Pharmacological Options in Heart Failure 1 & 2
1/21
Earn XP
Description and Tags
M.10, W.2, L.8+9
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
22 Terms
List the 4 different drug classes used for heart failure
Sympathomimetics
Diuretics
Vasodilators
Inodilators
Define Sympathomimetics
drugs that stimulate the sympathetic nervous system, mainly through B1-adrenoreceptors in the heart
Describe the MOA for Sympathomimetics
B1 receptor stimulation activates adenylate cyclase through a G-protein:
B1 receptor activation → ↑ cAMP → ↑Ca2+ → ↑cardiaccontractility
This leads to:
increased intracellular Ca2+
increased force of contraction (positive inotropy)
Increased heart rate (positive chronotropy)
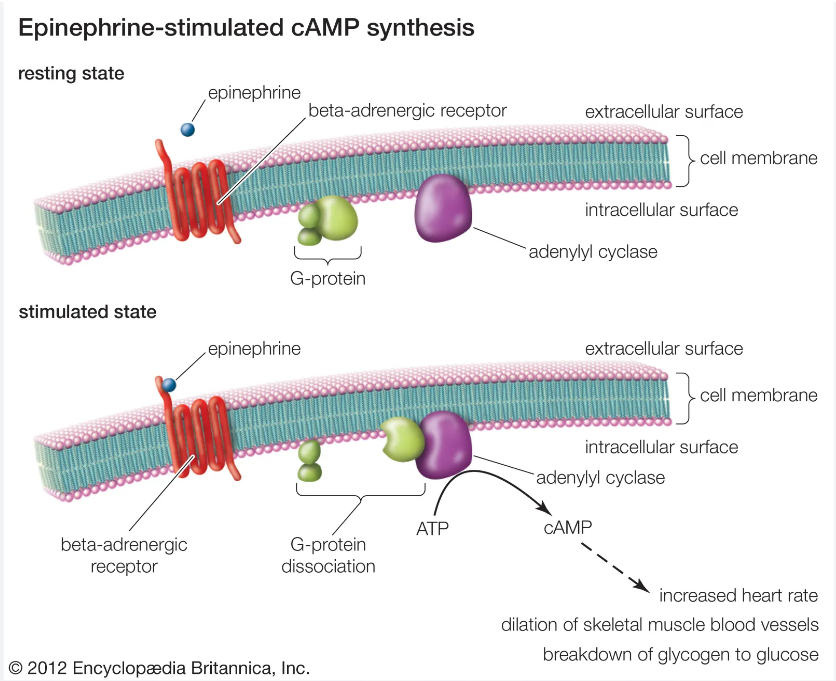
Describe the G-protein-coupled receptor and cAMP pathway and how that leads to increased intracellular Ca2+ for sympathomimetics
Drug or hormone binds to B1-adrenoreceptor on cardiac muscle cells
B1-adrenoreceptors activated by sympathetic neurotransmitters
Adrenaline (epinephrine)
Noradrenaline (norepinephrine)
Binding activates g-protein dissociation
G-protein binds to adenylate cyclase and activates it
adenylate cyclase converts ATP to cAMP
cAMP acts as secondary messenger inside the cell and activates protein kinase A (PKA)
PKA causes calcium channels to open and Ca2+ enters the cardiac cell
Sarcoplasmic reticulum also releases calcium
More Ca2+ = Increase force of contraction
Final result: Increased cardiac contractility
List an example of a synthetic B1-agonist and when it’s used
Dobutamine
used short term in severe acute heart failure with poor systolic function
List limitations and adverse effects of Sympathomimetics
Catecholamines can also stimulate a-receptors causing:
vasoconstriction
tachycardia
arrhythmias
Long-term use may down-regulate B-receptors, reducing effectiveness
What do diuretics do?
Increase:
urine production (diuresis)
sodium excretion (natriuresis)
reduce fluid overload and edema in heart failure
List the 5 types of diuretics
Loop Diuretics
Thiazide Diuretics
Potassium-sparing Diuretics
Other Diuretics:
Osmotic Diuretics
Carbonic Anhydrase Inhibitors
List examples, MOA and adverse effects of Loop Diuretics
Examples
furosemide
torasemide
MOA
Act in the thick ascending limb of the loop of Henle by inhibiting the Na+/K+/2Cl- cotransporter:
Na+/K+/2Cl- transporter inhibition → Increased Na+, K+, Cl- excretion → Increased waterloss
This decreases medullary osmolarity and reduces water reabsorption
Adverse Effects
dehydration
electrolyte loss
pre-renal azotemia
ototoxicity at high doses
List two examples of Potassium-sparing diuretics
Amiloride
Spironolactone
Define Amiloride (type of diuretic, MOA)
weak diuretic
MOA
reduces epithelial Na+ channels in collecting tubule
reduces K+ loss
Define Spironolactone (type of medication, MOA)
competitive aldosterone antagonist
(reduces action of aldosterone)
prevents Na+ and water retention
helps prevent “aldosterone escape”
What is the clinical importance of potassium-sparing diuretics?
combined with loop diuretics to reduce hypokalemia and improve survivial
What do vasodilators do?
Reduce:
preload
afterload
cardiac workload (“unloading the failing heart”)
List the 5 types of Vasodilators
Calcium channel blockers
a1-adrenoreceptor antagonists
Nitrates
ACE Inhibitors
Angiotensin II Receptor Blockers (ARBs)
Describe Calcium Channel Blockers (Classes and MOA)
Classes
Verapamil → mainly cardiac effects
Amlodipine → mainly vascular dilation
Diltiazem → intermediate effects
MOA
Block L-type calcium channels
relaxes blood vessels
decreases heart contractility
slows heart rate
Describe a1-adrenoreceptor antagonists (example, MOA, adverse effects)
Example
Prazosin
MOA
block a1-receptors
causing vasodilation and reduced peripheral resistance
Adverse Effects
hypotension
syncope
Describe Nitrates (example, MOA, adverse effects)
Example
Glyceryl trinitrate
MOA
Donate nitric oxide (NO), producing vasodilation:
NO → Increased cGMP → vascular smooth muscle relaxation
Adverse Effects
hypotension
syncope
Describe ACE Inhibitors (example, MOA + effects, adverse effects)
Example
Enalapril
Benazepril
Ramipril
MOA
Block conversion of angiotensin I to angiotensin II:
ACE inhibition → Decreased Angiotensin II → vasodilation + decreased aldosterone
arteriolar and venous dilation
reduced aldosterone
increased Na+ and water excretion
reduced edema
increased bradykinin-mediated vasodilation
Adverse Effects
hypotension
hyperkalemia
renal impairment