Physio. Ch.16 Pulmonary Ventilation
1/43
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
44 Terms
Respiration
The process of gas exchange in the body
Subdivided
- Internal respiration
- External respiration
Internal respiration
Also known as cellular respiration
Use of O2 in ATP production
- Produces CO2 as byproduct
External respiration
Exchange of oxygen and carbon dioxide between the atmosphere and body tissues
Requires respiratory & circulatory systems
Multi-step process
- Step 1: Pulmonary ventilation
- Step 2: Exchanging of O2 and CO2 between air spaces of the lung and blood diffusion
- Step 3: Transport of O2 and CO2 through pulmonary circulation by the blood
- Step 4: Exchange of O2 and CO2 between blood and tissues
Pulmonary ventilation
Movement of air into the lungs and out of the lungs by bulk flow
Conducting zone
Division of the respiratory system
Upper part of the respiratory tract that conducts air to lungs
- Humidifies and brings air to body temperature
Referred to as “dead space”
- Named this because no conduction is done here
Respiratory zone
Division of the respiratory system
Site of gas exchange within the lungs
Made of simple squamous epithelium cells
Structures
- Type 1 alveolar cells
- Type 2 alveolar cells
- Alveolar macrophages
Pleural sac
A membrane surrounding each lung
Subdivided
- Parietal pleura
- Visceral pleura
Parietal pleura
Lines the thoracic cavity
Attaches to the chest wall
Visceral pleura
Outer surface of the lungs
Intrapleural space
Thin space between the visceral and parietal pleura
Filled with intrapleural fluid
Bulk flow
The mass movement of air into and out of cells
Powered by pressure gradients between alveoli and outside air
- The pressure gradient is produced by muscular pumps
Rate of bulk flow: How fast air flows in to out of the lungs
- Calculate: Flow = (Patm - Palv) / R
Airway resistance
Mechanism used to control pressure gradients
Controlled by diameter of respiratory airways
- Inversely related
Atmospheric pressure (Patm)
Pressure of the outside air
760 mm Hg (1 atm) at sea level
- Decreased as altitude increases
All other lung pressures are expressed relative to atmospheric pressure
Intra-alveolar/intrapulmonary pressure (Palv)
Pressure within the alveoli relative to the atmosphere
During inspiration value is -3 (less than atmospheric so air will flow to it)
During rest value is 0 (same as the atmospheric so air won’t move either way)
During exhalation value is 3 (more than atmospheric so air will away from it)
The difference between intra-alveolar pressure and atmospheric pressure (Palv and Patm) is the pressure gradient that drives ventilation
Intrapleural pressure (Pip)
Pressure of the fluid in the pleural sac
Caused by the opposite directions of pull from the chest wall and lung wall
Always negative
- If not the lung will collapse
At rest is -4mmHg
During inspiration is -6mmHg
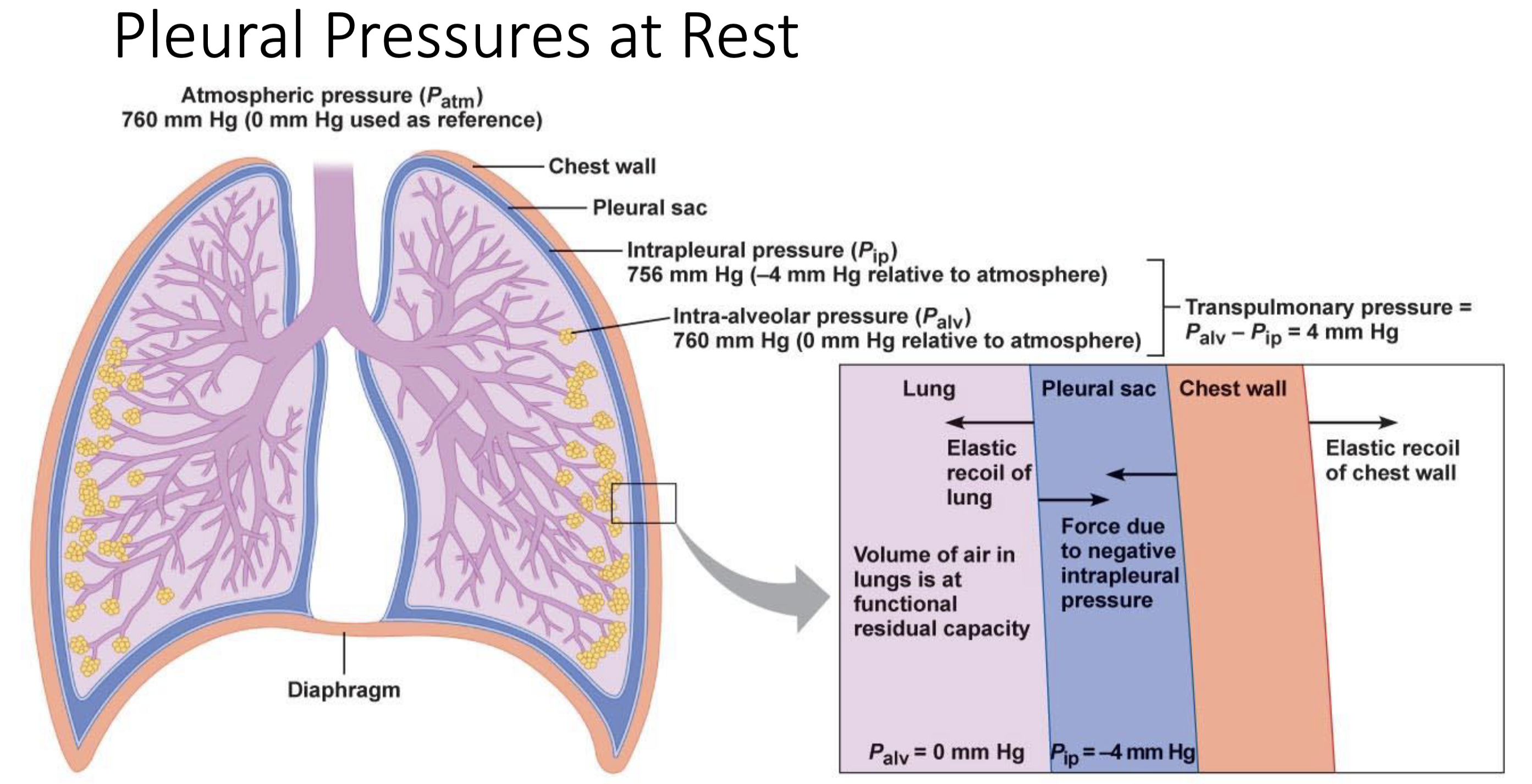
Transpulmonary pressure
Pressure difference between the intra- alveolar pressure and intrapleural pressure
- Calculation: Palv – Pip
Increase in transpulmonary pressure → increases distending pressure across lungs → Causes lungs (alveoli) to expand
At rest 4mmHg
Functional residual capacity (FRC)
Volume of air in the lungs between breaths
Pneumothorax
Air enters the pleural space, raising intrapleural pressure
Without negative intrapleural pressure, lung collapses due to its elastic recoil
Subdivided
- Spontaneous
- Tension
Typically only happens in one lung at a time
- Promotes survivability because the body still has one lung to function
Spontaneous pneumothorax
Type of pneumothorax
Air leaks due to damage from inside
- Broken rib
- lung disorders: COPD, cystic fibrosis, or rupture of a lung blister)
Tension
Type of pneumothorax
Caused by trauma/open chest wound
Boyle’s Law
Inverse relationship between pressure and volume
Inspiration: Increased volume, decreased intra-alveolar pressure → Air flows in
Expiration: Decreased volume, increased intra-alveolar pressure → Air flows out
Mechanics of breathing
The muscles of respiration change the volume of the lungs → create pressure gradients → drives air flow into and out of lungs
Respiratory Muscles
Inspiratory muscles: diaphragm + external intercostals
- Often active
Expiratory muscles: internal intercostals + abdominal muscles
- Often passive
Alveoli
Changes in alveoli volume are produced by changes in the volume of the thoracic cavity
Process of Inspiration
Stage 1: Neural stimulation of inspiratory muscles causing Diaphragm contraction (flattens & moves downward) and External intercostals contraction (ribs pulled up & out)
Stage 2: Thoracic cavity volume increases & parietal pleural pulls on visceral pleura
Stage 3: Intrapleural pressure decreases, which increases transpulmonary pressure
Stage 4: Greater distending force across the lungs causes alveoli to expand with the chest wall → Decreases the intra-alveolar pressure to below atmospheric pressure
Stage 5: Air flows into alveoli due to pressure gradient
Quiet breathing
Passive process with no muscle contraction
Step 1: Relaxation of inspiratory muscles → recoil of chest
wall and lungs to resting positions
Step 2: Visceral pleura pulls on parietal pleura
Step 3: Volume of the thoracic cavity decreases
Step 4: Alveolar pressure rises above atmospheric pressure
Step 5: Air flow out due to pressure gradient
Active expiration
Contraction of expiratory muscles causes a greater pressure gradient
Lung Compliance
Change in lung volume that results from a given change in transpulmonary pressure
- Very high compliance
Dependent on
- Elasticity of the lungs
- Surface tension of the fluid lining the alveoli
Elasticity
Factor that affects lung compliance
Surface Tension
Factor that affects lung compliance
Resistance to distension created by the thin film of water that lines the alveoli
Greater tension means less compliance
Pulmonary surfactant: Decreases alveolar surface tension by interfering with the hydrogen bonding between water molecules
Pulmonary surfactant
Decreases alveolar surface tension by interfering with the hydrogen bonding between water molecules
Airway Resistance
Resistance of the entire airway system in the respiratory tract
Determined by differences in the diameter of different individual airways
Larger resistance requires larger pressure gradient overcome
- Low resistance under normal conditions
Effected by
- Elasticity, mucus secretion, and smooth muscle activity in the bronchioles
Bronchodilation
Dilation of the bronchioles
Caused by sympathetic stimulation
- Epinephrine is released in response to high CO2 levels
Epinephrine binds to B2
Norepinephrine binds to B2
Bronchoconstriction
Constriction of the bronchial
Triggered by parasympathetic stimulation and histamine releases
- Parasympathetic: ACh binds to M3
- Intrinsic: histamine released
Respiratory Distress Syndrome (RDS)
Pathophysiology when surfactant production is low
Causes septic shock in adults
Causes alveolar collapse in babies
Surfactant
Hydrophobic protein and phospholipids that reduces surface tension
Prevents collapse and allows a residual volume of air to remain in lungs
Production begins in week 24 - 28 of pregnancy
Asthma
Pathophysiology
Increased airway resistance, spastic contractions of bronchiole smooth muscle and increased mucus secretion and inflammation of bronchiole walls
Chronic obstructive pulmonary disease (COPD)
Chronic increases in airway resistance
Subdivided
- Emphysema
- Chronic bronchitis
Emphysema
Type of COPD
Destruction of airway walls & elastic CT
Chronic bronchitis
Type of COPD
Inflammation and thickening of airway lining, high mucus production, destruction of normal tissue & fibrosis