Exam II
1/61
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
62 Terms
Chronic kidney disease (CKD)
CKD- progressive, irreversible, loss of kidney function
risk factors: diabetes(poor glycemic control causes kidney damage), uncontrolled hypertension (perfusion issue), NSAID use/overuse, nephrotoxic substances, family history?
how does this occur:
FIVE stages:
GFR >90 mL/min: focus on prevention and risk factor management: control diabetes, htn, lifestyle mods, monitor kidney function
GFR 60-89 mL/min: focus on slowing progression, montior kidney function q6-12
GFR 30-59 mL/ min: continue to manage complications: Protein, Na, K restrictions, Monitor anemia, Assess Ca/ K balance, phosphate binders with meals, Monitor for bone disease, Monitor kidney function q3-6m
GFR 15-29 mL/ min: prepare for kidney replacement therapy, Strict diet: protein 0.6 g/kg, K 60- 70, Na 1-3g, Assess vitamin/ minerals, Monitor fluids, Dialysis education and planning
GFR <15 mL/ min: ESKD, kidney replacement therapy: Dialysis, Diet restrictions, Monitor dialysis complications, Vascular access care
clinical manifestations: decreased output, diluted urine, tremors(high magnesium), edema, htn, sob, uremic symtpoms: fatigue, nausea, anorexia, albuminuria
labs: potassium(increased), sodium(decreased then increased in end stage), magnesium(increased-tremors-can give calcium gluconate), phosphorus(originally increased then decreased); calcium(originally decreased then calcifies and increases), H/H (decreased)
urinalysis will show: proteinuria, hematuria(tea colored urine), foamy, high WBC
sodium and fluid balance: hypernatremia, edema
altered potassium excretion: cardiac dysrhythmias
impaired metabolic waste elimination: metabolic acidosis, high
altered calcium and phosphorus: decreased calcium and increased phosprous
decreased production of erythropoietin: decreased RBC production- anemic(low o2, dizzy, headache, pale, sob)
diet: low sodium, low potassium
top priority: avoid NSAIDS, fluid restrictions, avoid processed foods and high sodium foods, check vascular access for bruit and thrill before hemodialysis
treatment: calcium acetate- high phosphorus,
hyperkalemia
risk factors: ckd, oliguria, anuria, k sparing meds
clinical manifestations: peaked t waves, cardiac dysrhythmias, muscle weakness, often asymptomatic until severe, fatigue, dyspnea
treatment: restrict intake of K to 60-70 mEq, avoid salt subs, ecg monitoring
C BIG K DROP
C-calcium gulconate
B-beta 2 agonist
I insulin
G glucose
K kayaxalate
D diuertics
dialysis
how to explain this to patient: CKD progressed to stage 5, kidneys don’t work properly and cant filter out waste from blood so this will do it for them and replace it.
what are the options: hemodialysis and peritoneal dialysis
what to expect: nutrition therapy and fluid restrictions, daily weights
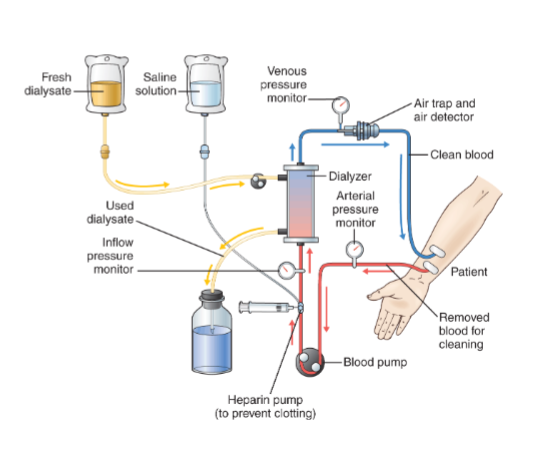
hemodialysis
how often does the patient receive: 3 times a week for 3-4 hours
where can it be performed: center for it, hospital, some at prisons
what type of diet should a patient be on, foods to avoid: low sodium, low potassium, low protein, high carb
types of access a patient could have, which is long term and which is short term:
AV fistula (surgical vein and artery together in forearm)- synthetic tube, first line to increase blood flow, cant use it right away(needs to mature first), permeant
AV graft- synthetic tube placed between an artery and vein, permanent
Central venous catheters: Inserted into subclavian, internal jugular, or femoral vein
Subcutaneous devices: Surgically implanted ports with catheters in large central veins
Temporary access requires longer treatment time (4-8 hours) due to smaller catheter lumens
complications: infection, equilibrium syndrome(nausea, vomiting, seizures, coma), cardiac events, low bp, hemorrhage, dizziness, weak, cramping
nursing assessment: full set of vitals before and afterwards, blood sugar, weight, changes in mental status, drowsiness, fatigue
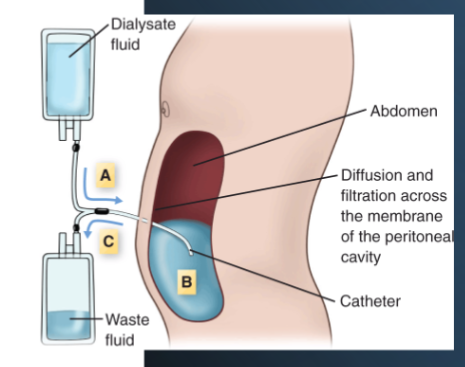
peritoneal dialysis
how often is it received: every day for 8-10 hours
where is it performed: home- usually when sleeping
why does a patient receive this and not HD: if they couldn’t get a fistula or graft (access problems), when waiting for AV fistula to mature
different types of access: abdomen (surgically placed)
contraindications: recent abdominal surgery, excessive scaring in peritoneal region
complications, nursing interventions: peritonitis- infections of peritoneum or blood vessels in stomach- fluid will look cloudy (prevent by maintaining sterility when touching catheter)
nursing assessment: watch fluid may look cloudy if its peritonitis, pain level
peritonitis
complication of peritoneal dialysis
infection of peritoneum or blood vessels in stomach
fluid will look cloudy and painful
prevent this by maintain sterility
diagnostic- culture the fluid
fluid overload
commonly seen in kidney disease patients
edema, crackles, abdominal girth, overweight
worried most about: pneumonia
indicated: call the doctor, obtain CBC and BNP, request order for chest x ray, obtain wound culture from infected dialysis site, obtain second IV access
nonindicated: blood sugar, extra fluids, request order for creatine clearance test(already know he has kidney disease), provide education to PD care(will do this eventually but not in an emergency situation)
failure to rescue
hyperkalemia can quickly lead to further damage or patient death
failure to recognize early cues
reasons why signs of inflammation occur
heat/redness- due to increased blood flow to site of inflammation
swelling-accumulation of fluid and cells
acute inflammation
predominant cell- neutrophil
time course- rapid onset
nature of response- physiologic
tissue dmaage- usually mild and resolves wquickly
chonric inflammation
macrophage and t lymphocyte
slow onset, long lived
pathologic
often severe and progressive
what labs indicate the presence of inflammation
CBC-WBC
c reactive protein
esr
which type of food would the nurse teach a patient with chrons disease to avoid
wheat
which medication would the nurse amdinister iv to a pateint with chrons disease who reports numbness, tingling, and painful muscle contractions and whose deep tendon reflexes are hyperactive on examination
magnesium sulfate
which patient goal wiudl the nurse establish when providing care for a pateint admitted with hypocalcemia secondary to chrons disease and sevre diahrea
negaive chvostek sign
ulcerative colitis diet
flaxseeds
pateit with ulcerative colitis is rpecsirbed sulfasalazine and corticosteriod therapy, whihc change would the nurse expect in the patients medication regimen would occur
corticosteriods would eb tapered
which nursing action would help minimize a pateients discomfort when experiecing an exacerbation of ulcerative colitis
restricting lactose containing foods, rest in bed(dont walk)
which potential complication is associated with chrons disease
fistulas, osteoporosis, malabsorption, abscess formation
chrons disease
can involve any part of the gi tract, often affects the colon and terminal ileum
signs: RLQ abdominal pain, chronic diarrhea, weight loss, steaturia(fatty stools), fatigue,
have an increase risk for fistula formation that can cause bladder infections, dehydration
malabsorption risk- usually vitamin b12 deficiency anemia, low potassium, low albumin, low protein
diagnostics- colonoscopy with multiple biopsies of colon and terminal ileum, inflammation may have a skip area with normal appearing mucosa. small bowel may show cobblestone appearance. capsule endoscopy may help when traditional endoscopy cannot visualize the entire small intestine
labs: elevated crp and esr, low albumin(malabsorption), low Hb(anemia), low potassium
complications: fistulas(abnormal tunnel forms between the bowel and another structure: drainage, fever, pain, infection skin irritation) , strictures(chronic inflammation and scaring can narrow the bowel lumen: cramping, pain, distention, n/v) may be present in urinary tract- SIGN IS TAN COLORED URINE, perforation(severe abdominal pain, rigid board like adomen, high hr, low bp, fever), abscesses: localized pocket of infection may form in the bowel wall or surrounding tissue: fever, localized abdominal pain, tenderness, leukocytosis; could need antibiotics, drainage, or surgery
treatment: D5 half normal saline, infliximab, methyl prednisone, loperamide, not treated with surgery only complications are
PRIORITY CONCEPT IS NUTRITION
nursing considerations: assess stool, don’t restrict fluid, monitor weight, don’t limit meals, daily calorie count, low fiber/low fat diet/high protein,
effective treatment plan: monitor bmp, increase in albumin, decrease in stool frequency, increase in weight, decrease in crp(FIRST) and esr, normal colored urine
ulcerative colitis
colon issue
signs/symptoms: bloody loose stools, abdominal cramping, fatigue, presence of melena in the stool, intolerance to milk/milk products, use of NSAIDS for pain, low hr, sudden urge to have bowel movement(tenesmus), weakness, dehydration
more blood loss- iron deficiency anemia
diagnostics: every 10 years colonoscopy biopsy(will show inflamed hemorrhagic mucosa, ulcerations, and irregular mucosa), stool culture rules out infection as cause
labs: low iron, low Hb, low albumin(hypoalbuminemia), low serum potassium, elevated esr
treatment: sulfasalazine, methyl prednisone, diphenoxylate, surgery(laparoscopic surgery), ileostomy placed in small intestine, colostomy in colon
nursing consideration: monitor stool, don’t hold sulfanzine for a systolic bp below 100, dont give NSAIDS, monitor bmp, don’t encourage ambulation, get bedside commode, monitor if no stool is passed
education: preop, colostomy care(monitor skin, stool will form 2-3 days postop, avoid caffeine/spicy/gassy foods/nuts/veggies with skin/rice/tomato’s/corn/peas, empty when halfway full, change pouch every 3-7 days, loose stool is normal for ileostomy, stoma is red and moist)
complications: perforation(toxic megacolon—>sepsis/hypovolemic shock)-(hr increase, bp decrease, absent bowel sounds, distended abdomen-NOTIFY RRT)
continuous inflammation
first line medication treatment for ulcerative colitis
sulfasalazine
signs of low potassium
heart palpitations
dysrythmias
what is priority before administering infliximab
screen for TB
lab test to monitor when taking sulfasalazine
cbc- can cause blood disorder and anemia
liver fucntion
renal fucntion
which complciations are assoicated with crohns disease
fistula formation
bowel obstruction
malabsportion
perforation
ulcerative colitis vs Crohn’s
UC: confined to rectum and colon(continuous), bleeding more likely, more at risk for colon cancer, diarrhea with puss and blood, could be asymptomatic, cause is unknown, inflammation, edema, fluid and electrolyte loss, malnutrition, iron deficiency anemia
Crohn’s: whole gi tract, noncontinuous, all the layers of the intestinal wall, cobblestone appearance on colonoscopy that stop body from absorption nutrients, fistulas, obstruction, fissures, abbesses, vitamin b12 anemia
pulmonary embolism
continuous pulse ox, montior vitals, lung sounds, cardiac status every 1-2 hours, assess for dyspnea, dysrythmias, crackles, cyanosis
anticoagulants and monitor labs
signs: sudden sob, pleuritic chest pain(sharp/ stabbing that intesifies when you cough), hemoptysis(coughing up blood), anxiety, restlessness, pain raidating to shoulder
nursing interventions: oxygen via 100% rebreather, anticogaualtion, monitor PTT/INR, asses repsirtory status, call RRT FIRST, ecg, abg(alkolosis), d dimer, heparin drip
assessment findings: PESTO (pleuritic chest pain, elevated rr, sob, tahcycardia, o2 decreased)
risk factors: FAT BAT(fracture/recent surgery, a fib, travel, birth control, active cancer, tobacco use
prveention/care: HAD CLOTS (hydration, ambulation, dvt prevention, compression devices, leg exercises, obsevre for sudden chest pain, teach antigoaluation safety, stop smoking
b12 deficency anemia
signs/ symptoms: fatigue, pale, skin, paresthsia of the ahnds and feet, glossitis(beefy red tongue), difficulty with balance, decreased HGB, tachycardia
treatment: b12 injections, b12 nasal/oral, animal proteins, fish, eggs, nuts, dairy, beans, citrus, leafy greens, VEGANS/VEGETARIAN: fortified cereal, cheese, supplement, synthetic meat, seafood
iron defenicey anemia
signs: fatigue, pale skin, fissures in the corner of the mouth, decreased hgb, tachycardia, low ferritin(10-15)
treatment: ferrous sulfate, ferumoxytol, iron dextran, red meat, organ meat, egg yolks, kidney beans, leafy greens, raisins, iron and vitamin c
impauired gas exhcnage early manifestations and late manifestations
early: tahcypnea, tachycardia, restlessness, anxiety, mild dyspnea on exertion, pale skin/mucous membranes
late:sevre dyspnea at rest, cyanosis, confuasion, dysrythmias, hypotension, syncope, distended neck veins, crackles in lungs, cardaic arrest/ shock
a client with pancreatitis should avoid what becuase it can tirgger pancreatic stu=imulation
fatty/fried foods, alcohol
biliary system
liver: makes bile
gallbladder: stores and concentrates the bile
pancreas: exocrine: secretes hormones in the blood stream (insulin/ glucagon) endocrine: helps blood sugar levels
whihc symtpom of postcholecystectomy syndrome shiudl the pateitn report
vomitig, diarrhea, epigastric pain
if a patient wqith acute pancreatitis isnt able to eat fter 48 hours what shoudl the nurse do
j tube feedings
what would the nruse montior to ebulate efefctiveness of pancreatic enzyme tehrapy
consistiency and number of stols
cholecystitis
risk factors: obesity, hyperlipidemia, female, pregnancy, rapid weight loss(body is more likely to develop stones), high fat diet, estrogen therapy(increases cholesterol saturation in the bile)
signs: RUQ epigastric pain that radiates to right shoulder, vomiting, diarrhea, pain after eating fried foods, nausea, rebound tenderness, dehydrated
PRIORITY CONCEPT: pain
expected orders: npo, fluids, pain relief(opioid for severe and ketorlac for moderate), nausea relief (monitor tele), ultrasound, HIDA csan
treatment: cholecystectomy(gallbladder removal:open/closed; carbon dioxide gas inflates abdomen, laparoscope is inserted through port, images transmitted to monitor, surgeon grasps gallbladder and clips off main arteries, drops into specimen bag, port valve left in place to left carbon dioxide escape, if there are complications they cut open more)
after surgery what is expected and whats concerning:
expected: mild shoulder pain, small amount of serosanguinous drainage, wbc slightly elevated
unexpected: fever, increasing abdominal distention
education: shoulder pain after surgery from carbon dioxide(encourage ambulation, heat in painful area), typically same day surgery, don’t soak in tub, ice on and off for 20 min for stomach/incisional pain, post cholceectomy syndrome (avoid fatty foods bc you have intolerance) low fat diet(can still develop gallstones even if gallbladder is out), ambulate, incentive spirometry, no ng tube needed, no pca pump, iv fludis and clear liquids until po is tolerated, no drains, can return to activies in a week, shower day after surgery, surgical glue will fall of naturally,
notify surgeon if vomiting, returning pain, signs of infection, opening of incision, delayed wound healing, fever
pancreatitis
risk afctors: alchol use, gallstones, hypertriglyceridemia
signs: epigastric pain radiating to back, pain worse when supine, elevated alt, amylase, wbc, lipase, glucose, low calcium,
secreting enzymes too early that results in auto digestion and leads to fibrosis of the pancreas
ask: when did the pain start( after fatty foods/when drinking), is it worse when supine, rating, location, characetristics, what makes it better/worse, radiating?, history of cholecystitis(gallstones and ercp(takes out gallstones) put them at higher risk)
assess: respiratory function, may find diminished breath sounds, grey/blue discoloration around umbilicus (putting pressure on it), bowel sounds(absence can show paralytic ileus), pancreatcileus(gaurding reboudn tnederness)
PRIORITY: reduce pancreatic stimualtion by decreasing gi motility, PAIN DECREASE
interventions: npo, possible ng tube, administer iv fluids, montior output hourly(shows they have proer perfusion), administer pain meds
education: small frequent meals(moderate to high in carbs, high in protein, low fat, bland/no spices), npo to decrease pancreatic enzyme secretion, respiratory distress syndrome(could happen in aucte and chornic)
acute expected/worsening condition:
expected: elevated lipase, epigatsric pain raidating to back, hyperglycemia
worsening: cullen sign(grey blue of stomach), hypotension, hypocalcemia
if worsening signs are showing hypovolemic shock may be happening (low bp, high hr, high rr, low o2, low urine output)
a pateint has just undergone a laproscopic cholesectomy is reporting shoukder pain . what si the cuase of this pain
carbon dixoide gas
barium enema
indications: to detect IBS (Crohn’s or ulcerative colitis) shows polyps, tumors, strictures, ulcers. tube that goes in rectum and contrast goes through
prep: npo, take laxatives the day before the test (magnesium sulfate), cleansing enema
recovery: monitor stool color
patient teaching: hydrate, take laxatives because the barium might cause constipation
colonoscopy
indications: IBS biospy (to confirm or assess for colorectal cancer). get biopsy to remove polyp, shows entire large bowel
prep: npo and bowel cleansing for 8 hours, clear/liquid diet for 1-3 days before, drink electrolytes, avoid red/purple/orange since it looks like blood
recovery:
patient teaching: signs of bowel perforation (fatigue bleeding)
HIDA scan
indications: to detect cholecystitis. flow in biliary system, to see if gallstones are blocking anything. radioactive tracker that they inject into the veins
prep: npo 4-6 hours before, no opioids since it slows down everything
recovery: assess for allergies
patient teaching:
ERCP
indications: visualize liver, gallbladder, pancreatic duct. use contrast dye. can be diagnostic or treatment (can remove gallstones).
prep: npo for 6-8 hours
recovery: can cause perforation, hypovolemic shock, abdominal pain and gas
patient teaching: can cause pancreatitis
which statement is true abotu the differences in the anataomy and physiology between infants and older children. infants have
a porportionally larger tongue than older children
anatomy in inafnts that cause difficulty in oxygenation
larger tongue
more narrow trachea
immature airway, more floppy
mostly breathe through their nose(tachypnea, tachycardia)-suction mucus
get tired quicker-dont have high stamina
immature immune system
fewer and smaller alveoli
moire mucous memebrane cewlls
at what age may a child with sickle cell disease first experience dactylitis
6 months
when youre first bone you have fetal hemoglobin at 5-6 months it converts to hemoglobin a which is what normal people ahve if you dont have sickle cell
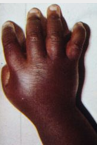
dactylitis
inflammation/swelling of fingers or toes as a result or acute sickle cell
6 months
treatments: would give anti-inflammatory (ketorolac), penicillin everyday, give opioid as if they had a VOE in arm/leg, IV fluids
what would you not do with acute chest syndrome
nebulized racemic epinephrine
acute chest syndrome
chest/back pain, fever
kinda like pneumonia for specifically sickle cell patients
do cbc, wbc may be high so it requires antibiotics
splenic sequestrations
blood pooling into spleen(protects against infection)
hgb will be low because blood is not circulating anymore
lethargic, irrtable, low hgb
palpate spleen
sickle cell
Two kinds:
-acute- CVA (stroke), acute chest syndrome, splenic sequestration, Priapism, Bacteremia(bacteria in the bloodstream), VOE/VOC(when rigid, sickle-shaped rbc block small blood vessels, restricting blood flow and causing sudden, severe, and potentially damaging tissue ischemia and pain), Dactylitis(swelling)
-chronic- low hemoglobin, tachycardic, Hyperbilirubinemia (dying rbc), HgbS, Elevated reticulocyte count (bone marrow is working overtime to produce immature rbc-if its normal it would be a sign the body isn’t making enough rbc), Elevated sedimentation rate (rbc settle faster than normal)
bone marrow makes- wbc, rbc, platlets
considerations: avoid steroids
treatment- stem cell transplant,
which is included in the assessment of an infants respiratoryv status
retractions
which is considered a risk factor for respiratory syncytial (RSV)
formula fed babies and preemies
male at higher risk than females
obtaining general history for oxygenation RSV
start narrow to broad
questions: what symptoms, when did it start, risk factors/history, vaccinations, who lives at home, siblings, daycare, etc, exposed to smoke, diet, family history(asthma), travel, gestational age, apgar, nicu, elimination(do they have less or the usual amount of dirty diapers)
assessment-retractions, o2, rr
virus can cause what
bronchiolitis (lower airways)
rsv, flue, covid, metapneumo—> cough, rhinorrhea, fever, wob, dehydration
larygngotracheobronchitis LBT
signs: barky cough/seal like cough, retractions, low grade fever, tachycardia, high rr, stridor, hypoxemia, stridor,
upper airway problem
gradual onset, pulse ox
interventions: steam to open airway, sit upright, blast of cold air, monitor
treatment- racemic epinephrine , dexamethasone
epiglottitis
sudden onset, hypoxemia, stridor, difficulty swallowing, intubate, tripod position, high fever
no pulse ox when they come in bc its a medical emergency
treatment- antibiotics