Ultrasound and Biofeedback
1/63
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
64 Terms
diagnostic/real time ultrasound
views internal structures - ultrasound for babies
therapeutic ultrasound
heating tissue to decrease pain and increase healing
therapeutic ultrasound uses
pain management
trigger point management
tendonitis/bursitis
scars, adhesions
sprain/strains
absorption of medications
wound healing
fracture management
physical properties of US
sound
frequency
intensity
mode
BNR
treatment area
refraction
reflection
sound
high frequency sound waves
mechanical energy converted to thermal energy
US > 20,000 Hz (human hearing limit) → not audible
ultrasound without gel
= useless
need the gel to let the functions of it go into the tissue
how does it work
transducer head
piezoelectric crystal
high frequency, alternating electrical current
crystal expands and contracts, producing sound waves
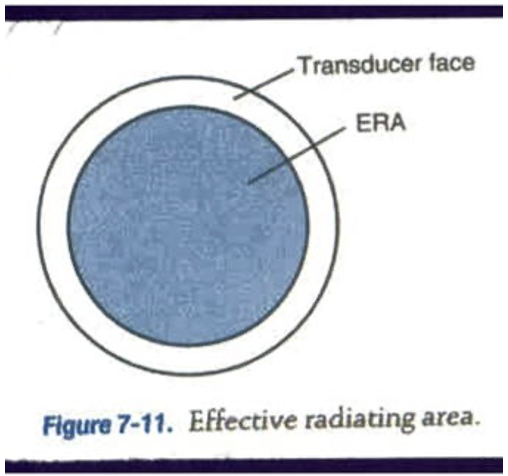
effective radiating area (ERA)
area that radiates the US
ERA < the sound head
increase the ERA will heat tissue faster
treatment considerations of ERA
size of treatment area
movement of transducer head → should never be held in the same position because it can lead to burns
frequency
= waves/sec
alternating compression-expansion cycles per second (MHz)
depth of US penetration inversely related to frequency
1 MHz vs 3 MHz
1 MHz - frequency
penetrates up to 3-5 cm
deeper structures, i.e. joint capsules, muscle, fascia
3 MHz
penetrates 1-3 cm
superficial structures, i.e. superficial tendons, lateral epicondylitis, ankle tendons/ligaments, etc
Intensity (W/cm2)
wave amplitude
rate at which energy is delivered
spatial average intensity (average over the ERA)
no guidelines for therapeutic intensity
1.5 W/cm2 = common setting
best practice for intensity
use the lowest intensity possible to achieve the desired therapeutic effect - most set at 1.5 W/cm2
mode
duty cycle = 20%
pulse duration/pulse period x 100%
beam nonuniformity ratio (BNR)
BNR = peak intensity/average intensity
usually preset, but good to understand
hot spots of BNR
higher the BNR
greater risk for burning and increasing discomfort
treatment implications
low BNR = more uniform
less hot spots
costs more $
keep it moving
prevents burning
treatment area
2-4 x ERA to get significant heating
treatment implications: treating large muscles or areas is ineffective
you can still do a big muscle like a calf, but you’d have to split it into sections which takes a lot of time
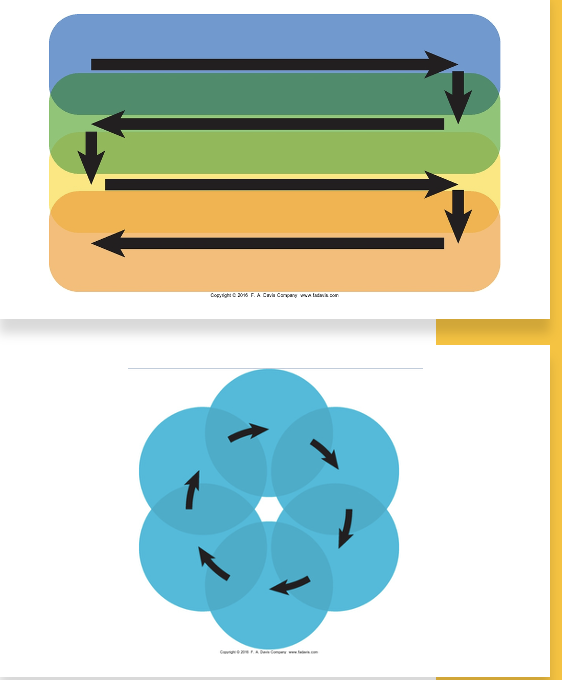
moving the sound head
overlap by ½ the ERA
remain perpendicular and in contact with skin
reflection
a lot of US is reflected, and not absorbed into skin
coupling agent/medium helps to transmit the waves into skin rather than being reflected
aqueous gel
underwater technique for wounds/irregular surfaces
1 cm above skin
gel bad
don’t use creams or ointments
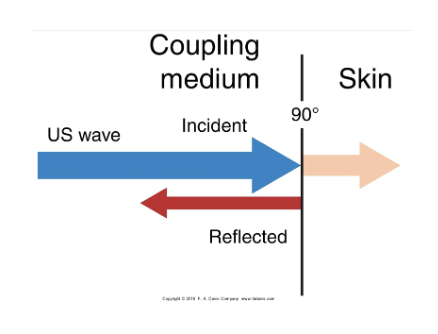
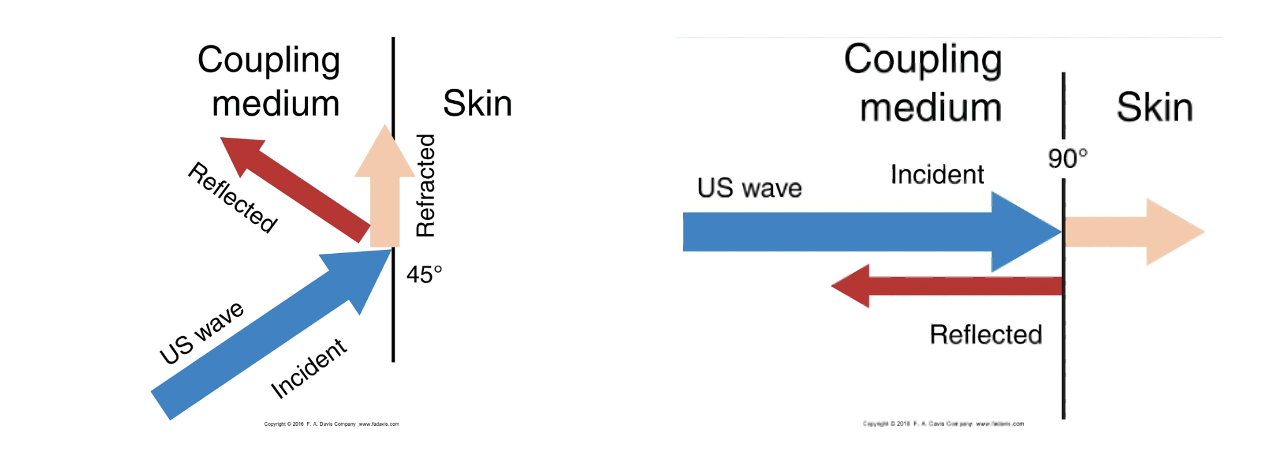
refraction
if we don’t have a coupling medium, waves are refracted and don’t go into skin, vs if you do have a coupling medium, skin absorbs waves
sound head
perpendicular to the skin, not at an angle
absorption of US waves
machine should not be turned on until it’s ready to go → prepped with gel and in position
treatment duration is dependent on:
treatment area size
treatment depth
US settings (intensity, frequency, mode)
specific condition treated
treatment duration: 1 MHz
1 MHz US (1.5 W/cm2, 2 x ERA) → 11 min to warm up skeletal muscle 3.5° C
**deeper tissue
treatment duration: 3MHz
3 MHz US (1 W/cm2, 2 x ERA) → 6 min to warm up superficial muscle 5.3° C
**superficial tissue
tissue cooling rate
tissue cools rapidly after US treatment
treatment implications: 4-5 minute window to stretch
skeletal muscle = 2 minute window
patellar tendon = 2-5 min window
achilles tenon = immediately or within 4 mins
variation and variability of US units
no 2 machines are the same
adjust treatment protocols based on unit and applicator
variation and variability of tissue response
more heating in more dense tissue
dense tissues
ligaments, tendons, bone
greater and faster rise in temp
less dense tissue
muscle, blood, skin
treatment parameters of dense tissues
decrease duration or intensity, increase area, growth plates (would be bad to US growth plates because it could have an impact on their growth)
variation and variability of pt. response
responders: good
non-responders: doesn’t feel warming
over-responders: be cautious to not overheat
be cautious and try to slow increase in intensity, few sessions
thermal US
continuous US (100% duty cyce)
*always pick this!
non-thermal US
pulsed US (<100% duty cycle)
*don’t pick this
thermal effects of US
tissue temperature elevation
≤ 6 cm depending on frequency
increased tissue temp dependent upon: intensity, frequency, duration
results in increased blood flow, pain threshold, and elasticity
non-thermal effects of US: cavitation
formation, growth, and pulsation of gas bubbles
impacts cell membrane permeability
controversial
*prob won’t see or use this
non-thermal effects of US: acoustical streaming
forward movement of fluid
by US waves
relies on cavitation
controversial
*prob won’t see or use this
Us documentation should include…
duty cycle
frequency
intensity
duration
ERA
treatment area
coupling agent
client position
client response
why is it being utilized
contraindications to US
pregnancy - over low back or abdomen
CA - over known/suspected malignancy
over active epiphyseal bone growth
TB infection
hemorrhagic conditions
impaired circulation
popular consensus of contraindications to US
over eyes, reproductive organs, anterior neck
application over pacemakers or any electronic device
DVT or thrombophlebitis
myositis ossificans (formation of bone inside muscle tissue after a traumatic injury)
precautions to therapeutic US
over plastic or cemented implants
over spinal cord or regenerating nerves
impaired sensation, cognition, communication
acute injury
areas of infection
US for myofascial pain/trigger points
strong evidence to treat pain: continuous US
conflicting evidence for increased pain threshold
unsubstantiated effect on cervical range of motion (ROM)
recommendations for pain tx: US for myofascial pain/trigger points
1 or 3 MHz, continous at 1.5 W/cm2 for 10 min
4-5x/week for 2-3 weeks
US for back pain
strong evidence for continuous US
exercise and US significantly improved function, lumbar ROM, endurance
recommendations for pain tx: US for back pain
1 MHz, continuous at 1-2 W/cm2 for 10 mins
3x/week for 4 weeks
US for shoulder pain
thermal: insufficient evidence for nonspecific conditions
non-thermal: no evidence for nonspecific shoulder pain and dysfunction
best evidence: continuous US might be beneficial as adjunct to stretching and exercise
US for inflammatory conditions
lateral epicondylitis
little and conflicting evidence with thermal or nonthermal
manage pain and function
US for carpal tunnel syndrome: thermal
strong substantiated evidence that reduces pain and improves functional outcomes
Continuous US, 1 or 3 MHz, at 0.5-1.5 W/cm2 for 5-10 min
5x/week for 4 weeks
US for carpal tunnel syndrome: pulsed US
minimal evidence, some positive studies
Pulsed (20%) US, 1 MHz, at 1 W/cm2 for 15 min
5x/week for 3 weeks
US for calcific tendonitis
thermal: moderate evidence for pain and dysfunction
pulsed US: minimal evidence, but positive
parameters widely varied
trying to break up calcium deposits
recommendations for pain tx and increase functions: calcific tendonitis
Continuous US, 1 or 3 MHz, at 1-2 W/cm2 for 10 min
3x/week for 4-8 weeks
US for bursitis
questionable and insufficient evidence → for pain, improved function, or ROM
US for arthritis
thermal: positive evidence for pain reduction, minimal evidence for increased ROM and/or functional improvement
pulsed: min, studies, no improvements in pain, ROM, or function when added to exercise
recommendations for pain tx and increase functions: arthritis
Continuous US, 1 MHz, at 1-2 W/cm2 for 5-10 min
3x/week for 2-3 weeks
US for soft tissue healing: wound healing
continuous US: conflicting and insufficient evidence for wound healing
pulsed US: insufficient but positive
US for soft tissue healing: remodeling scar
insufficient evidence for US
US for soft tissue healing: tissue extensibility
evidence from varied applications (knee, ankle, shoulder)
conflicting outcomes
not recommended but very poor studies
insufficient power or too large tx areas
US for soft tissue healing: tissue swelling/ankle edema
insufficient evidence
other uses for therapeutic US: phonophoresis
topical agent on skin or in US gel
conflicting/insufficient evidence
enhance absorption of topical agent - not likely
thermal effect may enhance diffusion of topical agents into the skin
not recommended for pain or inflammation
low-intensity pulsed US (LIPUS)
pulsed
med. frequency (1.5 MHz)
low intensity (0.3 W/cm2)
stationary application
strong evidence and good justification
fresh and delayed bone fractures
stimulate osteogenesis
**only time you should really used pulsed US
strong substantiated evidence for continuous US
pain for myofascial pain syndrome and trigger points
pain and dysfunction with painful low back conditions
pain and dysfunction of carpal tunnel syndrome
pain associated with arthritis
moderate substantiated evidence for continuous US
dysnfunction with nonspecific shoulder conditions
calcific tendonitis
bursitis
wound debridement
pulsed US insufficient or conflicting evidence
need better studies
except for LIPUS for slow healing fractures
definition of biofeedback
utilization of alternative sensory input to drive desired motor output
teaching/learning technique reliant on immediate feedback
decreasing ineffective movement/increasing desired outcome
goal of biofeedback: motor awareness
improves awareness of motor or kinesthetic performance or physiologic response using
EMG → visual or auditory representation of mm activation
PT can adjust sensitivity of reading
high sensitivity when goal is relaxation
treatment time = 10-15 mins
low sensitivity when goal is mm re-education
treatment time 5-10 min per mm groups
isometric contractions held 6-10 sec at 2/3 max intensity
goal of biofeedback: improved postural awareness
visual awareness of midline with positive or negative reinforcement
weight acceptance, weight shift
different from visual cues alone (mirror)