PDA III Schizophrenia background
1/22
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
23 Terms
General features of schizophrenia
-Important psychological functions are "split" apart (thought, emotion, motivation)
-Not split personality disorder
-No defined neuropathology or genetic cause: vary between pts
-Type of psychosis
-Chronic condition
-1% of population uniformly across cultures
-Onset is in late teens or early twenties: consequence of abhorrent brain development
Psychosis
-Disruption and distortion of thought and perception
-Loss of reality
Abhorrent brain development
-Construction of the brain was a little off
-Explains why onset occurs after puberty
Schizophrenia symptom classifications
-Positive symptoms: pt has, that a healthy person doesn't have
-Negative symptoms: pt doesn't have, that a healthy person does have
-Cognitive deficits
Positive symptoms
-Hallucinations (usually auditory, usually negative)
-Delusions (strong beliefs not based on reality, usually of persecution/grandeur)
-Paranoia
-Disconnected and illogical speech: sentences that don't make sense
Negative symptoms
-Reduced speech
-Flat or inappropriate affect (emotions)
-Avolition (loss of motivation/initiative)
-Social withdrawal
-Anhedonia (loss of pleasure)
-Lack of personal hygiene
Cognitive deficits
-Impaired working memory: very short term memory loss
-Impaired executive function:
Executive function
-Prefrontal cortex of the brain: makes you who you are
-Emotions, thoughts, knowledge, rules of society, manners, strategy
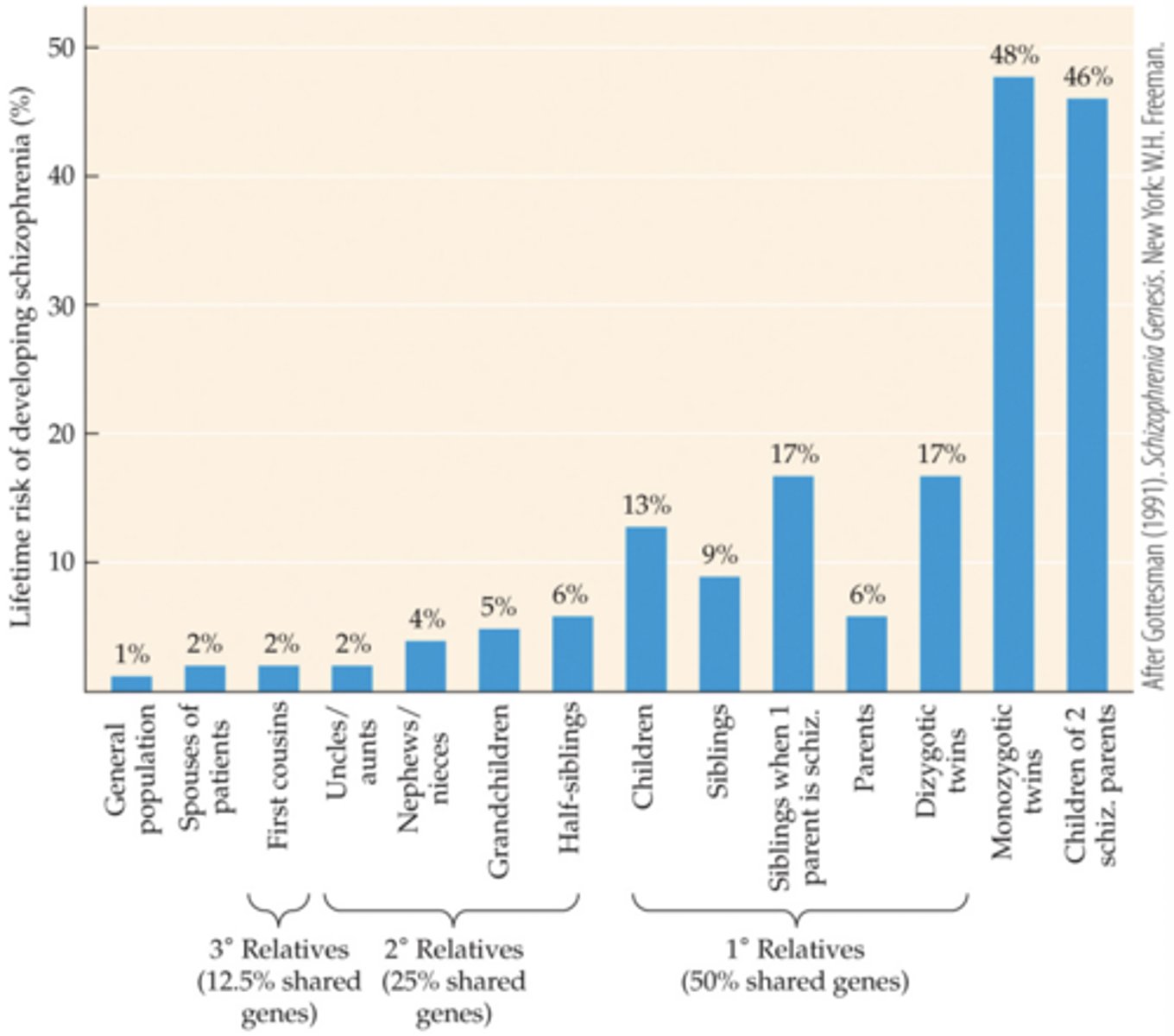
Lifetime risks of developing schizophrenia
-Strong genetic factor
-Some environmental factor: the womb, complications in birth (siblings vs dizygotic twins)
Schizophrenia hypothesis
-Occurs during times of rapid brain development (birth and puberty)
-Neural disorder of brain development
Neurochemical basis (2 hypotheses)
-DA hypothesis
-Glutamate hypothesis
-Serotonin hypothesis
DA hypothesis
-Symptoms (especially positive symptoms) are due to excessive dopamine activity in the brain
-Amphetamine and cocaine worsen positive symptoms
-All antipsychotics block D2 receptors (two exceptions)
-Some negative symptoms and cognitive deficits seem to be due to decreased dopamine function in the prefrontal cortex
Decreased DA relation to negative symptoms and cognitive deficits
-In monkeys, toxins that deplete DA produce working memory deficits similar to schizophrenia
-In PD (loss of DA neurons), there is a flat affect and avolition
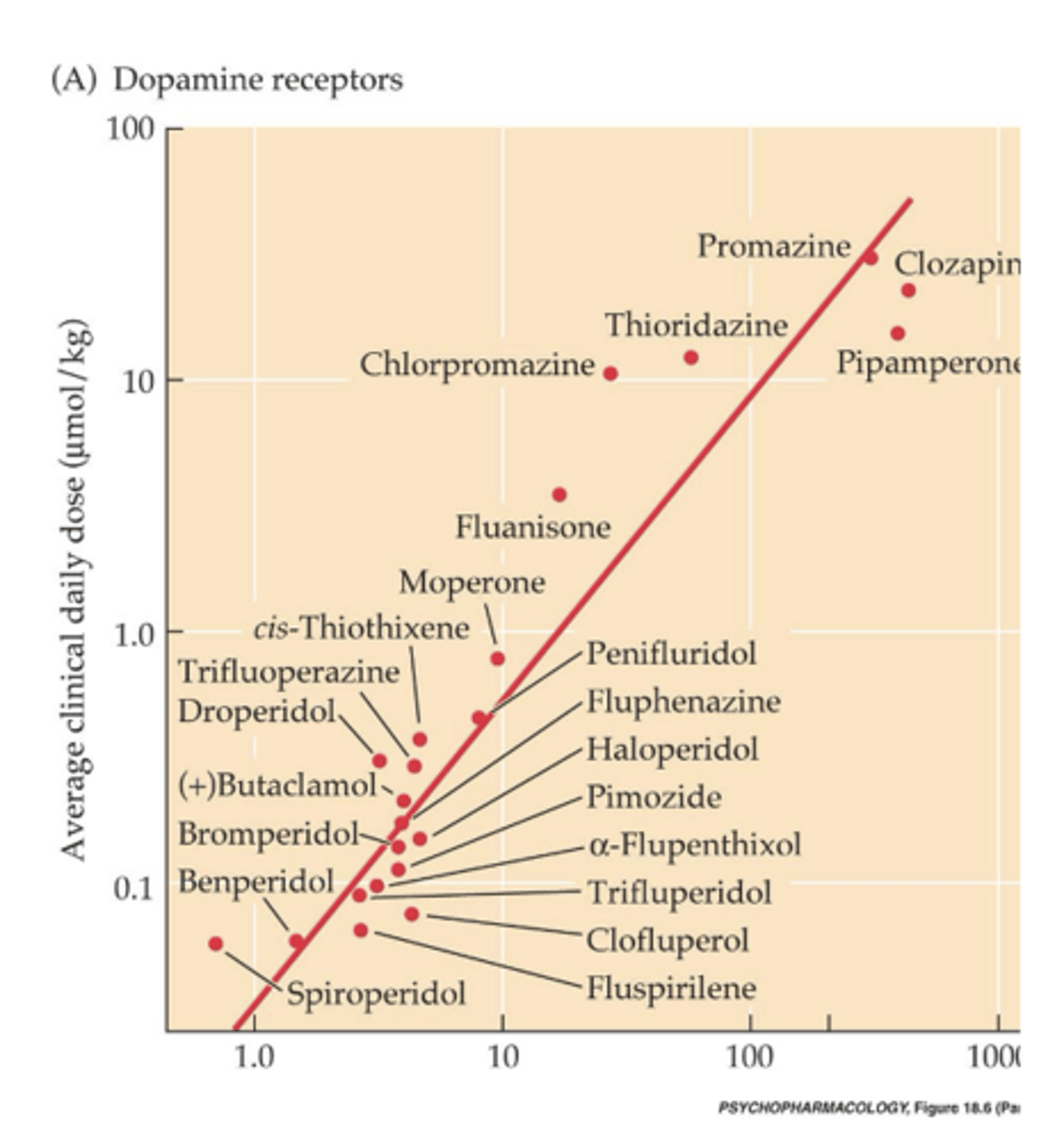
Dopamine concentration graph
-As it takes more drug to bind, the amount of drug needed to control symptoms goes up
-Bottom left has high affinity and high potency
-Linear relationship
-Drugs don't have a linear relationship in any other receptor in the brain
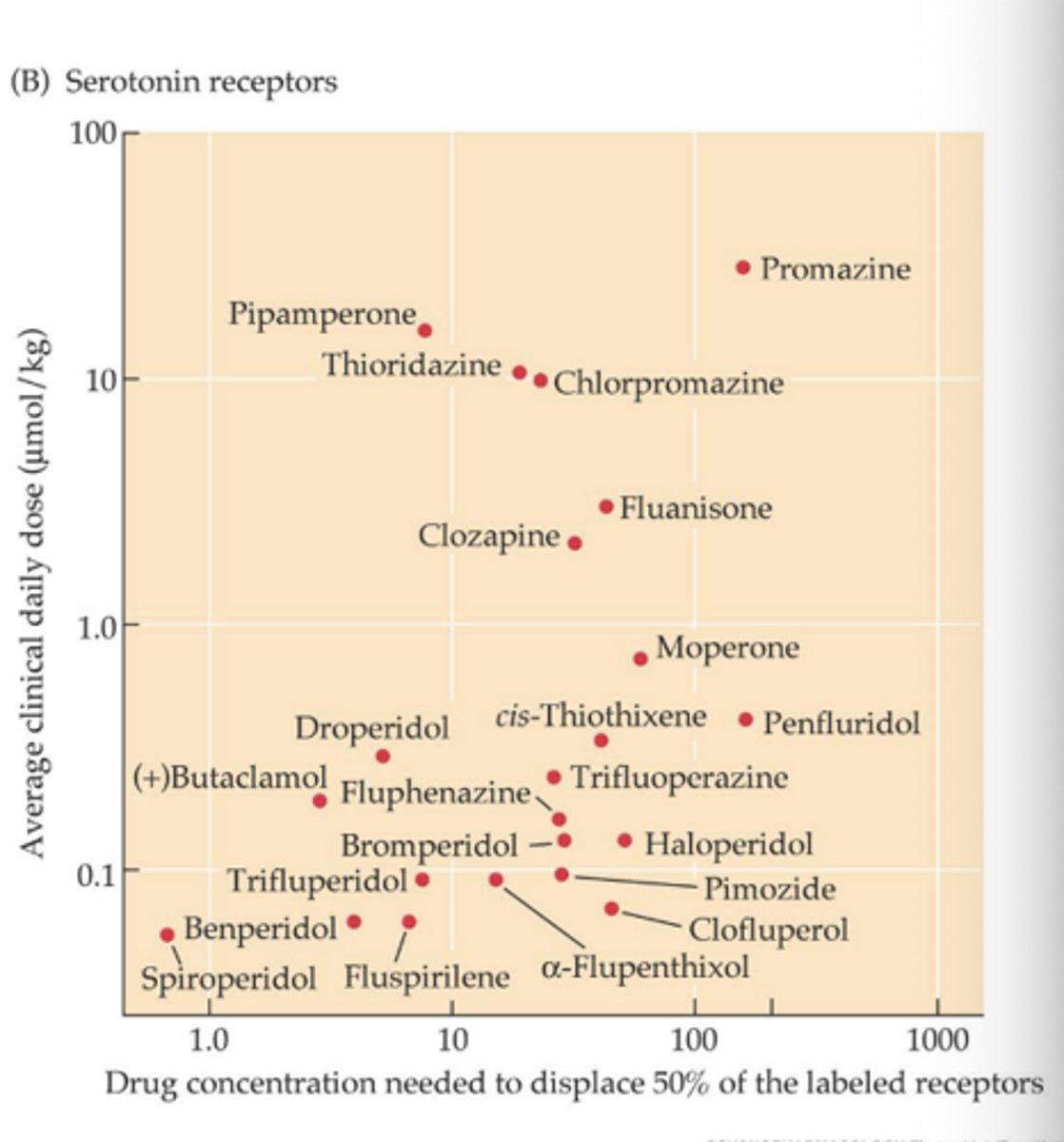
Serotonin concentration graph
-No correlation
Glutamate hypothesis
-Phencyclidine (PCP) is a psychotomimetic (drug that causes psychosis)
-PCP produces both positive and negative symptoms
-Mechanism of PCP is to block glutamate receptors: suggests that glutamate receptors are dysfunctional in schiz
-No drugs
Serotonin hypothesis
-Hallucinogenic drugs (LSD< mescaline, psilocybin, ecstasy) activate 5-HT receptors
-Second gen antipsychnotics block D2 and 5-HT2A receptors
-Second gen antipsychotics just as efficacious as older ones for positive symptoms
-More efficacious for negative and cognitive symptoms
Four key DA pathways
-Nigrostriatal pathway: S. Nigra to striatum
-Mesolimbic pathway
-Mesocortical pathway
-Tuberoinfundibular pathway
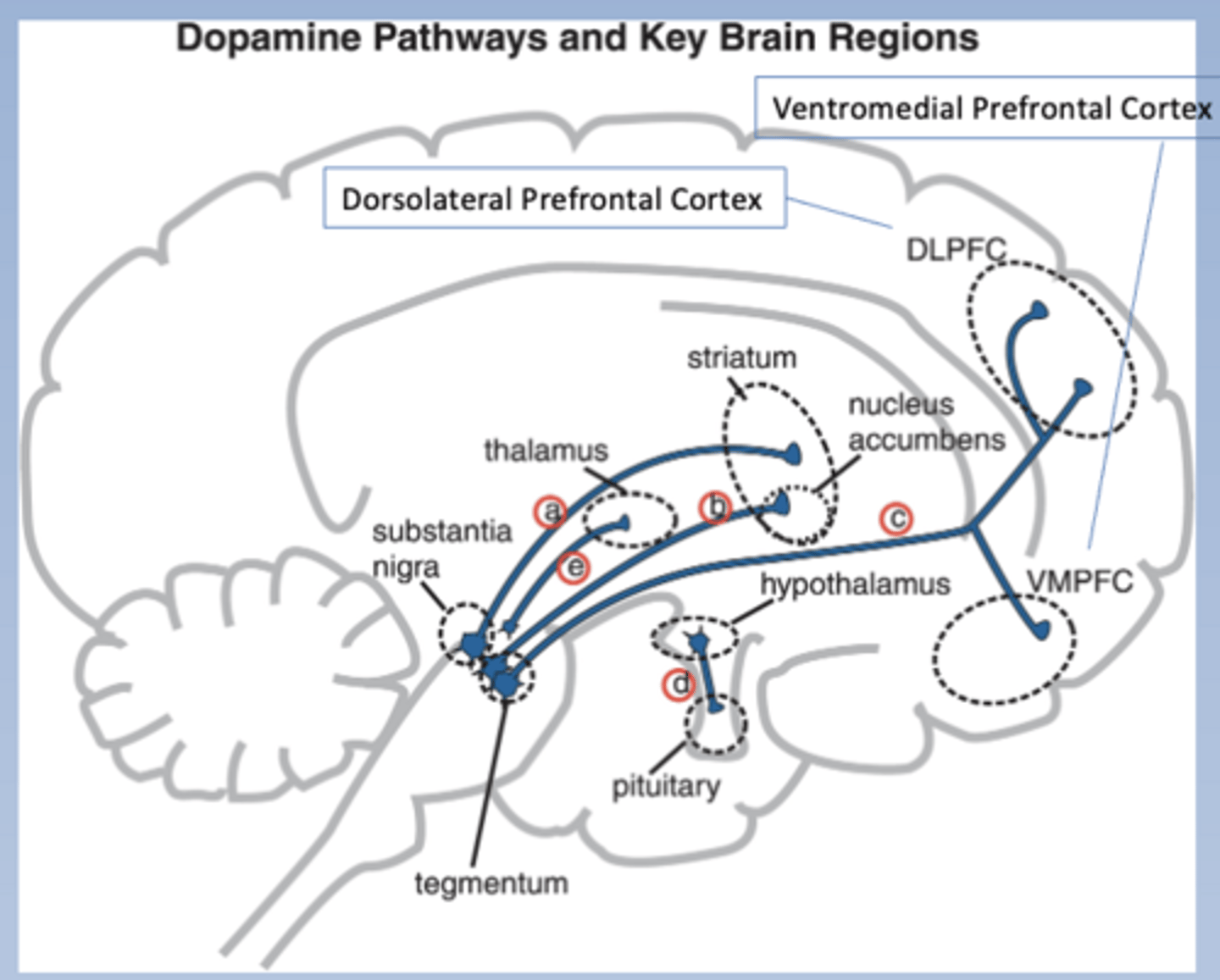
Nigrostriatal pathway
-Substantia nigra to striatum
-Striatum is aka dorsal striatum, motor striatum
-Modulates movement
-Associated w/ motor side effects of anti-psychotics (parkinsonism)
-Pathway a
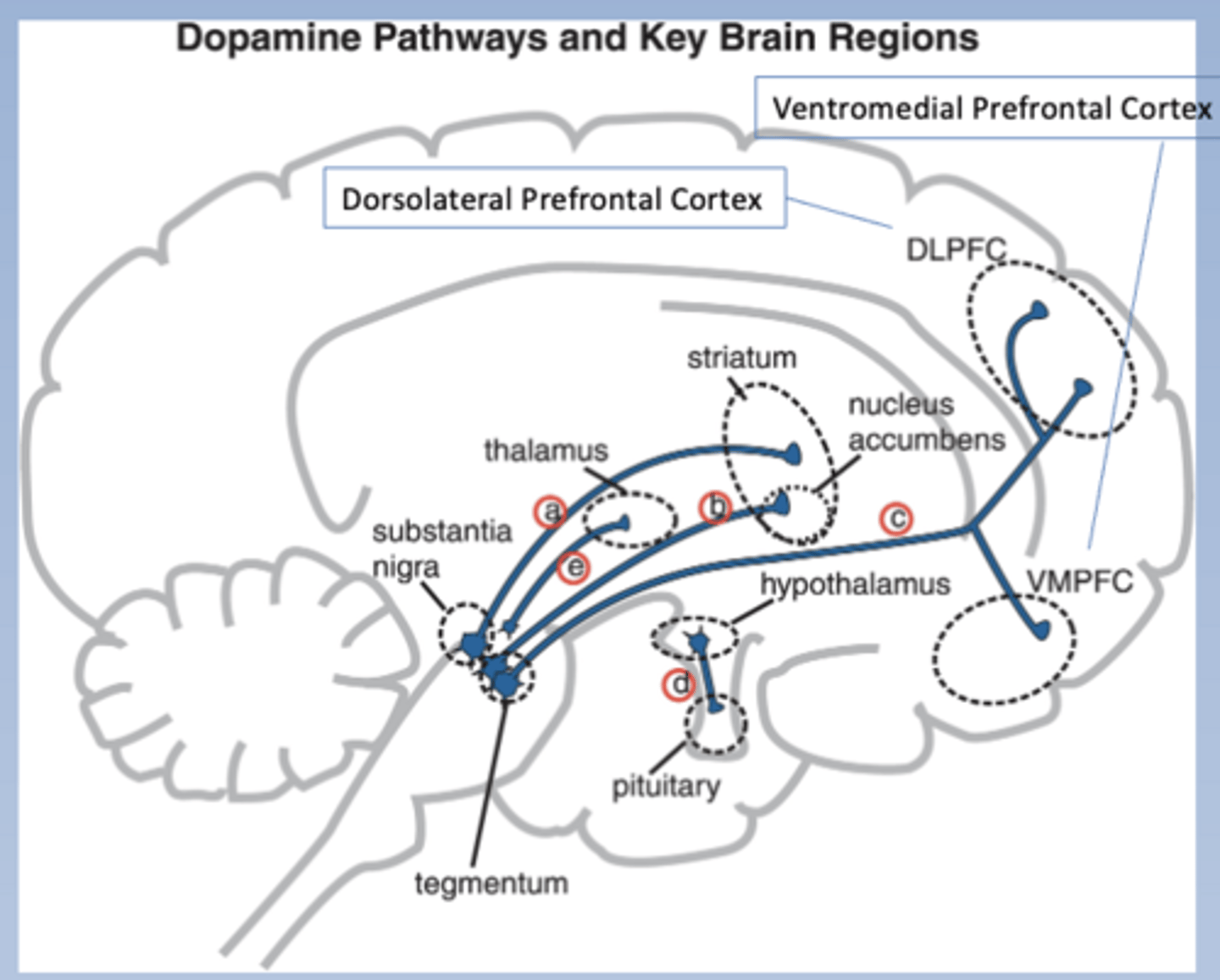
Mesolimbic pathway
-Tegmentum to nucleus accumbens in the limbic system (and others)
-Nucleus accumbens is a part of the striatum (may call it the ventral striatum or the emotional striatum)
-Hyperactive in schizophrenia (associated w/ positive symptoms)
-Pathway b
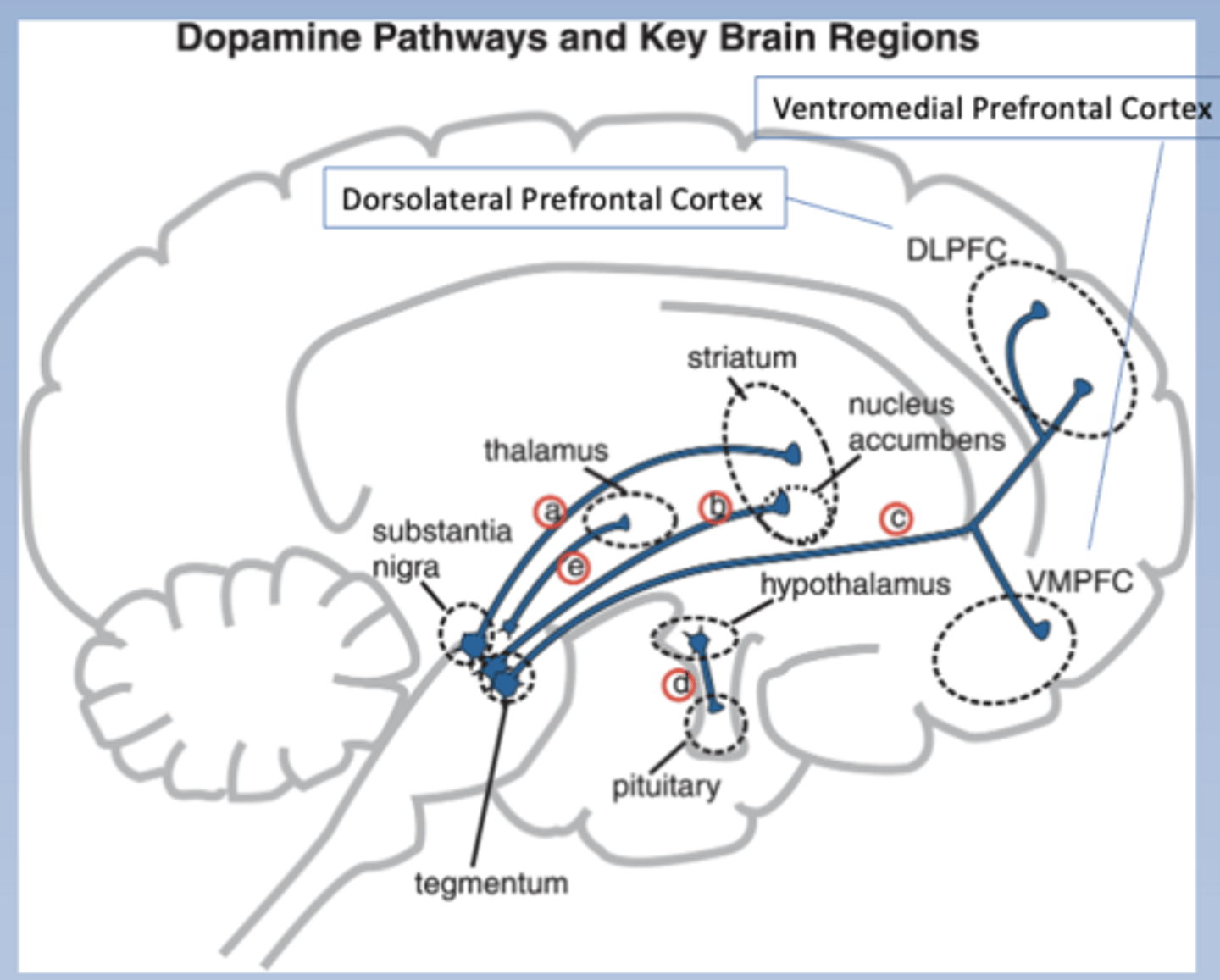
Mesocortical pathway
-Tegmentum to cortex
-DLPFC: dorsolateral prefrontal cortex
-VMPFC: ventromedial prefrontal cortex
-Hypoactive in schizophrenia (associated with negative symptoms and cognitive deficits)
-Pathway c
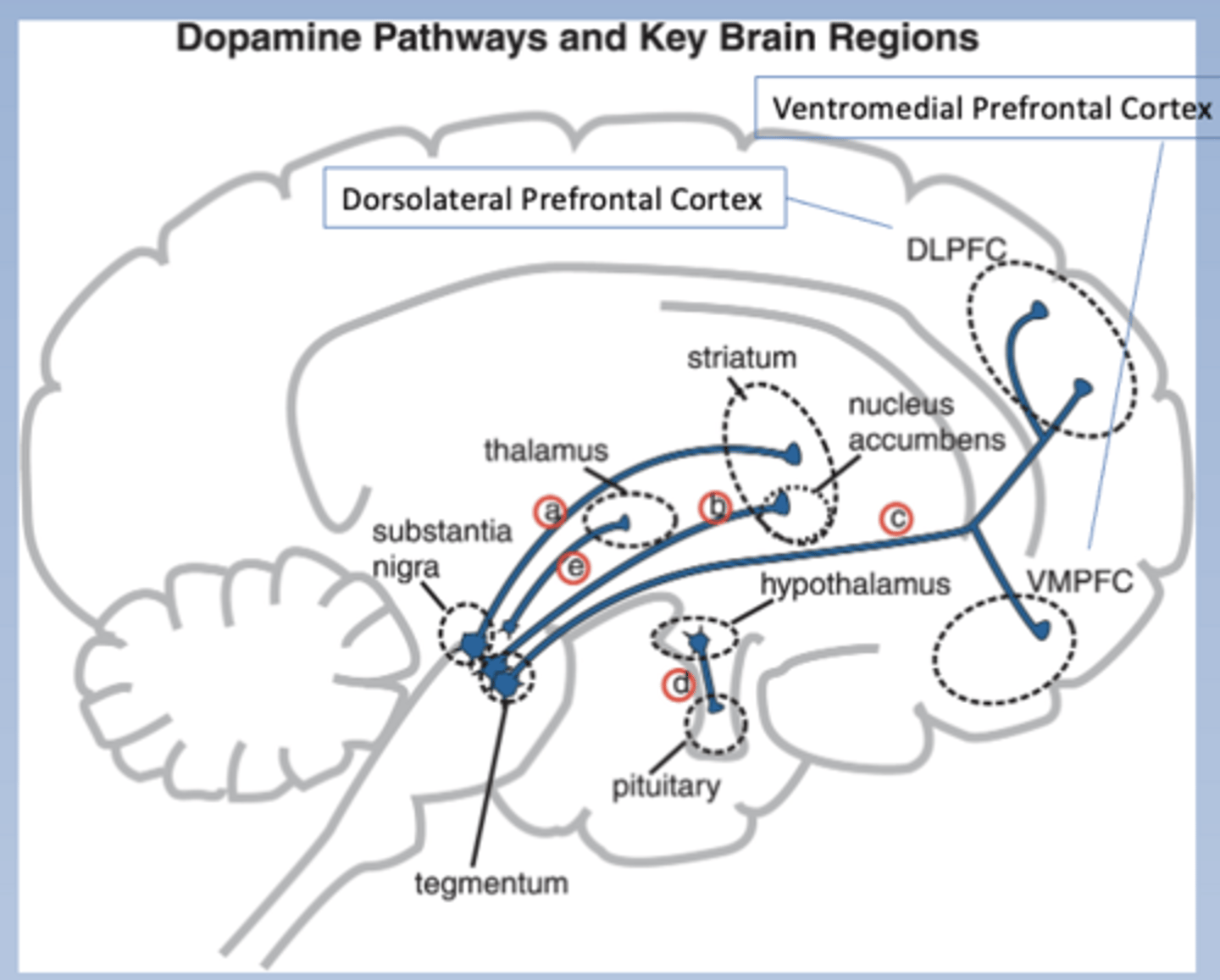
Tuberoinfundibular pathway
-ALA tuberohypophyseal pathway
-Hypothalamus to pituitary
-Pathway inhibits prolactin production and secretion
-Associated with neuroendocrine side effects of anti-psychotics
-Pathway d
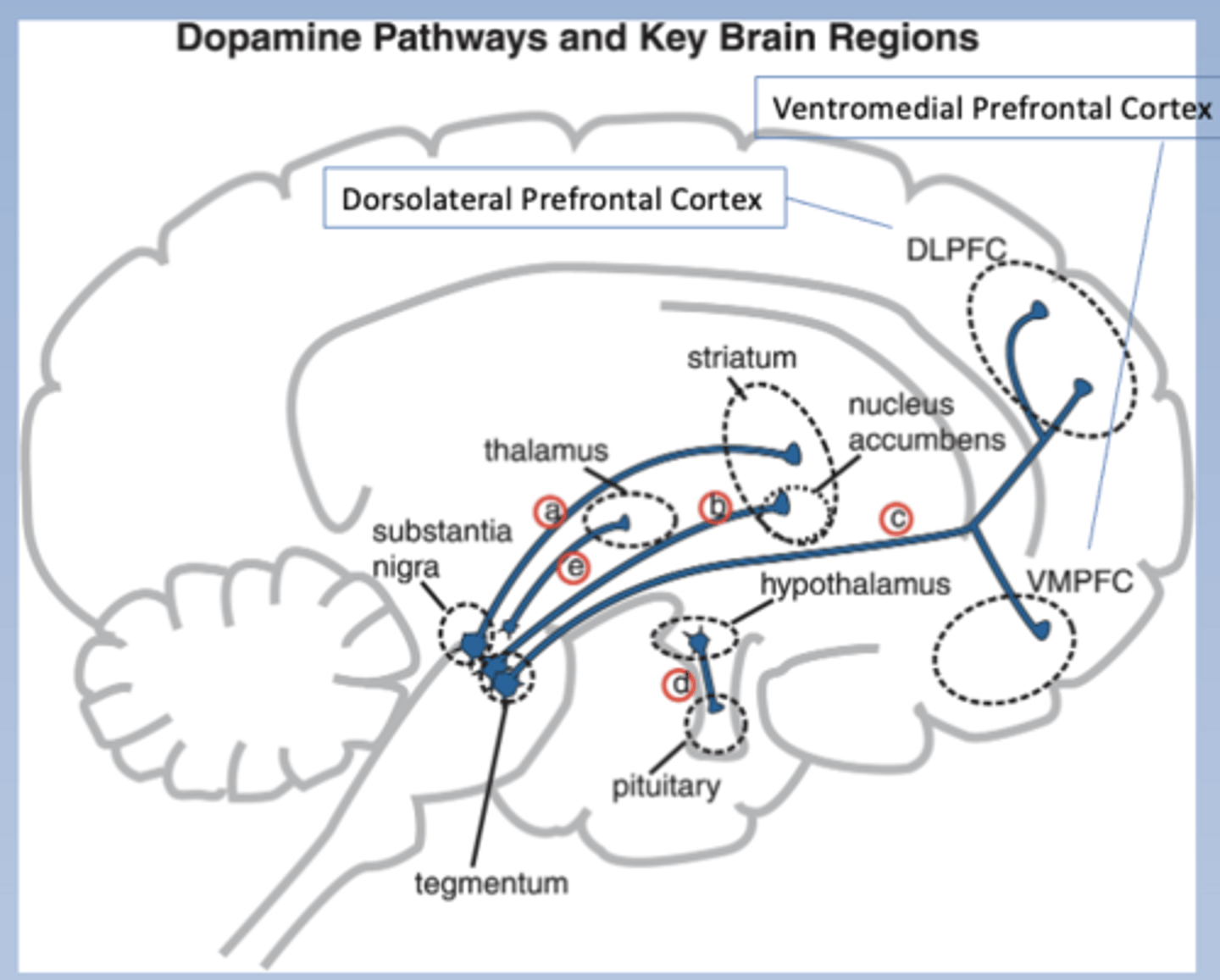
Ventral tegmental area
-Refers to both mesolimbic and mesocortical pathways