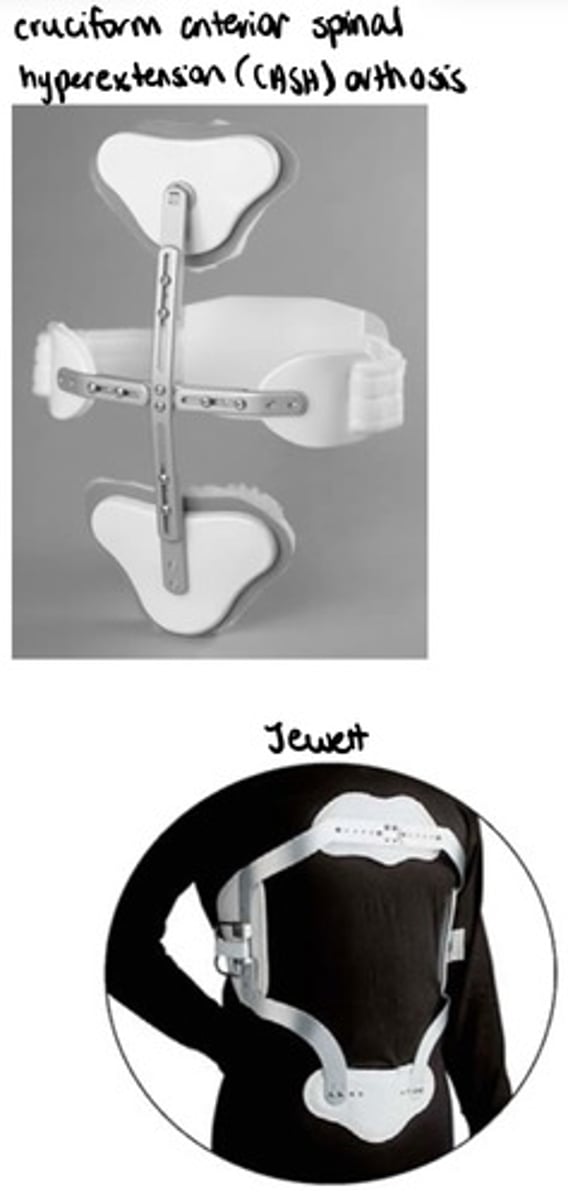
What does CASH stand for?
cruciform anterior spinal hyperextension orthosis
What is a CASH orthosis?
hyperextension orthosis
anterior super-structure
posterior straps for central support point
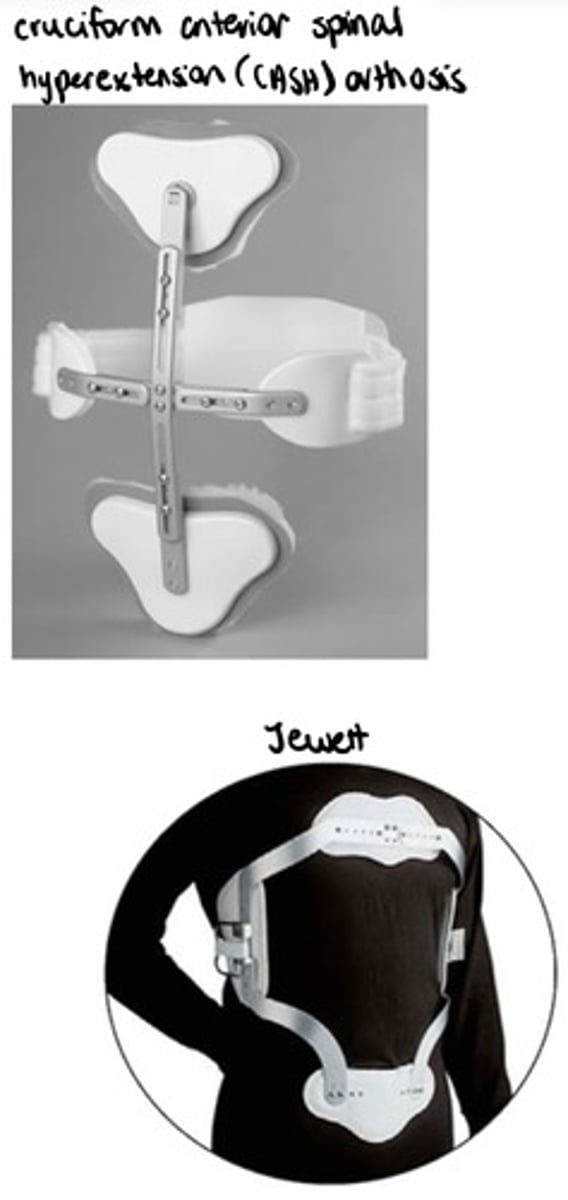
What is a Jewett orthosis?
hyperextension orthosis
lateral supra-structure
rigid tab for central support point
What characterizes a semi-rigid TLSO?
circumferential spinal orthosis from SC junction to above T9
incorporates semi-rigid panels for support
biomechanical capacity
reduces vertical load (hydrostatic compression)
reduces motion in thoracic/lumbar spine with panels
cannot immobilize spine
What characterizes a custom molded TLSO?
thermoplastic
from SC junction to above inferior angle of scapulae (above T9)
biomechanical capacity
hydrostatic compression
limits FL/EXT/LAT/ROT
customize to patient's needs
TLSOs typically extend above T9 to approximately .
T7
What are the trimlines for a custom thermoplastic TLSO?
anterior/superior: 12mm inferior to sternal notch
anterior/inferior: 12mm superior to pubic symphysis, inferior to ASIS with adequate clearance for rectus femoris
lateral/superior: 37mm inferior to pectoralis tendon for adequate clearance
lateral/inferior: 12mm proximal to greater trochanter
posterior/superior: 12mm inferior to lowest point of scapular spine
posterior/inferior: sacrococcygeal junction
What characterizes a rib belt?
elastic strap around rib cage
may be used for chest muscle strain or rib fracture
may restrict breathing (pneumonia)
remove 4x/day

What characterizes a pectus orthosis?
used for pectus carinatum
pectus orthosis or "TO"
custom fit or custom fabricated
adjustable (accommodate deformity reduction)
goal: apply tolerable posteriorly-directed pressure to sternal protrusion

What characterizes a hip spica?
thigh cuff connected to spinal orthosis (rigid or with joint)
custom of prefabricated
hip joint ROM set by MD (typically limited to 30-60 degrees of locked at 45 degrees)

When do you choose to use a hip spica?
impairment of L4, L5, and/or S1 (unrestricted hip FL translates to motion at L5/S1 and possible higher)
What is the goal of a sacroiliac orthosis?
treat sacroiliac joint dysfunction
What is one sacroiliac orthosis and what does it do?
sacroiliac belt (SI belt)
applies medially directed forces bilaterally on iliac crests (reduces motion at SI joint)
What is the 3PPS for controlling extension/aiding flexion?
1 posteriorly-directed corrective force
2 anteriorly-directed stabilizing forces (inferior and superior)
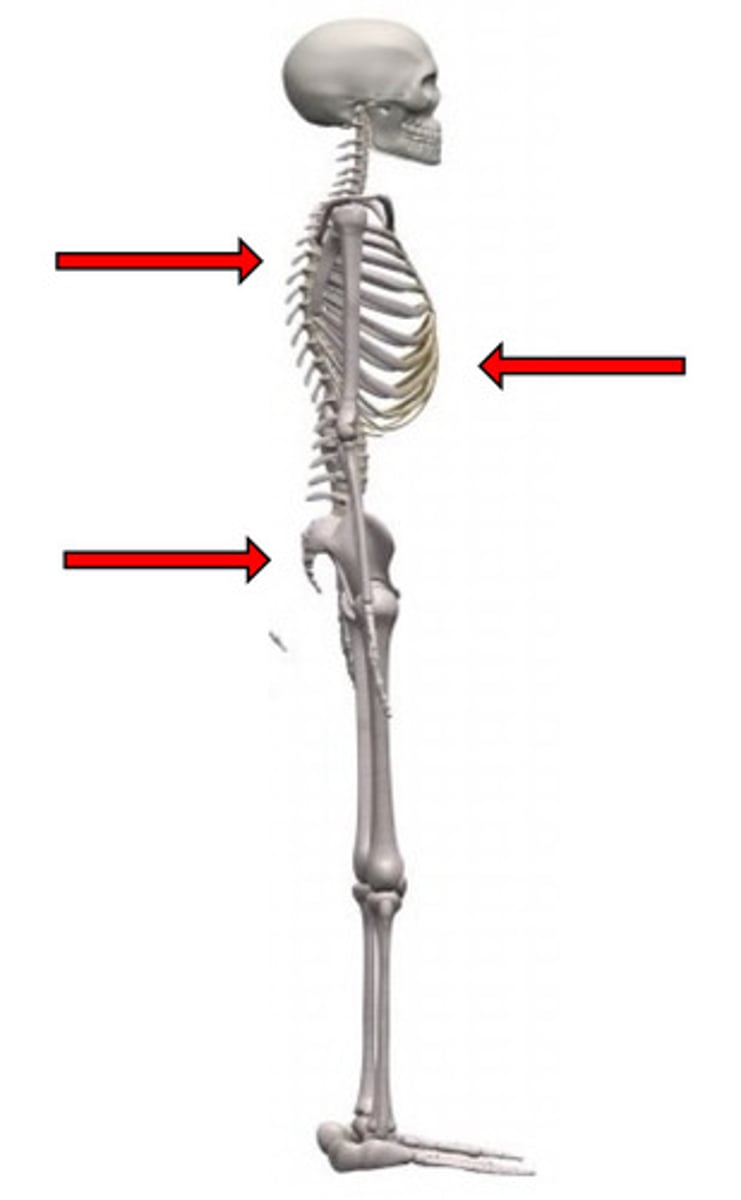
What components of conventional orthoses accomplish anterior control when controlling extension/aiding flexion?
corset/apron front (LSO/TLSO)
What components of conventional orthoses accomplish posterior control when controlling extension/aiding flexion?
thoracic band (LSO)
interscapular band (TLSO)
pelvic band (LSO/TLSO)
What is the 3PPS for controlling flexion/aiding extension?
1 anteriorly-directed corrective force
2 posteriorly-directed stabilizing forces (inferior and superior)
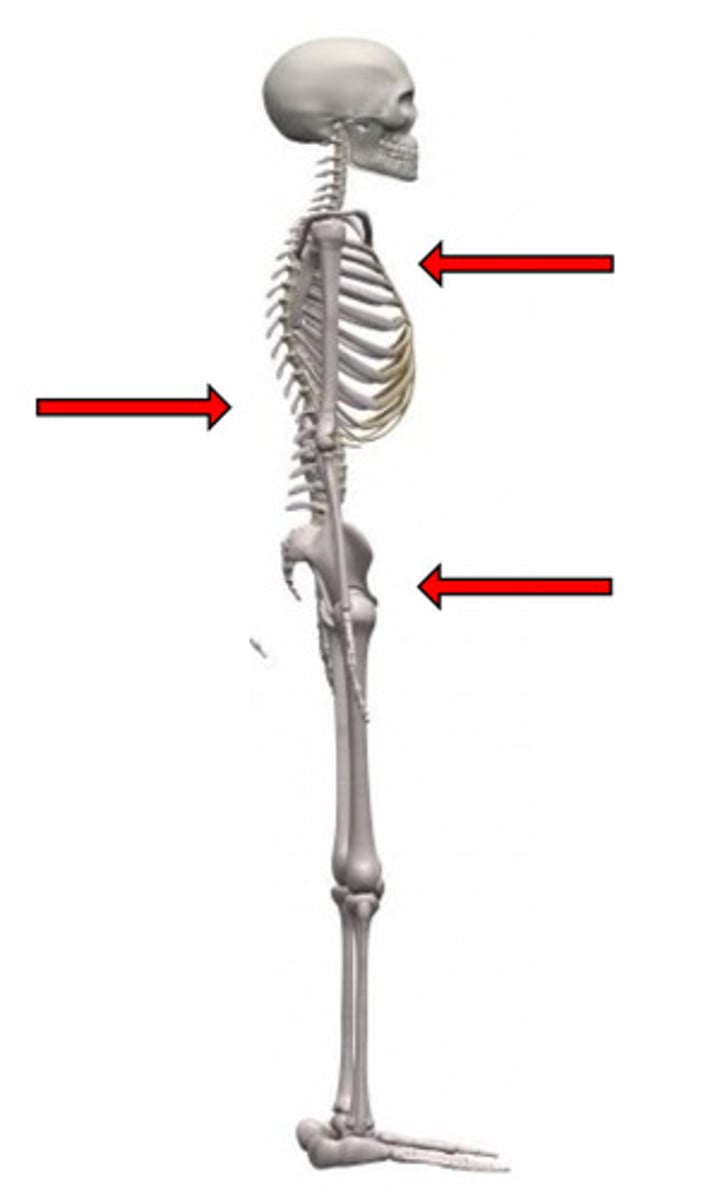
What components of conventional orthoses accomplish anterior control when controlling flexion/aiding extension?
proximal/distal corset/apron front (LSO/TLSO)
sternal pad (TLSO)
axilla straps (TLSO)
Sternal pads should be distal to the sternal notch.
1/2" distal
What components of conventional orthoses accomplish posterior control when controlling flexion/aiding extension?
paraspinal bars (LSO/TLSO)
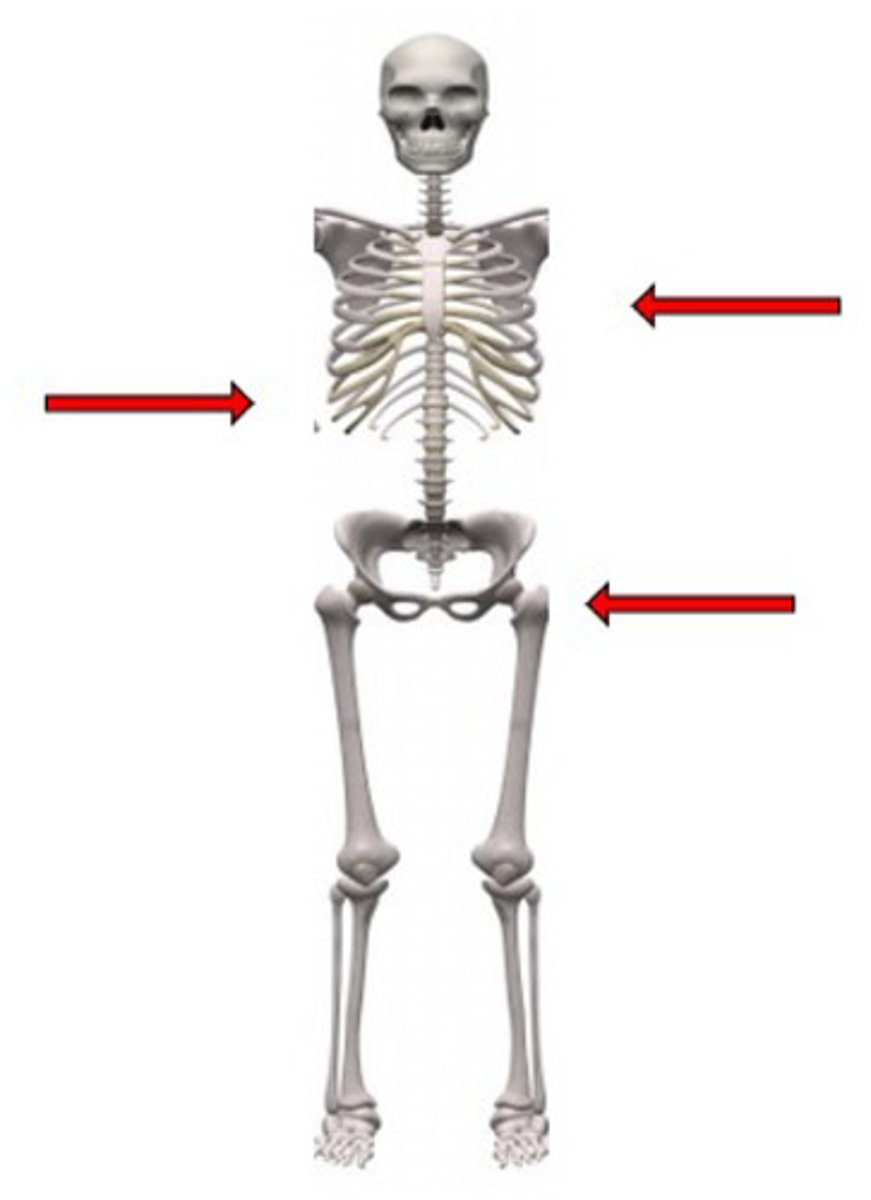
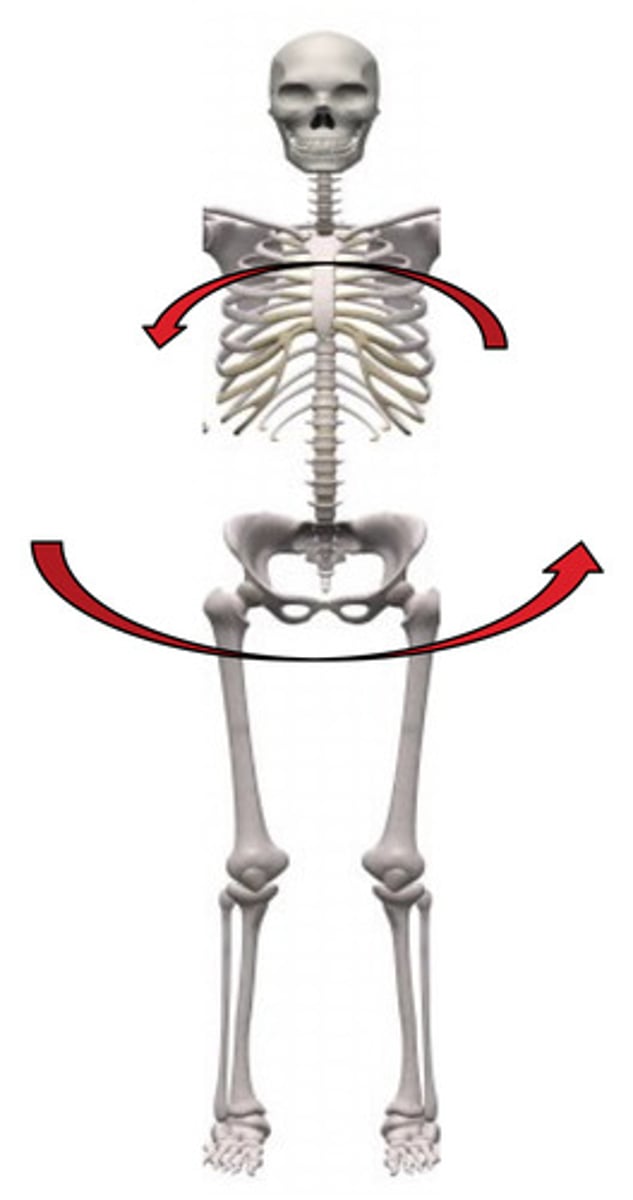
What is the 3PPS for controlling lateral bending/aiding contralateral bending?
1 medially-directed corrective force
2 laterally-directed stabilizing forces (inferior and superior)
(or vice versa)
What components of conventional orthoses accomplish ipsilateral control when controlling lateral flexion/aiding contralateral flexion?
lateral thoracic band (LSO/TLSO)
lateral pelvic band (LSO/TLSO)
What components of conventional orthoses accomplish contralateral control when controlling lateral flexion/aiding contralateral flexion?
lateral upright (LSO/TLSO)
To control rotation, a thermoplastic orthosis acts proximally at the and distally at the .
ribs/scapulae
iliac crests/trochanter
What components of conventional orthoses accomplish rotational control?
thoracic bands (LSO/TLSO)
pelvic band (LSO/TLSO)
interscapular band (TLSO)
paraspinal bars (LSO/TLSO)
lateral uprights (LSO/TLSO)