MOA of antiemetics
1/16
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
17 Terms
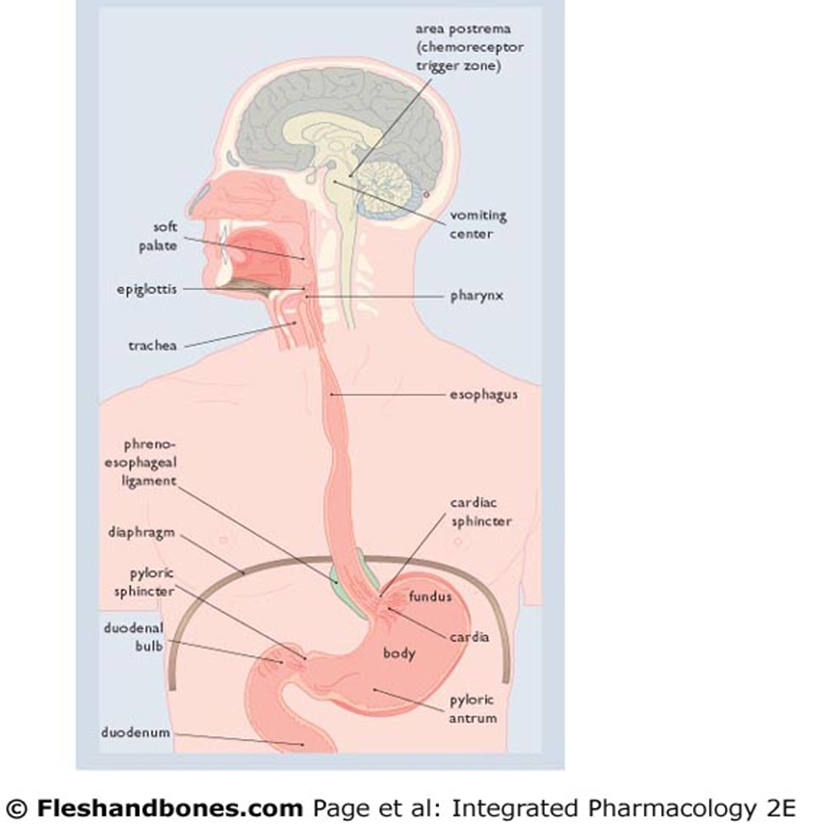
The emetics reflex
•An autonomic nervous system disturbance causes pallor and sweating
•Relaxation of the lower part of the oesophagus and abdominal muscles
•Increased tension on the gastric and oesophageal muscles
•Stimulation of afferent nerve endings – symptoms of nausea
•Sequential contraction of the upper small intestine pyloric sphincter and pyloric (lower) portion of the stomach – expels their contents into the fundus and body (upper region) of the stomach which are relaxed
•Deep and sharp inspiration occurs
•Reflex closing of the glottis & raising of the soft palate
•Rhythmic contractions of the abdominal muscles (retching) compresses stomach
•Evacuation of stomach contents though the relaxed oesophagus due to increase in intragastric pressure
*FOR INFO ONLY
Some are more susceptible to nausea and vomiting than others
•The emetic risk varies among individuals as it is multifactorial
•Research suggests that females have a lower emetic threshold than males on average
•Someone with a low emetic threshold will commonly have it across a range of emetic stimuli.
•Someone who has travel sickness will often have sickness as a symptom if they have migraines and is at therefore at greater risk of CINV. A patients response also tends to be consistent so if they have a lower emetic threshold they should be given prophylactic antiemetics for chemotherapy N/V regardless of the emetic potential of the therapy itself.
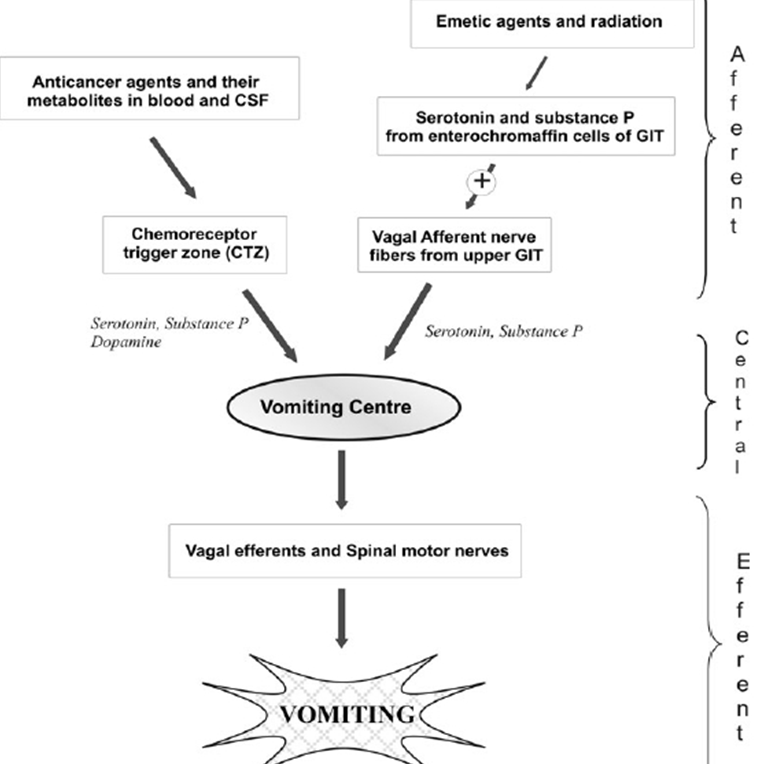
The neurophysiology of vomiting
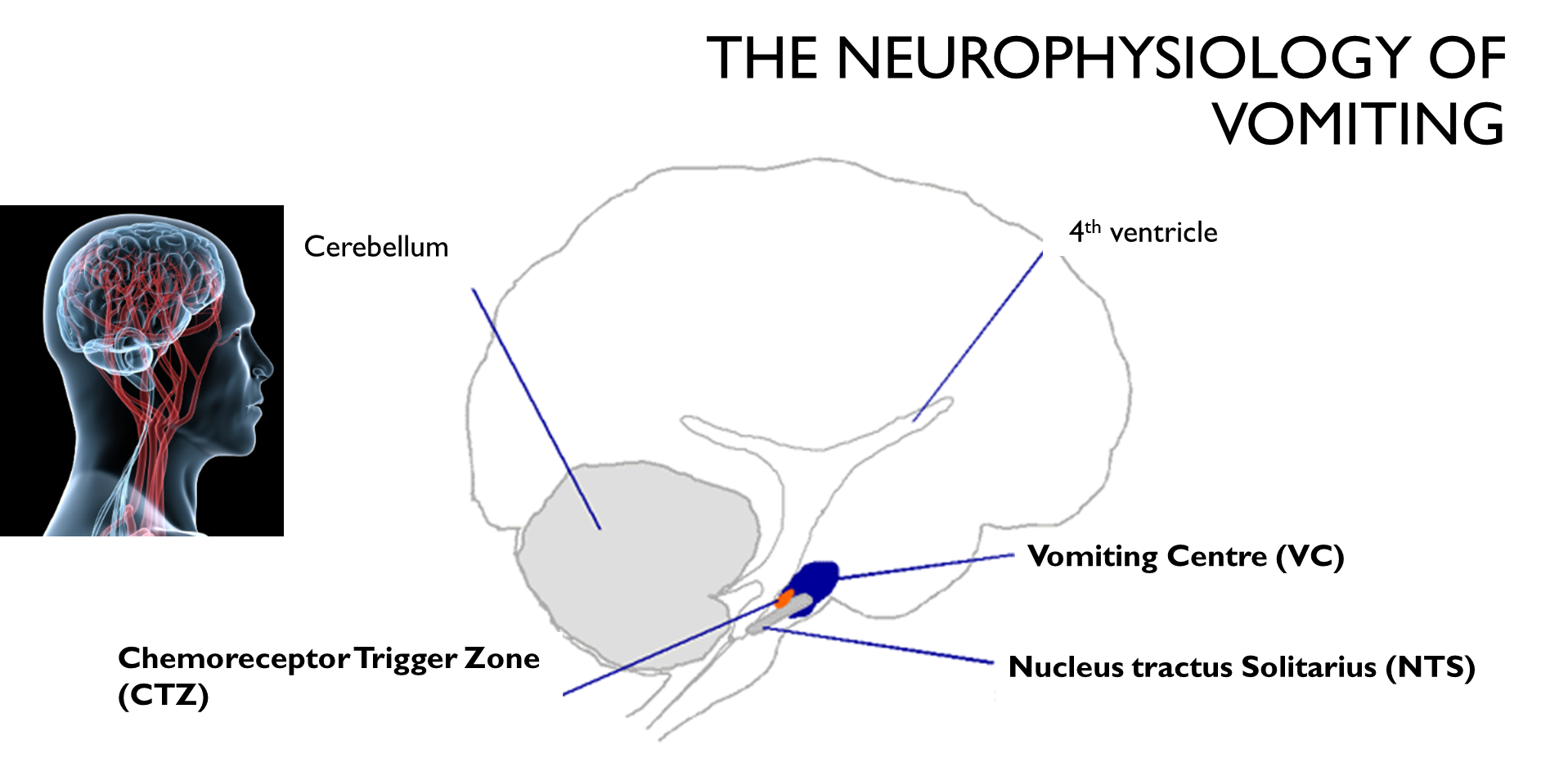
There are a number of regions in the brain that are involved in receiving signals associated with emetic vomiting. The CTZ, NTS and vomiting centre. The CTZ receives signals from the periphery via the circulation. The NTS is a site for convergence of afferent inputs into the vomiting centre, which is the integration centre for the emetic response.
The integration of Signals is complex
Integration of signals is complex which explains why there is a difference in tolerance to stimuli. There are also genetic variations in the proteins involved in this pathway.
CTZ does not have an effective BBB
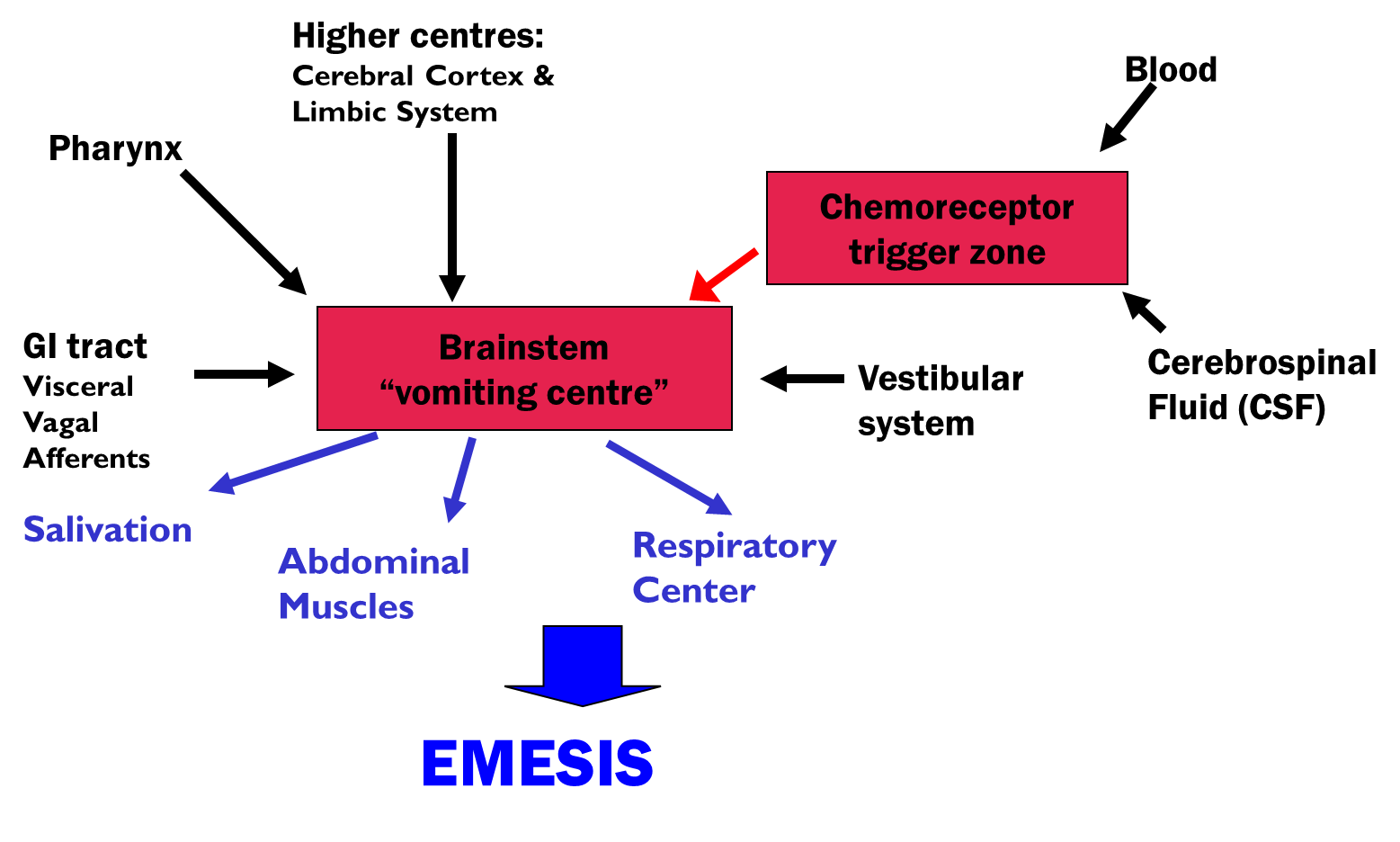
The brain stem vomiting centre receives inputs from the periphery from the GI tract via the afferent neurons of the vagus nerve. The vomiting centre also receives input from the pharynx and the cerebral cortex and limbic system.
It also has inputs from the vestibular system involved in maintaining balance, which is important in terms of the symptoms of nausea and vomiting associated with motion.
The vomiting centre integrates all these signals and sends impulses to various parts of the body,
including the pharynx, the diaphragm, abdominal muscles, resulting in the process of emesis.
Chemoreceptor Trigger Zone (CTZ)
•Found close to the 4th ventricle
•Lacks an effective blood brain barrier → permeable to polar molecules in both the blood and the cerebral spinal fluid.
•Chemosensitive receptors detect noxious stimuli in cerebrospinal fluid & circulation and has neuronal pathways to the nucelus tractus. Both of these will receive vagal afferent fibres from the GI tract and relay information to the vomiting centre.
•Drugs
•Chemicals
•Toxins
•Connected to the nucleus tractus solitarius (NTS)
•Both receive vagal afferent fibres (from the GIT) and relay information to the vomiting centre
CTZ receptors – 5HT3, D2 dopamine, opioid, low levels M1 mACHR
NTS receptors –D2 dopamine, opioid, mACHR, H1 histamine
Vomiting Centre (VC)
•Responsible for coordination of emetic response
•Collection of interconnecting neuronal networks
•Receives inputs from:
Chemoreceptor trigger zone
Cardiovascular system
Vagus nerve which monitors intestinal contents and gastric tone
Cerebral cortex and limbic system
- olfactory tubercle (olfactory) → explains why cells can be emetic stimuli
- amygdala (emotional / anticipatory)
- hypothalamus (hormonal / stress)
-ventral thalamic nucleus (pain)
VC receptors
D2 dopamine, 5-HT3 serotonin, opioid, M1 mACHR, NK1 Substance P, H1 histamine
Causes of nausea and vomiting
•Infections
•gastroenteritis, hepatitis, septicaemia
•GIT disorders
•peptic ulcer disease, obstructions, cancer, appendicitis
•CNS
•tumour, migraine, anxiety, anticipatory
•Therapy induced
•Analgesics - morphine and related opioids activate CTZ directly
•5HT receptor agonists and SSRIs (central and GI effects)
•Dopamine receptor agonists
•Drugs which cause GI damage
•Abdominal radiation
chemotherapy drugs can directly irritate the lining of the GI tract. This irritation can be signalled to the VC via the vagus nerve and serotonin acting at the 5HT3 receptor.
Chemotherapy can lead to the release of serotonin and substance p from the cells of the GI tract.
These chemicals can stimulate receptors in the brain associated with nausea and vomiting.
These can also be released due to damage to the guts caused by chemotherapy.
The inflammatory response to this damage can also release prostaglandins and takokinines such as substance P.
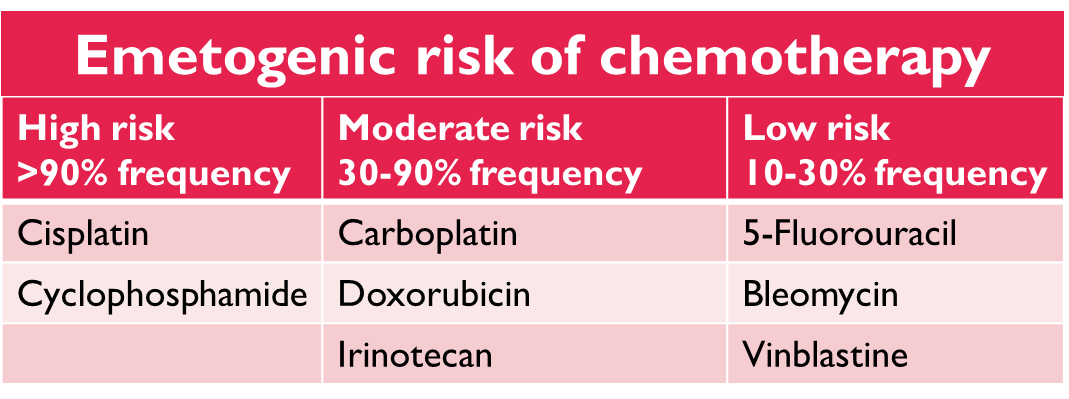
Chemotherapy induced nausea and vomiting (CINV
•Cisplatin is highly emetic. Without prophylactic therapy it will induce vomiting in almost all patients. Its thought to act via 5H3 in the periphery.
•Peripheral effects - Free radicals produced thought to cause calcium dependant exocytosis of 5HT from enterochromaffin cells which stimulates vagal afferents, leading to activation of vomiting centre.
•Central effects - Substance P co-released with 5HT can cross the BBB
Chemotherapy induced nausea and vomiting (CINV)
•CINV is biphasic
•Stage 1 – Acute stage
•Universally experienced
•1-3hr latency followed by nausea and vomiting that peaks at 6-8 hr (frequency) decreases by 12 hr with less over next 4 hrs
•Stage 2 – Delayed stage
•Experienced by a subgroup of patients
•Occurs after 16 hrs, peaks at 24-72 hrs and can occur for 1-5 days
The acute phase is neuronal in origin and is relayed by the by the vagus nerve. The delayed phase id due to activation of the CTZ via chemotherapy agents and transmitters released into the circulation. We know that 5H3 receptors are involved but blockade of this does not completely prevent this. Therefore we know that other mediators are involved as well e.g. substance P and dopamine. Receptors in the NTS and the vomiting centre are activated by substance P that is released from the vagal afference innovating these area. Substance P can also cross the BBB and is released in the periphery and may also act centrally in the delayed stage.
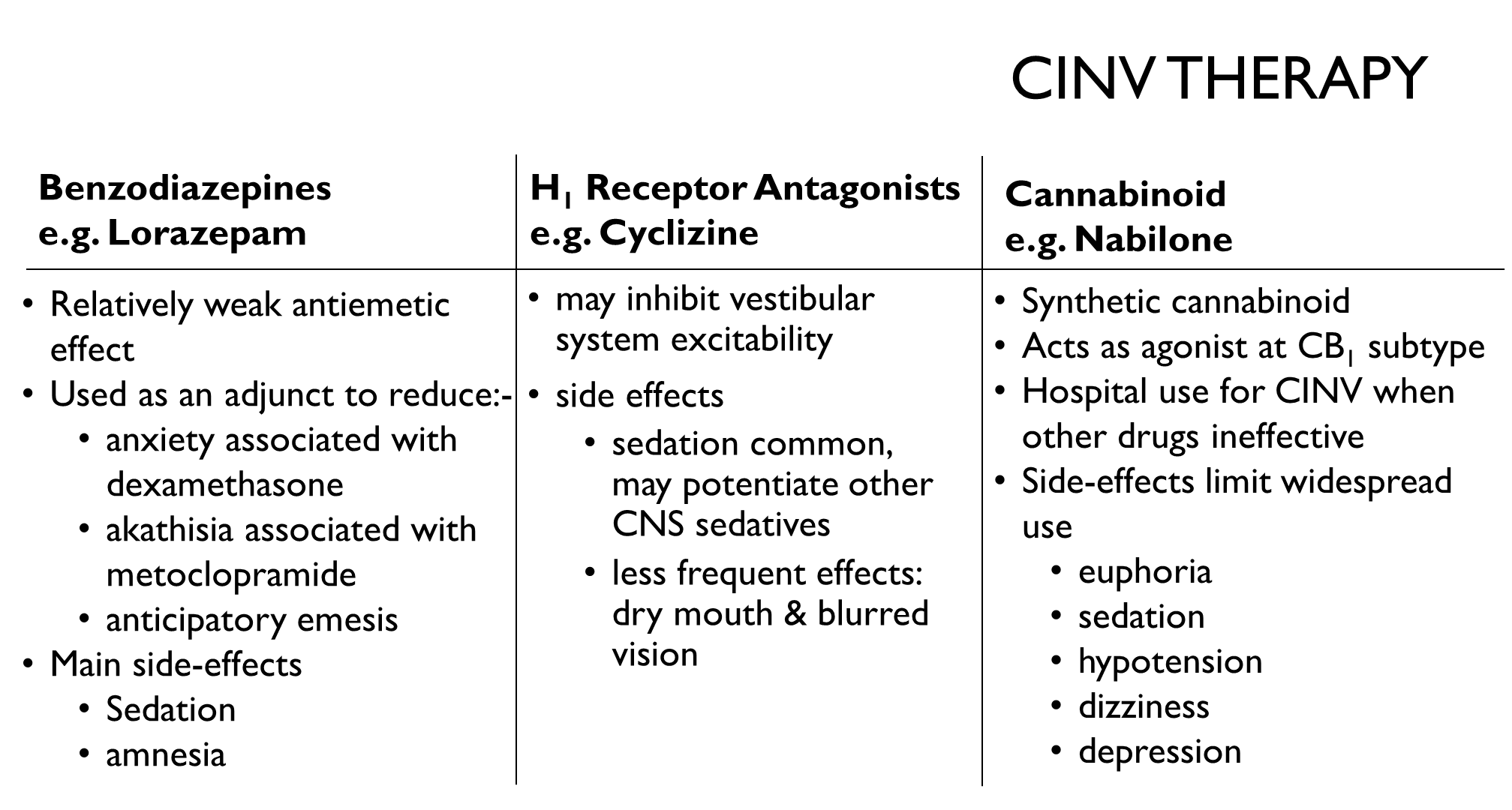
CINV Therapy
Neurokinin1 Receptor Antagonists
e.g. Aprepitant
•Blocks the action of Substance P at NK1 receptors in CNS, vagal afferent neurons in the GIT & its GIT paracrine actions
•Recommended for high and moderately emetogenic chemotherapy e.g. cisplatin
•Used for the delayed stage of CINV in combination with 5HT3 antagonist and dexamethasone
•Side effects – inhibition of CYP3A4 which has implications for other medications that are metabolised by this enzyme
CINV Therapy
5HT3-Receptor Antagonists
e.g. Ondansetron, Granisetron, Palonostron
•Used for the prevention and treatment of acute CINV. They're effective because five actually three receptors are present and several critical sites involved in emesis the vagal nerve endings, the vagal afferent nerve endings in the gut, the NTS which receive signals from vagal afferents. The highest number of vagal afferent are found in the CTZ and NTS,
•Less effective for management of delayed CINV unless combined with dexamethasone and aprepitant.
•Peripheral actions –
abolishes vagal afferent response to 5-HT
Acts at the CTZ by crossing the blood brain barrier.
•Central actions - acts at the NTS and VC
•Side-effects - mild headache, constipation, dizziness.
Its not sedating and has few interactions with the drugs and has no autonomic nervous effects.
CINV Therapy
Dopamine D2 Receptor Antagonists
Metaclopramide
•central & peripheral D2-antagonist at low doses, weak 5-HT3 blocker and 5HT4 agonist at higher doses
•crosses the BBB - extrapyramidal side-effects
•EMA recommendations for use regarding safety - need to learn this!
Domperidone
•Peripheral action only
•Acts at the CTZ
•Does not cross BBB
CINV Therapy
Phenothiazines
e.g. Prochlorperazine
•mixed pharmacology - act as antagonists at D2 receptors in the CTZ, also acts at M1- and H1-, Adenosine and 5HT receptors. It is added to CINV therapy that is not responding to other treatment due to its action at a wide range of receptors involved in the emetic response.
Extrapyramidal side effects → restlessness, dystonia, sustained contractions of muscles and tardive dyskinesia.
Corticosteroid
e.g. Dexamethasone
•Mechanism of action unknown -may relate to a reduction in prostaglandin levels. CYP3A4 is involved in its metabolism.
•Side-effects
•insomnia
•increased mood changes
CINV Therapy
Why The Need FOR CINV Therapy?
•CINV affects between 60-80% of patients with cancer
•Treat prophylactically - The risk of CINV increases with each cycle of chemotherapy where it was not managed well
•Improves Quality of Life
•Increased treatment success: CINV can be associated with premature discontinuation of treatment
•Reduces risk of complications e.g. dehydration and electrolyte imbalances
CINV Therapy
•Treatment is evidence based for CINV
On the risk of emesis
On the stage of emesis
•The effectiveness of prophylactic treatment reduces with each cycle of chemotherapy.
•If therapy fails an additional anti-emetic should be given of a different therapeutic class and any medication was previously being given on a 'when required' basis this should be switched to a regular dosing schedule.
CINV Therapy
•Prevention of acute symptoms
Low risk - dexamethasone or lorazepam
High risk - 5HT3-receptor antagonist in combination with dexamethasone and aprepitant
•Prevention of delayed symptoms
Moderately emetogenic chemotherapy - 5HT3-receptor antagonist in combination with dexamethasone
Highly emetogenic chemotherapy - dexamethasone and NK1 receptor antagonist