AOV - final
1/76
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
77 Terms
What is the unique relationship between the accommodation and vergence systems? important
Accommodation and vergence systet are closely linked systems, which interact to keep things single and clear, especially during near vision. If we increase convergence, we will also increase accommodation!!!
Near target → accommodation increases to keep the image clear.
Near target → convergence increases to keep the image single.
one cannot be tested without the other when evaluating function!!
Accommodation and vergence systems are assessed using the same four clinical domains
posture
amplitude
range/reserves
facility
What are the 4 aspects measured for both accommodation and vergence? What do these measure?
Posture
Accommodation: lead vs lag (MEM/binocular cross cylinder)
Vergence: phoria/alignment
Amplitude
Maximum ability
Accommodation: NPA
Vergence: NPC
Range / reserves
How much extra response can be exerted or relaxed while maintaining function (clear/single binocular vision)
Accommodation: PRA/NRA
Vergence: PRC/NRC BI/BO fusional reserves (PFV/NFV
Facility
Flexibility/speed/sustainability of changing response
Accommodation: lens flippers
Vergence: BI/BO prism flippers
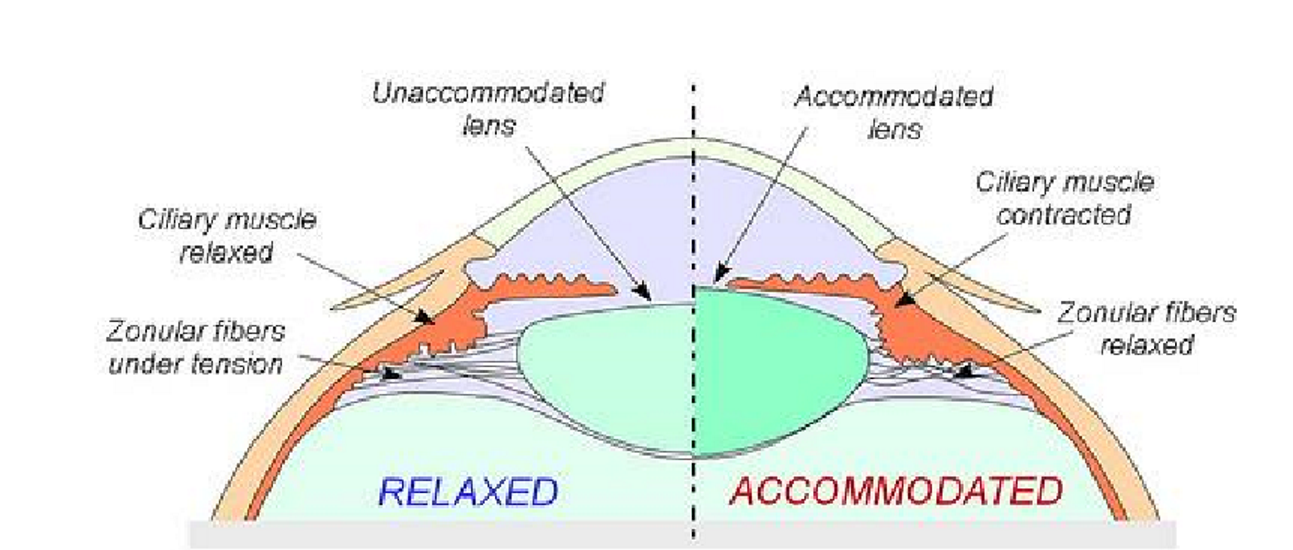
describe what happens during accommodation (zonules, lens etc)
near target → zonules relax → lens width increases (accommodated lens)
distant target → zonules strained → lens width decreases
How do you measure the 5 aspects of accommodation?
Posture
Binocular cross cylinder
MEM retinoscopy (monocular estimate method near retinoscopy
Amplitude
NPA
Relative accommodation
NRA/PRA at near
PRA at distance
Facility
accommodative flippers
±2.00 DS flippers first
±1.00 DS only if patient cannot clear ±2.00
Convergence accommodation
AC/A
what are 4 factors that stimulate accommodation. give clinical examples
blur → not focusing at the right distance, changing focusing target according to distance
Proximal awareness (if it’s up close I’ll likely have to read it) → awareness of something being close
Vergence movements → convergence stimulates accommodation
tonic accommodation → in the dark, or with no clear target, the eye rests at baseline focus (tonic accommodation) rather than true optical infinite
what innervates accommodation system? What neutransmitter acts on what receptor in what muscle(s)? What is the antagonistic pathway to accommodation
parasympathetic innervation
ACh mediated; muscarinic receptors; ciliary muscle and sphincter pupillae
sympathetic innervation
noradrenaline-mediated; relaxes ciliary muscle and dilates pupil
what impacts accommodation ability (can name like 3) … prob not that important and kinda obvious
AGE!
luminance → in dim light the accommodative response is reduced relative to accommodative demand
neurological deficit → ex CNIII probs
ametropia (ex. refractive error I think)
amplitude of accommodation in ppl with refractive error…. From best to worst. Why
myopes → emmetropes → hyperopes
myopes are good at accommodating because the power of their lens is already too high (focused Infront of retina). Less accommodation of the lens needed to view things at close distances.
what test measures combined evaluation of accommodation and vergence
Convergence accommodation (AC/A)
what is the binocular cross cylinder technique? What does it measure? How does it work? How to correct
measures accommodation posture (how accurately is the accommodative system focusing relative to where the visual stimuli is located?)
patient observes a cross target at habitual reading distance (40 cm)
binocular
+/- 0.5D cross cylindrical power (at 90 degrees)
if addition isn’t enough or eye is under-accommodated = horizontal lines clearer
referred to as lag
add until vertical lines are clearer
if vertical lines are clearer the eye is over-accommodated
referred to as lead
add minus until horizontal lines are clearer
why are amplitude accommodative tests performed monocularly? (NPA)
If you did it binocularly, the result could be contaminated by vergence/fusion factors
what is a normal NPA value?
NPA ≥
15D − 0.25 × age
what are the normal facility values (prob not that important)
monocular: 11 cpm ± 5; adults about 8 cpm
binocular: 10 cpm ± 5; adults about 8 cpm
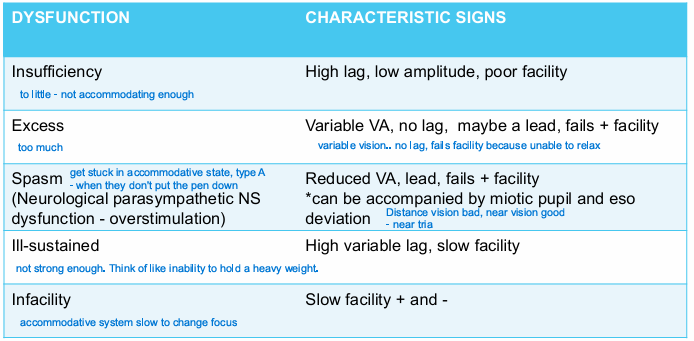
what are 5 accommodative dysfunctions and their signs? -important i think
insufficiency (not accommodating enough)
high lag, low amplitude, poor facility
excess (accommodating too much)
no log/maybe lead, high amplitude, fails + facility
spasm (stuck in accommodative state)- neurological parasympathetic NS dysfunction - overstimulation
ill-sustained (not strong enough)
infacility (too slow to change focus)
slow facility
what could be some causes of the following:
A 21 yo university student presents to you with symptoms of intermittent blurred vision in lectures especially towards the end of semester and after looking close for lengthy periods
accommodative excess or spasm
accommodative infacility
define vergence
a vergence is the simultaneous movement of both eyes in opposite directions to obtain or maintain single binocular vision
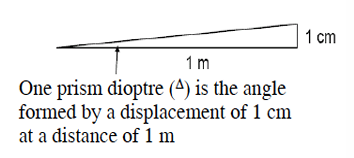
what is vergence measured in?
prism dioptres
the vergence system can be affected by many factor. name 3 categories and give some exampeles
Anatomical factors
EOM insertion
size, shape of globe
Neurological
any lesions affecting innervation of CNIII, IV, VI
general
fatigue, alc, medication
what is tonic vergence?
baseline convergence of the eyes without visual stimuli or acommodation
wiuthout tonic vergence, vergence sits aat
what do these tests measure?
vergence posture
how accurately are the eyes pointing relative to where the visual stimulus is located?
what is PRC and NRC? what does it measure. How to record
positive relative convergence
how much extra convergence can the patient use while maintaining single binocular vision?
negative relative convergence
How much extra divergence can the patient use while maintaining single binocular vision?
measures fusional vergences
measure in blur/break/recovery
Blur = target first becomes blurry
Break = target becomes double / fusion is lost
Recovery = you reduce the prism, and the patient reports the target is single again
ex. BO 10/16/10
would you do BI or BO first for NRC/PRC? Which one is which>
NRC (Base IN) should be first
then PRC (BO)
what is vergence facility? do the flippers use equal prisms? Why or why not
How quickly and efficiently can the vergence system change to uptake a convergence or divergence response on demand?
no (Prism facility/flippers (12^ Base out & 3^ Base in))
MORE base out (12) because our convergence ability is much better than our divergence ability
Minimum expected PRC/NRC measurements (near and distance): are expected PRC/NRC measurements lower at distance or near? WHY
PRC values > NRC values (eyes are better at converging than diverging)
PRC minimum expected
Near: 10/16/10 BO
Dist: 10/16/10
NRC minimum expected
Near: 10/16/10 BO
Dist: -/6/4
much lower in the distance! When we are looking distant we can’t really diverge much further
normal posture/phoria values (near and distance)
near: 3 exo ± 3^
dist: 1 exo ± 1^
normal vergence facility values
near: 15 cpm
vergence dysfunctions and characteristic signs (just give one for each)
Dysfunction | Characteristic signs |
|---|---|
Convergence insufficiency / CI | Near exo > distance exo; reduced PRC and BO facility; receded NPC |
Convergence excess / CE | Near eso > distance eso; reduced NRC and BI facility |
Divergence insufficiency / DI | Distance eso > near eso; reduced NRC at distance; distance blur/diplopia |
Divergence excess / DE | Distance exo > near exo; reduced PRC at distance |
Basic esophoria | Distance = near esophoria |
Basic exophoria | Distance = near exophoria |
Vergence infacility | Reduced BI/BO facility |
what could explain this case?
A 45 yo woman presents with symptoms of intermittent diplopia and blur after reading more than 15 minutes when reading in bed • It doesn’t go away unless she stops and gets some rest
Vergence dysfunction?
Decompensated heterophoria?
Refractive error?
what must you test before testing accommodation and vergence? Why?
Binocularity! (e.g. cover test, stereopsis, VA difference)
What is AC/A and how is it used clinically?
AC/A = accommodative convergence / accommodation
How much convergence changes for each dioptre of accommodation.
units Δ/D
does accommodative-convergence (AC/A) increase or decrease with age
AC/A = accommodative convergence / accommodation
Accommodative-convergence increases with age (the amount of convergence generated per diopter of accommodation)
This is likely due to the fact that our accommodation reduces with age and as a result the convergence response increases to compensate – so AC/A should increase as we get older
how does the AC/A test work? What are the steps?
We alter the amount of accommodation and measure vergence changes as a result of that change on pretence card (ex. relax + or stress -)
prentice card (6 base down infront of eye)
establish near reading
repeat with +2, +1, -1, -2 flippers and document responses
in AC/A, would you expect more eso or exo readings with plus and minus lenses?
+ = relax accom, more exo
- = strain accom, more eso
when accommodative demand increases (minus lens), what happens to the AC/A ratio and the amount of convergence that is created
AC/A increases
convergence increases with increased accommodative effort
what is PRA/NRA? what does it measure? how does it work
range/amplitude of accommodation
PRA - positive relative accommodation
add minus lenses until the target becomes blurry
measuring the amount of accommodation that can be EXERTED while maintaining binocular single vision, without changing the vergence
NRA - negative relative accommodation
add plus lenses until the target becomes blurry
The amount of accommodation that can be RELAXED while maintaining binocular single vision, without changing vergence
colour vision: opia vs anomaly
opia = missing cone photopigment
anomaly = anomalous cone photopigment
What are the main congenital colour vision deficiency types? (3 categories → 6 types)
Protan defects
long-wavelength / “red” cone system
protanopia = missing red cone photopigment
protanomaly = anomalous red cone photopigment
Deutan defects
medium-wavelength / “green” cone system
deuteranopia = missing green cone photopigment
deuteranomaly = anomalous green cone photopigment
Tritan defects
short-wavelength / “blue” cone system
tritanopia = missing blue cone photopigment
tritanomaly = anomalous blue cone photopigment
what is the prevalence of congenital CVD?
8% in men (1/12), 0.5% in women
what is the most common colour vision defect (CVD) subtype
deuteranomaly (5%)
How does testing differ for congenital vs acquired colour vision defects? important
Congenital CVD
binocular
often stable
Acquired CVD
may be monocular/asymmetric
arises from damage along colour vision pathway
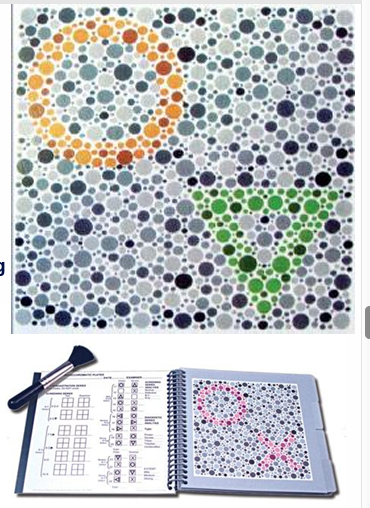
what colour vision test category is Ishihara?
Pseudoisochromatic plates
name three colour vision test categories (there are more but 3 should be fine)
pseudoisochromatic plates
ishihara
HRR
F2
Arrangement tests
D15, Adams, Lanthony, H16
FM100
Anomaloscopy (colour matching)
Computerised testing
CAD
Konan CCT-HD
Occupational specific testing (testing to see if someone can do specific task)
lanterns
Wire tests
what test category gives us a definitive diagnosis?
Anomaloscopy
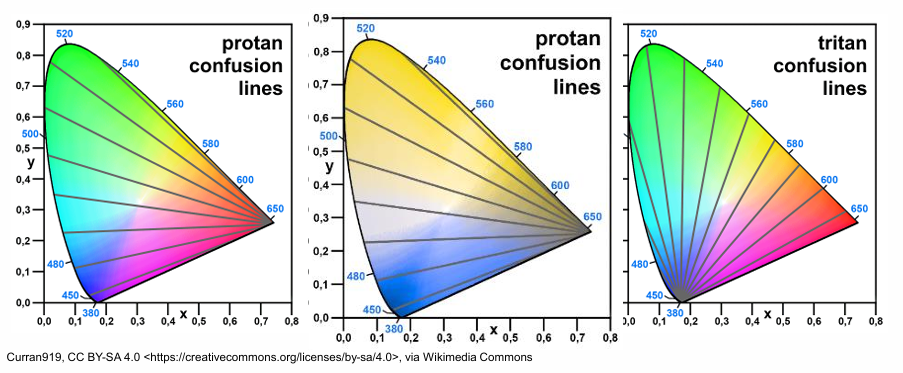
How are pseudoisochromatic plates designed? Are they good for detection or grading?
use colour camouflage
designed using colour confusion lines
lines along which someone with that particular deficiency will see the same colour
good for detection, not very reliable for grading
What are the 6 types of plates in the 24 plate edition? what do they see
introduction plate
seen by all observers
checks VA sufficient
detects malingerers
transformation
normal sees one figure, CVD sees different figure
vanishing
CVD sees nothing
hidden
CVD sees a figure, normal may not
classification
attempts protan/deutan classification
Protans confuse red and grey- say “6” or (2) 6 • Deutans confuse purple and grey- say “2” or 2(6)
tracing
for kids - trace with cotton bud
Pros and cons of Ishihara
pros:
high sensitivity and specificity, not sensitive to luminance changes
sensitivity 1.0, specificity 0.98
cons:
red/green testing only, no tritan plates
Does not test severity - number of errors is not an index of severity
diagnosis by type is not reliable
some ppl combine dots when they shouldn’t’ but not necessarily indication of CVD
describe the HRR test. What is it useful for
Test Tritan defects, and diagnostic plates examines severity
like Ishihara but only symbols. Similar sensitivity and specificity
may detect Tritan defects
includes screening plates to test P, D and T
if a pass is obtained CV id normal
14 diagnostic plates provide type and extent (mild, moderate or severe) of defect
not perfect
What is the F2 plate used for? What would result indicate?
F2 plate may detect tritan defects.
Normal colour vision:
sees 2 squares in correct location
green clearer/more defined than blue
Possible tritan error:
only sees blue, or blue is clearer
Not tritan error:
only sees green
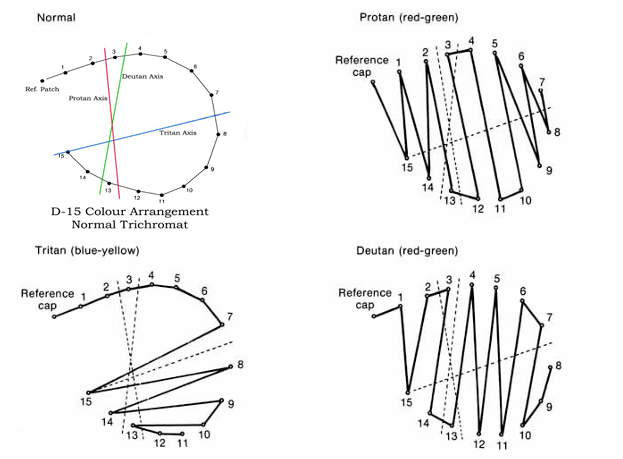
What is the Farnsworth D15 determine? What category is it?
D15: hue discrimination / arrangement test
Used to:
separate mild CVD from moderate/severe CVD
classify type by orientation of crossing errors
in D15, what will the patient place next to eachother if they have a CVD? what will this look ilike on the recording
colours lying on their confusion loci will be placed next to eachother
look like a crossing
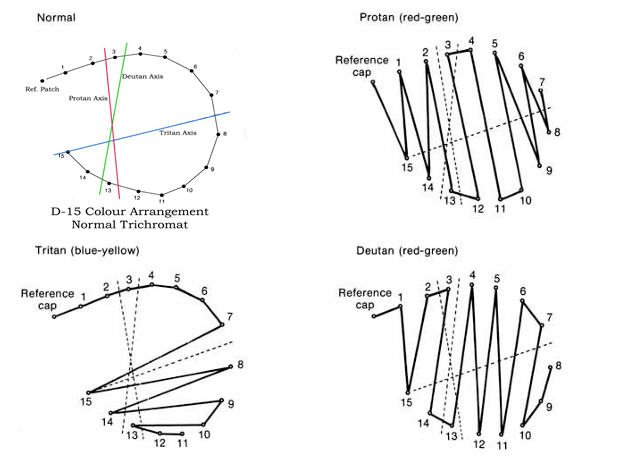
How does D15 work? Principle and fail rate
hue discrimination
Principle: patients will place colours lying on confusion loci are placed next to each other.
order of colours as arranged by the patient is recorded on a circular diagram
Fail:
generally 2 or more diametrical crossings
Not significant:
minor transposition error
especially around colour 7
Compare D15, Lanthony, and H16, Adams
All use confusion-line principles at different saturation levels.
D15
standard saturation
moderate/severe screening
Desaturated = Adams and Lanthony
More saturated = H16
more saturated
only red-green
fail = 3+ errors
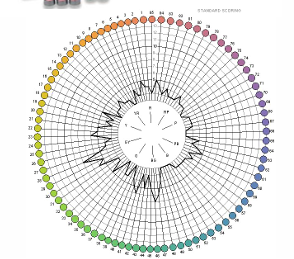
What is the Farnsworth-Munsell 100 Hue test used for? What is it interpreted by? What type of CVD would it be good for
FM100 = hue discrimination / arrangement test
patient arranges 85 closely spaced coloured caps in hue order
interpreted by:
total error score (severity)
distribution of errors around the hue circuit (type P, D T)
mild deficiencies may go undetected
what is the normal values for FM100? What is FM100 useful for?
take square root of total error score
normative values change with age!
useful for acquired CVD
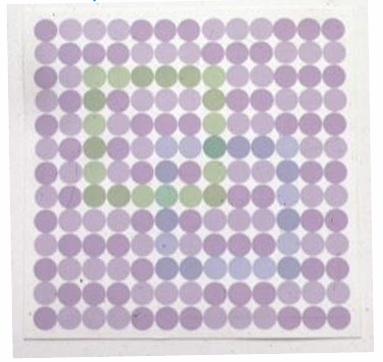
what test is a coloured cap mixed in with neutral greys? What does this test provide indication of?
Mollon Reffin Minimalist
Coloured cap mixed in with neutral greys and patient needs to identify it
good for kids
Provides an indication of severity along protan, deutan and tritan axis
what is the gold standard test for diagnosis? What is
anomaloscopy
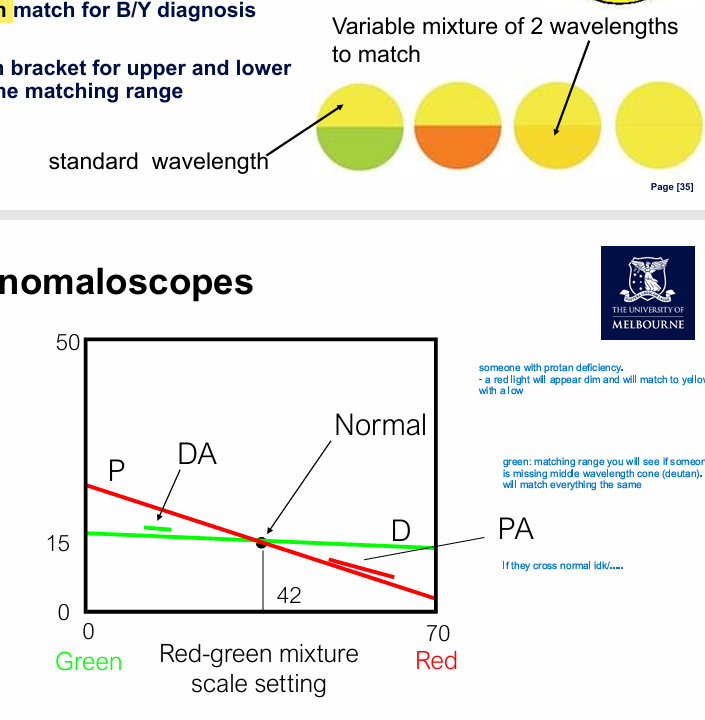
how does Anomaloscopy work? What are the 2 equations
Anomaloscopy - colour matching test by additive colour mixing w/ spectral colours.
Equations:
Rayleigh equation match = red-green diagnosis
red/green mixture until it appears yellow
abnormal mixture of green/red: more green = DA, more red = PA
Moreland equation match = blue-yellow diagnosis
Process:
rough match
bracket upper/lower limits
plot matching range
What does the Medmont C-100 do?
Main function: differentiate protan vs deutan.
Patient views yellowish flickering light from alternating red/green LEDs and adjusts until flicker disappears/minimises.
Useful because:
quick: 1–2 minutes
inexpensive
good sensitivity/specificity
may detect female carriers of protan/protanomalous genes

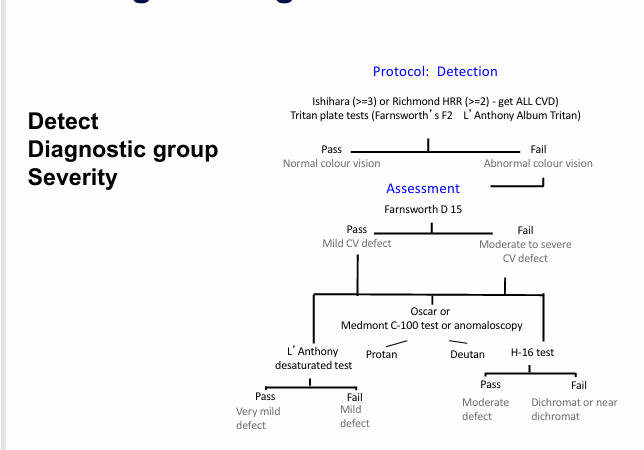
IMPORTANT - in clinic, how would you screen/detect, assess severity, and diagnose
Detect = Ishihara, HRR, tritan plate test
pass = normal CV
fail = abnormal CV
Assess severity: Farnsworth D15 (pass = mild, fail = moderate to severe)
pass = desaturated test
fail = H-16 saturated test
Anomaloscopy or medmont c-100
confirm protan, deutan, tritan
vergence system: define posture and give 2 clinical tests that can measure this
Posture: the resting alignment of the eyes relative to the visual target when fusion is disrupted. Ex. how accurately the eyes are pointing when they’re allowed to drift
cover test
Prentice card
Von Grafe
Maddox rod
vergence system: define amplitude and give a clinical tests that can measure this
amplitude: the maximum amount of convergence or divergence the system can do while maintaining single vision
NPC
vergence system: define facility and give a clinical tests that can measure this (be specific)
facility: how quickly and efficiently can the vergence system switch between convergence and divergence demands. It reflects the speed of the vergence response.
12 base out and 3 base in flippers
vergence system: define reserves and give 2 clinical tests that can measure this
reserves: how much spare capacity of fusional vergence available beyond the patient’s habitual posture while maintaining clear and single vision.
PFV/NFV
BO (PRC) and BI (NRC) ranges at distance and near, measured in prism dioptres with blur/break/recovery
what is the normal range for AC/A test? How to calculate?
normal range = AC/A = 4prismD /D ± 2 (i.e. 2-6 prism diopters/D)
AC/A ratio = (phoria with additional minus lenses - baseline phoria) / power of additional minus lenses
accommodation posture: what it means and tests to measure
posture: Accuracy of the accommodative response: is the patient focusing on, behind (lag), or in front (lead) of the near target
binocular cross-cylinder
MEM retinoscopy
accommodation amplitude: what it means and tests to measure
amplitude: Maximum amount of accommodation the patient can generate
NPA
accommodation reserves: what it means and tests to measure
reserves: spare capacity of the accommodative response. How much can accommodation be relaxed or stimulated while still maintaining a single and clear target?
NRA/PRA
PRA - positive relative accommodation
add minus lenses until the target becomes blurry
measuring the amount of accommodation that can be EXERTED while maintaining binocular single vision, without changing the vergence
NRA - negative relative accommodation
add plus lenses until the target becomes blurry
The amount of accommodation that can be RELAXED while maintaining binocular single vision, without changing vergence
accommodative facility: what it means and how to measure
facility: how quickly and efficiently accommodation can change back and forth (when strained and relaxed)
measured with ± 2 DS flippers first (if can’t clear then go to 1)_
NRA/PRA normal value
Normal range: +2.00 ±0.50 D
similar for negative I think
normal binocular X cyl result
+0.5 ± 0.5
normal near and distance phoria values
near: 3 ExoP ± 3
distance 1 exo ± 1
normal near and distance NRC/PRC value (and what prisms do u use)
NRC
measured in blur/break/recovery
near: 10/16/10 BI
distance: -/6/4 BI
PRC
measured in blur/break/recovery
near: 10/16/10 BO
dist: 10/16/10 BO
normal vergence facility values
12BO/3BI
near: 15cpm
normal accommodation facility (monocular and binocular)
mono
11cpm ± 5SD (8cpm for adults)
bino
10 cpm ± 5 SD (8cpm for adults)
normal AC/A range?
2-6 prism diopters
what will happen to the AC/A ratio as we INCREASE negative lenses
AC/A ratio increases
* Increases as we strain accom and with age
normal NRA/PRA values
PRA: -2.5 D (and higher)
NRA: +2.5D (and higher)