T5 - IE3 - Infectious Diseases I - Kang - Acute Otitis Media (AOM)
1/67
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
68 Terms
Epidemiology: most common diagnosis for which antimicrobial therapy is prescribed in ________ and _________
- infants
- children
50% of the children in the US will experience AOM
AOM
acute otitis media
AOM Epidemiology: highest incidence between ___ and _____ months of age
- 3
- 24 (months of age)
Acute Otitis Media
inflammation of the middle ear with fluid accumulation (effusion) accompanied by signs and symptoms of acute illness
Acute Otitis Media: __________ of the ______ ear with fluid accumulation (effusion) accompanied by signs and symptoms of acute illness
- inflammation
- middle (ear)
Acute Otitis Media: inflammation of the middle ear with ______ ____________ (______) accompanied by signs and symptoms of ______ illness
- fluid accumulation (effusion)
- acute (illness)
Eustachian tube: regulation of ____________ _________ between ______ sides of the tympanic membrane
- (regulation of) atmospheric pressure
- both (sides of the tympanic membrane)
Protection from nasopharyngeal secretions
Ear Anatomy
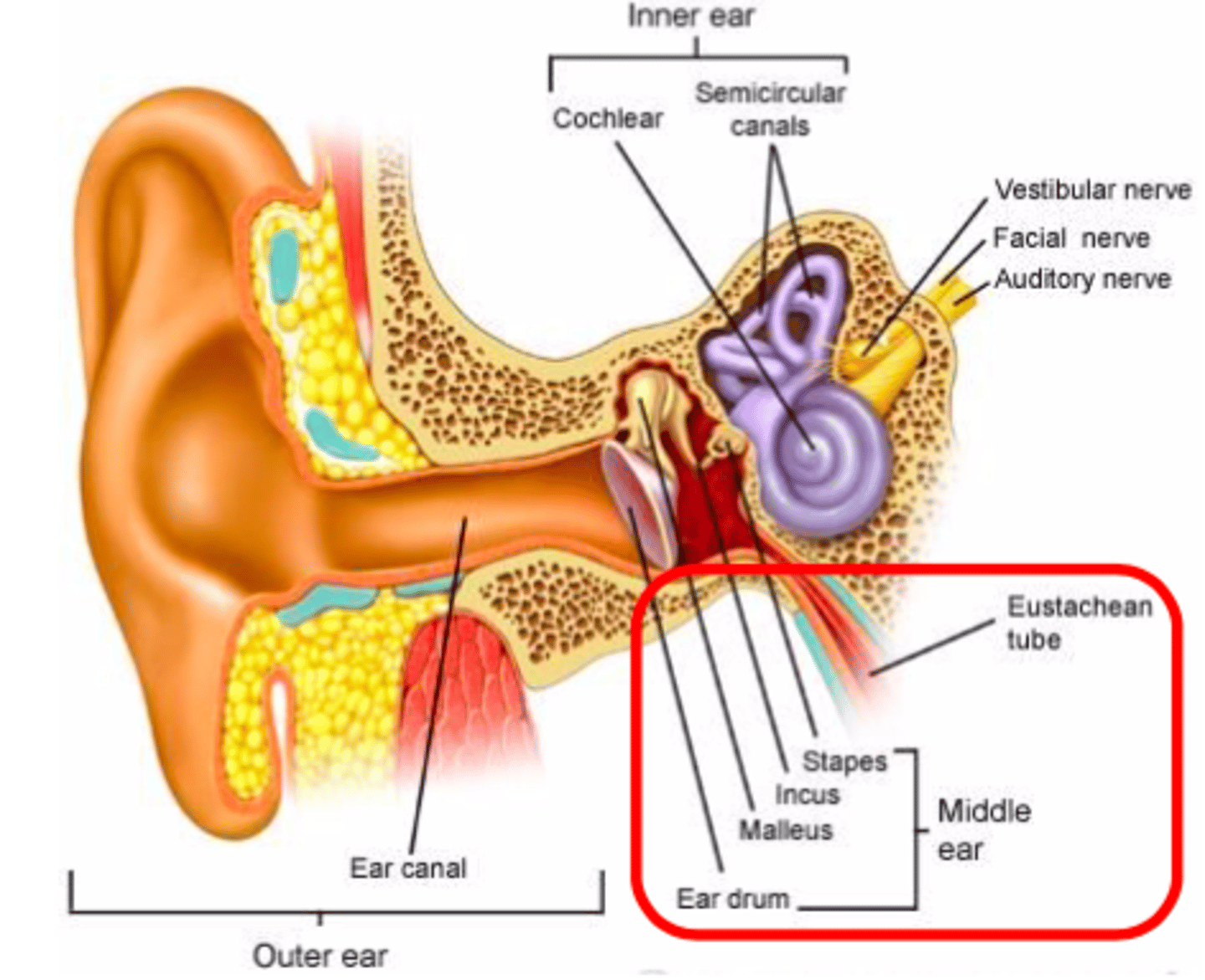
Eustachian tube: _____________ secretions from the middle ear into the nasopharynx
- draining (secretions)
Eustachian tube: draining __________ from the _________ ear into the nasopharyn
- (draining) secretions
- middle (ear)
AOM Pathophysiology Figure
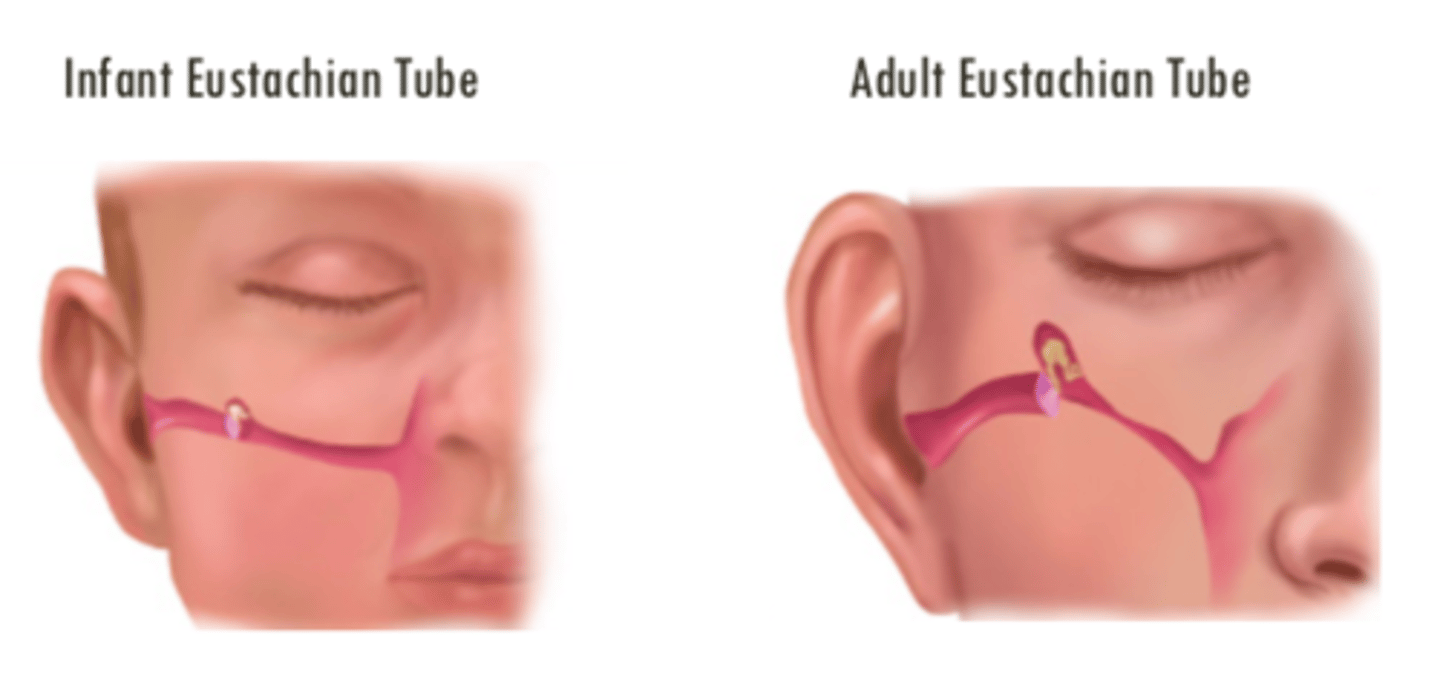
The infant Eustachian tube is much ___________ in comparison to the adults and infants are more susceptible due to lack of _____________ ______
- (much) flatter
- (lack of) immune system
Risk Factors for AOM
age (pediatric)
day care / siblings
no breastfeeding
lower socioeconomic status
exposure to cigarette
winter
anatomic abnormality
- cleft palate
- down syndrome
1st episode when < 6 months
Bacterial Etiology of AOM
streptococcus pneumonia
haemophilus influenzae
moraxella catarrhalis
Viral Etiology of AOM
respiratory syncytial virus (RSV)
rhinovirus
parainfluenza virus
influenza virus
RSV
respiratory syncytial virus
Clinical presentation of AOM - symptoms
otalgia (ear pain)
otorrhea (discharge from the ear)
hearing impairment
fever
non-specifics: irritability, lethargy, anorexia, vomiting
Otalgia
ear pain
Otorrhea
discharge from the ear
Clinical presentation - physical exam (otoscopic exam)
middle ear effusion (MEE)
redness
bulging
opacity
immobility of the tympanic membrane
MEE
middle ear effusion
Pharmacotherapy - general recommendations: treatment considerations, initiate treatment in all __________ AOM cases
- (all) severe (AOM cases)
Severe AOM: Moderate to severe otalgia > 48 hours or fever ≥ 39°C
Severe AOM
moderate to severe otalgia > 48 hours
OR
fever ≥ 39°C
Severe AOM: __________ to ________ _______ > 48 hours
OR fever ≥ 39°C
- moderate
- severe otalgia (> 48 hours)
Severe AOM: moderate to severe otalgia > 48 hours OR fever ≥ ____°C
- (fever ≥) 39(°C)
Severe AOM: moderate to severe otalgia ___ ____ hours
- > 48 (hours)
Mild to moderate AOM
mild otalgia and a temperature of < 39°C
Mild to moderate AOM: _____ otalgia AND a temperature of ___ ______ °C
- mild (otalgia)
- < 39 (°C)
Initiate treatment in < 2 years; age ≥ 2 years reasonable to observe for 48 hour UNLESS bilateral AOM
Mild to moderate AOM - initiating treatment
Initiate treatment in patients <2 years
age ≥ 2 years reasonable to observe for 48 hour UNLESS bilateral AOM
- when antibiotics deferred, AOM resolves spontaneously in majority of patients (SNAP study, WASP)
Clavulanate is a ___-___________ ____________
- β-lactamase inhibitor
Thus, can help in combo with amoxicillin for the treatment of AOM; since gram negative bacterias produce β-lactamase
Gram negative bacteria produce _____-_________
- β-lactamase
So if patient fails amoxicillin for AOM, we can try Augmentin since it has clavulanate to inhibit the β-lactamase enzymes from gram negative bacteria if amoxicillin is not efficacious
We initiate treatment for mild to moderate AOM in patients ___ _____ years of age because these patients have a ______ ___________ immune system
- < 2 (years of age)
- less developed (immune system)
Patient JM, 2.5 year old, presents to the clinic with severe otalgia for the past 3 days and a fever of 38°C
Do we initiate treatment?
Yes
Although JM is 2.5 years old and his fever is only 38°C, he has severe otalgia for the past 3 days which is defined as SEVERE AOM.
Patient TS, 2 year old presents with some mild pain in the ear and discharge with a temperature of 38°C for the past day
Do we initiate treatment?
No
We should wait to observe for 48 hours.
TS is a 2 year old with mild pain and discharge with a temperature of 38°C, defined as mild to moderate acute otitis media. When antibiotics deferred, AOM resolves spontaneously in majority of patients.
Patient BL, 18 months presents to the clinic with some pain in her ear for the past 24 hours and a temperature of 38.6°C
Do we initiate treatment?
Yes
Although BL only has mild to moderate AOM, she is below 2 years old and requires treatment due to the lack of a developed immune system.
Patient TS, 3 year old presents to the clinic with some mild pain and discharge in both ears. He has a measured temperature of 37.4°C
Do we initiate treatment?
Yes
TS may have mild to moderate AOM but it presents as bilateral, we should initiate treatment
General recommendations: duration of treatment
Age < 2 years: 10 days
Age ≥ 2 years: 5-7 days
General recommendations - duration of treatment: age < 2 years
10 days
General recommandations - duration of treatment: age ≥ 2 years
5 - 7 days
Antibiotic therapy: if patient has NO antibiotics in the prior month, NO conjunctivitis, no h/o recurrent AOM, no risk factors
Amoxicillin (AMOXIL) high dose
or
Amoxicillin / clavulanate (AUGMENTIN) high dose
Amoxicillin
AMOXIL
Amoxicillin/Clavulanate
AUGMENTIN
Amoxicillin HIGH DOSE
90 mg / kg / day divided BID or TID
Amoxicillin/clavulanate (HIGH DOSE)
14:1 formulation
90 / 6.4 mg / kg / day
divided BID
If the patient has taken antibiotics in the past 30 days, failed response to Amoxicillin, concurrent conjunctivitis, history of recurrent AOM, risk of antibiotic resistance (day care, not vaccinated, living in area with a high prevalence resistance)
Preferred:
Amoxicillin / Clavulanate (AUGMENTIN) high dose
- 90/6.4 mg/kg/day divided BID
Recurrent AOM is defined as...
≥ 3 AOMs in 6 months or ≥ 4 AOMs in 12 months with at least 1 episode in the past 6 months
Recurrent AOM is defined as: __ ___ AOMs in 6 months or ___ ____ AOMs in 12 months with at least __ episode in the past __ months
- ≥ 3 (AOMs in 6 months)
- ≥ 4 (AOMS in 12 months)
- 1 (episode)
- (past) 6 (months)
Alternative therapies for AOM
Cefdinir (14 mg/kg/day PO divided BID or given daily)
Cefpodoxime proxetil (10 mg/kg/day PO divided BID)
Cefuroxime axetil (30 mg / kg / day PO divided BID)
Ceftriaxone (50 mg / kg IV or IM once daily x 3 days)
Cefdinir dosing for AOM
14 mg / kg / day PO divided BID or QD
Cefpodoxime proxetil
10 mg / kg / day PO divided BID
Cefuroxime axetil
30 mg / kg / day PO divided BID
Ceftriaxone
50 mg / kg IV
or
IM once daily for 3 days
Alternative therapy for AOM: Ceftriaxone is typically used for children with ____________ _______ or who are unable to __________ PO administration
- persistent vomiting
- tolerate (PO administration)
When antibiotics are prescribed for AOM, clinical improvement should be noted within ____-_____ _____
- 48-72 hours
Inadequate response to antibiotic treatment AFTER 48-72 hour of initial antibiotic treatment: IF failed amoxicillin...
may try high-dose Augmentin
If failed Augmentin or oral 3rd generation cephalosporins
Inadequate response to antibiotic treatment AFTER 48-72 hour of initial antibiotic treatment: IF failed amoxicillin and then FAILED Augmentin or oral 3rd generation cephalosporins...
May try Ceftriaxone (50 mg IM or IV for 3 days)
If failed series of antibiotics
- Tympanocentesis
- (Tympanocentesis is not available) clindamycin ± cefdinir, cefixime, or cefuroxime
Inadequate response to antibiotic treatment AFTER 48-72 hour or initial antibiotic treatment:
IF failed amoxicillin... FAILED Augmentin or oral 3rd generation cephalosporins
and FAILED Cetriaxone
May use...
tympanocentesis
If tympanocentesis is not available
clindamycin ± cefdinir, cefixime, or cefuroxime
Recommended Order for AOM
Amoxicillin
-> Augmentin or oral 3rd generation cephalosporin
-> Ceftriaxone
-> tympanocentesis or clindamycin ± cefdinir, cefixime, or cefuroxime
Tympanocentesis
puncture of the tympanic membrane with a needle to aspirate middle ear fluid
Penicillin Allergy: Cefdinir, cefuroxime, cefpodoxime, and ceftriaxone are __________ _______ to be associated with cross-reactivity with penicillin allergy
- highly unlikely
Other choices: clindamycin? macrolides?
Other choices for penicillin allergy patient for AOM
cilndamycin
macrolides
Pain relief options for AOM
acetaminophen PO
- 15 mg/kg/dose up to 4 times daily pen pain; NTE 1000 mg/day
ibuprofen
- 10 mg/kg/dose up to 4 times daily pen pain; NTE 2400 mg/day
Prevention of recurrent otitis media
Insertion of typanostomy tubes
vaccination
modification of risk factors
Prevention of recurrent otitis media - vaccination
pneumococcal conjugate vaccine
influenza vaccine annually
H. influenza vaccine (Hib)
Prevention of recurrent otitis media - modification of risk factors
minimize use of day care if possible
encourage exclusive breastfeeding for at least 6 months
encourage avoidance of tobacco smoke exposure
Prevention of recurrent otitis media - modification of risk factors: _____________ use of day care if possible
- minimize (use of day care)
Prevention of recurrent otitis media - modification of risk factors: encourage exclusive _____________ for at least 6 months
- breastfeeding (for at least 6 months)
Prevention of recurrent otitis media - modification of risk factors: encourage avoidance of _______________ __________ _________
- (avoidance of) tobacco smoke exposure