Week 6, 11 and 12 PHAR3911
1/132
Earn XP
Description and Tags
Kidneys, Liver, and Solid-Organ Transplant
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
133 Terms
Functions of the liver
Metabolism (carbohydrates, lipids and protein)
Detoxification (drugs and toxins)
Storage (carbs, fats, protein, iron, vitamins)
Waste products removal (bilirubin)
Plasma protein synthesis (albumin, clotting factors)
Bile production
Filtration, phagocytosis and antigen presentation
Acid/Base balance (bicarbonate and H+)
Liver roles in carbohydrate metabolism
Glycogenesis (in response to insulin)
Glycogenolysis (in response to glucagon)
Gluconeogenesis (in response to glucagon)
Glucagon stimulates which processes in the liver?
Glycogenolysis
Gluconeogenesis
Insulin stimulates which process in the liver?
Glycogenesis
Liver roles in lipid metabolism
– Lipoprotein synthesis
– Oxidation of fats
– Synthesis of cholesterol, phospholipids, steroid hormones
– Metabolism of steroids
Jaundice, dark urine, pale stool is a sign of what?
Liver and biliary dysfunction - the bile is not clearing from the gallbladder (so bilirubin is building up systemically)
Liver roles in protein metabolism
deamination and transamination of amino acids
removal of ammonia via urea formation
synthesis of amino acids
Hepatic encephalopathy is a sign of liver dysfunction in which area of metabolism?
Impaired hepatic protein metabolism - impaired removal of ammonia toxin, leading to brain dysfunction
Hyperaldosteronism, hypercortisolism or gonadal dysfunction are signs of liver dysfunction in which area of metabolism?
Impaired lipid metabolism (of cholesterol, phospholipids and steroid hormones)
Malabsorption of fats and fat-soluble vitamins is a sign of liver dysfunction in which liver role?
Impaired biliary clearance; biliary disease/dysfunction
Which cells of the liver remove bacteria
Kupffer cells
Increased total bilirubin is a sign of which diseases?
Anaemia such as
haemolytic anaemia
haemolytic disease of the newborn
sickle cell anaemia
pernicious anaemia
Increased conjugated bilirubin is a sign of which diseases?
bile duct obstruction
cirrhosis
hepatitis
Is ALT specific or non-specific for liver function?
ALT: specific to the liver and liver damage, as it is found in hepatic cytosol and is not associated with other tissue.
Is ALP specific or non-specific for liver function?
ALP: non-specific, because other tissues can release ALP too, such as:
bone
bile duct
placenta
Is AST specific or non-specific for liver function?
AST: non-specific, because it is found in many parts of the body, especially:
muscle
Is bilirubin specific or non-specific for liver function?
Bilirubin: specific (specifically indicates liver excretion); build up indicates liver dysfunction specifically of excretion, as it is usually cleared by the liver. Causes the jaundice and the pale stool colour (pale stool because low bilirubin in faeces and high bilirubin in bloodstream).
What are the two liver aminotransferases (AKA transaminases)?
ALT: Alanine aminotransferase
AST: Aspartate aminotransferase
Is GGT specific or non-specific for liver function?
GGT: specific, changes reflect obstruction of biliary tract and damage of biliary capillaries.
Bilirubin and albumin reflect which liver functions?
– Bilirubin – excretory function
– Albumin – synthetic function
Which biomarker is easily influenced by alcohol?
GGT
Diagnostic criteria for liver disease
ALT more than three times the upper limit of normal
OR
ALP of more than twice the upper limit of normal
OR
Total bilirubin more than twice the upper limit of normal if associated with any elevation of ALT or ALP
Paracetamol, aspirin and cocaine are examples of drugs associated with which type of drug-induced liver injury?
Predictable (intrinsic) drug-induced liver injury
Herbal medicines, antibiotics, NSAIDs are examples of drugs associated with which type of drug-induced liver injury?
Idiosyncratic (spontaneous) drug-induced liver injury
What is the onset and mechanism of idiosyncratic/spontaneous drug-induced liver injury
Delayed onset, may become apparent after 1-3 months
Usually due to formation of a toxic metabolite and may be driven by immune (allergenic) or non-immune (metabolic) mechanisms
What can be taken to relieve pruritis (itching) associated with liver injury / cholestatic liver disease?
cholestyramine
How to manage drug-induced liver injury
Withdraw drug
Supportive diet: high protein, high carbohydrate + energy
cholestyramine (4 g/day) for severe pruritus
If paracetamol: NAC antidote
What is Hy’s Law
Drug-induced liver injury leading to jaundice has a case fatality rate of 10-50% (without a transplant).
Which viral hepatitis subtypes usually resolve on their own without sequelae?
Hepatitis A and Hepatitis E
Is Hepatitis B curable?
No
Is Hepatitis C curable?
Yes
Which viral hepatitis sub-types have a vaccine?
Hep A and Hep B
What biomarker changes may suggest viral hepatitis?
increased AST and ALT
mildly elevated ALP
presence of acute phase antibodies e.g. anti-HAV/IgM
If INR is significantly elevated in viral hepatitis, what should be administered?
Vitamin K
Chronic hepatitis is defined as hepatitis lasting more than ______
6 months
How is chronic hepatitis diagnosis confirmed?
Via liver biopsy
What is available for proven Hep-A or Hep-B exposures?
Human immunoglobulin
Hepatitis A vaccines are recommended for which patient groups?
Vaccine recommended for:
– Travelers to high-risk areas
– IV drug use
– Men who have sex with men
– Recipients of blood products
– People with occupational exposure
– Patients with chronic liver disease
Hepatitis B vaccines are recommended for which patient groups?
Universal vaccination recommended of all children from birth + boosters.
Hepatitis B management
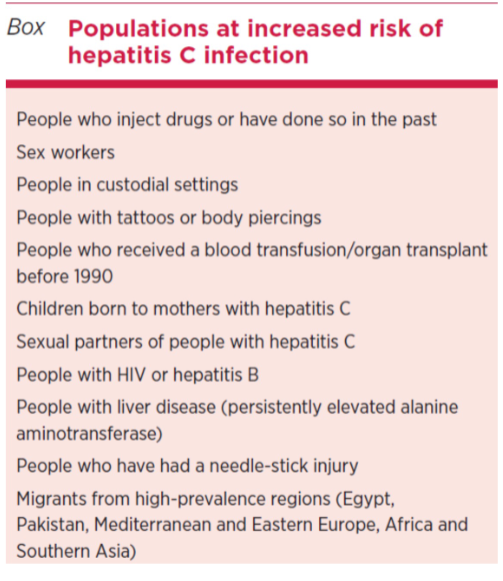
Which patient groups are at risk of Hep-C?
Peg-interferon is used for which type of viral hepatitis?
Hepatitis B
What kind of antivirals are used to treat Hepatitis C?
DAAs (Direct Acting Antivirals)
What is steatosis also known as?
Fatty liver disease
What is NAFLD and NASH?
NAFLD: Non-Alcoholic Fatty Liver Disease
NASH: Non-Alcoholic Steatohepatitis
Progression of Fatty Liver Disease
NAFLD (asymptomatic, fat)
NASH (inflammation + fibrosis/scarring)
Liver Cirrhosis (severe fibrosis, end-stage liver damage)
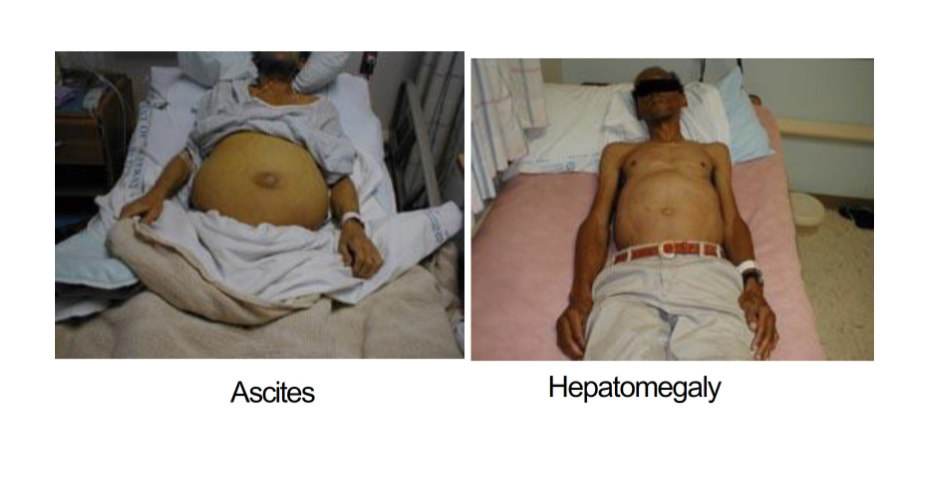
Ascites and hepatomegaly are signs of
End-stage liver damage
Causes of liver cirrhosis
Cryptogenic (unknown cause)
Alcoholic liver disease
Hepatitis B or C
Autoimmune hepatitis
Hemochromatosis
Wilson disease
Alpha-1 antitrypsin deficiency
Drug-induced liver disease
Type IV glycogen storage disease
Examples of two drugs that can cause liver cirrhosis
Methotrexate
Amiodarone
Management of hepatic encephalopathy
Protein (>30g/day)
Prebiotics
Probiotics
Antibiotics (e.g. rifamixin) to eliminate gut bacteria that produce ammonia
Minimum amount of protein a day for people with liver disorders and complications
> 30 g per day
Most validated non-invasive test for assessing liver cirrhosis?
Vibration-controlled transient elastography (VCTE) with FibroScan
Liver cirrhosis management
– Prevention: alcohol avoidance
– Nutrition: protein supplement intake (branched chain amino acids), low salt diet
– Supplemental vitamins
– Liver transplant
Management of ascites (fluid build up in the abdomen in end-stage liver damage)
– adequate protein/energy intake
– Na restriction
– Fluid restriction
– Avoid Na retention drugs e.g. NSAIDs
– Spironolactone
– Frusemide
– Paracentesis: remove fluid to relieve abdominal pain and respiratory distress.
How to prevent bleeding oesophageal varices?
Propanolol to reduce heart rate, lowering portal hypertension
Contraindications to liver transplant
Advanced hepatocellular carcinoma
Uncontrolled extrahepatic infection
Active alcohol/substance misuse disorder
Coronary/cerebrovascular disease
Inadequate social support
Ten year survival rate for adults and children following liver transplant
Ten-year patient survival
72.3% for adults
85.2% for children
How does acute infection, inflammation and cirrhosis alter CYP enzyme activity?
Cirrhosis reduces enzyme capacity
Cytokines downregulate enzyme activity
The liver has the largest store of which vitamin? How many months does this storage last?
Vitamin A (50-60% of the body’s total supply)
10 months
Which vitamins does the liver store?
Vitamin A
Vitamin D
Vitamin B12
Risk factors of Drug-Induced Kidney Injury
– History of CKD
– Advanced age
– Critical illness
Medicines most implicated in Drug-Induced Kidney Injury
– aminoglycosides,
– NSAIDs, ACEIs, ARBs,
– calcineurin inhibitor immunosuppressants (tacrolimus, cyclosporine)
– intravenous contrast dye,
– amphotericin,
– piperacillin/tazobactam plus vancomycin
– diuretics
Which drugs can cause pseudo-nephrotoxicity (no actual kidney damage despite raised markers)?
mesalazine
trimethoprim
A patient with declining renal function, high calcium levels and acute systemic symptoms may be presenting with…
Calcium alkali syndrome
What do you do to treat calcium alkali syndrome?
IV pamidronate
stop calcium and vitamin D supplements
Which statin presents a greater risk to the kidneys than all others?
Rosuvastatin
What is pseudohaematuria and what drug can cause it?
The false appearance of “blood” in urine.
Mesalazine reacting with toilet bleach can cause this effect.
When should dialysis be initiated?
AEIOU indications:
Acidosis
Electrolyte abnormality
Intoxicants
Overload (volume overload refractory to diuretics)
Uremia
GFR indications:
Stage G4: GFR less than 30
Stage G5 (kidney failure): GFR less than 15
The two processes that drive dialysis
Diffusion
Convection
What is the preferred vascular access for hemodialysis and why?
A surgically-created AV fistula because it enables high pressure, fast blood flow
Haemodialysis duration and frequency
4-6 hours three times a week
Longer dialysis sessions means…
Longer dialysis means
less diet and fluid restrictions
improved health and quality of life
Two types of peritoneal dialysis and their differences
continuous ambulatory peritoneal dialysis (CAPD): manual, moves with you
automated peritoneal dialysis (APD): overnight via a cycler
CKD is defined as…
Kidney damage OR GFR below 60 ml/min/1.73sqm for 3 months or more
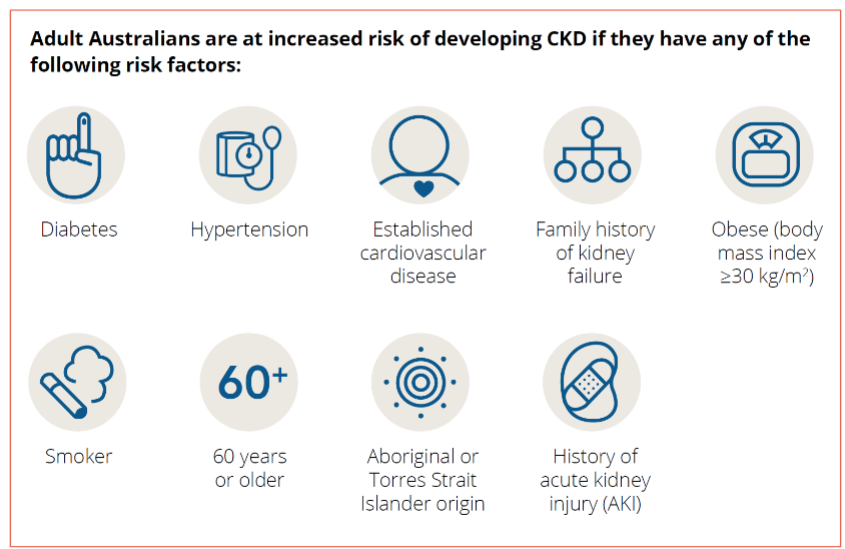
CKD risk factors
Main symptoms of uremia
Cramps
Restless legs
Hiccups
Coma
Top 2 causes of CKD
Diabetes Mellitus (Type 2)
Hypertension
CKD non-pharmacological management
Smoking cessation
Alcohol restriction
Diet, including:
Sodium restriction
Phosphate restriction
Carbonated beverage restriction
If hyperkalaemic, potassium restriction
Exercise
Weight management
Preferred agents for managing hypertension in CKD
ACE inhibitors or ARBs
Dihydropyridine Calcium Channel Blockers are also beneficial
ACE inhibitors and ARBs are nephroprotective long term even though they can be nephrotoxic. An ACE inhibitor or ARB can be continued as long as…
As long as:
eGFR does not deteriorate by more than 25% within 2 months of initiation
AND
Potassium stays below 6 mmol/L
How to manage proteinuria or albuminuria?
ACEI/ARBs
reduce salt intake
SGLT2 inhibitor
If a patient has CKD, they may need lipid management. What is the decision tree for this?
Over the age of 50 years
eGFR greater than 60 mL/min: start statin only
eGFR below 60 mL/min: start statin and ezetimibe
Under the age of 50 years
Coronary disease, previous stroke, diabetes or 10% risk of heart attack in 10 years time: start statin
Glucose control in CKD patients can be managed with which kinds of drugs?
• Oral hypoglycaemic agents
• Gliptins
• Incretin mimetic
• Insulin
• SGLT2 inhibitors
What different consequences of CKD need to be managed in a CKD patient?
impaired glucose control
hypertension
dyslipidemia
sodium imbalance
impaired vitamin D and phosphorus metabolism
anaemia
What therapies are used to maintain sodium balance in patients with CKD?
Sodium restriction
Diuretics (NOT potassium sparing)
Thiazide and related diuretics can be used in which stages of CKD?
Stages 1-3
(ineffective once GFR is below 30)
Loop diuretics can be used in which stages of CKD?
All stages
K+ -sparing diuretics can be used in which stages of CKD?
K+ -sparing diuretics are not usually used in CKD because they present an increased risk of hyperkalemia.
Main symptom of metabolic acidosis
Shortness of breath on exertion not explained by anything else
How is metabolic acidosis from CKD managed?
Not treated unless bicarb less than 15 mmol/l or pH less than 7.30
Can be treated with sodium bicarbonate (risk of high sodium)
Threshold for hyperkalemia
Potassium greater than 7 mmol/L
Acute hyperkalemia management
Calcium gluconate IV
Insulin and glucose IV
Sodium (or calcium) resonium orally or enema
Chronic hyperkalemia management
stop drugs causing hyperkalaemia
reduce dietary potassium
correct acidosis:
Thiazides or loop diuretics to eliminate potassium
cation exchange resins (polystyrene sulfonate, Resonium )
Persistent pruritis in CKD patients can be managed with
UVB light phototherapy
Presentation of both restless legs AND pruritis symptoms in CKD can be managed with
gabapentin
Managing phosphorus and vitamin D metabolism in CKD: agents (classes) used
Vitamin D supplements
Phosphate binding agents
Calcimimetics (Calcinet)
Which vitamin D supplements can be used in CKD?
Calcitriol
Paricalcitol
Cholecalciferol (if renal function is intact, or in combination with calcitriol in advanced CKD)
Which vitamin D supplement is only useful in renal function is intact?
Cholecalciferol
How is anaemia managed in CKD?
ESA: erythropoiesis-stimulating agents
potentially iron, folate or B12 supplements alongside
iron infusions
Hemoglobin (Hb) should not exceed ______ g/L (increased risk of CV events).
130 g/L