3. large animal med- equine colic workup
1/42
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
43 Terms
what is colic? how common is it?
colic=vague term for abdominal pain
incidence of 10% of horses per year (75% cases are mild/only require 1 dose of pain meds)

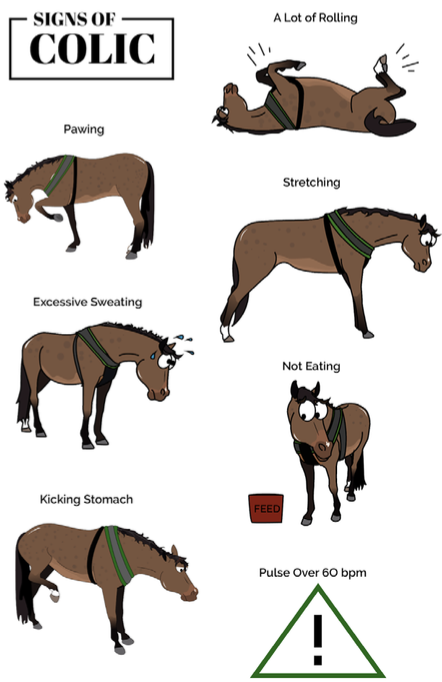
what are signs of colic/abdominal pain in horses?
-lying down for long periods
-decreased appetite
-restlessness
-quivering upper lip
-looking at sides
-repeated stretching
-kicking at belly
-crouching/trying to lay down
-sweating
-rolling
what history questions should be asked when working up a colicking hrose?
-clinical signs/level of pain/duration
-meds given and response
-recent management/diet changes
-last defecation
-drinking/appetite
-presence of abdominal distention
-previous colic episodes/colic sx
-breeding/pregnancy
-deworming
-current diet

what is included in the physical exam of a horse with colic?
-distance exam (posture, attitude, appetite)
-grade pain level
-BCS and weight
-basic general exam (TPR, digital pulses)
-perfusion/hydration status
-GI auscultation/percussion

what diagnostics are done for horses presenting with colic?
-nasogastric intubation
-rectal exam
-belly tap
-abdominal U/S and rads
-CBC/chem
-fecal float (parasites) and sedimentation (sand)
-oral exam
-gastroscopy
how much reflux is normal in horses?
<2L of net fluid in a full sized horse

how is net refluxed calculated when performing nasogastric intubation in horses?
reflux= total volume of fluid obtained - volume of fluid instilled

if you are giving oral fluids through the NG tube, what is the max amount you can give for a full sized horse?
give no more than 8-10L
what are complications of nasogastric intubation?
-epistaxis (if tube hits ethmoids)
-pharyngeal/esophageal trauma (esp if tube left in for several days)
-aspiration (accidental NT intubation)

what restraint is necessary when performing a rectal exam in horses?
physical restraint +/- chemical (sedation) restraint
how is rectal relaxation achieved for rectal exams?
buscopan IV (smooth muscle relaxant), local lidocaine
how are rectal exams performed to prevent complications?
-use lots of lube
-evacuate rectum of feces
-never force arm against peristalsis
what structures are normally palpated via rectal examination in horses?
-aorta and iliac arteries
-caudal pole of left kidney
-nephrosplenic ligament
-caudal border of spleen
-pelvic flexure
-small colon with fecal balls
-bladder
-female repro organs
-cecum (medial cecal band)
what are the limitations of rectal exams in horses?
-only caudal 1/4-1/3 of abdomen can be palpated in a full size horse
-unable to perform in small patients
what is the main complication of rectal exams?
rectal tears
-always inspect rectal sleeve after rectal exam
-inform owner of concern
-bare arm exam to determine location/depth
-refer

what are indications of performing an abdominocentesis?
-persistent colic (differentiate from surgical vs non-surgical)
-to diagnose peritonitis
-to diagnose GI rupture (recommend euthanasia)
-if neoplasia is a differential
what are clinical signs of peritonitis?
fever
mild/chronic colic
diarrhea
what should normal peritoneal fluid look like?
-clear to straw colored
-watery (equine fluid should not clot)
-cytology: neuts and mononuclear cells predominate in horses

what is the normal WBC/TP/lactate/glucose of normal peritoneal fluid in horses?
WBC: <5000 cells/uL
TP: <2.5g/dL
lactate and gluose similar to blood values
what is the color of abdominal fluid in horses with a strangulating lesion? what is the lactate, glucose, total protein? WBC/diff/morphology?
1. color: serosanguinous
2. lactate: 2x that of blood
3. TP: 2.5-6g/dL
glucose: similar to serum
neutrophils predominate/may be degenerate, >5,000-50,000 WBC,
what is the color of abdominal fluid in horses with septic peritonitis? what is the lactate, glucose and total protein? WBC/diff/morphology?
1. color: cloudy
2. lactate: elevated (bc bacteria produce lactate)
3. TP: elevated
4. glucose: lower, differences >50mg/dL (bc bacteria are consuming glucose)
5. neutrophils predominate/may be degenerate, elevated-100,000 WBC, intracellular bacteria
what is seen in septic abdomens with markedly septic inflammation?
cell destruction
what is the color of abdominal fluid in horses with a GI rupture? what is the lactate, glucose and total protein? WBC/diff/morphology?
color: green to brown
lactate: elevated
TP: elevated
glucose: lower than serum, difference >50 mg/dL
neutrophils predominate/degenerate/intracellular bacteria, elevated WBCs
how is enterocentesis (accidental gut puncture) differentiated from GI rupture with peritoneal fluid analysis?
with enterocentesis, will see:
-plant matter
-mixed extracellular bacteria and protozoa
-variable TP
-low nucleated cell count/white blood cell count (<1000); can increase tho in subsequent taps by 4 hours
are complications caused by abdominocentesis common?
no (0.47%)
what are possible complications of abdominocentesis?
-skin hemorrhage
-splenic penetration (P is fine, but complicates analysis)
-enterocentesis (puncture colon)
-cellulitis and SQ abscessation (animals with septic peritonitis)
-failure to succeed (cant get fluid/unsuccessful tap)
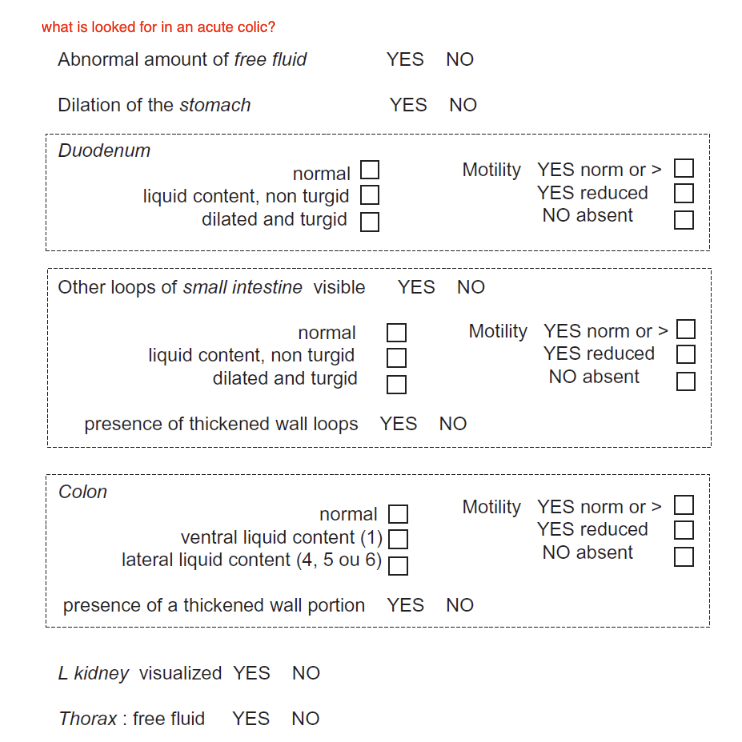
what are indications for abdominal ultrasound for colic workups?
-signs of colic for which diagnosis could not be made
-helpful in deciding if surgical intervention should be performed
-chronic and intermittent colic
-unexplained weight loss, decreased appetite and diarrhea
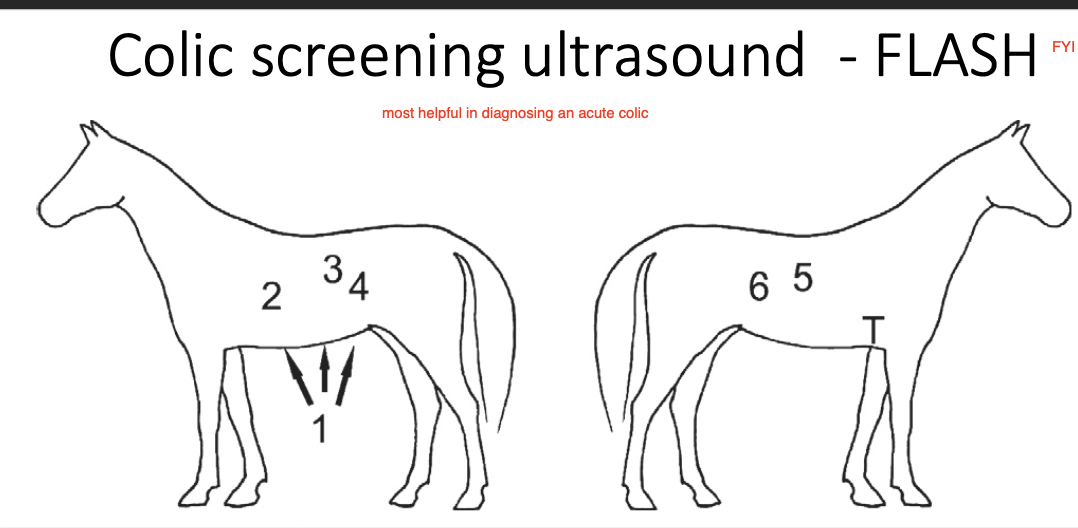
what are limitations of abdominal ultrasound for colic workups?
-blocked by gas (esp if colon is full of gas)
-maximum depth is 25-35cm with a 3.5mHz curvilinear probe
what lab work is performed for horses presenting with colic?
1.CBC
2. chemistry (kidney and liver dz, lyte abnormalities, decreased albumin [colitis])
3. blood gas (evidence of dehydration, lytes, lactate level)
what causes of colic can a CBC help diagnose?
1. helps with evidence of infection (peritonitis, abdominal abscess); neutrophilia
2. acute inflammation/endotoxemia (colitis, colon torsion); neutropenia
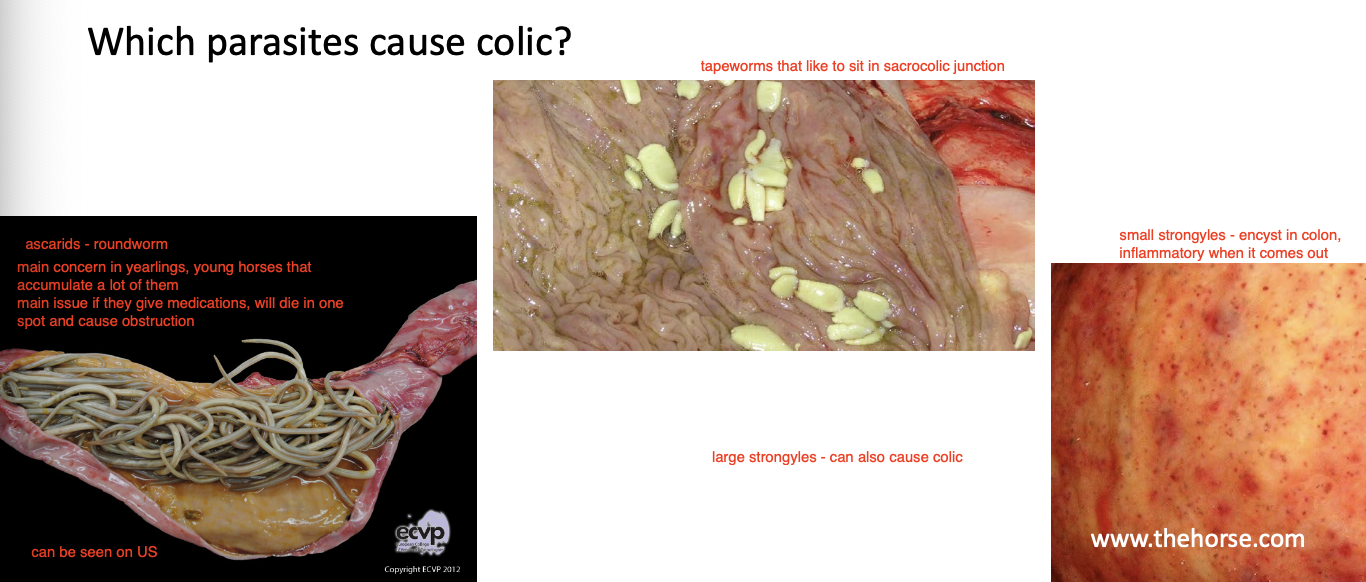
what parasites causing colic can be identified in fecal flotations?
-roundworms (ascarids- cause obstruction when dead)
-tapeworms
-small strongyles (encyst in colon)
-large strongyles
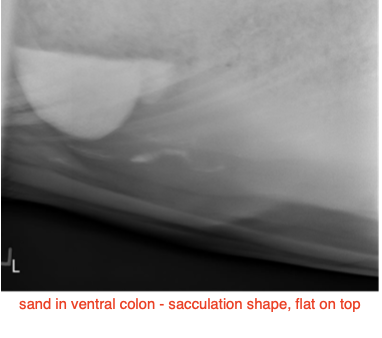
what can crude fecal sedimentation be helpful for?
to see if passing sand in stool — does not necessarily mean sand is a cause of colic

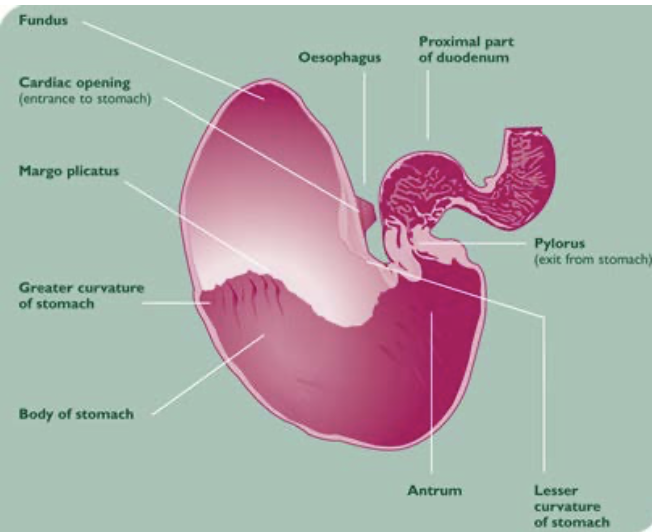
what are indications for performing gastroscopy for horses with colic?
-chronic, low grade colic
-suspicion of gastric ulcer or neoplasia
-to perform duodenal biopsy (concern for IBD)
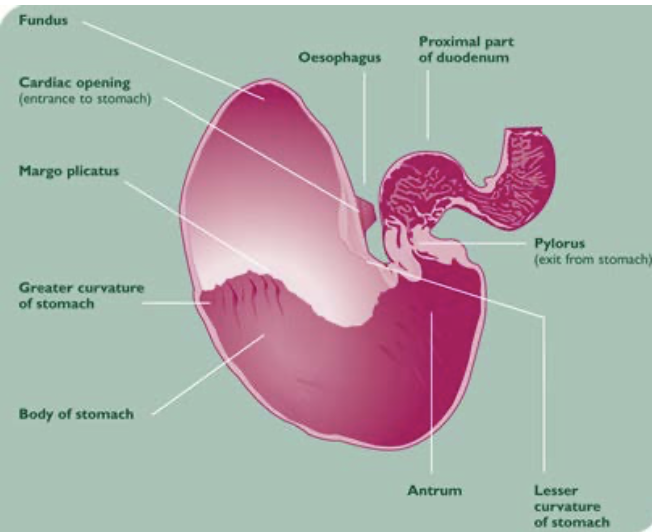
how should horses be prepared for gastroscopy?
fast for 12-16 hours, remove water 1 hour prior
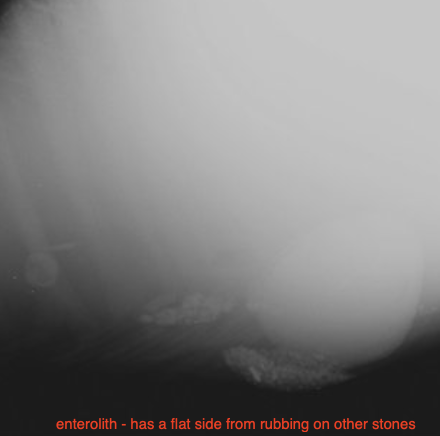
what are indications of taking abdominal radiographs?
-suspicion of enteroliths or sand
-chronic colic
-areas that enteroliths are common
what are GI causes of non-obstructive (distention/inflammation) colic?
-spasmodic/gas colic
-proximal enteritis
-IBD
-colitis
-sand
-peritonitis
-gastric ulcers

what are GI causes of simple obstructive colic?
-stomach impaction
-small intestinal impaction (ileum)
-ascarid impaction
-eosinophilic enteritis (mural bands)
-large colon impaction
-large colon displacement (right or left dorsal)
-enteroliths
-cecal impaction
-small colon impaction
what are GI causes of strangulating obstructive colic?
-strangulating lipoma of SI or small colon
-SI volvulus
-mesenteric rent
-epiploic foramen entrapment
-gastrosplenic entrapment
-intussusception
-large colon torsion
what are non-GI causes of colic?
1. neurologic: vestibular dz, rabies
2. cardiac dz leading to collapse
3. muscular dz causing tie-up
4. hepatic disease
5. pleuropneumonia
what are causes of chronic/intermittent colic?
-gastric ulcers (mild signs in adult horse)
-enteroliths
-sand colic
-IBD
-abdominal mass
-peritonitis
-intestinal adhesions
-parasitism
what are indications for colic surgery?
1. diagnosis of strangulation
2. intestinal obstruction that fails to respond to medical therapy
3. high level of pain/persistent pain (even when strangulating lesion is not obvious)

how are strangulating lesions diagnosed?
1. ultrasound findings: 2 populations of small intestine, small intestinal dilation, thickening of intestinal wall
2. abdominal fluid (serosanguinous, elevated abdominal lactate compared to peripheral)
3. rectal exam: small intestinal distention
4. suspicion of large colon volvulus
what are indications for referral?
-suspected surgical lesion on patient w/ surgical option
-need for intensive medical therapy (colitis, reflux, severe dehydration, recurrent pain)
-client expectations