Ch 9 + 11: The Body Senses & Movement
1/31
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
32 Terms
Body Sense: Somatosensory Systems
→ sent to somatosensory cortex (post central gyrus)
Proprioception = movement, action & location (awareness of body)
Skin senses = conditions a body surface (touch)
Vestibular system = body position & movement (balance & position)
Interoceptive system = states of internal organs
Procrioception
= informs us abt position & movement of our limbs & body
maintaining posture + moving limbs (ex. used to sit & stand)
grasping & locating objects (ex. grabbing water bottle w/o looking)
→ how we know our body position w our eyes closed
if damaged:
floppy ragdoll movements
rely on vision for movement (ex. cant move w eyes closed)
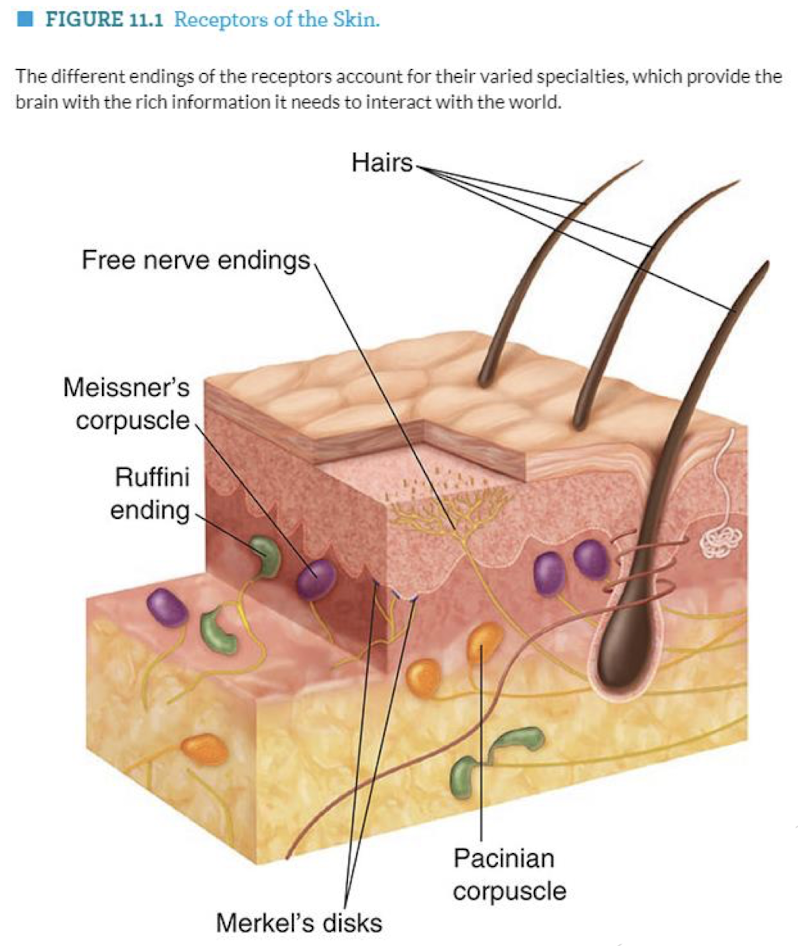
Skin Senses
= touch, temp, texture & pain
distinct with their own receptors & pathways to brain via spinal cord
we have more skin receptors (higher density) on areas of skin used to detect more
Types of Receptors
Free nerve endings = detect temp & pain
→ at the ends of neuronal dendrites
Encapsulated receptors = detect touch & texture
→ enclosed in a membrane
Types of Encapsulated receptors: 4 (work in pairs)
meissner’s corpuscles = brief burst of impulses
merkels disks = sustained response
→ detect texture + fine detail
→ located near surface of skin
pacinian corpuscles = fire once @ beginning
Ruffini endings = continues firing
→ detect skin stretching (pressure) + perception of grasped objects shape
→ located deeper in skin
Types of Free nerve endings:
Temperature receptors = detect temp
TRPs (family of protein ion channels) : each open @ diff temp
Pain receptors: 3 distinct pain types
thermal = TRPs for extreme temps
chemical = TRPS for extreme spicy pain (why u perceive spice as hot & mint as cool)
mechanical = detects painful impact/pressure on skin
Vestibular Sense
= to maintain balance + gives info abt head position & movement
located in ear
mech
liquid in canals bends hair cells → activates neurons
ONLY bend in one direction, THUS only detect one-way movement → why u get dizzy
shift in liquid can make signals in both directions
inside saccule: hair cells feel movement of otoliths
if an otolith enter canals → get vertigo
cochlear & vestibular nerve → combine to form cranial nerve
note: the trickle & saccule are useful when standing still
ex. can detect direction of movement while sitting on a train
note: alcohol thins liquid in canals → faster bending

Somatosensory cortex & posterior parietal cortex
dermatome = segment of the body served by a SIGNLE spinal nerve
process
body senss info enters spinal cord (via spinal nerves) or brain (via cranial nerves)
info crosses over the midline in medulla → thalamus
—> now L body controlled by R brain
thalamus send info to somatosensory cortex (projection area for body sense neurons, located in parietal lobe)
Somatosensory cortex: Somatotopic map
Somatotopic map = represents the body in the somatosensory cortex
adjacent body parts are represented in adjacent parts of the cortex
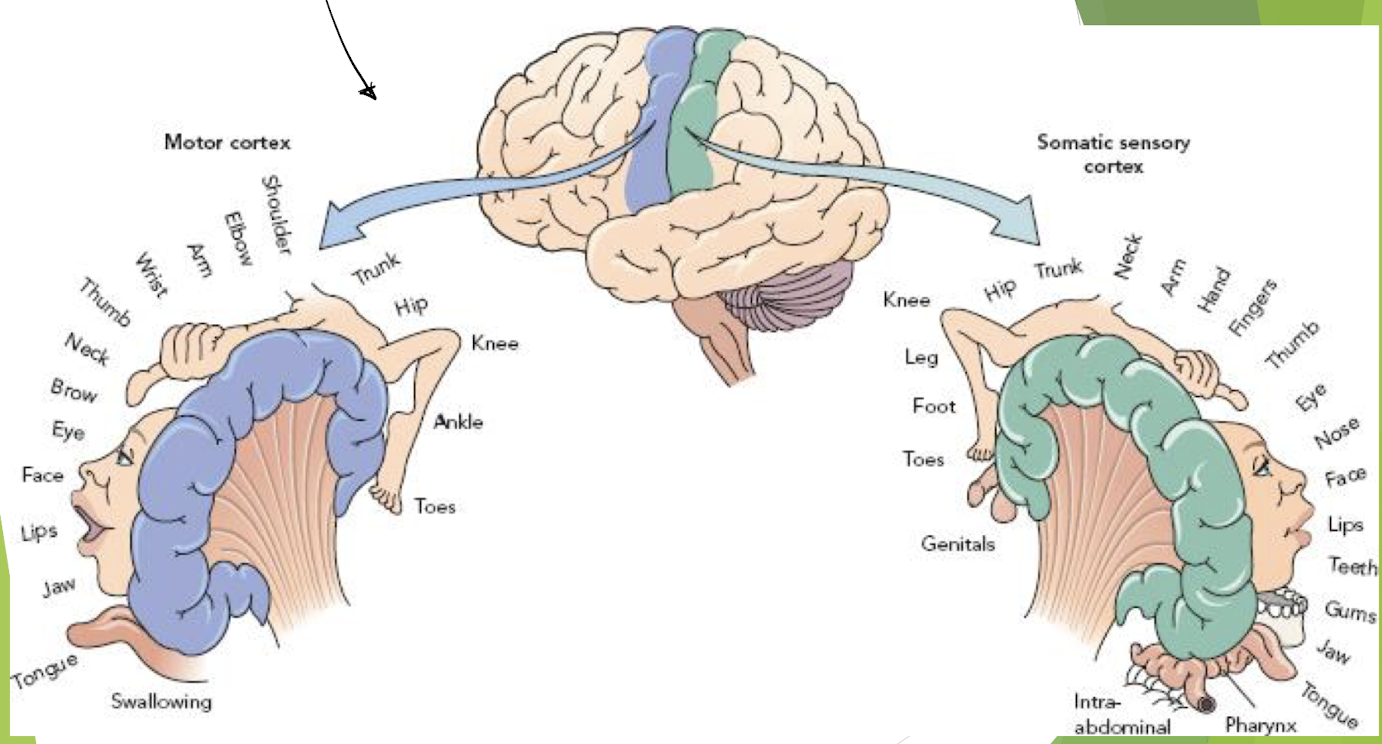
Somatosensory cortex: Primary Somatosensory cortex
= 4 areas that play a role in processing sensory info from body
each area has a somatotopic map
process
info → thalamus → 2 subareas ( info from app side of body & from same smaller side)
those subareas extract some info → pass to the 2 areas
those process into → pass to secondary somatosensory cortex
path: primary → 2 sub areas (extract) → 2 sub areas (process) → secondary
Somatosensory cortex: Secondary Somatosensory cortex
= integrates info from BOTH sides of the body (NO separation by sides)
process
neurons here are responsive to stimuli with an acquired meaning (ex. touching something)
sends connections to hippocampus (in temporal lobe)
hippocampus: uses info to determine what the sense is
ex. what is the identity of what ur touching
Posterior Parietal Cortex
= association area that joins the body senses + vision + audition
→ integrates body with world - by determine body’s orientation in space
→ subareas repsond to diff senses (not just perceptual)
neurons fire before & after movement → send info to prefrontal cortex
Body Integrity Identity Disorder (apotemnophilia)
= NO brain damage or disorder, but are convinced their limb isn’t theirs
when limb is touched → NO response in superior parietal area
HOWEVER
skin conductance response to that limbs stimulation is 2x → suggests intense emotion abt that limb
ex. when nervous, the disordered hand sweats 2x more than the normal hand
Out-of-Body Experience
= hallucinates seeing their body from another location
may be caused by something affecting the parietal-temporal junction (electrical stim., TBI, epilepsy)
→ seems to be improper firing @this junction
note: more common in uni students - possibly bc of stress
Detecting Pain
begins when free nerve endings are stimulated
goes thru a diff. pathway thru the spinal cord than other skin senses
pain enters spinal cord → cross to other side of the body ] other skin senses cross at the medulla
THUS, we can feel pain but not pressure (touch) is a leg if an injury prevents crossing of touch
Inflammatory soup = signalling molecules released when in pain (histamine, proteins, lipids, neurotransmitters, cytokines)
triggers healing & longterm pain (ex. swelling, redness, pain)
→ glutamate (excitatory neurotransmitter) is released in spinal cord for mild pain, THEN substance P for intense pain
Substance P = hormone that increases pain sensitivity → now have lower pain threshold
2 Pain Pathways
Fast: registers localized pain → sends to somatosensory cortex via A-delta fibres (myelinated)
→ to help locate injury
Slow: sends longer-lasting, aching or burning pain to thalamus via C-fibres
→ a reminder of pain
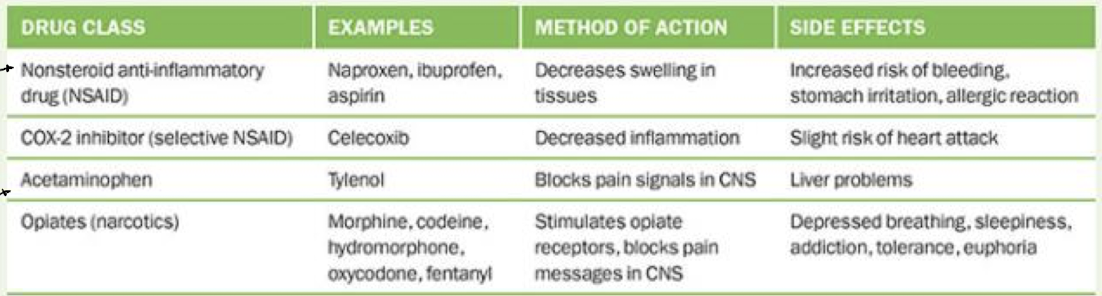
Treating Pain
opioids : block inflammatory soup
Nsaids : prevents creation of further pain ( lowers inflammatory soup)
anesthetics
acetaminophen : decrease pain signal, but DOESNT lower inflammatory soup
internal mech of pain relief
endorphins : act as neurotransmitters & hormones → act @ opiate receptors
→ ONLY work with highly specific conditions:
inescapable pain
during high arousal events (exercise, sex, mom saving baby)
naloxone = opioid antagonist → blocks pain relief from opioids & endorphins
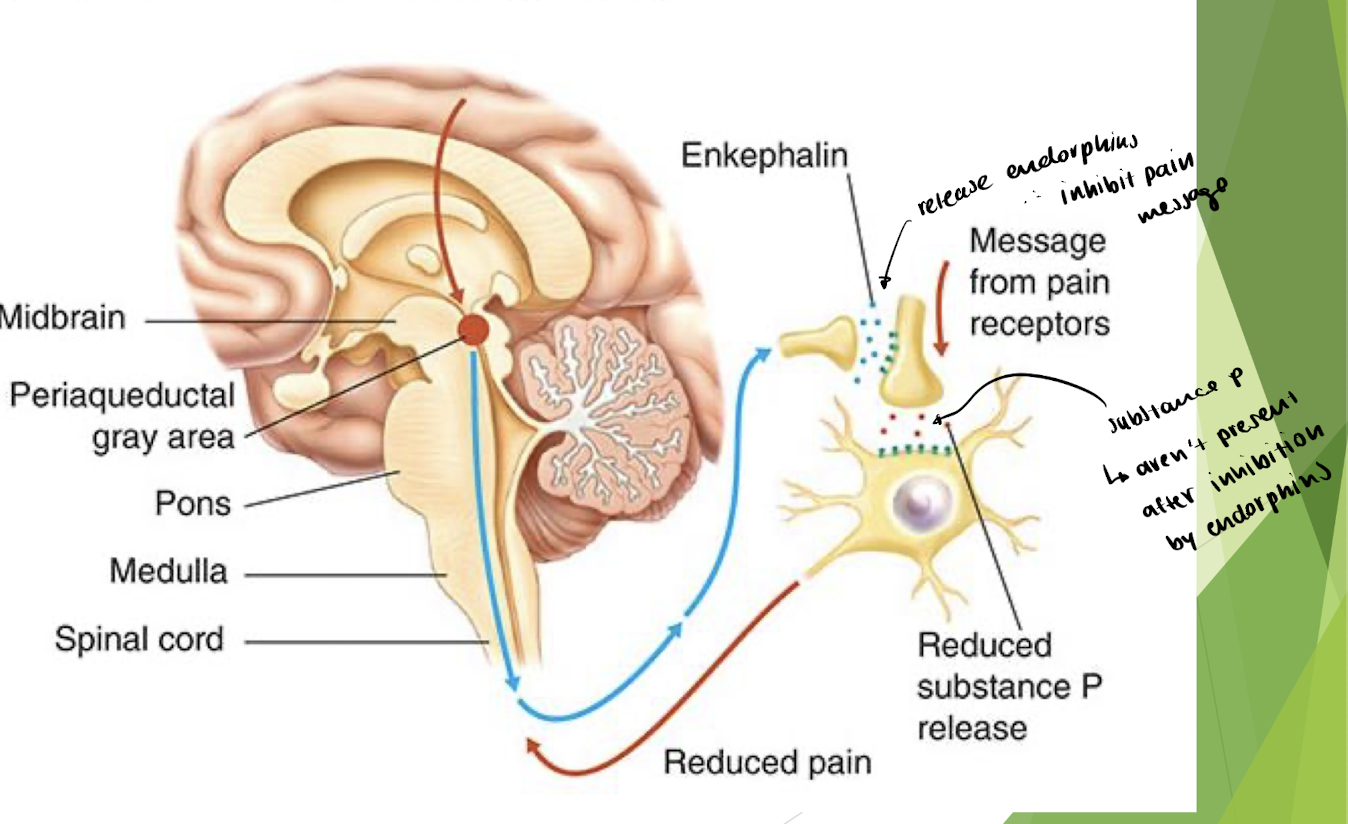
Descending Pain Inhibition Circuit: Gate Control Theory
Gate control theory = pressure signals sent to the brain trigger an inhibitory message that’s sent to the spinal cord → closes a neural pain gate
can still sense pain, but DONT perceive it
explains how endorphins work by inhibiting substance P (pain)
gate: Periaqueductal gray (PAG) = brain stem structure with endorphin synapses + where opioids act + where the inhibitory message is sent
→ endorphins are released here → inhibits release of substance P → closed pain gate
notes:
women have less receptors @ PAG → less pain relief from opioids
there are multiple neural origins for activating the endorphin circuit
PAG has cannabinoid receptors → weed has pain relief
Extremes of Pain
Congenital analgesia = insensitivity to pain, BUT can still feel some pain
linked to mutations in genes & elevated endorphin levels in spinal fluid (constantly blocking pain)
a group of disorders
possible reasons: no pain receptors, no inflammatory soup, no pain pathway
Chronic pain = pain lasting after healing
strongly correlated with depression
associated with certain genes
mild pain Is just as likely to become chronic as severe pain !!
ex. chronic back pain:
the strength of connectivity b/w nucleus accumbens & frontal cortex predicts this
ppl reward driven : more likely to develop chronic back pain after a surgery
→ NS changes functionally & structurally DURING chronic pain:
more sensitive pain pathways, easier APs bc of new connections b/w peripheral neurons in spinal cord, lower # of neurons releasing endorphins
→ brain changes occur DUE to chronic pain:
more responsive brain stem pathways
higher slow pain (prefrontal cortex, anterior cingulate cortex & insula activation)
more of the somatosensory cortex is devoted to pain
longer pain = more grey matter lost
Phantom pain = pain in a missing limb
→ due to random firing of cortical areas still devoted to that limb
→ may be due to foreign neruons intruding on the somatosensory area of that limb - another body part trying to use those neurons
anaesthetics DONT work - bc theres no signal or inflammatory soup to lower
usually decreases over time
Movement: Muscles
skeletal muscle = move body + CAN fatigue if overused (striated muscle)
used in voluntary movement
muscle tissue = many cells (muscle fibres)
Muscle cells : controlled by motor neurons that synapse w a muscle cell at the neuromuscular junction
→ use ACh (excites mysoin) to cause contraction
a single motor neuron can control multiple muscle cells
the fewer muscle fibres a motor neurons controls → more precise movements
ex. fingers = small ratio (1 neuron : 1 muscle cell)
ex. bicep = large ratio (1 neuron : 100 muscle cells)
muscle fibres contain: mysoin (actiavted by ACh) + actin filaments
Movement: Antagonistic Muscles
= muscle pairs that produce opposing movements at a joint
result: smooth movements, precision in stopping & minimal tremor → less fatigue
ex. biceps decrease arm angle & triceps increase arm angle
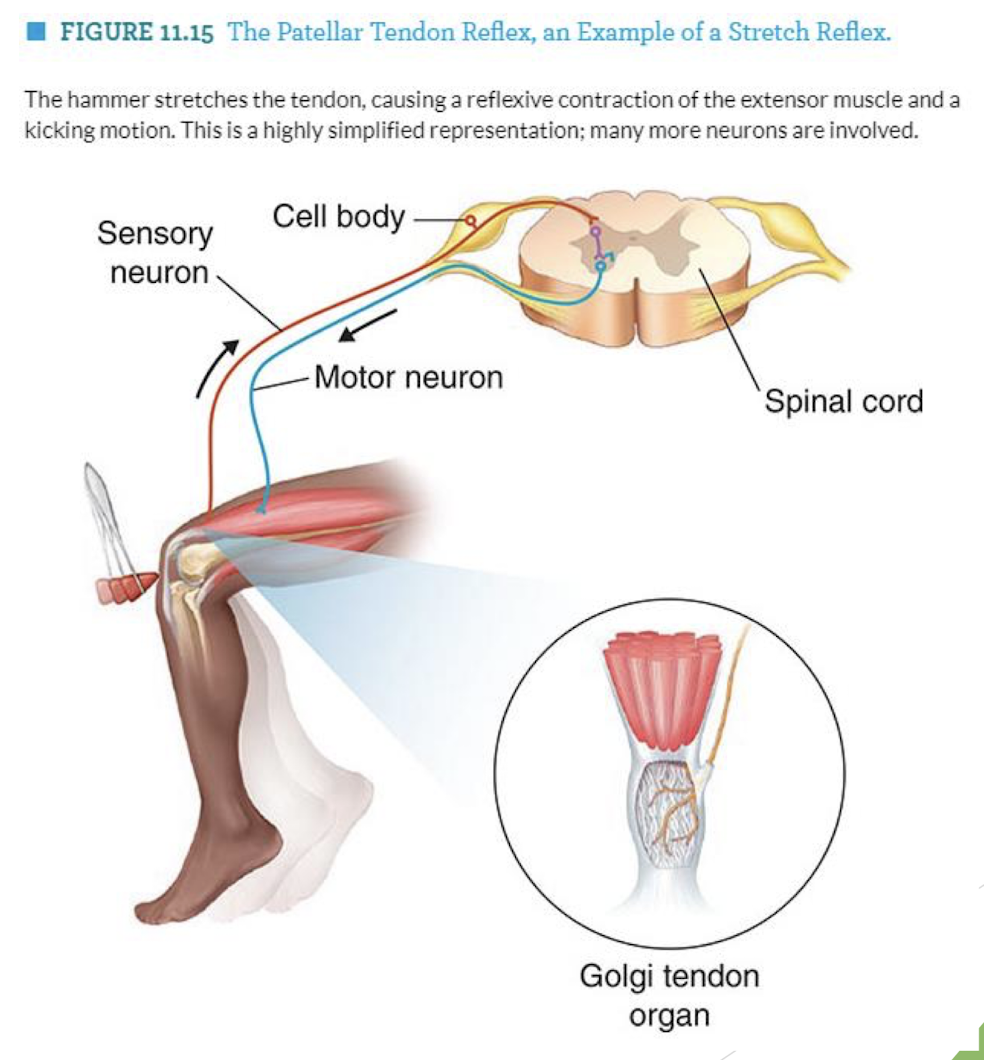
→ controlled by spinal reflexes
Spinal Reflexes = ONLY use the spinal cord for movement (no brain)
triggered by:
→ muscle spindles = stretch receptors in muscles
→ Golgi tendon organs = tension receptors in muscles
-trigger spinal reflexes → inhibit over-contraction of muscles → allowing dynamic adjustment to increased external load
Movement: Central Pattern Generators
CPGs = neuronal networks that produce rhythmic pattern of motor activity until told to stop
brain ISNT involved
in the spinal cord/muscles
ex. walking, swimming, flying, breathing
ex. those with spinal injuries can still perform elicited stepping movements
Brain & Movement
using : hierarchical orgnaization of the forebrain, brain stem & spinal cord
via: motor cortex
components of motor cortex
primary motor cortex (precentral gyrus)
2 major secondary motor areas
supplementary motor area
premotor cortex
→ spinal cord doesn’t start VOLUNTARY movement until told by brain
→ movement is still influenced by rest of brain, not just the motor cortex
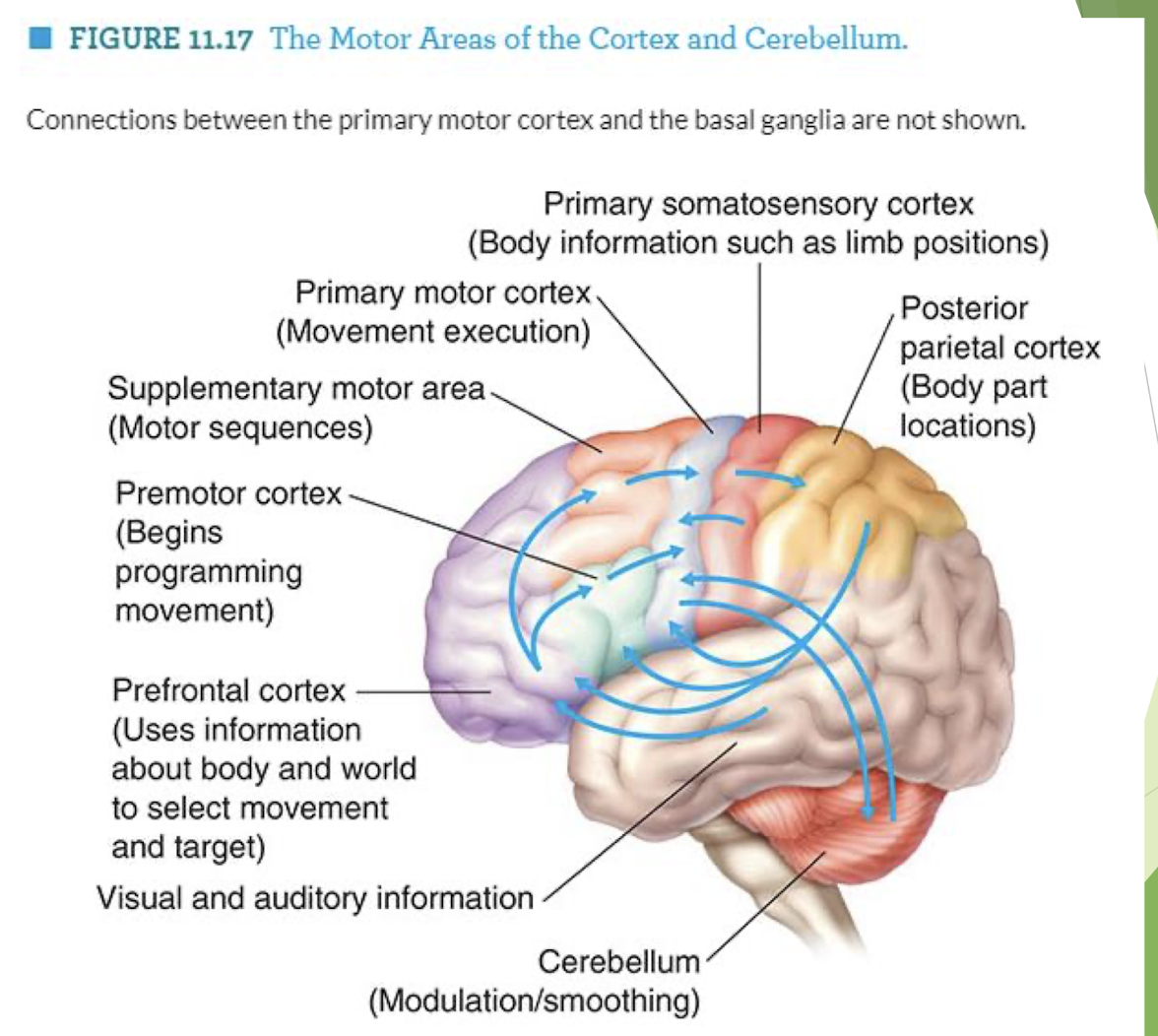
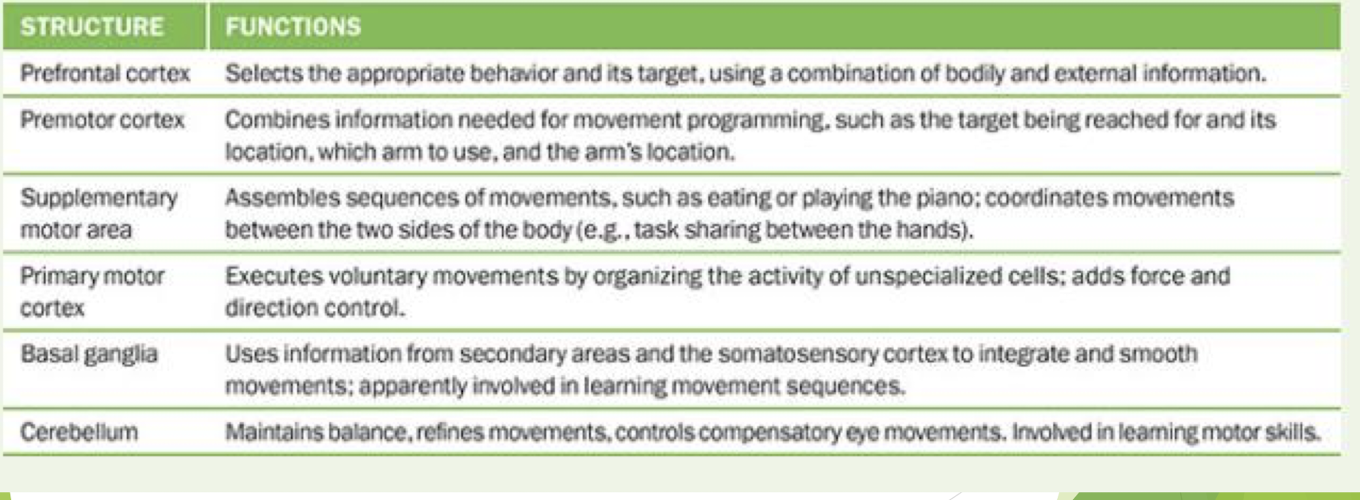
Brain & Movement: 1. Prefrontal Cortex
roles:
plans actions & considers their consequences
receives info from ventral visual stream abt object identity
does integration of sensory info with body info (from posterior parietal cortex)
holds this info in memory while selecting an appropriate movement
“I want to bake a cake”
Brain & Movement: 2. Secondary Motor Areas - Premotor cortex
programs movement
by: combining info from prefrontal cortex & posterior partial cortex
→ plans exact steps
→ most active right BEFORE a movement
→ has diff. specialized cells
“this is the receipt to use”
Brain & Movement: 3. Secondary Motor Areas - Supplementary motor area
assembles séquences of movements
Brain & Movement: 4. Primary motor cortex
organization & execution of VOLUNTARY movements
by: assembling complex movement sequences from input of secondary motor areas, somatosensory cortex & posterior parietal area
→ most active DURING the movement
→ cells aren’t for specific movements, just for specific parts of the body
ex. use same finger cells to do diff movements
send to:
basal ganglia
cerebellum
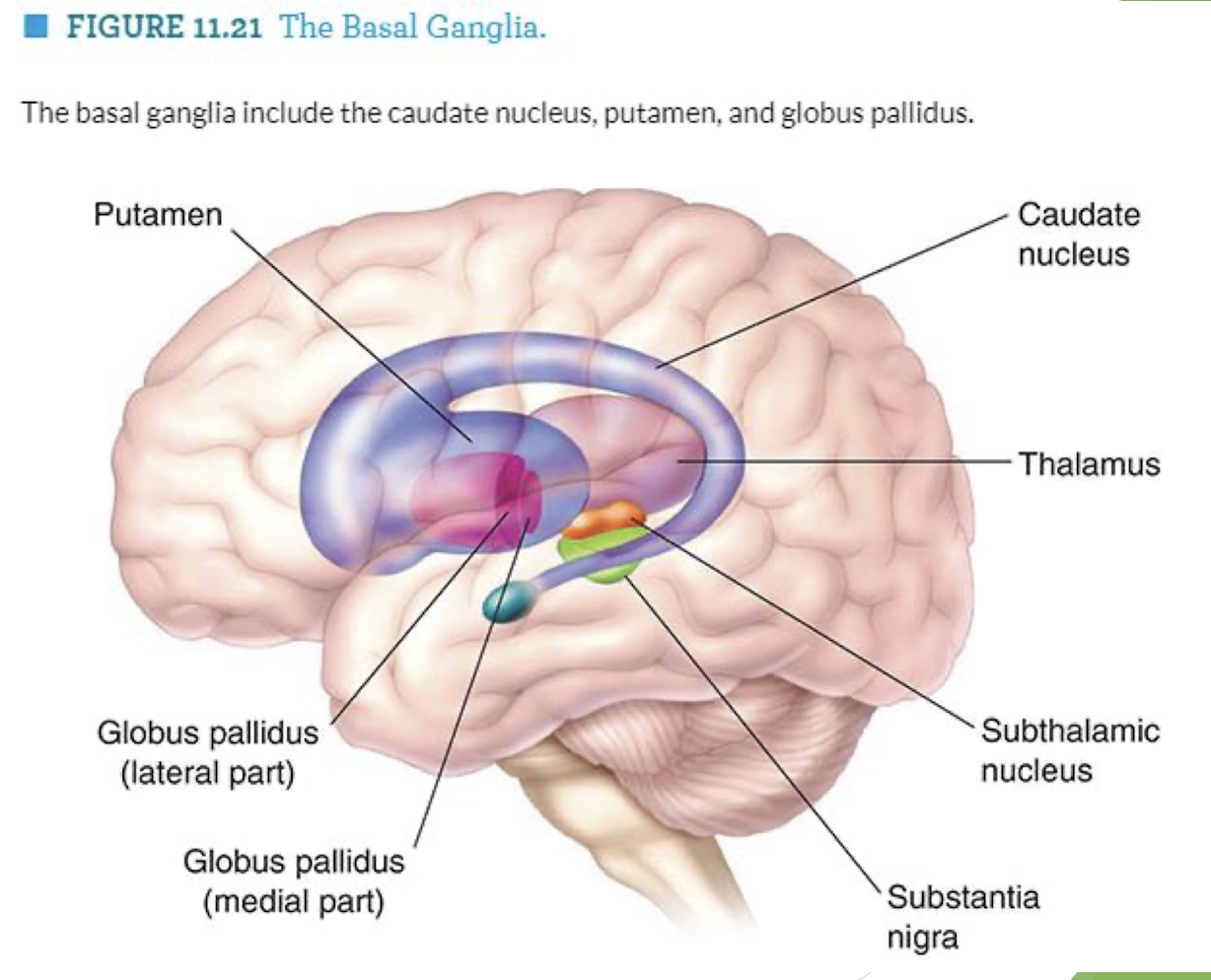
Brain & Movement: 5. Basal Ganglia
use info from primary & secondary motor areas & the somatosensory cortex to integrate + smooth movements
role: fine tunes movements
includes: caudate nucleus, putamen, globus pallidus, substantia nigra
Brain & Movement: 6. Cerebellum
compares body’s movements to what was planned → adjusts & sends corrections back to primary motor cortex
uses motor cortex info: to determine order & timing of muscular contractions
uses vestibular system info: to maintain posture & balance, refine movements, & control eye movements
Brain & Movement: Summary
Disorders of Movement: Parkinson’s Disease
= motor tremors, rigidity, loss of balance & coordination, difficulty moving & initiating movements
causes:
deterioration of substantia nigra (basal ganglia)
lewy bodies may contribute to cognitive deficits (cause scarring → CANT make new neurons)
genetic & environmental factors (TBIs, toxins)
normal fxn of substantia nigra = sends dopamine to basal ganglia to control stop/start movements
→ lose this signal wit Parkinsons
note:
can reduce risk by 50% by smoking nioctine
can reduce risk by 80% by drinking coffee - possibly bc it blocks adenosine receptors
Disorders of Movement: Parkinson’s Disease - Treatments
note: cant just inject dopamine bc it CANT cross the blood brain barrier
levodopa = to make dopamine, bc the substantia cant make enough
doesn’t work in severe cases bc theres not enough cells to use it
stem cells : has side effects of tics (too much dopamine) + only lasts ~3yrs + develop tumours at injection sites
lesions to subthalmaic nucleus & globus pallidus (areas controlled by substantia) : stops shaking, BUT difficult to lesson these areas bc they’re defined by fxn not structure
deep brain stimulation (DBS) = inside brain electrode stimulation
invasive, but EFFECTIVE
increased risk of weight gain by making food more pleasurable
Disorders of Movement: Huntingtons Disease
= degenerative disorder of motor system, involving cell loss in the striatum & cortex
death within 15-30 yrs of onset
takes years to notice & starts w small involuntary movements
result:
cognitive & emotional deficits : impaired judgment, depression, personality changes
motor symptoms - due to degeneration of GABA (inhibitory) releasing neurons in striatum
involves basal ganglia & cortex
cause: Huntingtin gene - DOMINANT
have extra bases in gene & the longer the gene the MORE severe w a shorter lifespan
onset: ~40-50yrs old
this is why it doesn’t prevent passing on the gene to offspring
Disorders of Movement: Huntingtons Disease - Treatments
combinations of:
antidepressants
antipsychotics : to lower excess movements & emotional components
tetrabenazine : to reduce excess dopamine/excitation
note: a new injection silences the gene for 9months in rats & 8weeks in monkeys
Disorders of Movement: Myasthenia graves (MG)
= muscular weakness due to low #’s or sensitivity of AChR → NEED more ACh
autoimmune disease
can be so extreme a respirator is needed, bc it affects ALL muscles → diaphragm cant move
continued loss of AChR as it progresses
Treatments:
drugs that inhibits acetylcholinesterase (breaks ACh) → prolong ACh in synapse
Thymetcomy = remove thymus → removes producer of the antibodies destroying AChR
full symptoms elimination 8m-1yr for 80% of ppl
remaining 20% see some symptoms improve
Disorders of Movement: Multiple Sclerosis (MS)
= motor disorder caused by demyelination & neuron loss in CNS
early sign: impaired synchronous activities (ex. hands moving at diff times bc of signal lag)
leads to: pain, incontinence, double vision, …
causes:
possibly bc of immune system over-activation (specific T-cells are linked)
genetic & environmental influences ] need gene & environ to activate
certain diseases activate MS
Treatments:
NO drug can reverse damage done before treatment
chemotherapy or stem cells can help - 45% don’t progress in symptoms for 4-5yrs