Lecture 8 - CNP
1/60
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
61 Terms
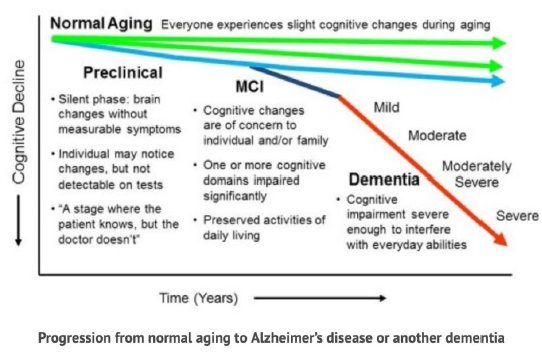
Forms of cognitive decline in aging (3)
• normal cognitive decline, abnormal aging
• with abnormal cognitive decline, there can be mild cognitive impairment and major cognitive impairment (=dementia)
• dementia can be caused by different forms of illnesses, e.g. Alzheimer’s, vascular problems in brain
What is normal aging associated with?
• with declines in certain cognitive abilities
What may contribute to changes with aging?
• declines in volume of gray and white matter + changes in white matter function
• changes are small and shouldn’t result in impairment in function
2 types of intelligence
• crystallized intelligence
• fluid intelligence
Crystallized intelligence (what is it, how does it change with age)
• skills, abilities, knowledge that are overlearned, well-practiced and familiar → e.g. vocabulary and general knowledge
• remains stable or improves with normal aging
Fluid intelligence (what is it, how does it change with age)
• abilities involving problem-solving and reasoning
• processing speed and executive functions
• declines with normal aging
Cognitive changes in processing speed
• declines with age → fluid intelligence
Cognitive changes in attention
• no declines in simple tasks
• declines in complex tasks
→ fluid intelligence
Cognitive changes in memory
• mixed declines with age → fluid intelligence
Cognitive changes in language
• in general: no decline
• but declines in visual confrontation naming, verbal fluency
→ more crystallized than fluid intelligence
Cognitive changes in visuospatial abilities
• simple tasks: no decline
• cognitive tasks: decline
→ mixed intelligence
Cognitive changes in executive function
• mixed decline with age → fluid intelligence
Which types of memory decline with age? (3)
• delayed free recall → spontaneous retrieval of information from memory without cue
• source memory → knowing source of learned information
• prospective memory → remembering to perform intended actions in future
Which types of memory remain stable with age? (3)
• recognition memory → ability to retrieve information when given cue
• temporal order memory → memory for correct time or sequence of past events
• procedural memory
Structural and functional changes in normal cognitive aging (3)
• cortical thinning and gray matter volumetric brain shrinkage
• decreased white matter density → esp. frontal + occipital regions
• loss of dopaminergic receptors → attentional dysregulation, executive dysfunction, difficulty with contextual processing
Protective factors for “successful” cognitive aging (3)
• lifestyle
• cognitive reserve
• cognitive retraining
Protective lifestyle factors for successful cognitive aging (4)
• intellectually engaging activities → puzzles, discussion groups, reading, using PC, bridge, board games, musical instrument, careers with high complexity, high educational attainment
• physical activities and active and healthy lifestyle → exercise, esp. which improves cardiovascular health, gardening, dancing
• social engagement/social stimulation → travel, cultural events, socializing with friends and family
• limit cardiovascular risks
Cognitive reserve
• = flexibility and adaptability of brain or networks to cope with brain damage
• positively associated with levels of education + associated with way of life
Cognitive retraining
• teaching strategies to improve memory, reasoning and speed of processing → results very inconsistent
dementia
• umbrella term for number of neurological conditions, distinct from mental illness
• major symptom: decline in cognitive function due to physical changes in brain
Types of neurocognitive disorders in DSM-5 (2)
• mild cognitive impairment (MCI) → minor neurocognitive disorder
• dementia → major neurocognitive disorder
Main difference between MCI and dementia
• ability to function independently in daily life still relatively intact in MCI
Diagnostic criteria for MCI according to DSM-5 (5)
• modest cognitive decline:
→ concerns about mild decline compared with previous level of functioning
→ modest impairment documented by objective cognitive assessment (1-2 standard deviations below mean)
• no interference with independence in everyday activities
• cognitive problems don’t occur in context of delirium of another mental disorder
Prognosis of MCI (3)
• MCI can be precursor of all forms of neurodegenerative diseases
• proportion of people with MCI don’t have underlying neurodegenerative disease
• chance to develop dementia within 5-10 years after MCI diagnosis on average ~50%
Progression from normal aging to Alzheimer’s disease or another dementia
Neurobiological and neuropathological changes in MCI
• MCI may be associated with early stages of changes that are associated with dementia
Treatment of MCI (3)
• no proven intervention effective in decreasing symptoms of MCI, or delaying or preventing progression of MCI to dementia
• reassessment if needed to monitor progression of MCI
• psychoeducation and cognitive training
Diagnostic criteria for dementia in DSM-5 (5)
• significant cognitive decline in one/more cognitive domains:
→ concerns about significant decline compared with previous level of functioning
→ substantial impairment documented by objective cognitive assessment (>2 sd below mean)
• interference with independence in everyday activities
• cognitive problems don’t occur in context of delirium or another mental disorder
How is the etiological subtype of dementia defined?
• by underlying brain pathology
3 main etiologies of dementia
• Alzheimer’s disease (and variants)
• vascular disease
• Frontotemporal Dementia (spectrum)
Other etiologies of dementia (10)
• Lewy bodies
• Huntington’s disease
• Parkinson’s disease
• HIV
• TBI
• Prion disease (Creutsfeld Jacobs)
• Medication, substance use
• other somatic causes
• multiple etiologies (e.g. mix vascular & AD)
• unspecified
Alzheimer’s disease
• neurodegenerative disease that causes dementia
• most common cause of dementia, accounts for ~70% of all dementia cases
Clinical presentation of AD (5)
• first + most prominent symptom: gradually progressive memory loss
• some cases atypical clinical presentation starting with predominant language, visual, executive or behavior impairments (variants)
• as AD progresses, multiple cognitive domains become affected
• neuropsychiatric symptoms such as depression, apathy, anxiety also common
• final stage: overall cognitive loss and person completely dependent on their environment
Diagnostic criteria of AD (4)
Determine clinical syndrome of major neurocognitive disorder
Vague onset and gradually progressive course (months to years)
Cognitive impairment involves minimum of 2 of following domains: memory, executive functions, language, visuospatial functions
No evidence of substantial concomitant cerebrovascular, neurological or psychiatric disease that could explain cognitive symptoms
How can the level of certainty be further increased based on additional evidence? (3)
• formal neuropsychological evaluation
• neuroimaging (CT, MRI, PET) or cerebrospinal fluid analysis
• evidence of causative AD genetic mutation (very rare)
Neuropathology of AD (4)
• abnormal accumulation and deposition of extracellular plaques of amyloid-beta protein
• intracellular tangles of protein tau
→ leading to degeneration of nerve cells and ultimately brain atrophy
→ can only be confirmed post-mortem
Non-modifiable risk factors for AD (3)
• older age
• female sex
• genetic predisposition
Potential causes of AD (3)
• amyloid cascade hypothesis
• vascular hypothesis
• both hypotheses combined
Amyloid cascade hypothesis
• abnormal accumulation of amyloid-beta protein is primary driver of AD, so clearing amyloid-beta plaques main focus of new therapies → clinical efficacy inconclusive
Criticism of amyloid cascade hypothesis (3)
• lack of coherent evidence
• not yet clear whether plaques and tangles are cause of AD or consequence
• failure to provide effective treatment
Vascular hypothesis
• vascular risk factors lead to reduced blood flow and oxygen deficiency in brain → leads to metabolic reaction that causes overproduction of amyloid-beta protein
Modifiable risk factors for AD → lifestyle changes (11)
• higher education
• prevention of TBIs
• prevention of hypertension
• little alcohol consumption
• prevention of obesity
• no smoking
• prevention of depression
• prevention of social isolation
• physical activity
• prevention of air pollution
• prevention of diabetes
What are most reported cognitive complaints that patients initially present with? (3)
• difficulty remembering recent events
• forgetting appointments
• word-finding problems
Clinical course of AD can be divided into which stages? (4)
(• Preclinical AD)
• MCI
• Mild dementia
• Moderate dementia
• Severe dementia
Clinical Dementia Rating (CDR)
• semi-structured interview to assess clinical stage of AD
Mild dementia (CDR1) (2)
• problems in other cognitive functions start to emerge: language production, orientation in time and place, planning and performing activities
• leading to clear limitations in life
Moderate dementia (CDR2) (3)
• more extensive cognitive impairments occur
• person increasingly dependent on others in daily life
• basic activities of daily living, e.g. dressing, become more difficult
Severe dementia (CDR3) (4)
• final stage
• completely dependent
• confused
• incontinent
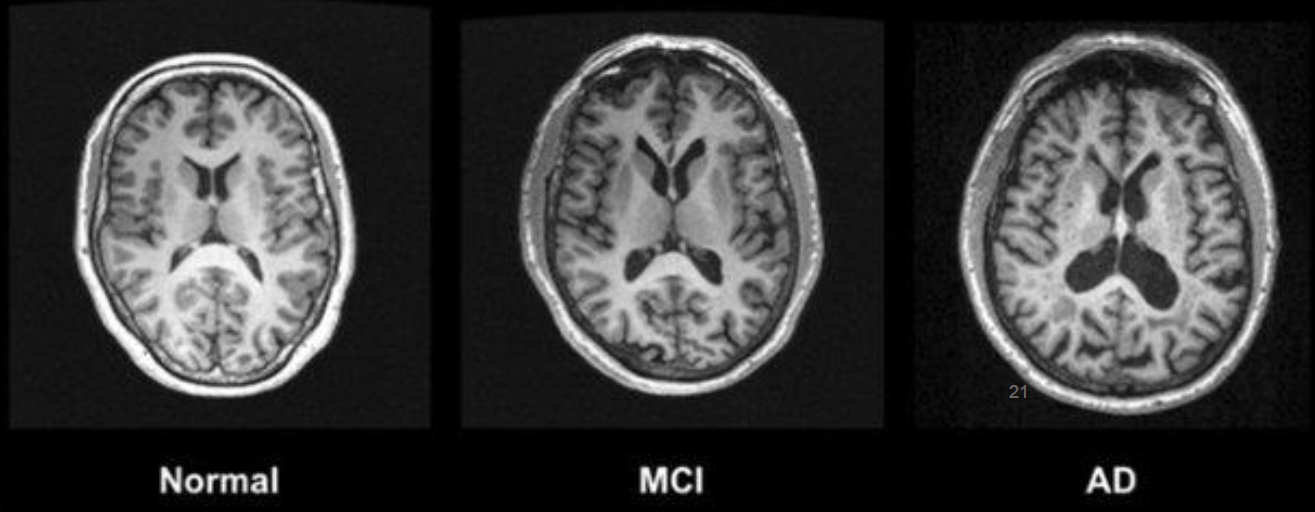
Brain changes in AD in structural neuroimaging (CT/MRI) (3)
• extreme shrinkage of cerebral cortex
• severely enlarged ventricles
• extreme shrinkage of hippocampus
Brain changes in AD in EEG
• slowing of alpha activity
Brain changes in AD on PET-scan
• reduction in cerebral metabolic rate for glucose
What is the clinical diagnosis of AD currently based on?
• (medical) history of patient
• clinical examination
• neuroimaging (CT, MRI, or PET)
• neuropsychological testing
Diagnostic cycle (4)
Complaints analysis → clinical interview
Problem analysis → neuropsychological assessment, assessment of neuropsychiatric symptoms, assessment of other symptoms
Diagnosis
Indication for treatment
Who to conduct clinical interview with and why? (3)
• with patient and close relative
• reduced insight into deficits (anosognosia)
• patients with dementia/AD commonly deny/trivialize complaints
Which questions to ask during clinical interview (7)
• subjective complaints of cognitive dysfunction (e.g. memory, concentration,…)
• onset + progression of cognitive problems
• psychiatric symptoms (e.g. mood and anxiety)
• level of independence (activities of daily functioning)
• assessment of global cognitive functioning with screening test (e.g. MMSE)
• family and medical history
• medication use
What to assess in neuropsychological assessment (4)
• memory (declarative episodic memory) → early stages: anterograde long-term memory impairment, later stages: also retrograde memory impairment and semantic memory problems
• executive function and problem solving → cognitive flexibility and planning problems
• attention → mental flexibility and divided attention problems
• other cognitive problems, e.g. visuospatial perception, language, or apraxia
Which tests can be used in neuropsychological assessment? (6)
• Visual association test
• Word recall (list, short stories)
• Trail Making Test
• Stroop Test
• Digit span
• Clock drawing
Neuropsychiatric symptoms in AD (8)
• depression
• anxiety
• apathy, social disengagement and/or irritability
• psychosis (incl. hallucinations and/or delusions)
• agitation, aggression, and/or wandering
• motor unrest
• sleeping problems
• eating problems
Other possible symptoms in AD (3)
• olfactory dysfunction
• seizures (10-20% of cases, usually in later stages of disease)
• motor signs (typically in later stages of disease)
Treatment options for AD (4)
• can’t be cured, but medication to inhibit cognitive symptoms to certain extent:
→ Cholinesterase inhibitors for patients with mild to moderate AD
→ Memantine (N-Methyl D-aspartate antagonist) for patients with moderate to severe AD
• psychoeducation
• cognitive training (early stages)
• manage behavioral symptoms