GW BGZ2026 Case 1 - Therapeutic and toxic effects of compounds - a matter of dose and timing?!
1/49
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
50 Terms
Describe the anatomy of the kidney and explain the function of each major part.
The kidneys are two bean-shaped organs located retroperitoneally on either side of the spine, just below the rib cage. Their primary functions are filtering blood, removing waste products, regulating water and electrolyte balance, maintaining acid-base balance, and producing hormones such as renin and erythropoietin.
The major anatomical structures include:
Renal cortex: The outer region where blood filtration begins. It contains the glomeruli and the proximal and distal convoluted tubules.
Renal medulla: The inner region consisting of renal pyramids that contain loops of Henle and collecting ducts.
Renal pyramids: Funnel urine toward the renal papillae.
Minor and major calyces: Collect urine from the renal pyramids.
Renal pelvis: A funnel-shaped chamber that collects urine before it enters the ureter.
Ureter: A muscular tube that transports urine to the urinary bladder through peristaltic contractions.
Explain the structure of a nephron and describe the function of each component.
The nephron is the functional unit of the kidney, with approximately one million nephrons in each kidney. Each nephron consists of:
Glomerulus: A network of capillaries where blood filtration occurs. Water and small molecules pass into Bowman's capsule while proteins and blood cells remain in the circulation.
Bowman's capsule: Surrounds the glomerulus and collects the filtrate.
Proximal convoluted tubule (PCT): Reabsorbs about 65% of filtered water and sodium, nearly all glucose and amino acids, bicarbonate, and chloride.
Loop of Henle: Creates the osmotic gradient necessary for concentrating urine. The descending limb allows water to leave, while the ascending limb pumps sodium and chloride out but is impermeable to water.
Distal convoluted tubule (DCT): Fine-tunes electrolyte concentrations, especially under the influence of aldosterone.
Collecting duct: Performs the final adjustment of urine concentration. ADH increases water reabsorption here by inserting aquaporin channels.
Describe the three major processes involved in urine formation.
Urine formation consists of three processes:
Glomerular filtration: Blood pressure forces water and small solutes through the filtration membrane into Bowman's capsule while proteins and blood cells remain in the bloodstream.
Tubular reabsorption: Useful substances such as water, glucose, amino acids, sodium, chloride, and bicarbonate are transported back into the blood. This prevents loss of essential nutrients and maintains fluid balance.
Tubular secretion: Additional substances, including hydrogen ions (H⁺), potassium ions (K⁺), drugs, and toxins, are actively transported from the blood into the nephron. This helps regulate pH and eliminate harmful compounds.
Explain how ADH regulates water balance.
Antidiuretic hormone (ADH), also called vasopressin, is released from the posterior pituitary when plasma osmolarity increases or blood volume decreases. ADH binds to receptors on collecting duct cells, causing insertion of aquaporin-2 water channels into the membrane. This greatly increases water reabsorption back into the bloodstream. As a result, urine volume decreases, urine becomes more concentrated, blood volume increases, and plasma osmolarity decreases. Without ADH, large amounts of dilute urine are produced.
Explain the Renin–Angiotensin–Aldosterone System (RAAS).
RAAS is activated when blood pressure or blood volume falls.
The sequence is:
Juxtaglomerular cells in the kidney release renin.
Renin converts angiotensinogen (from the liver) into angiotensin I.
Angiotensin-converting enzyme (ACE), mainly in the lungs, converts angiotensin I into angiotensin II.
Angiotensin II:
causes vasoconstriction,
stimulates aldosterone release from the adrenal cortex,
stimulates ADH release,
increases thirst.
Aldosterone promotes sodium reabsorption and potassium secretion in the distal tubule and collecting duct. Water follows sodium, increasing blood volume and blood pressure.
How does the sympathetic nervous system regulate kidney function?
During stress, exercise, or blood loss, the sympathetic nervous system becomes activated. Sympathetic nerves constrict the afferent arterioles supplying the glomeruli, reducing renal blood flow and glomerular filtration rate (GFR). Less filtrate is formed, resulting in decreased urine production. Sympathetic stimulation also promotes renin release, activating RAAS. These responses conserve water and sodium while maintaining blood pressure during emergencies.
What is molar mass, and how is it used in calculations?
Molar mass is the mass of one mole of a substance and is expressed in grams per mole (g/mol). It is calculated by adding the atomic masses of all atoms in the chemical formula.
For example, NaCl has:
Sodium (Na): 22.99 g/mol
Chlorine (Cl): 35.45 g/mol
Therefore, the molar mass is 58.44 g/mol.
The formula relating mass and moles is:
Moles = Mass ÷ Molar mass
For example:
11.7 g NaCl ÷ 58.44 g/mol = 0.20 mol.
Explain molarity, mg/L, and how standard curves are used.
Molarity (M) is the number of moles of solute dissolved per litre of solution.
Formula:
Molarity = Moles ÷ Volume (L)
Example:
0.2 mol dissolved in 1 L equals 0.2 M.
Mass concentration is often expressed in mg/L.
Example:
500 mg dissolved in 2 L equals 250 mg/L.
A standard curve is used to determine the concentration of an unknown sample. Known standards are prepared, their absorbance is measured, and a graph of absorbance versus concentration is created. The absorbance of an unknown sample is then measured, and its concentration is determined by comparing it to the graph.
Describe the four layers of the digestive tract wall.
Every section of the gastrointestinal tract contains four basic layers:
Mucosa: The innermost layer consisting of epithelium, lamina propria, and muscularis mucosae. It is responsible for secretion, absorption, and protection.
Submucosa: Contains connective tissue, blood vessels, lymphatic vessels, and the submucosal nerve plexus.
Muscularis externa: Composed of an inner circular and outer longitudinal muscle layer that produce peristalsis and segmentation.
Serosa (or adventitia): The outer protective connective tissue layer. The serosa also reduces friction between abdominal organs.
Explain how carbohydrates, proteins, fats, and water are absorbed in the small intestine.
Carbohydrates are digested into monosaccharides such as glucose, which enter intestinal epithelial cells through transport proteins before entering the bloodstream.
Proteins are digested into amino acids and small peptides, which are absorbed into blood capillaries within the villi.
Fats require bile salts for emulsification. Pancreatic lipase breaks triglycerides into fatty acids and monoglycerides, which form micelles. Inside intestinal cells, they are reassembled into triglycerides, packaged into chylomicrons, and transported into lacteals before reaching the bloodstream.
Water is absorbed mainly by osmosis, following electrolytes and nutrients that have already been absorbed.
What are villi and microvilli, and why are they important?
Villi are finger-like projections lining the small intestine that greatly increase the surface area available for nutrient absorption. Each villus contains blood capillaries for absorbing sugars and amino acids, as well as a central lymphatic vessel called a lacteal for fat absorption.
Microvilli are microscopic projections on the apical surface of epithelial cells that form the brush border. They further increase the absorptive surface area and contain digestive enzymes that complete carbohydrate and protein digestion before absorption.
Explain the four components of ADME.
ADME describes how drugs move through the body.
Absorption: Movement of a drug from its site of administration into the bloodstream. Bioavailability depends on factors such as route of administration, pH, blood flow, and first-pass metabolism.
Distribution: Movement of the drug from blood into tissues. It depends on blood flow, lipid solubility, plasma protein binding, and tissue affinity.
Metabolism: Chemical modification of drugs, mainly in the liver. Phase I reactions involve oxidation, reduction, or hydrolysis, while Phase II reactions involve conjugation.
Excretion: Removal of drugs and metabolites, mainly by the kidneys through filtration, secretion, and reabsorption, although bile, sweat, saliva, and lungs may also contribute.
Describe Phase I and Phase II drug metabolism.
Phase I reactions introduce or expose functional groups on drug molecules. These reactions include oxidation, reduction, and hydrolysis, and are primarily catalyzed by cytochrome P450 enzymes such as CYP1A2, CYP2E1, and CYP3A4. Phase I reactions may activate prodrugs, inactivate drugs, or generate toxic metabolites.
Phase II reactions attach endogenous molecules such as glucuronic acid, sulfate, acetate, or glutathione to drugs. Enzymes including UGTs, SULTs, NATs, and glutathione-S-transferases catalyze these reactions. Conjugation increases water solubility, making drugs easier to eliminate through the kidneys.
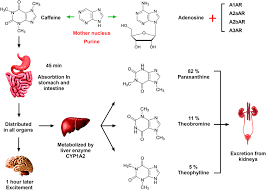
Explain the ADME of caffeine.
Caffeine is almost completely absorbed from the gastrointestinal tract, with nearly 100% bioavailability and peak plasma concentrations reached within 30–120 minutes.
It distributes throughout total body water, crosses the blood-brain barrier and placenta, and has a volume of distribution of approximately 0.6 L/kg.
Approximately 95% is metabolized in the liver by CYP1A2 into paraxanthine (80%), theobromine (10%), and theophylline (4%). These metabolites retain biological activity before being further metabolized.
Most metabolites are excreted in urine, while less than 5% of caffeine is eliminated unchanged.
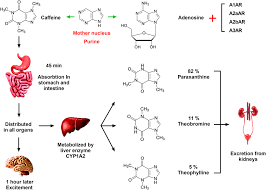
Explain the mechanism of action and metabolism of paracetamol.
Paracetamol relieves pain and reduces fever mainly by inhibiting cyclooxygenase (COX) activity within the central nervous system, reducing prostaglandin synthesis. A metabolite called AM404 may also activate TRPV1 receptors and enhance endocannabinoid signalling.
Most paracetamol undergoes glucuronidation (55–60%) by UGT enzymes and sulfation (30–35%) by SULT enzymes, producing non-toxic metabolites. About 5–10% is oxidized by CYP2E1, CYP1A2, and CYP3A4 to form the toxic metabolite NAPQI. Normally, glutathione conjugates NAPQI through glutathione-S-transferases (GSTs). In overdose, glutathione becomes depleted, allowing NAPQI to accumulate and cause severe liver damage.
Explain the mechanism of action and metabolism of ethanol.
Ethanol acts as a central nervous system depressant by enhancing GABA-A receptor activity, inhibiting NMDA glutamate receptors, and increasing dopamine release within the brain's reward pathway. It also affects serotonin, glycine receptors, calcium channels, and endocannabinoid signalling.
Most ethanol is metabolized in the liver by alcohol dehydrogenase (ADH), converting ethanol into acetaldehyde. Aldehyde dehydrogenase (ALDH2) converts acetaldehyde into acetate, which is transformed into acetyl-CoA and enters the citric acid cycle. Chronic alcohol consumption induces CYP2E1, increasing ethanol metabolism and reactive oxygen species formation. A minor pathway involves catalase in peroxisomes.
Explain first-pass metabolism and bioavailability.
After oral administration, drugs are absorbed from the intestine into the portal circulation and pass through the liver before entering the systemic circulation. During this first pass, liver enzymes may metabolize part of the drug, reducing the amount that reaches the bloodstream unchanged. This process is called first-pass metabolism.
Bioavailability is the fraction of an administered dose that reaches systemic circulation unchanged. Drugs with extensive first-pass metabolism have lower oral bioavailability and may require higher oral doses or alternative routes of administration.
Explain natural logarithms and how to read a natural logarithm scale.
The natural logarithm (ln) answers the question: "To what power must e (approximately 2.718) be raised to produce a given number?"
Important values include:
ln(1) = 0
ln(e) = 1
ln(7.39) = 2
ln(20.09) = 3
ln(54.6) = 4
On a natural logarithm scale, equal spacing represents multiplication by e rather than equal increases in value. For example, moving from ln = 2 to ln = 3 increases the actual value from approximately 7.39 to 20.09.
How do you convert between natural logarithms and normal numbers?
To convert a logarithm into a normal number, raise e to the given logarithm:
If ln(x) = 3, then x = e³ ≈ 20.09.
If ln(x) = 5, then x = e⁵ ≈ 148.41.
To calculate the natural logarithm of a number, use the ln function on a calculator:
ln(5) ≈ 1.609
ln(100) ≈ 4.605
Being able to move between logarithmic values and actual values is important when interpreting graphs with logarithmic scales.
Compare the major hormones involved in regulating kidney function.
Several hormones regulate kidney function to maintain fluid and electrolyte balance.
ADH increases water reabsorption in the collecting ducts, producing concentrated urine and increasing blood volume.
Aldosterone increases sodium reabsorption and potassium secretion in the distal nephron. Water follows sodium, raising blood pressure.
Renin initiates the RAAS cascade when blood pressure falls.
Angiotensin II causes vasoconstriction, stimulates aldosterone and ADH release, and increases thirst.
ANP (Atrial Natriuretic Peptide) is released when blood volume is high. It promotes sodium and water excretion, inhibits renin and aldosterone release, and lowers blood pressure. Together, these hormones continuously adjust kidney function to maintain homeostasis.
What is drug absorption, and what factors influence it?
Drug absorption is the movement of a drug from its site of administration into the systemic circulation.
It determines:
Rate of absorption → how quickly the drug begins to act.
Extent of absorption (bioavailability) → how much drug reaches the bloodstream.
Factors affecting absorption include:
Lipid solubility (more lipid-soluble drugs cross membranes more easily)
Drug ionisation (pH and pKa)
Molecular size
Surface area available for absorption
Blood flow to the absorption site
Gastric emptying and intestinal motility
Food intake
Drug formulation (e.g. immediate vs modified release)
Drug interactions
What is bioavailability, what is first-pass metabolism, and how do administration routes affect them?
Bioavailability (F) is the fraction of an administered dose that reaches the systemic circulation unchanged.
Intravenous (IV) administration has 100% bioavailability because the drug enters the bloodstream directly.
Oral drugs often have lower bioavailability due to:
Incomplete absorption
First-pass metabolism
First-pass metabolism is the metabolism of a drug in the:
Intestinal wall
Liver
before reaching the systemic circulation.
Routes that bypass first-pass metabolism include:
Intravenous
Sublingual
Transdermal
(Rectal administration partially bypasses first-pass metabolism.)
Describe the absorption of alcohol and the factors affecting blood alcohol concentration (BAC).
Alcohol is absorbed by passive diffusion.
Absorption occurs:
~20% in the stomach
~80% in the small intestine (duodenum and jejunum)
The small intestine is the major absorption site because it has:
Large surface area
Rich blood supply
Thin epithelial lining
The most important factor affecting absorption is gastric emptying.
Food:
Slows gastric emptying
Delays alcohol absorption
Reduces peak BAC
High-concentration spirits (>40%) may slow gastric emptying by irritating the stomach.
Women generally reach a higher BAC than men after consuming the same amount due to:
Lower total body water
Smaller volume of distribution
Describe the absorption and bioavailability of caffeine.
Caffeine is absorbed by passive diffusion.
It is absorbed mainly in the small intestine.
It has an oral bioavailability of approximately 90–100%.
Peak plasma concentrations (Tmax) occur within 30–120 minutes.
Food:
Delays gastric emptying
Delays Tmax
Has minimal effect on total bioavailability
Gastric pH has little influence on caffeine absorption.
Describe the absorption of paracetamol and the factors affecting it.
Paracetamol is absorbed mainly by passive diffusion.
Absorption occurs primarily in the:
Duodenum
Jejunum
Oral bioavailability is approximately 75–85%.
The most important factor influencing absorption is gastric emptying.
Food and opioids:
Slow gastric emptying
Delay absorption
Delay onset of analgesia
Peak plasma concentrations occur within:
30–60 minutes (immediate-release preparations)
What is drug distribution, and what factors influence it?
Drug distribution is the reversible movement of a drug from the bloodstream into tissues and body fluids.
Distribution depends on:
Blood flow to tissues
Capillary permeability
Lipid solubility
Plasma protein binding
Tissue binding
Molecular size
Highly perfused organs receive drugs first:
Brain
Heart
Liver
Kidneys
Less perfused tissues receive drugs more slowly:
Muscle
Fat
Bone
Only the free (unbound) drug is able to:
Leave the bloodstream
Bind to receptors
Produce pharmacological effects
Undergo metabolism and excretion
Explain plasma protein binding and volume of distribution (Vd).
Plasma protein binding limits the amount of free drug available.
Acidic drugs mainly bind to albumin.
Basic drugs mainly bind to α1-acid glycoprotein.
Only the unbound drug is pharmacologically active.
Volume of distribution (Vd) is the apparent volume that relates:
Amount of drug in the body
Plasma drug concentration
Interpretation:
Low Vd → drug remains mainly in plasma.
High Vd → drug distributes extensively into tissues.
Compare the distribution of alcohol, caffeine and paracetamol.
Alcohol
Distributes throughout total body water
Minimal plasma protein binding
Crosses the blood-brain barrier
Crosses the placenta
Vd: approximately 0.6–0.7 L/kg
Caffeine
Crosses the blood-brain barrier
Crosses the placenta
Protein binding: 10–35%
Vd: approximately 0.6 L/kg
Paracetamol
Distributes widely throughout body water
Crosses the blood-brain barrier
Crosses the placenta
Protein binding: 10–25%
Vd: approximately 0.9 L/kg
Describe the pharmacodynamic effects and mechanisms of action of alcohol
Acts as a central nervous system (CNS) depressant.
Affects multiple neurotransmitter systems simultaneously.
Mechanisms:
Potentiates GABA-A receptors
Increases inhibitory neurotransmission.
Results in:
Sedation
Anxiolysis
Impaired cognition and coordination
Inhibits NMDA (glutamate) receptors
Reduces excitatory neurotransmission.
Results in:
Impaired learning
Memory impairment
Cognitive slowing
Increases dopamine release in the mesolimbic reward pathway.
Produces:
Pleasure
Reinforcement
Addiction potential
Effects on other organ systems:
Cardiovascular
Low doses → Peripheral vasodilation
High doses → Myocardial depression
Endocrine
Inhibits antidiuretic hormone (ADH)
Causes:
Increased urine production
Dehydration
Liver (chronic use)
Steatosis (fatty liver)
Alcoholic hepatitis
Cirrhosis
Describe the pharmacodynamic effects and mechanisms of action of caffeine
Acts primarily as a CNS stimulant.
Primary mechanism: Adenosine receptor antagonism
Competitive antagonist of:
A1 receptors
A2A receptors
Normally adenosine:
Promotes sleep
Reduces neuronal firing
Blocking adenosine receptors increases neuronal activity.
Secondary mechanism: Phosphodiesterase (PDE) inhibition
Inhibits phosphodiesterase enzymes
Prevents breakdown of:
cAMP
cGMP
Increased cAMP produces:
Bronchodilation
Lipolysis
Increased cardiac contractility
Greater energy expenditure
Indirect neurotransmitter effects
Increases:
Dopamine
Norepinephrine
Acetylcholine
Physiological effects
CNS
Increased wakefulness
Improved attention
Reduced fatigue
Cardiovascular
Increased heart rate
Increased contractility
Respiratory
Bronchodilation
Kidneys
Mild diuretic effect
High doses may cause
Anxiety
Panic attacks
Arrhythmias
Describe the pharmacodynamic effects and mechanisms of action of paracetamol
Functions as a centrally acting analgesic and antipyretic.
Has minimal peripheral anti-inflammatory activity.
Mechanisms
Inhibits central cyclooxygenase (COX) activity.
Reduces prostaglandin synthesis in the brain and spinal cord.
Forms AM404, which contributes to analgesia.
Also interacts with:
Serotonergic descending pain pathways
Endocannabinoid system
TRPV1 receptors
Physiological effects
Analgesic
Reduces CNS prostaglandins involved in pain transmission.
Antipyretic
Acts on the hypothalamus.
Produces:
Lower temperature set point
Vasodilation
Sweating
Weak anti-inflammatory effect
Peripheral inflammatory tissues contain high peroxide concentrations that reduce COX inhibition.
What is drug metabolism?
Chemical alteration of drugs, mainly in the liver
Purposes:
Increase water solubility
Facilitate excretion
Usually terminate drug action
Can also:
Activate prodrugs
Produce active metabolites
Produce toxic metabolites
Compare Phase I and Phase II drug metabolism.
Phase I Reactions
Introduce or expose functional groups.
Processes:
Oxidation
Reduction
Hydrolysis
Main enzyme family:
Cytochrome P450 (CYP)
Phase II Reactions
Conjugation with endogenous molecules.
Examples:
Glucuronidation
Sulfation
Acetylation
Result:
More polar compounds
Easier excretion
Compare first-order and zero-order drug elimination.
First-order
Constant fraction eliminated
Rate depends on concentration
Most drugs
Zero-order
Constant amount eliminated
Occurs when enzymes become saturated
Examples:
Alcohol
Phenytoin
How are drugs excreted from the body?
Kidneys (urine) – major route
Bile/faeces
Lungs
Minor routes:
Sweat
Saliva
Breast milk
What are the three stages of renal drug excretion?
Glomerular filtration – filters only free drug
Tubular secretion – active transport into urine
Tubular reabsorption – depends on urine pH, ionisation and lipid solubility
Describe the metabolism of alcohol.
Mainly metabolised in the liver
Requires NAD⁺
Follows zero-order kinetics
Main pathway:
Ethanol → Acetaldehyde (ADH)
Acetaldehyde → Acetate (ALDH)
Acetate → Acetyl-CoA
Alternative pathways
MEOS (CYP2E1)
Induced by chronic alcohol use
Produces reactive oxygen species
Increases NAPQI formation from paracetamol
Catalase pathway
Minor pathway (<5%)
Occurs in peroxisomes
How is caffeine metabolised and excreted?
Metabolised mainly by CYP1A2
Major metabolites:
Paraxanthine (~80%)
Theobromine (~10%)
Theophylline (~4%)
Half-life: 3–7 hours
Excreted mainly in urine as metabolites
Describe normal paracetamol metabolism.
Phase II Pathways (90–95%)
These are the major detoxification pathways and produce non-toxic metabolites.
1. Glucuronidation (≈55–60%) Enzymes
UGT1A1
UGT1A6
UGT1A9
UGT2B15
Result
Formation of inactive paracetamol-glucuronide.
Excreted by the kidneys.
2. Sulfation (≈30–35%) Enzymes
SULT1A1
SULT1A3
Result
Formation of inactive paracetamol-sulfate.
Excreted in urine.
Key Point
Together, glucuronidation and sulfation account for 90–95% of normal paracetamol metabolism.
These are considered the normal detoxification pathways.
Minor Oxidation Pathway (5–10%) Phase I Oxidation Enzymes
CYP2E1 (most important)
CYP1A2
CYP3A4
Product
NAPQI (N-acetyl-p-benzoquinone imine)
Importance
NAPQI is a highly reactive and toxic metabolite.
Under normal circumstances, only small amounts are formed.
Detoxification of NAPQI Glutathione Pathway Enzyme
Glutathione-S-transferase (GST)
Process
NAPQI is rapidly conjugated with glutathione (GSH).
The resulting products are non-toxic and are excreted in urine.
Normal Situation
Adequate glutathione stores are available.
No liver injury occurs.
How does paracetamol overdose cause liver injury?
Phase II pathways become saturated
More drug enters CYP pathway
Increased NAPQI formation
Glutathione becomes depleted
NAPQI binds hepatocytes
Causes oxidative stress and hepatocyte necrosis
How does N-acetylcysteine (NAC) treat paracetamol overdose?
Replenishes glutathione stores
Provides cysteine for glutathione synthesis
Detoxifies NAPQI
Directly binds NAPQI when glutathione is depleted
Reduces oxidative stress
Improves hepatic blood flow
Most effective within 8 hours of overdose
What is clearance?
Drug clearance concepts are similar to clearance concepts of renal physiology. Clearance of a drug is the factor that predicts the rate of elimination in relation to the drug concentration (C):
Clearance, like volume of distribution, may be defined with respect to blood (CLb), plasma (CLp), or unbound in water (CLu), depending on where and how the concentration is measured.
What is rate of elimination?
The two major sites of drug elimination are the kidneys and the liver.
Measurement of unchanged drug in the urine may be used to determine renal clearance. Within the liver, drug elimination occurs via biotransformation of parent drug to one or more metabolites, or excretion of unchanged drug into the bile, or both.
Elimination of drug by the liver is difficult to measure directly, unlike renal elimination, so hepatic clearance is often assumed to be the difference between total systemic clearance and renal clearance.
For most drugs, clearance is constant over the concentration range encountered in clinical settings, ie, elimination is not saturable, and the rate of drug elimination is directly proportional to concentration: rate of elimination = CL x C
What is half-life?
Time required for drug amount or concentration to decrease by 50%.
Key relationship:0,693 x Vd/CL
Clinical importance:
Determines time to reach steady state.
Determines time needed for drug elimination after stopping therapy.
About 4–5 half-lives are needed to reach steady state or eliminate most of a drug.
What are the effects of combining caffeine and alcohol?
Alcohol is a central nervous system (CNS) depressant, while caffeine is a CNS stimulant. When combined, caffeine can reduce feelings of drowsiness caused by alcohol, making a person feel more alert. However, caffeine does not reduce blood alcohol concentration (BAC) or reverse alcohol-induced impairment.
Main effects of combining caffeine and alcohol:
Reduced perception of intoxication: People may feel less drunk than they actually are.
Impaired judgment remains: Decision-making, reaction time, and coordination are still affected by alcohol.
Increased risk-taking behavior: Individuals may be more likely to drive, continue drinking, or engage in risky activities.
Higher alcohol consumption: Feeling more alert may lead to drinking larger amounts of alcohol.
Cardiovascular effects: The combination may increase heart rate and cause palpitations in some individuals.
Sleep disturbance and dehydration: Both substances can contribute to poor sleep quality and dehydration.
What are AST and ALT, and how are they interpreted?
Enzymes released during hepatocyte injury
ALT
More liver-specific
AST
Also found in heart, muscle, kidney and brain
Normal range: ~8–40 U/L
Alcoholic hepatitis: AST:ALT >2:1
Paracetamol overdose: AST and ALT often >1000 U/L (may exceed 10,000 U/L)