1-41
1/54
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
55 Terms
Toxicology
branch of pharmacology which deals with the undesirable effects of chemicals on living systems, from individual cells to complex ecosystems
Corpus delecti
Body of evidence
any agent which may cause serious body injury, disease or death when applied, introduced into, or developed within the body
PARACELSUS (PATBvH)
“What is there that is not a poison”
MATHIEU ORFILA
Lex cornelia
First book���� regarding poisoning
Intoxication
toxicity associated with any chemical substance
POISONING
a clinical toxicity secondary to accidental exposure
OVERDOSE
an intentional exposure with the intent of causing self-injury or death
Hazard
likelihood that injury will occur in a given situation or setting
Risk
expected frequency of the occurrence of an undesirable effect arising from exposure to a chemical or physical agent
MUTAGENESIS
heritable changes in genetic material that are limited to the effects on the nucleic acid
Haptens
chemicals with molecular weights of less than 1000 and generally react with endogenous carrier molecules to become antigens before they exhibit immunogenicity
Clastogenesis
chromosomal breakage resulting in rearrangement of pieces of chromosomes
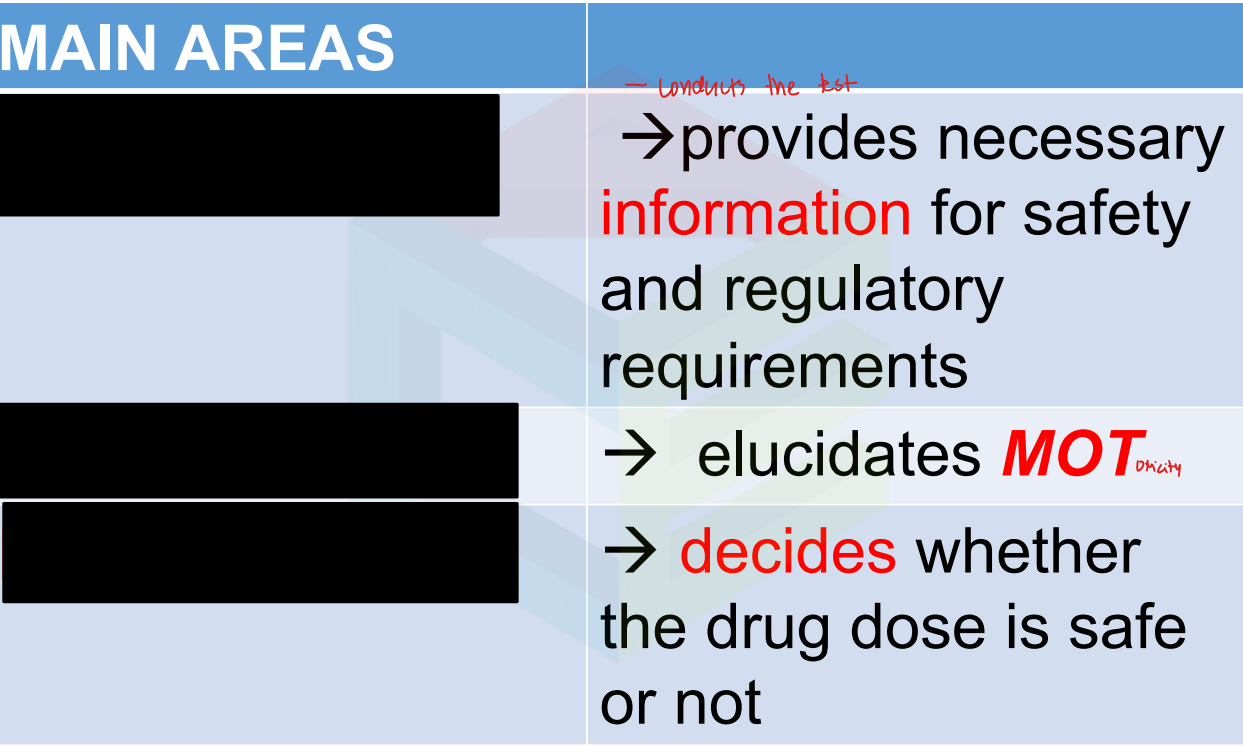
Decriptive, mechanistic, regulatory
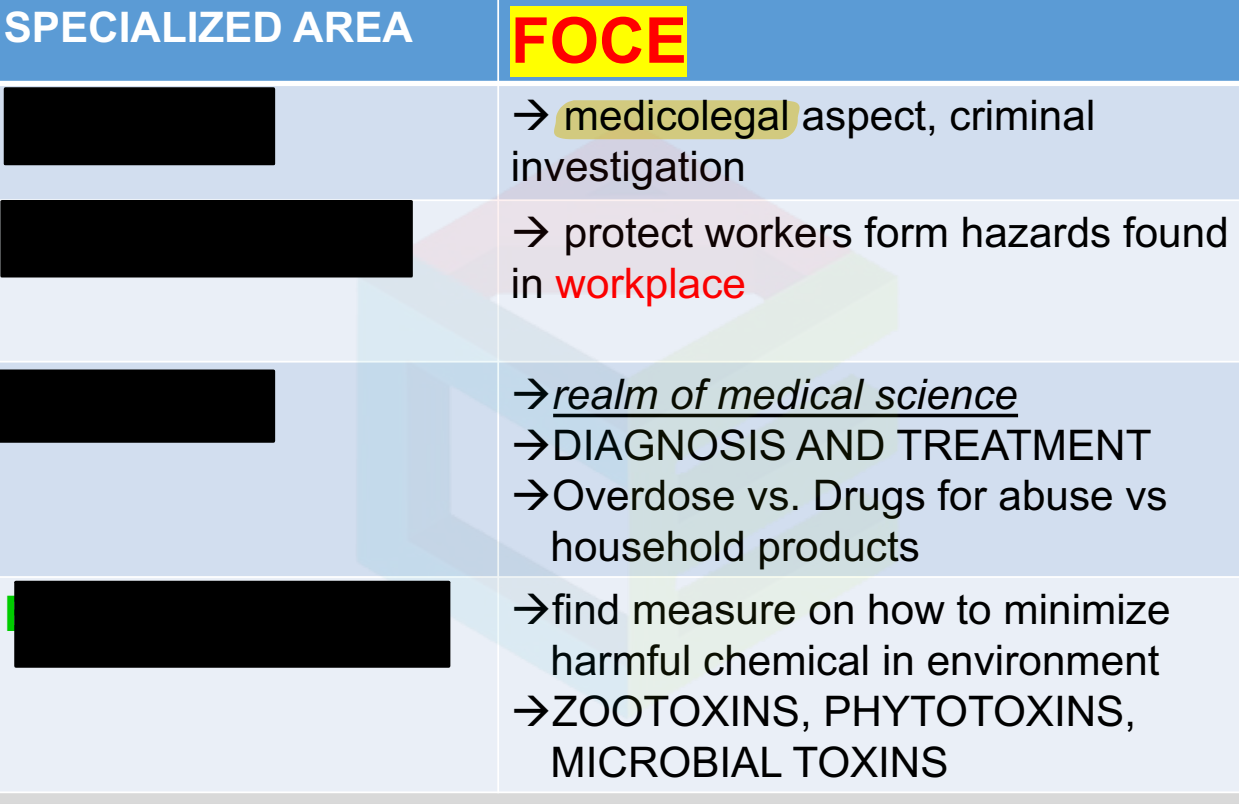
Forensic, environmental, clinical, occupational
Descriptive
Mechanistic
Regulatory
Forensic
Occupational
Clinical
Environmentally
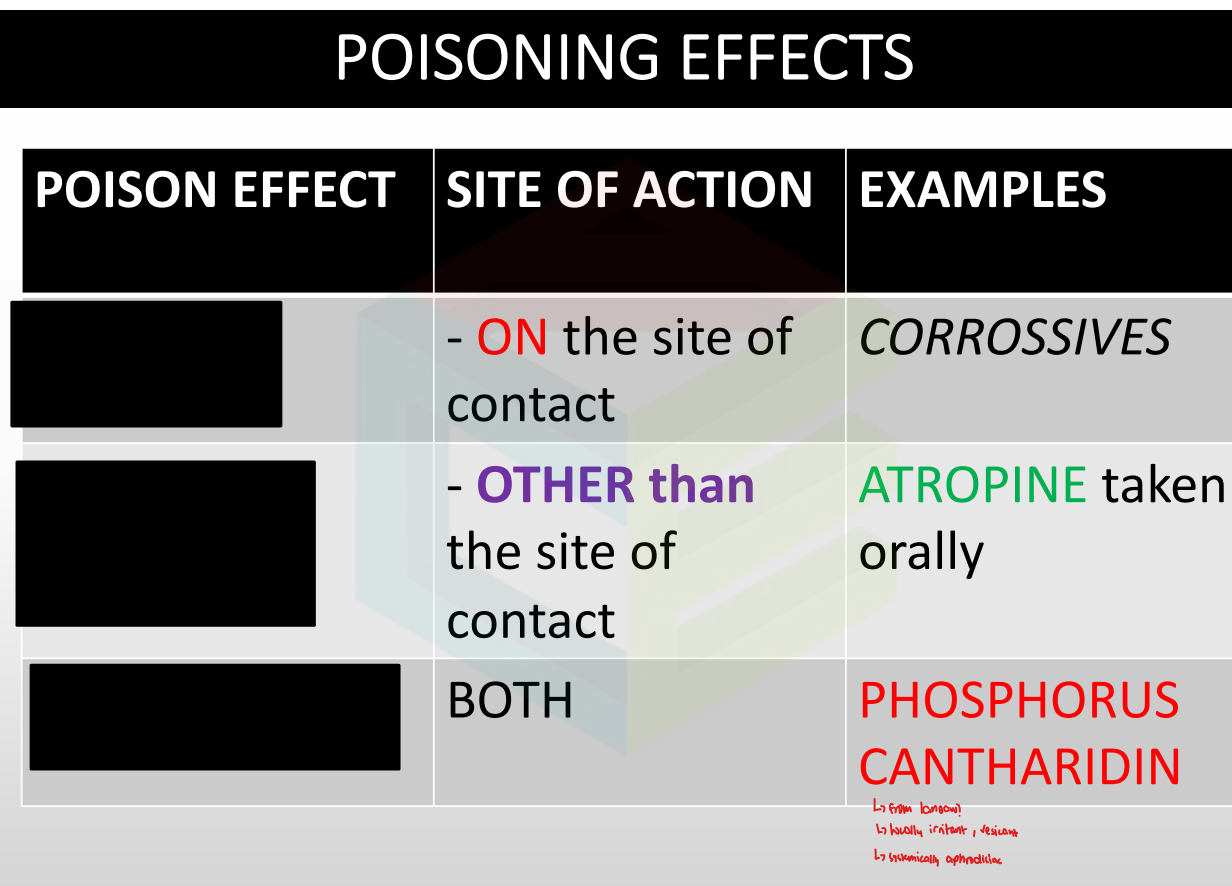
Local/remote
Systemic
Combination
Dispositional antagonism
A type of antagonism where the effect of the drug is cancelled through ADME
EX: Ipecac, AC
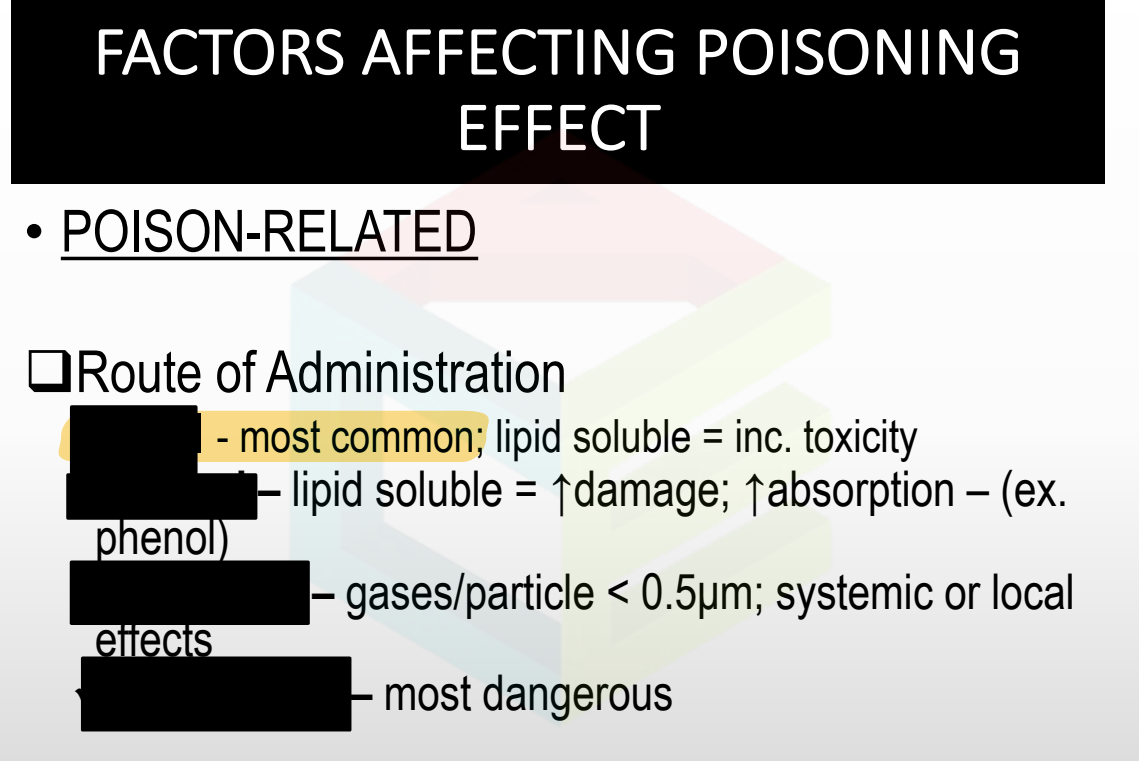
Route of ad, conc.
Age, habit, idiosyncracy, tolerance
Oral
Dermal
Inhalation
Intravenous
Antimalarial
Sulfa drugs
ASA
Acetanilide
Nalidix acid
INH
Nitrofurantoin
G6PD Deficiency causes hemolytic anemia. What are the triggers?
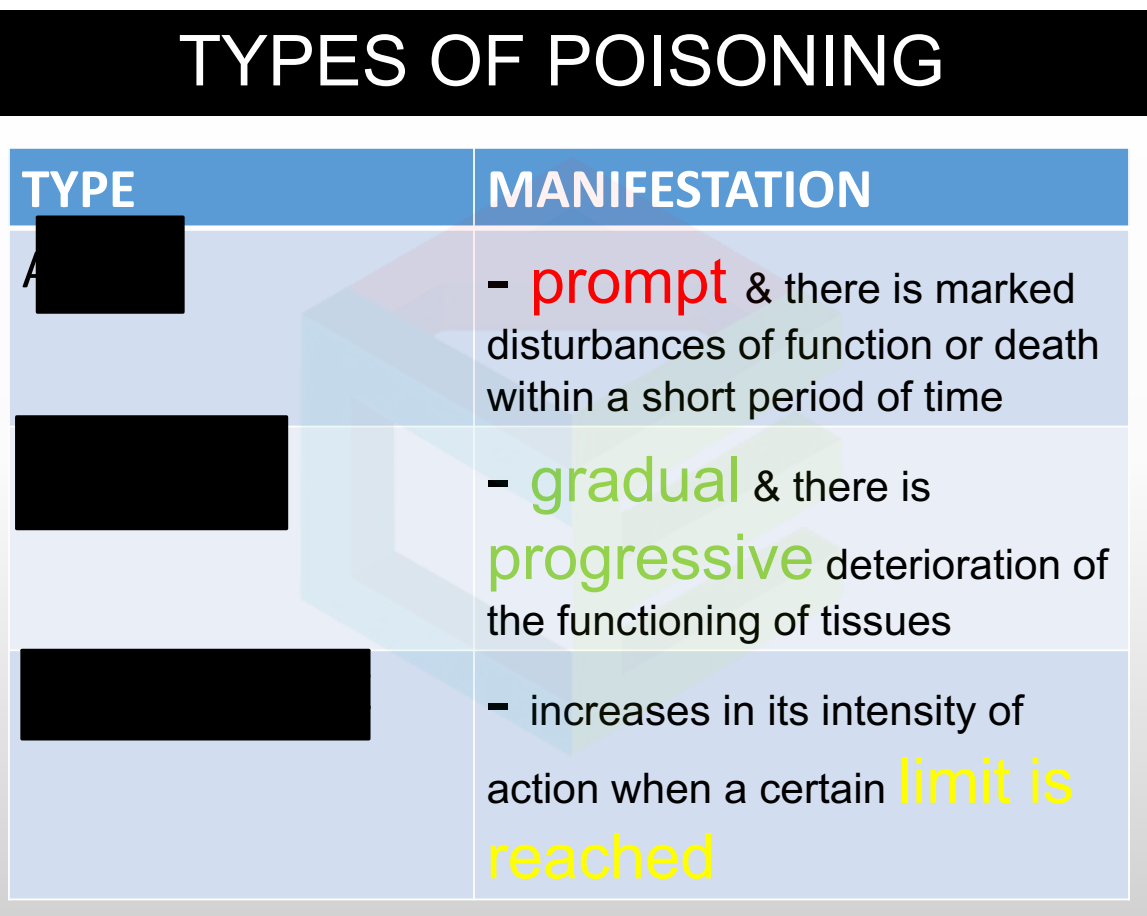
Acute
Chronic
Cumulative
<24 hours
Dietary
< Or = 1 month
1-3 months
>3 months
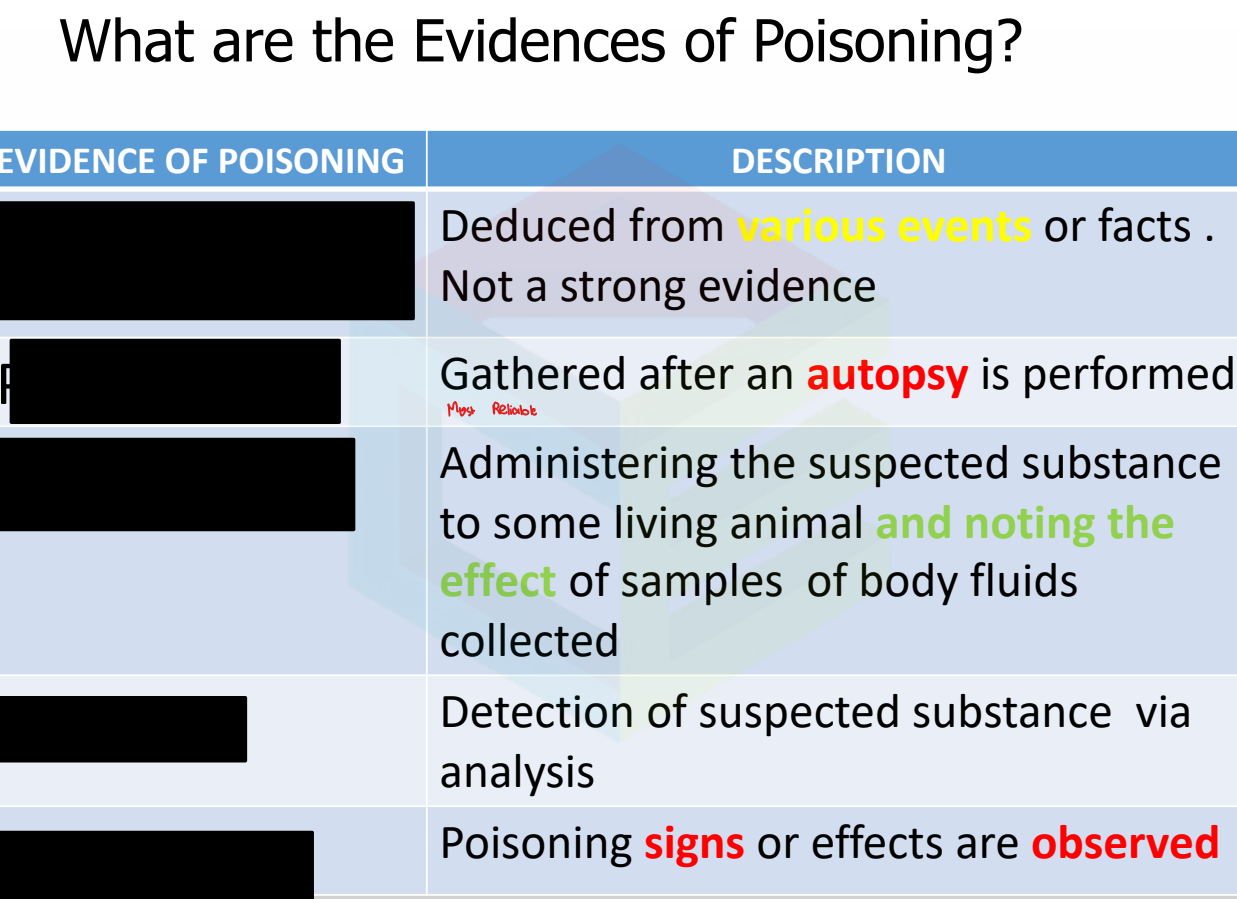
Circumstantial (Moral evidence)
Post mortem
Experimental
Chemical
Symptomatic
Initial assessment
Evaluate and support
A
B
C
Diagnosis/Decontamination
General Management of Poisoned Patient
Physiologic
Chemical
Mechanical
General types of antidote
Gastric lavage
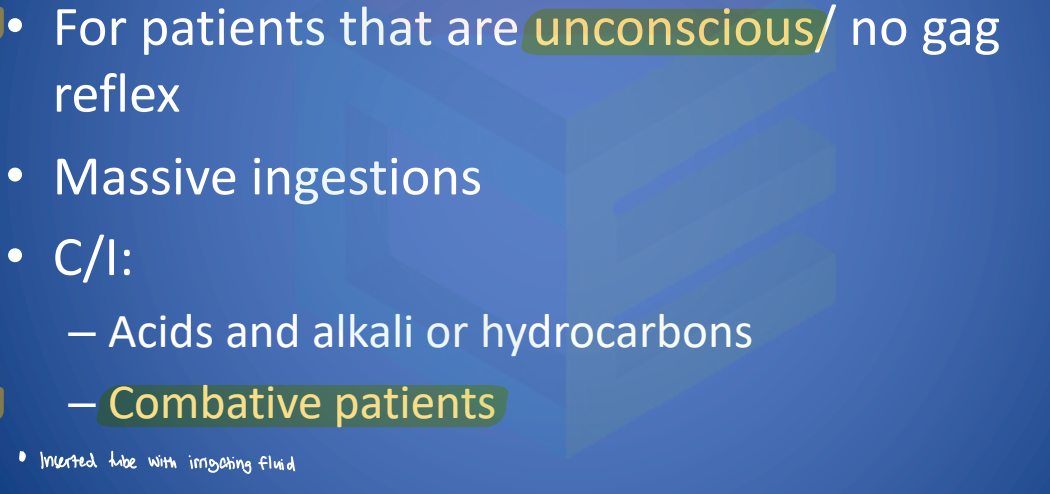
<60 mins
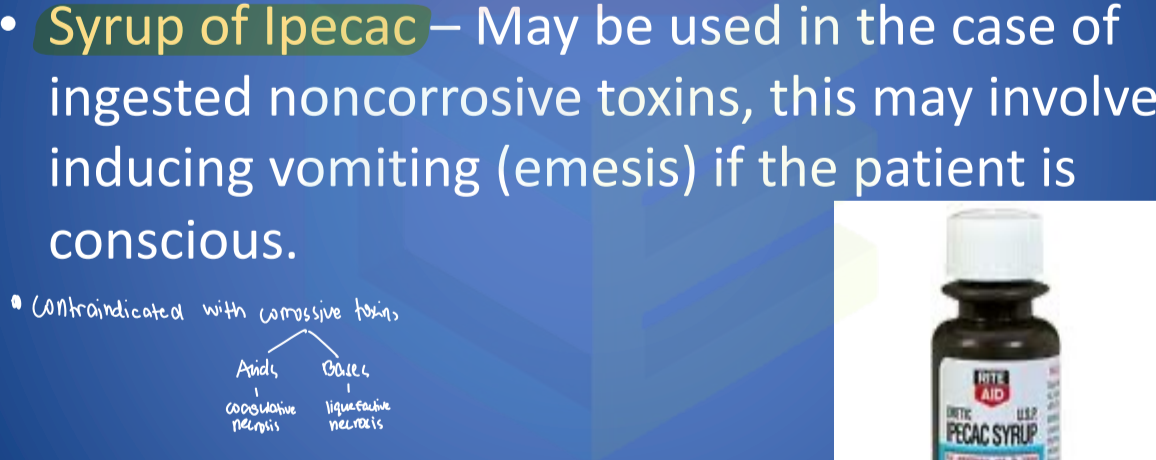
Emesis as a mechanical antiodite is only effective —
Two tbsp of soap in 100 mL water
Syrup of ipecac alternative
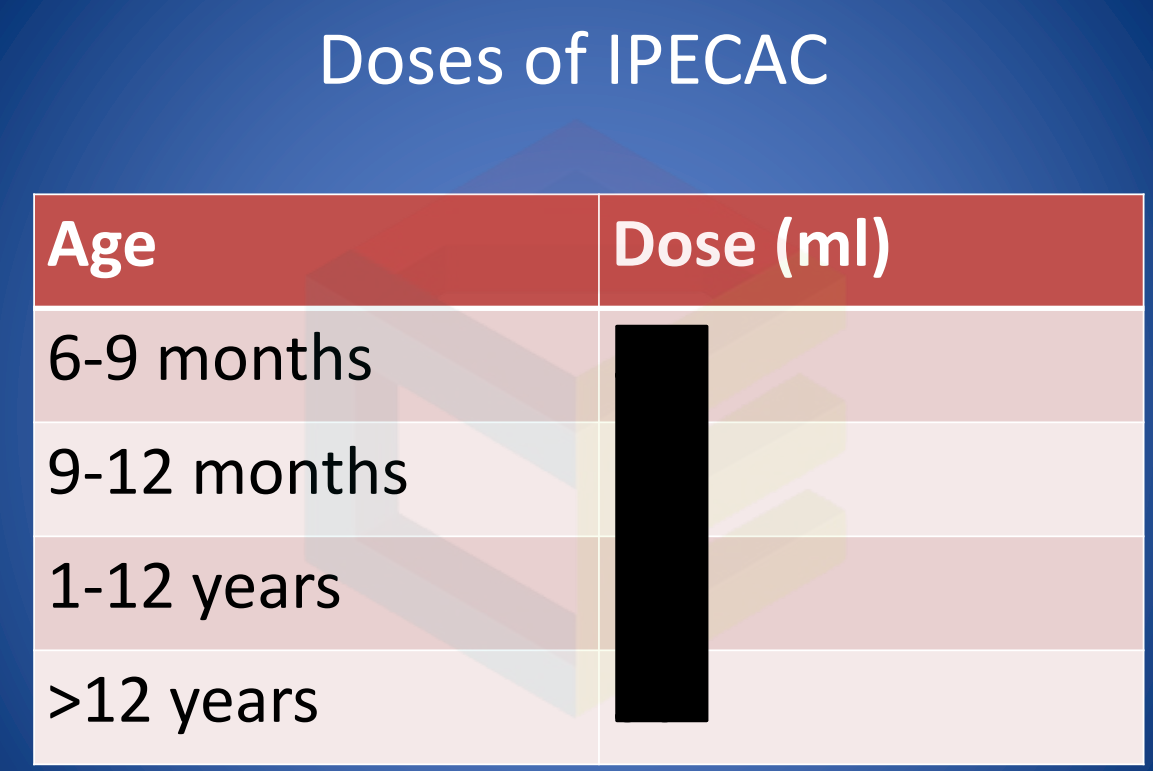
5 mL
10 mL
15 ml
30 mL
Cathartics
Mechanical antidote to induce evacuation of bowel
Precipitation
Alter the poison by forming an insoluble substance
2:1:1 AC/Tannic acid/MgO
What are the components of the universal antidote
CELLIMEMOPSS
Activated charcoal binds to toxins except:
NaHCO3
NH4Cl, Vit C,HCl
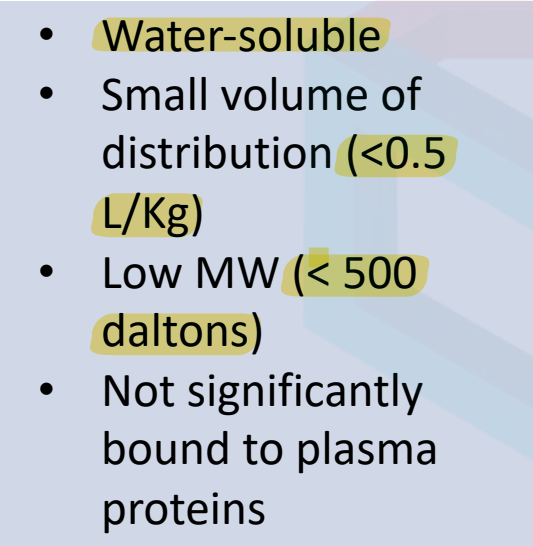
Hemodialysis
Extracorporeal method
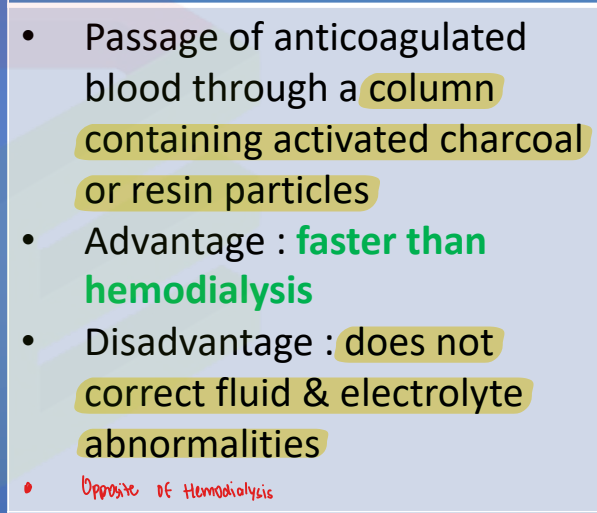
Hemoperfusion
Extracorporeal method
Gastric lavage
Emesis
Cathartics
Precipitation
Activated charcoal
Hemodialysis
Hemoperfusion
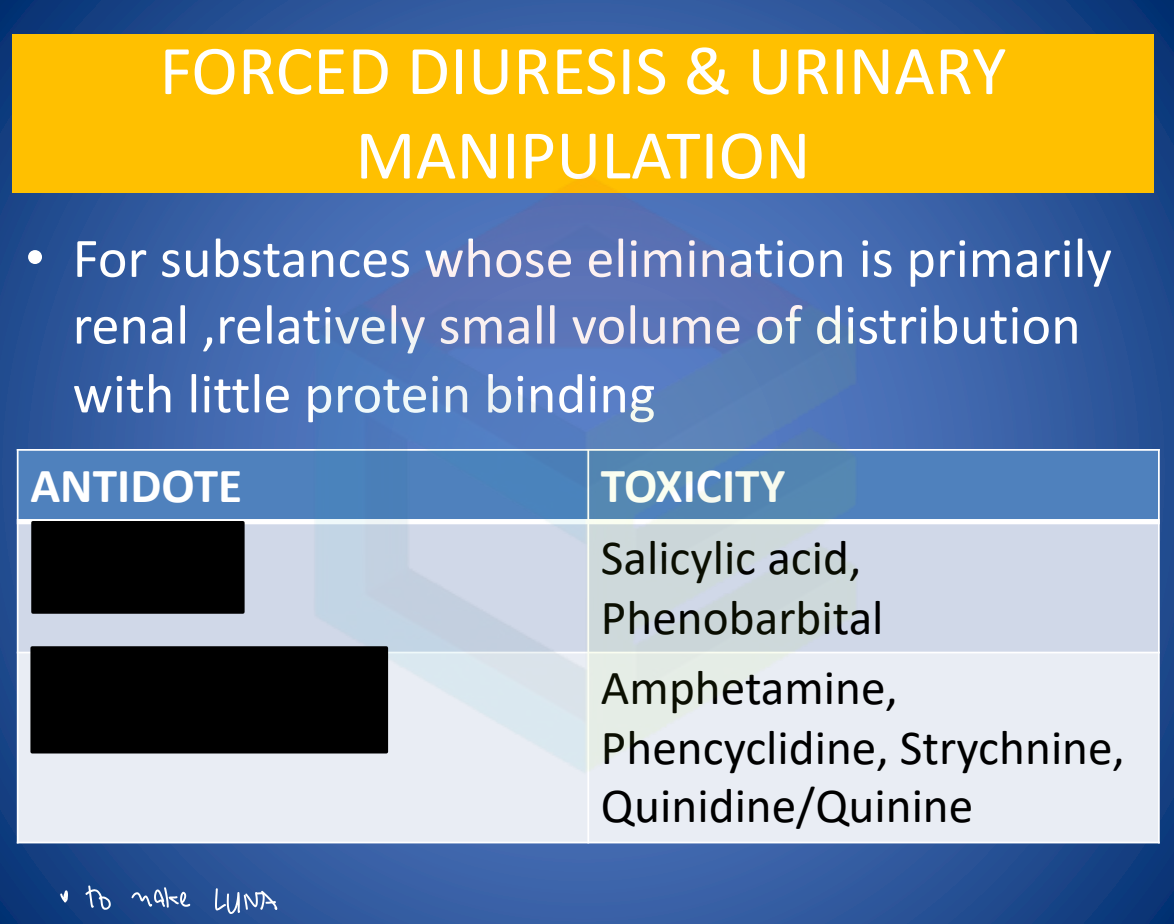
Forced diuresis/pH manipulation
What are the mechanical antidotes
Succimer (Dimercaptosuccinic acid/DMSA)
Unithiol
what are the water soluble analogs of dimercaprol
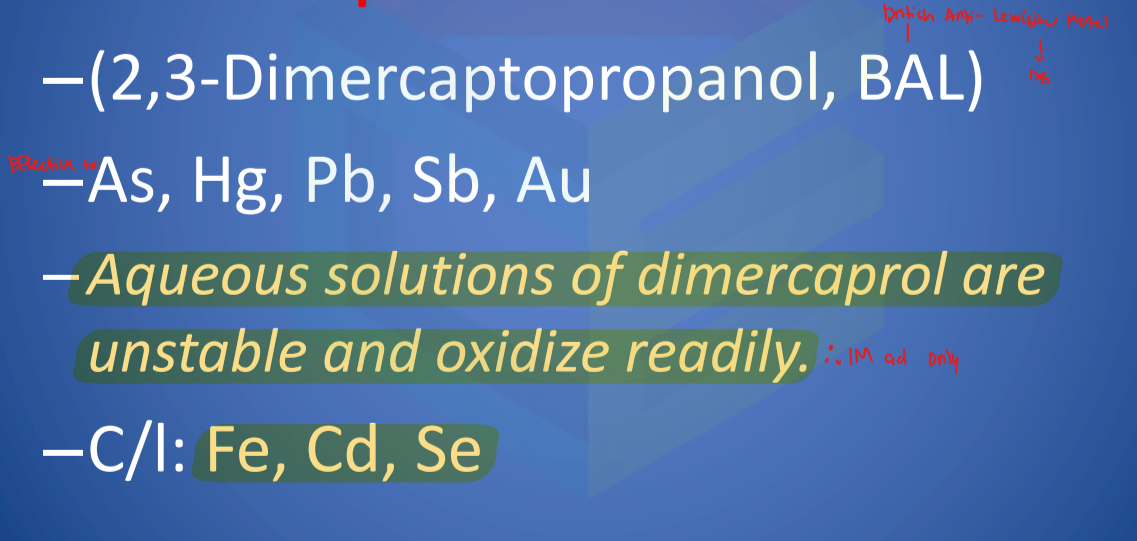
Dimercaprol
EDTA/Edetate calcium Disodium
Unithiol/Dimercaptopropanesulfonic acid DMPS
Penicillamine (Cuprimine)
D-DImethylcysteine
Deferoxamine
Deferasirox
tridentate chelator with a high affinity for iron
Prussian blue
Ferric ferrocyanide
Ferric hexacyanoferrate
has high affinity for certain univalent cations, particularly cesium and thallium
Irritants

Neurotics

Carcinogens

Asphyxiants

Lacrimators

Sternutator

Asthenics

Narcotics
