physiology test 3
1/303
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
304 Terms
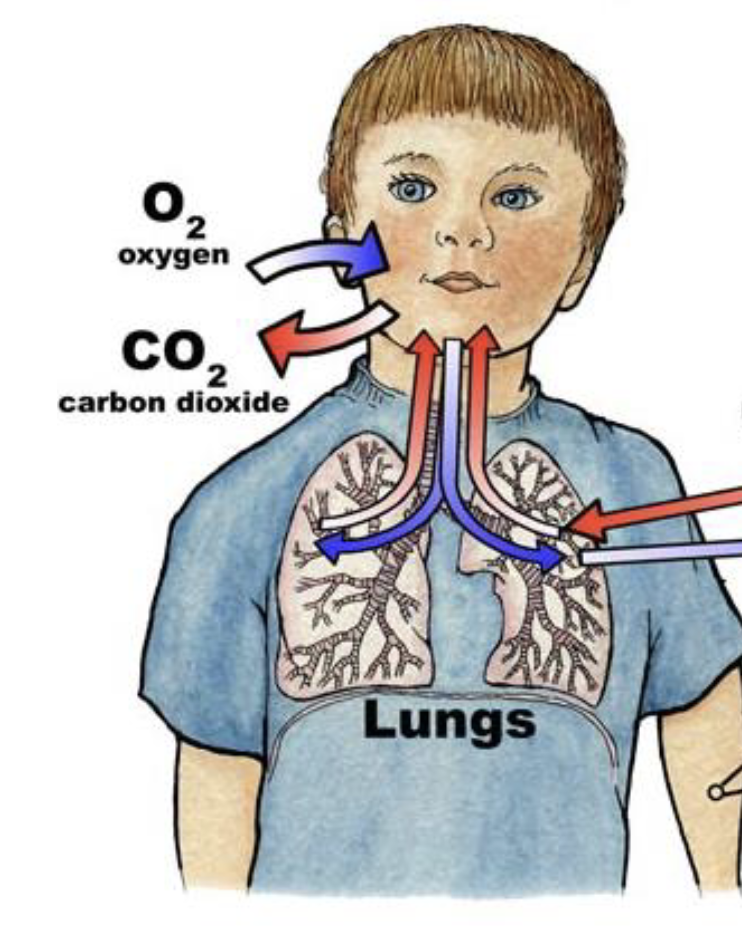
what are the different types of respiration
external respiration
cellular respiration
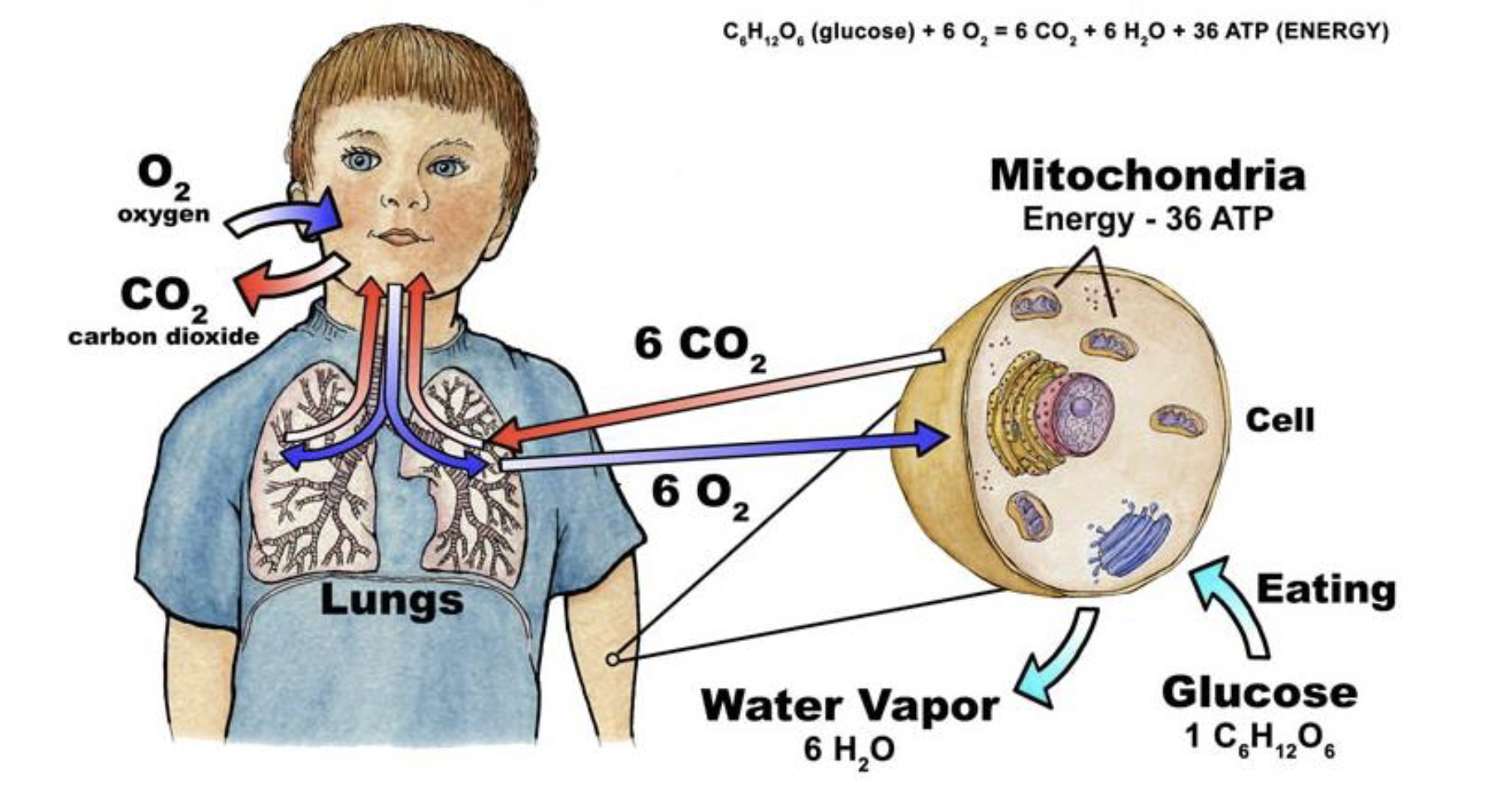
describe external respiration
the movement of gases between the environment and the body’s cells
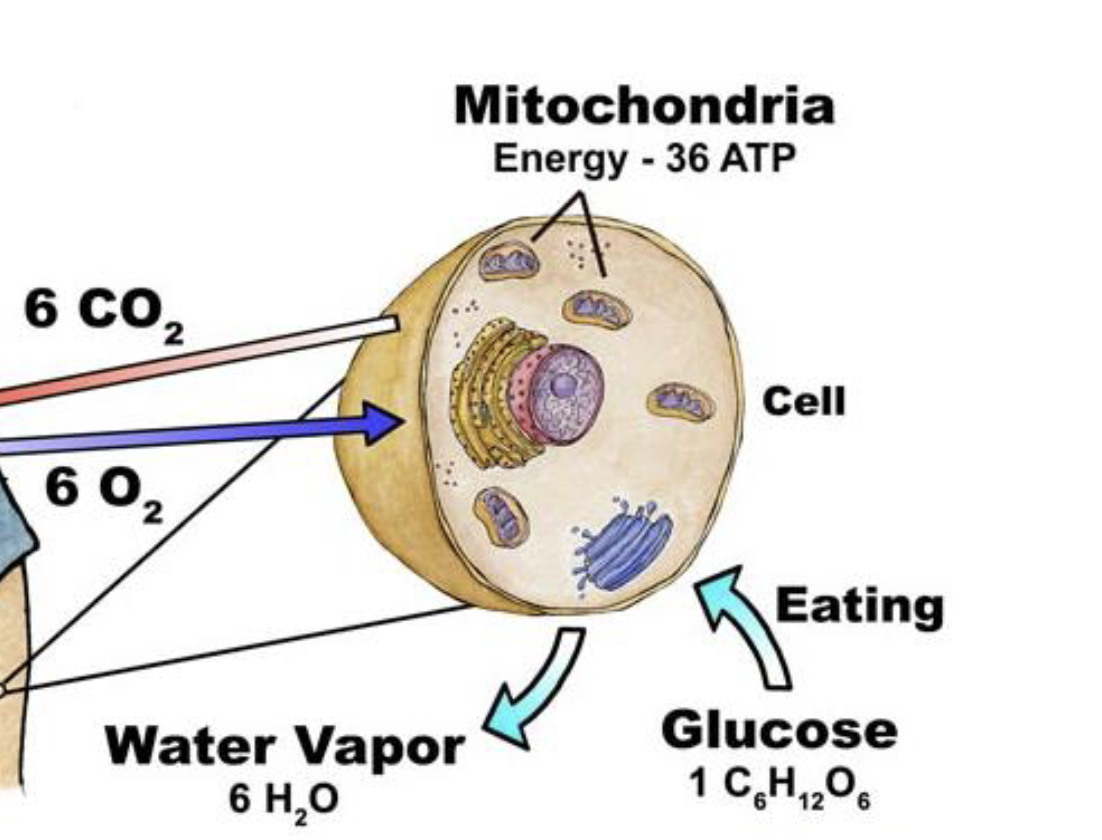
describe cellular respiration
what is going on in the mitochondria
intracellular reactions with oxygen (final electron acceptor) to produce energy in the form of ATP
what are the fundamental requirements for gas exchange
moist surface
thin barrier
large surface area
partial pressure gradients
ventilation and perfusion
describe a moist surface as a fundamental requirement for gas exchange
gases must dissolve in water before they can diffuse across membranes
solubility and how moist the surfaces are
gas particles have to dissolve into a liquid
describe a thin barrier as a fundamental requirement for gas exchange
the respiratory surface must be thin to minimize diffusion distance
fick’s law of diffusion
easy to pass through and increase rate of diffusion to supply oxygen into the bloodstream at the rate it is needed
describe large surface area as a fundamental requirement for gas exchange
a greater surface area allows for more efficient gas exchange
fick’s law of diffusion
describe partial pressure gradients as a fundamental requirement for gas exchange
gases move from an area of higher partial pressure to lower partial pressure
pressure dictates diffusion
Henry’s Law is the actual law behind this
describe ventilation and perfusion as a fundamental requirement for gas exchange
mechanisms to maintain gradients (e.g. breathing, blood flow)
bulk flow when brining in air from the atmosphere into our conducting system and then getting it into our bloodstream
what are the four processes in vertebrates that comprise external respiration
bulk flow of atmospheric air into and out of the lungs (i.e. ventilation)
diffusion of molecules between the air in the lungs and dissolved in the blood
CV transport of gases dissolved in the blood using bulk flow
diffusion of molecules between those dissolved in the blood and those dissolved in the interstitial fluid and cytosol
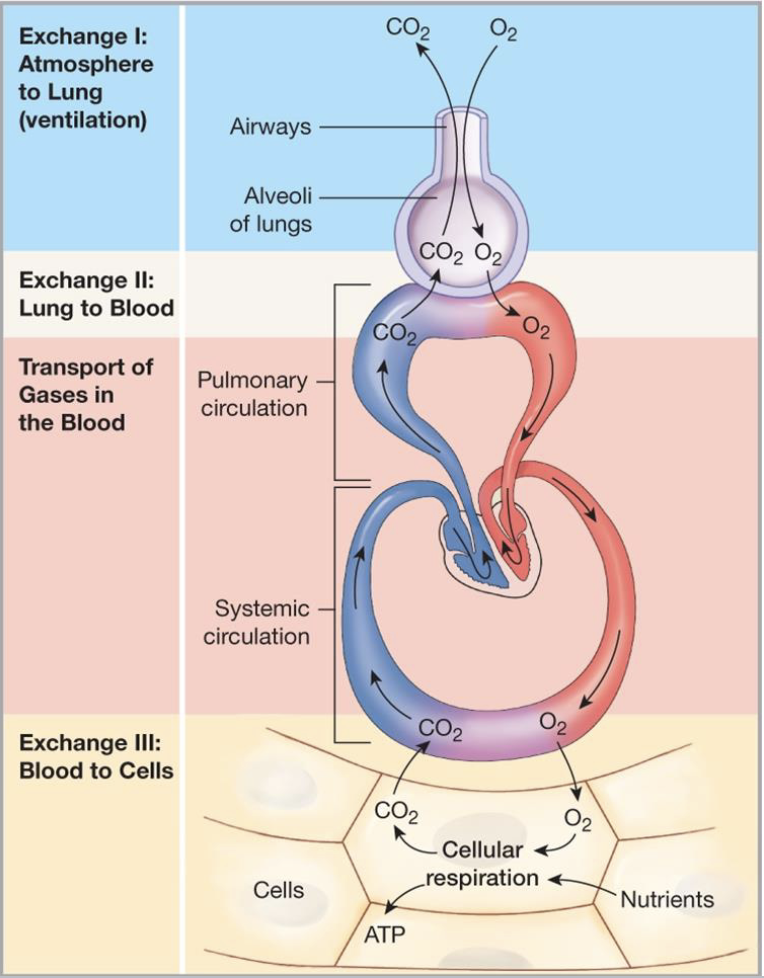
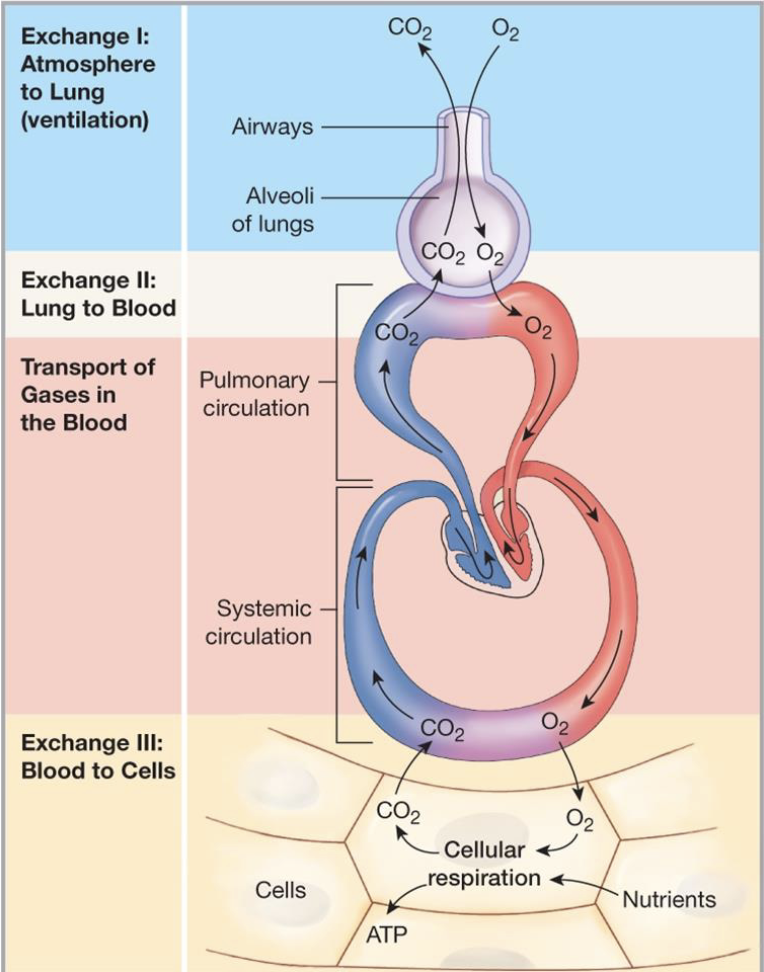
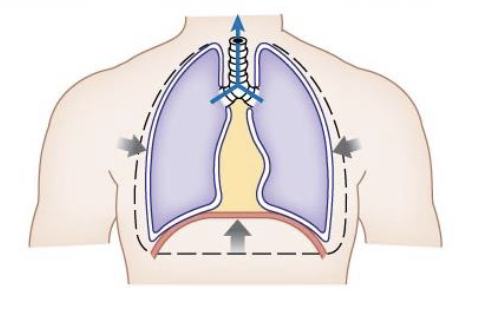
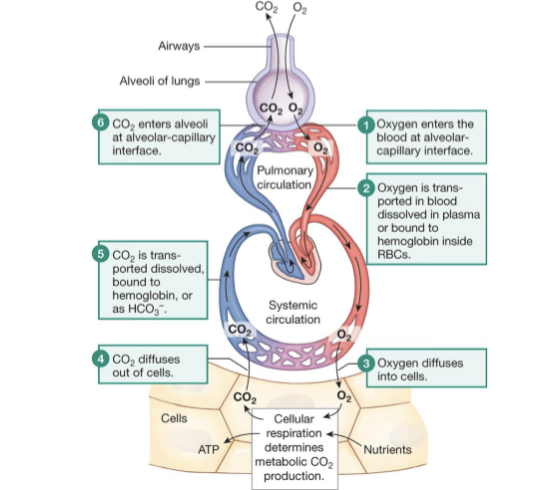
describe what is happening in this diagram
Oxygen is being inspired from the atmosphere
oxygen fills the aveoli
oxygen diffuse into the blood stream down a pressure gradient as there is more oxygen in the atmosphere than in the blood stream
higher pressure of oxygen in the blood than in the tissues (tissues constantly using up oxygen in the process of respiration)
oxygen diffuses into tissues
CO2 is produced as a biproduct of respiration
CO2 diffuses into the blood stream following the pressure gradient and then into the aveoli
describe the conducting system
part of the respiratory system not involved in the gas exchange (everything but the alveoli)
provides a low-resistance pathway for airflow and conditions inspired air
thick cartilage rings keep the structure fixed and open (so non-collapsible)
air gets warmed to the temperature of the body, humidified, and filtered here
total cross-sectional area increases with each division (even though the diameter of the airways gets smaller, they get exponentially more numerous); reduces the velocity of airflow
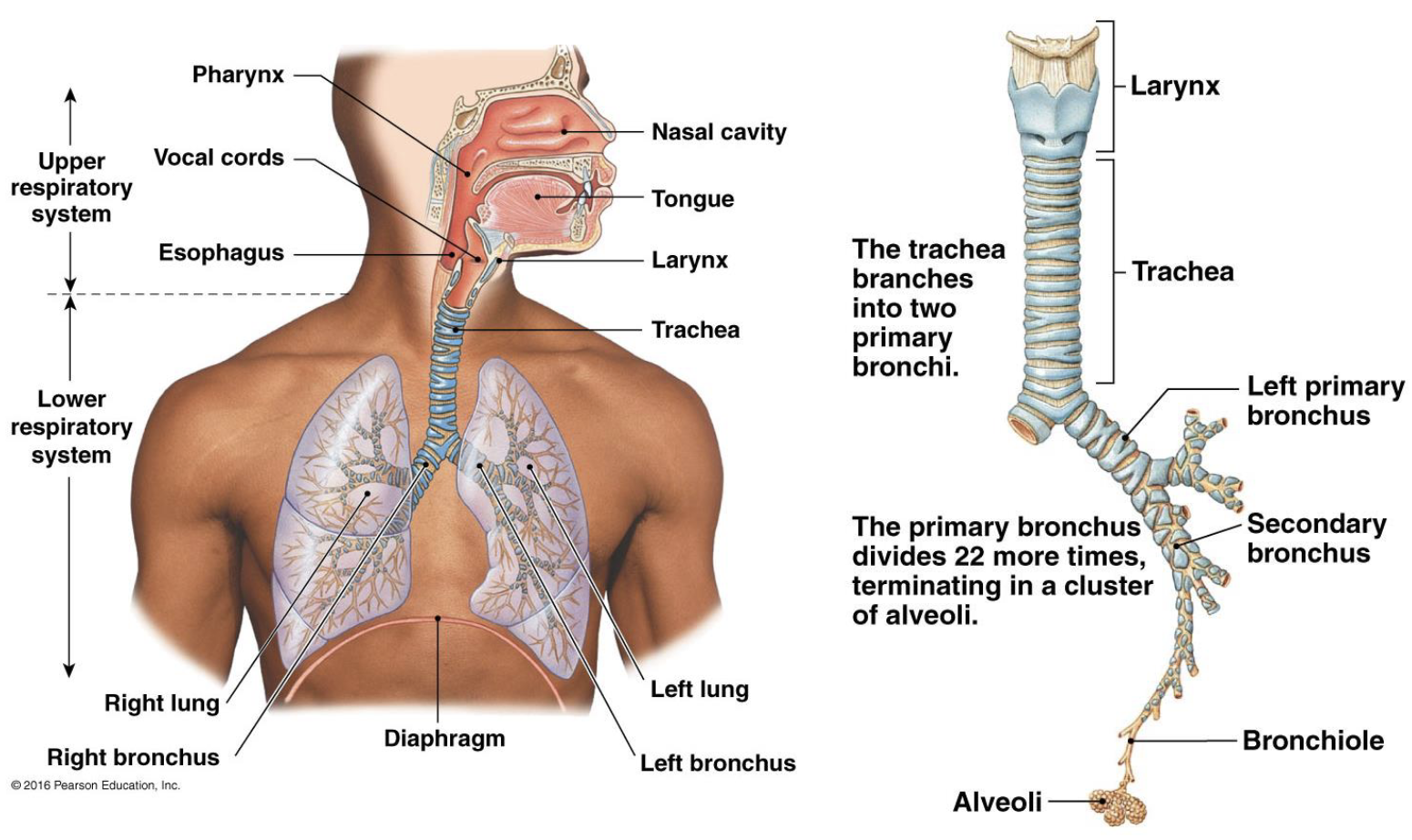
describe the diameter of the conducting system as it traveled to the aveoli
gets smaller as you go down the conducting zone
describe the cross-sectional area of the conducting system as it travels to the aveoli
total cross-sectional area increases as the amount increases, with more of the smaller parts
velocity of air flow allows more time for exchange
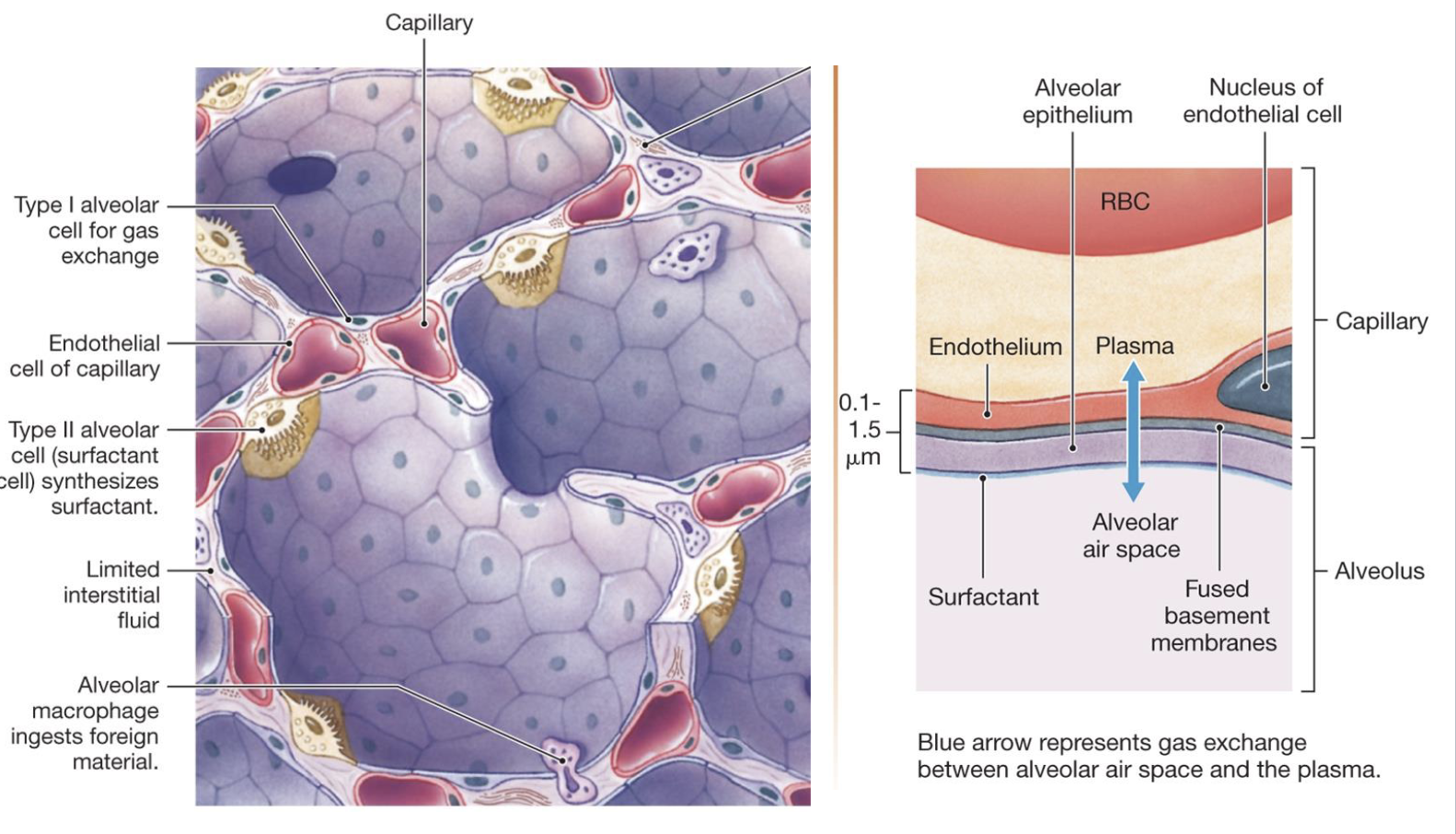
describe the aveoli
microscopic, thin-walled air sacs that are the primary site of gas exchange within the lungs, which facilitate the rapid and efficient exchange of O2 from inhaled air into the blood and CO2 from the blood into the alveolar air for exhalation
where gas exchange occurs
want to have a thin membrane for oxygen to enter the bloodstream and CO2 to exit the bloodstream
capillary beds surround in order to facilitate gas exchange
lots of moisture and high humidity surrounding the membrane sacs
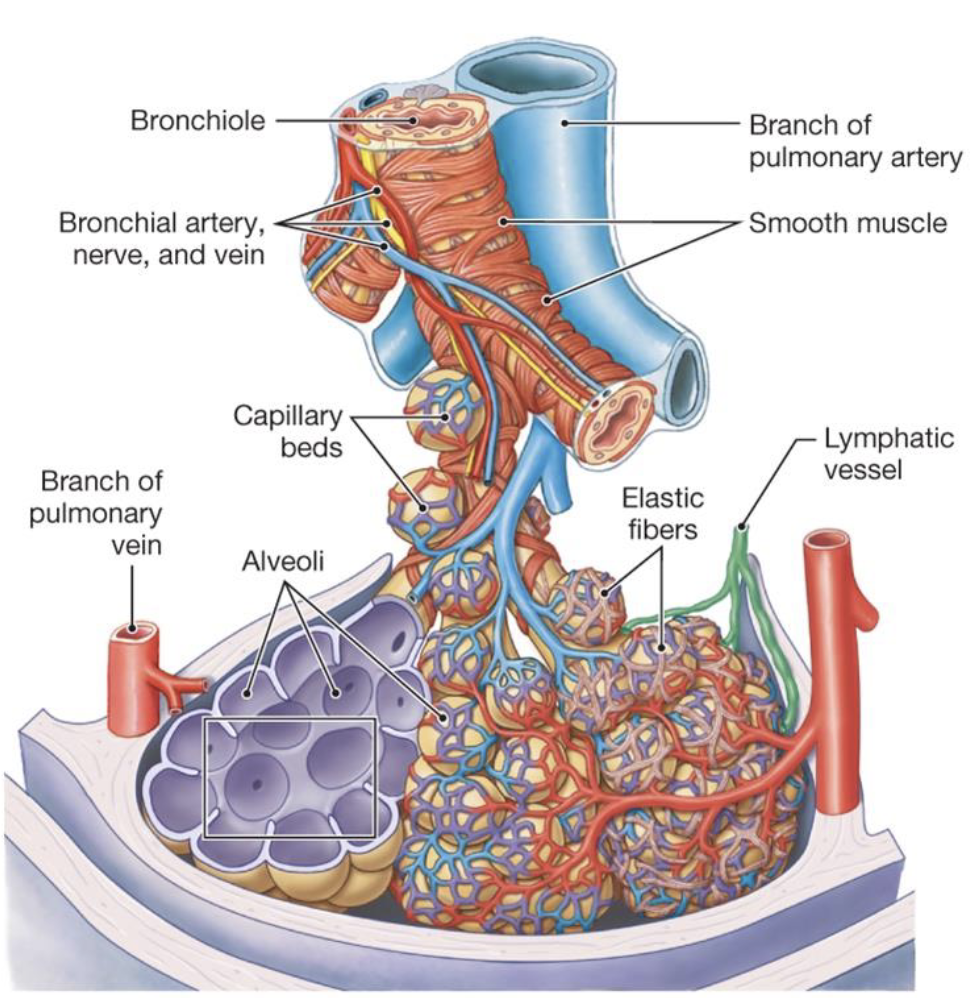
what are the three important factors of the aveoli
large surface area (about the area of a tennis court if you unravel all of it)
short diffusion distance (only 1 epithelial cell thick and 80-90% of the external surface is surrounded by capillaries)
large concentration gradient (always replenished)
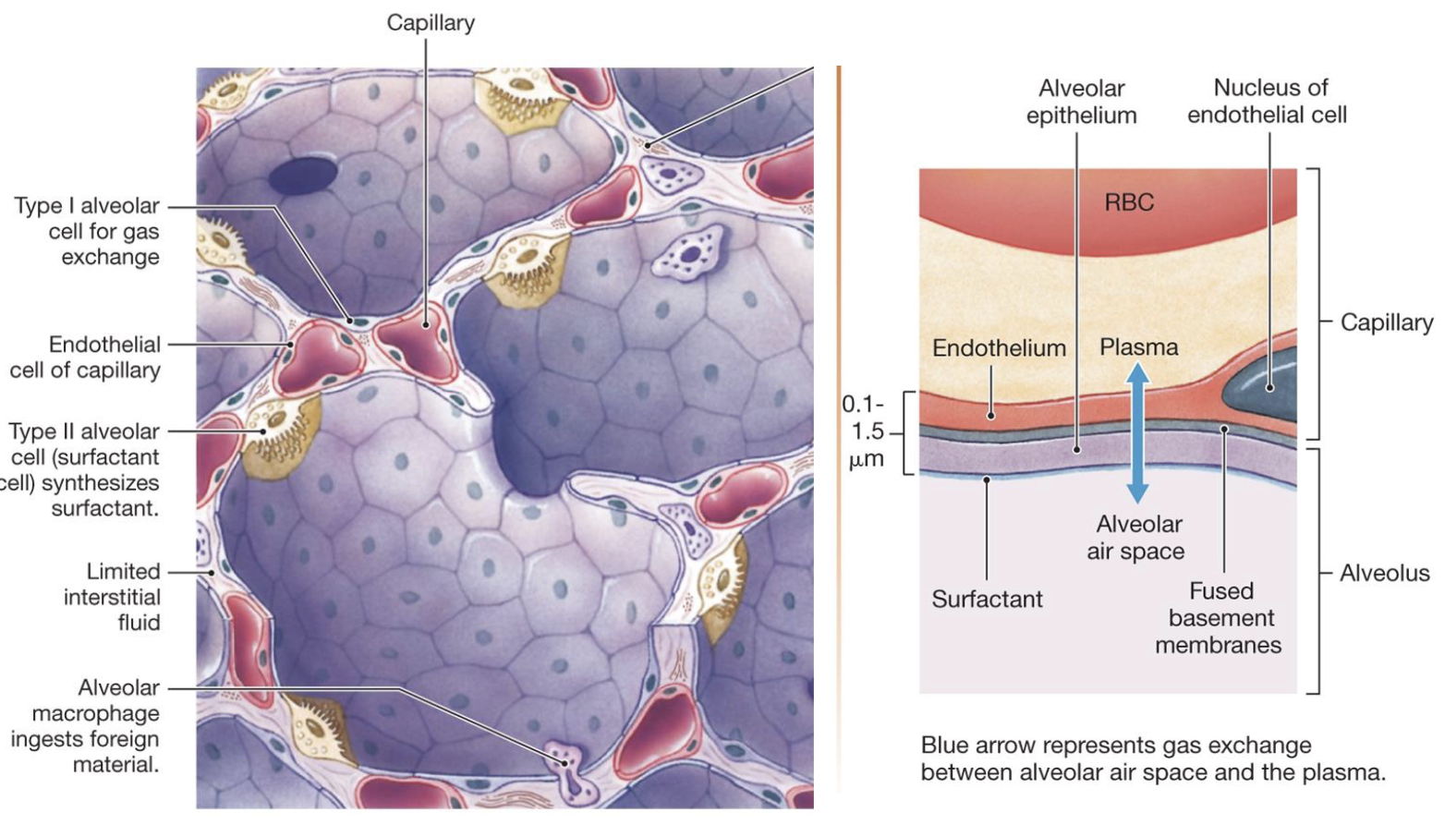
describe type I alveolar cells
involved in gas exchange
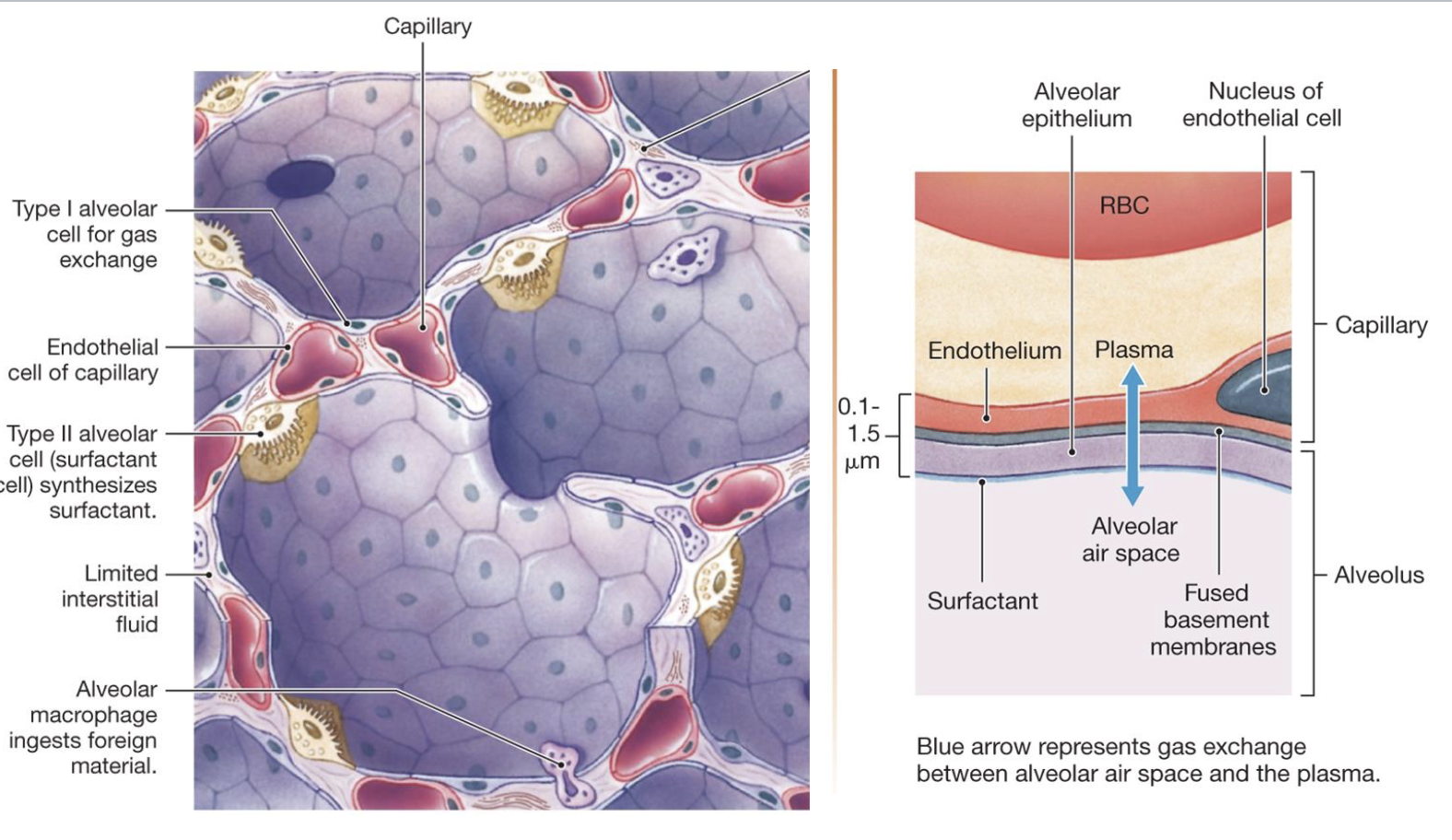
describe type II alveolar cell
aka surfactant cells
synthesize and secrete surfactant
decreases surface tension and allows for the expansion
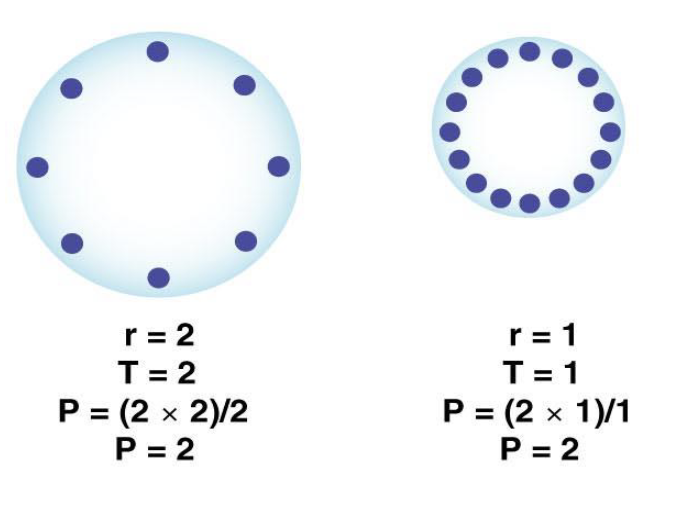
describe how surfactant reduces the surface tension inside alveoli so they require less effort to inflate
Law of LaPlace: P = 2T/r
if two bubbles have the same surface tension, the smaller bubble will have the higher pressure according to the law of LaPlace
surfactant reduces surface tension by H-bonding with surrounding moist areas to help break up the surface tension
equalize the pressure between the two sizes and make i easy to inflate for gas exchange to occur
describe why premature infants are susceptible to respiratory distress syndrome
can’t produce surfactant, so everytime they go to exhale, their aveoli collapse and cannot open up again
surfactant isn’t produced until about 34 weeks when type II alveolar cells become fully mature
leads to high alveolar surface tension leading to their collapse
treatment is to use a nebulizer to administer an aerosolized surfactant and ventilation support
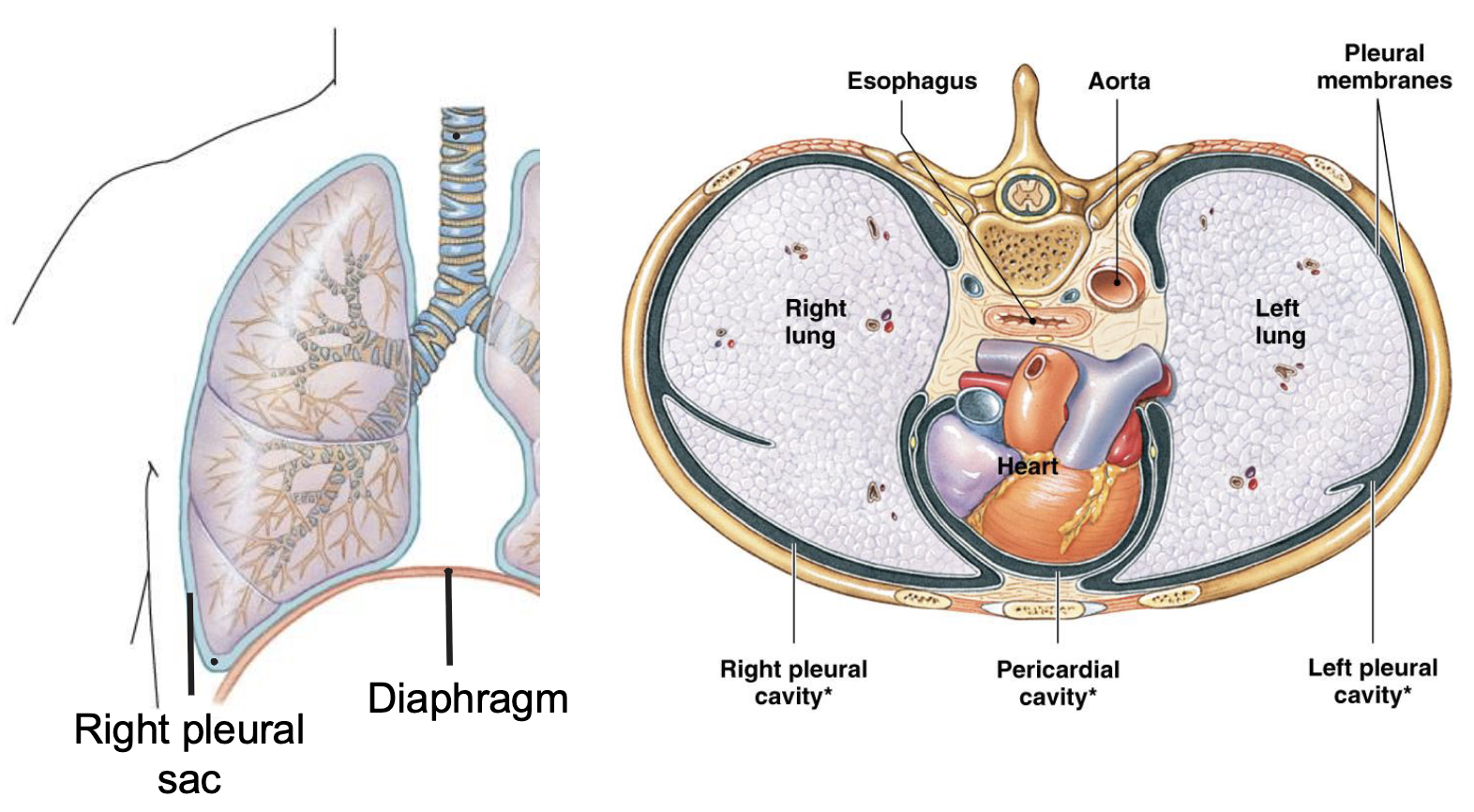
describe how lungs expand since they cannot expand on their own
plueral sac surrounds the lungs and keeps them compartmentalized to a certain extent
moisture creates a surface tension (negative pressure) because of the liquid nature of the sac that holds the chest wall and lungs together
anchors the lung to the chest wall because of the moist liquid nature of this sac, it makes it easier to stick to that chest wall
when the chest wall expands, it’s going to take the lung with it
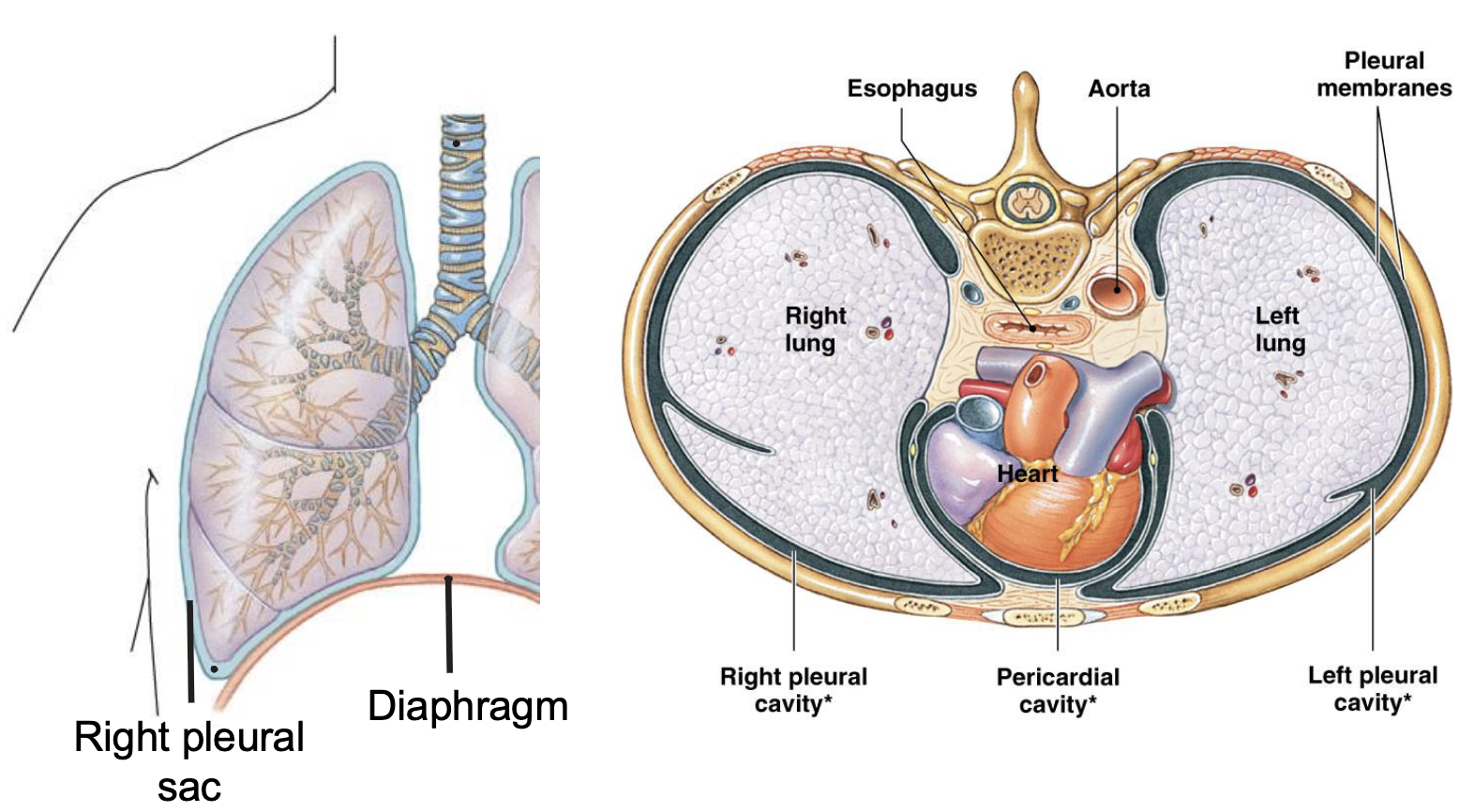
describe the pleural sac
a two-layered membranous sac that surrounds the lungs and lines the chest cavity which allows the lungs to move easily and inflate when breathing
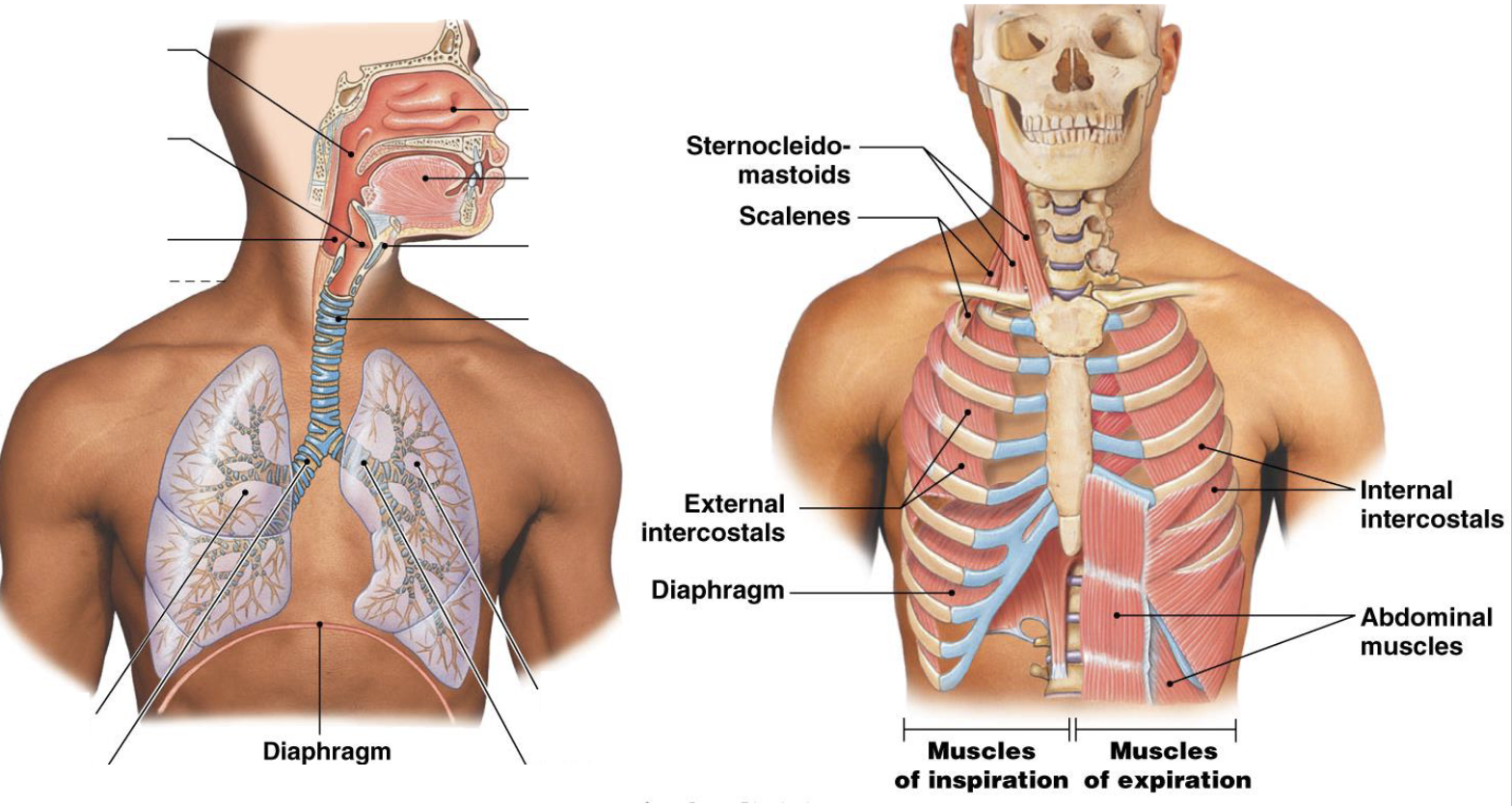
describe the role of skeletal muscles in ventilation
change the volume of the thoracic cavity, which alters the pressure in the lungs and creates the pressure gradients for airflow
skeletal muscles do the work to expand the chest wall and because the pleural sac is stuck to it, it just follows
the lungs and muscles have opposing forces as the tension is in opposite direction as the chest wall expands outward, the elasticity of the lungs wants to go inward
external and internal intercostals help expand and contract
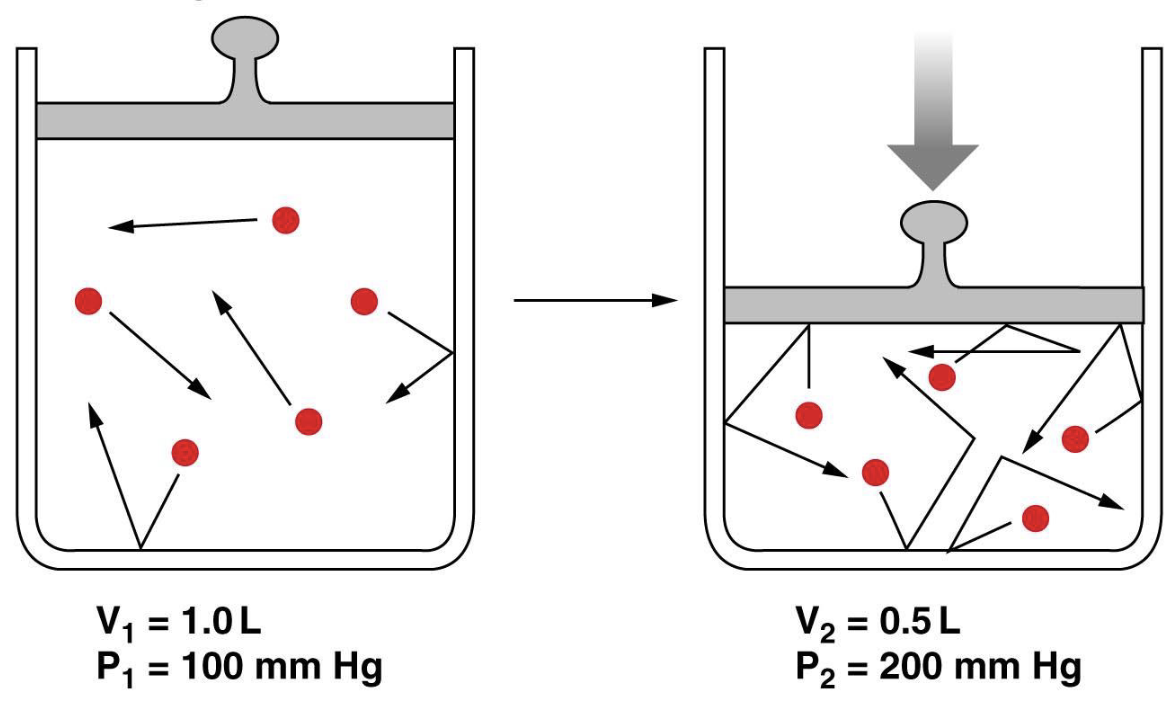
how are volume and pressure related
inversely proportional
boyle’s law: P1V1=P2V2
decreasing volume increases collisions and increases pressure (and vice versa)
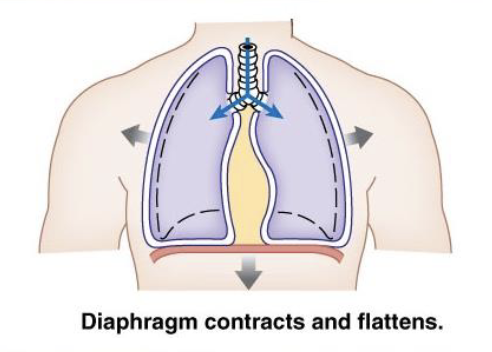
describe inspiration
thoracic volume increase (needs to make room so the diaphragm contracts and moves down)
diaphragm contracts down (give a mechanical boost to the lungs)
ribs contract outward
space inside lungs increases
pressure inside lungs decreases
pressure inside lungs is less than atmospheric pressure
air rushes into lungs
describe expiration
diaphragm relaxes, thoracic volume decreases (diaphragm relaxes and pushes up on the lungs and helping to force out the air)
diaphragm relaxes up
ribs relax downward
elastin causes lungs to shrink
space inside lungs decreases
pressure inside lungs increases
pressure inside lungs is greater than atmospheric pressure
air rushes out of the lungs
describe the functions of the pleural sac
creates a moist slippery surface that reduces friction during ventilation
holds lungs tight to the thoracic wall so that when it expands the lungs expand with it
uses cohesive forces to hold membranes together so hey move as one
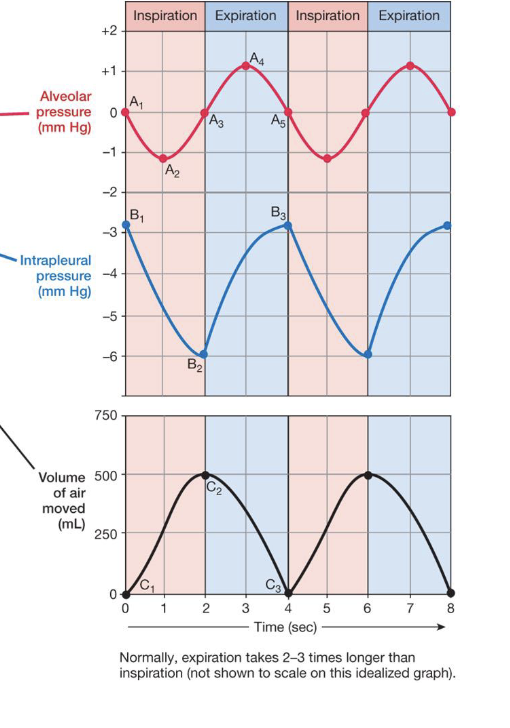
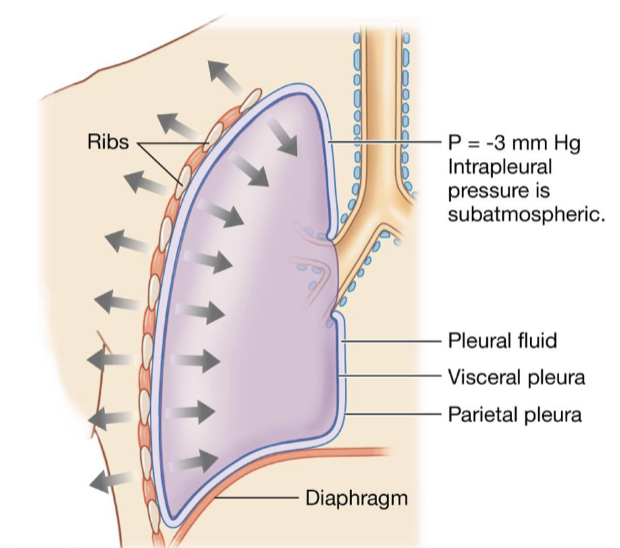
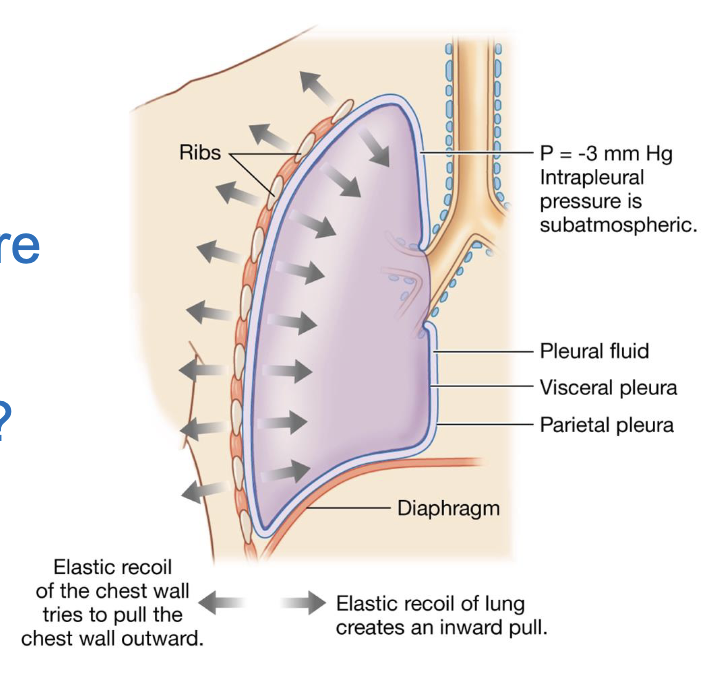
describe intrapleural pressure
negative pressure inside pleural sac is due to:
developmentally created in utero
chest wall elasticity
elastic recoil of lungs
resistance of pleural fluid to being “stretched”
pressure is opposing direction because of the lungs’ elasticity
when the rib cage expands, the lungs are going to go with it because its anchored o that pleural sac, but the elasticity of the lungs wants to snap back so that the pressure is the opposing direction
what would happen if the pleural sac were punctured and you tried to breathe
the lungs cannot properly work and there is a loss of compliance
the lung will collapse
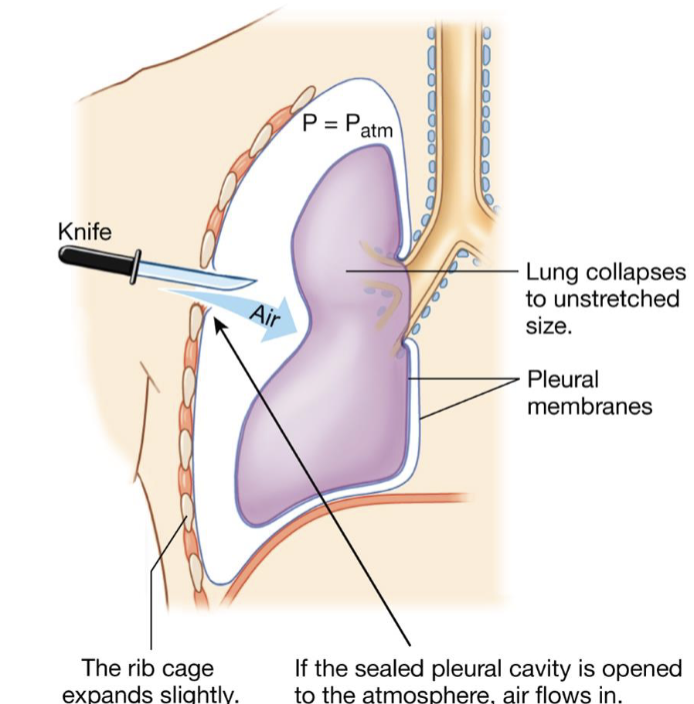
describe a pneumothorax
if the sealed pleural cavity is opened to the atmosphere, air flows in
the bond holding the lung to the chest wall is broken, and the lung collapses, creating air in the thorax
positive atmospheric pressure enters through the muscles
lost of compliance
describe anatomical dead space (ADS)
portions of the conducting zone that have some remainder of fresh or stale air
important in understanding the pressure gradient and how pressure is going to decrease when it gets to the alveoli
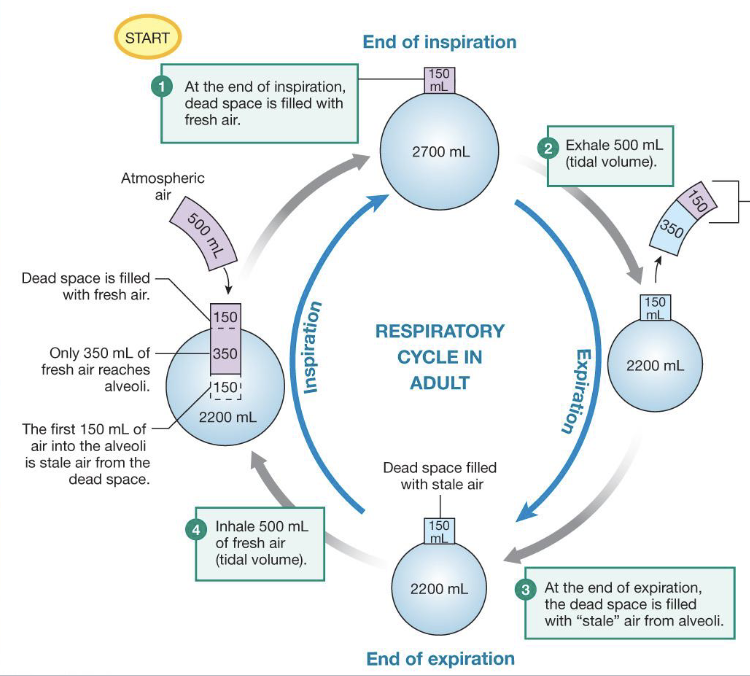
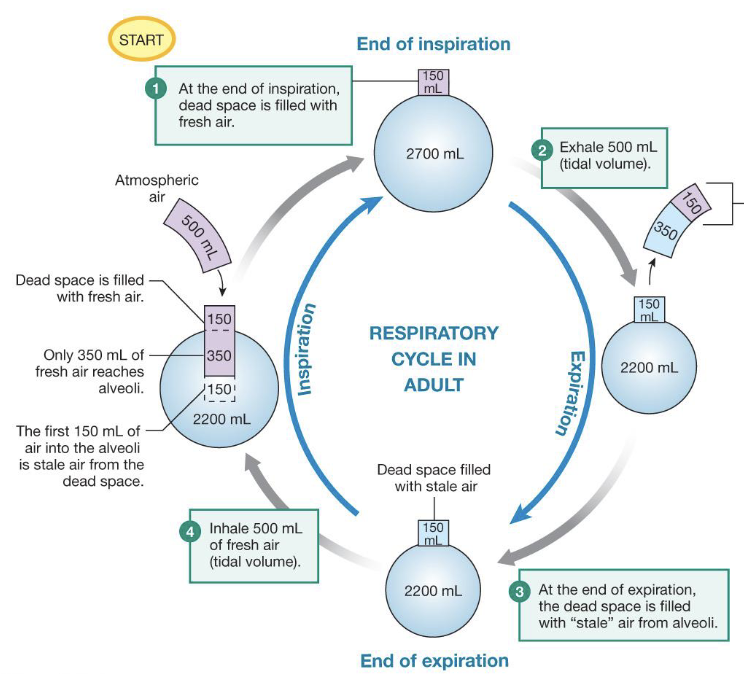
describe what is happening in this diagram
at the end of inspiration, there is 150 mL of fresh air left over in the conducting zone and 2700 mL of stale air in the alveoli due to gas exchange
when the body exhales 500 mL, the first 150 mL is the fresh air left over in the conducting zone and the final 350 is stale air from the alveoli
at the end of expiration, 150 mL of stale air remains in the conducting zone
when the body inhales 500 ml of fresh air, the first 150 mL is the stale air from the conducting zone and the second 350 mL is fresh air; there is 150 mL of fresh air that remains in the conducting zone
what is tidal volume
the amount of air that is going to be expelled
what does stale air refer to
air that has been mined of its oxygen by the oxygen diffusing into the blood stream
why is there always 150 mL of air in the conducting zone
conducting airways are reinforced with cartilage and do not collapse during ventilation
how much of your total blood volume does the pulmonary circulatory system contain at any given time
10 percent
what occurs as a result of the flow rate being high due to the extensive number of capillaries in the alveoli
it has a slower velocity than it does in the rest of your body
the blood pressure in the pulmonary circuit remains low (25/8 mm Hg rather than 120/80 mm Hg)

what are the steps for gas exchange with the blood in the capillaries
Ventilation leads to the bulk flow of atmospheric air into and out of alveoli
diffusion of gas molecules between air in the alveoli and the blood
transport of dissolved gases using bulk flow of blood in the CVS
diffusion of gas molecules between the blood and the ECF/cytosol of the cells
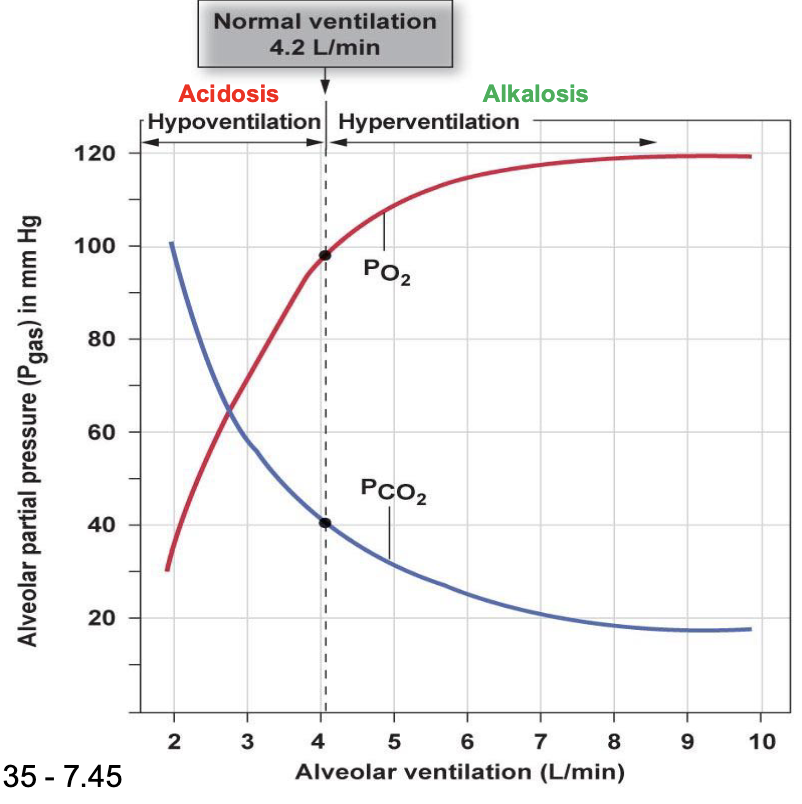
describe hypercapnia
elevated levels of CO2 in the blood
respiratory acidosis
pH decreases and in a more acidic state
not blowing off as much CO2
consumption of O2 out paces the amount coming in so O2 levels starkly decrease
describe hypoxia
too little O2 in the blood
describe respiratory alkalosis
due to hyperventilation (breathing at a faster rate than normal)
increase pH, causing basic conditions
increase in O2 partial pressure and concentration
breathing off all the CO2
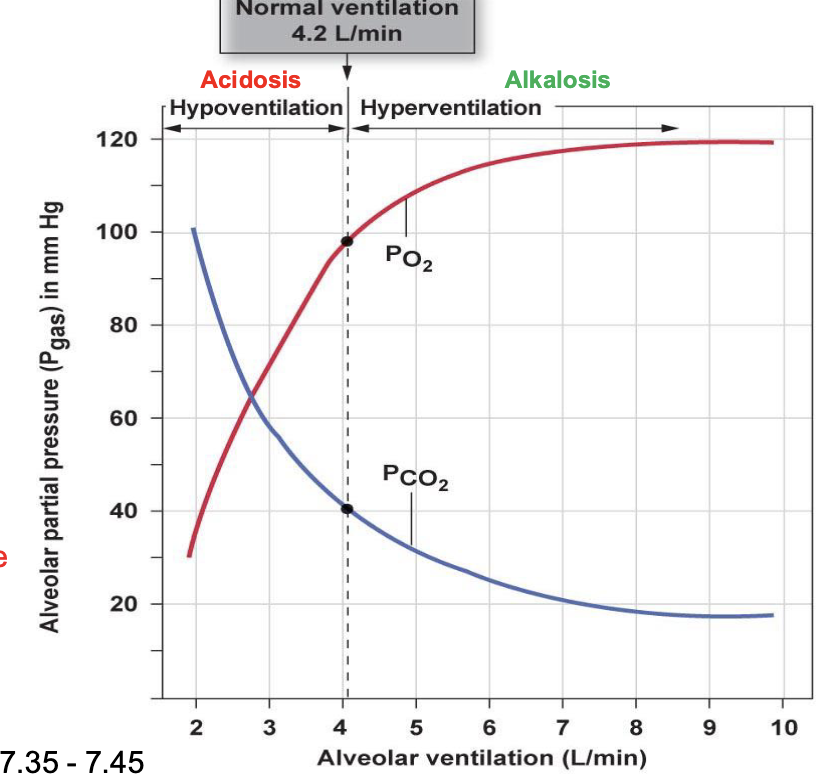
what is the physiological pH of blood
7.35-7.45
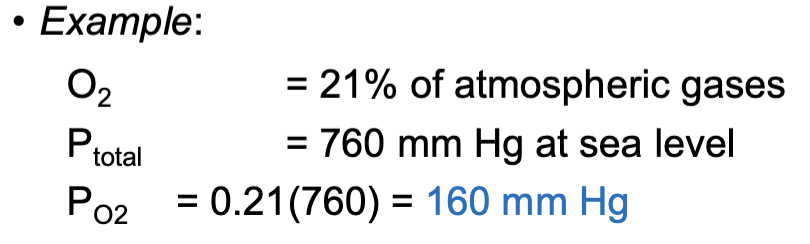
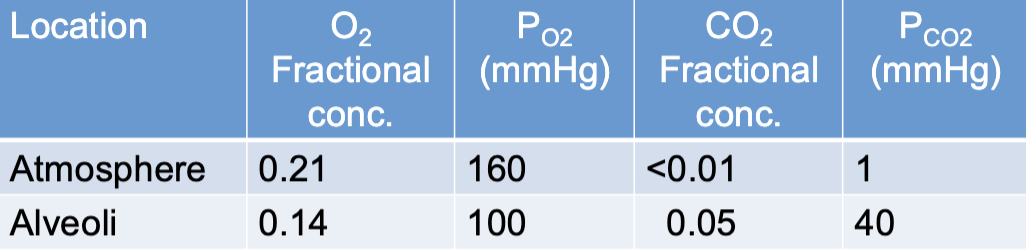
describe Dalton’s law
the total pressure of air is the sum of the partial pressures exerted by the individual gases
760 mmHg at sea level, decreases with elevation
describe partial pressure
the partial pressure of an individual gas can by calculated by multiplying the fractional concentration of a gas by the total air pressure
how does the presence of water vapor impact the partial pressures of other gases
the presence of water vapor contributes to the total air pressure, and therefore negatively impacts the partial pressures of other gases in the air
lowers the partial pressures
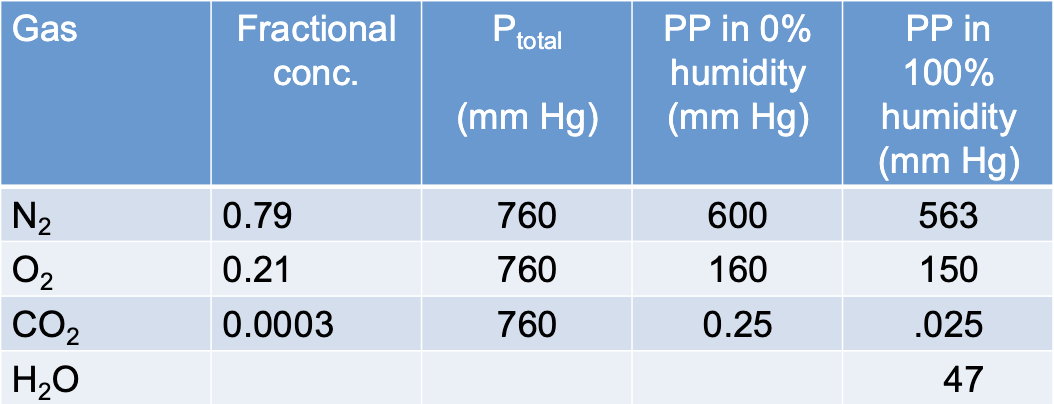
why is there a difference between atmosphere and alveolar gas composition
atmospheric air traveling through the conducting system is warmed to 37ºC and becomes 100% saturated with H2O (PH2O = 47 mmHg
PO2 of air entering the alveoli is already down to 150 mm Hg
anatomical dead space leaves stagnant air (air that doesn’t have O2 that mixes in) behind in the conducting system on exhalation
alveoli not completely emptied on exhalation (i.e. residual volume)
what law dictates that gases diffuse down partial pressure gradients
Henry’s Law
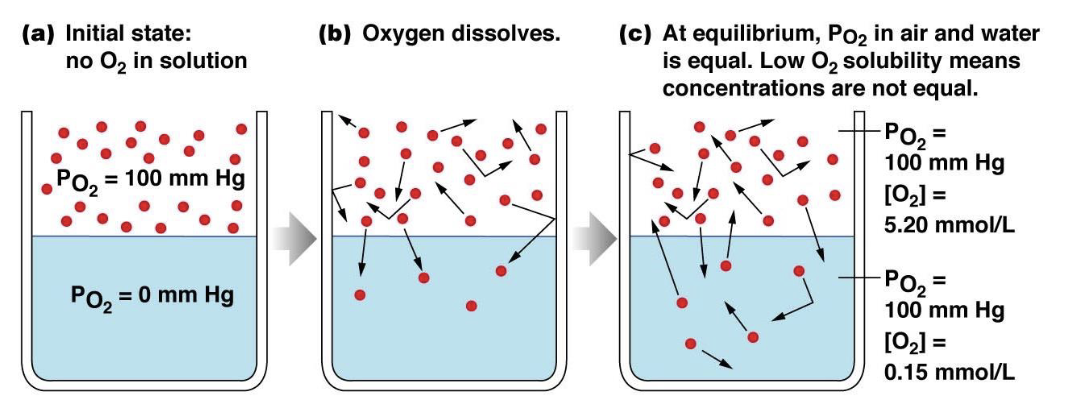
describe Henry’s Law
states that partial pressure and particle solubility determine diffusion of gas particles into a fluid, NOT particle concentration
the amount of gas that dissolves into a liquid is proportional tot he partial pressure of that gas in the gaseous phase and the solubility of that gas in a particular liquid
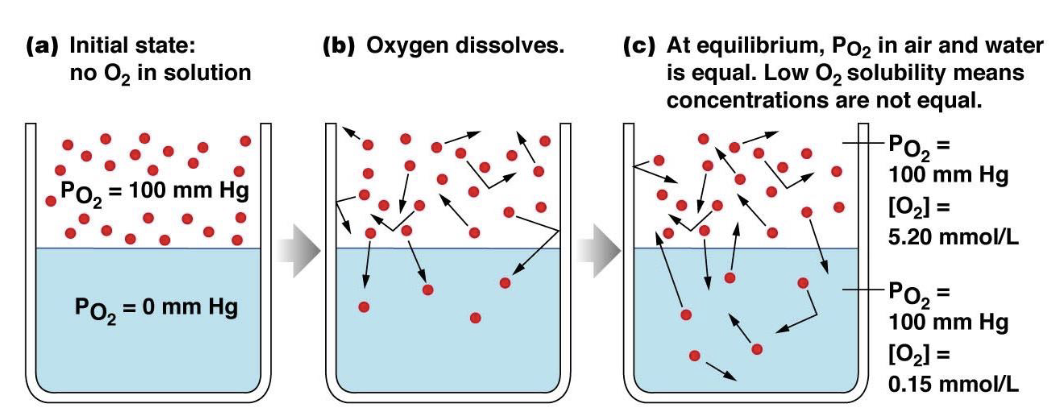
which has a higher solubility: O2 or CO2
CO2
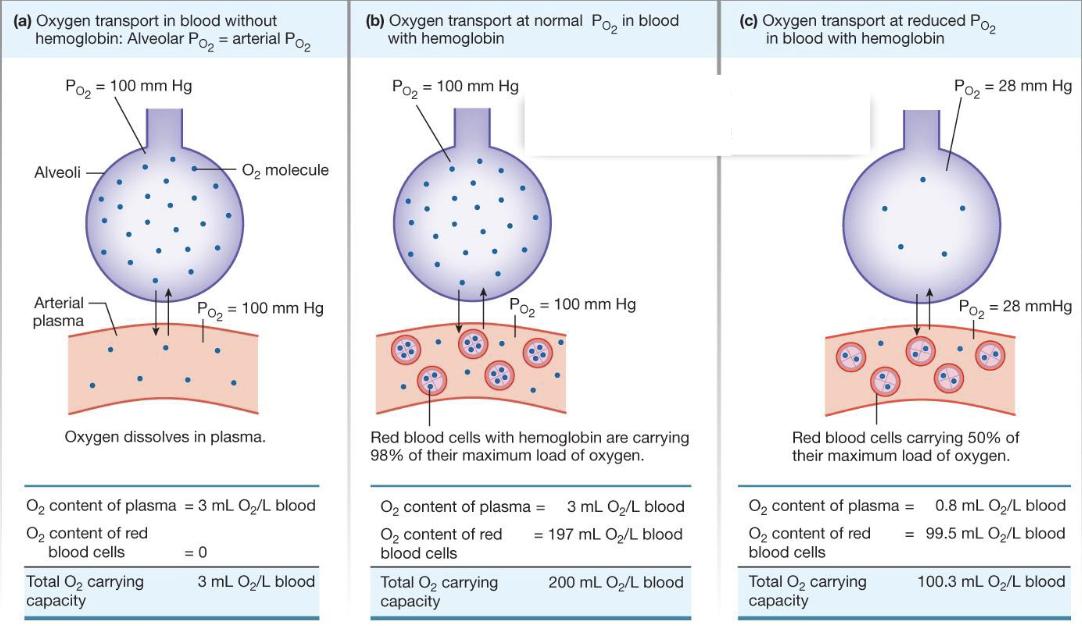
what is the role of hemoglobin in the blood
O2 transport in the blood
increases the amount of O2 that the blood can hold
without it, the blood can hold minimal O2
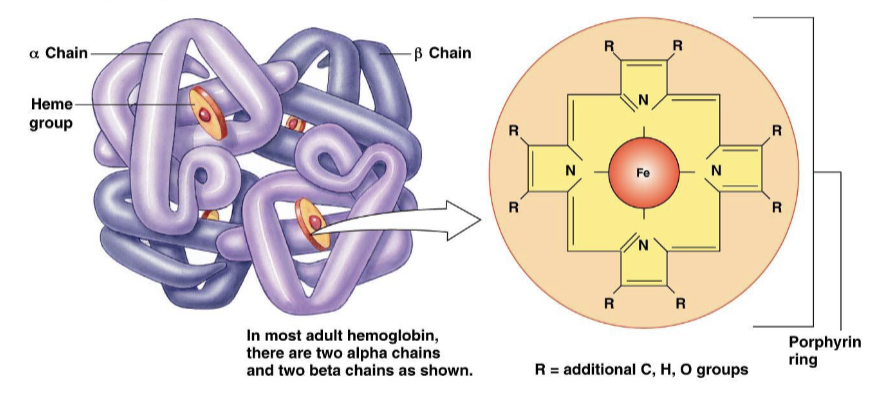
describe hemoglobin (Hb)
a molecule composed of four protein globin chains, each surrounding a central heme group
each heme group consists of a porphyrin ring with an iron atom in the center
each hemoglobin molecule can reversibly bind to four oxygen molecules
when hemoglobin is bound to oxygen, it is referred to as oxyhemoglobin (HbO2)
with each O2 that binds, there becomes a stronger affinity for the next O2 to bind
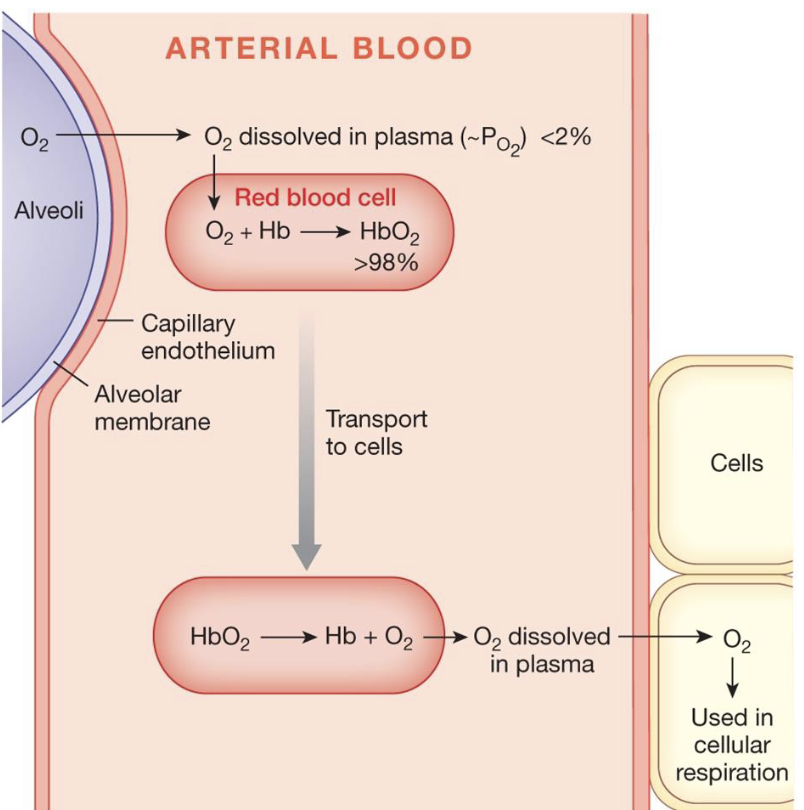
describe hemoglobin in arterial blood
when O2 leaves the alveoli, <2% is dissolved in the plasma and the rest (>98%) is in the form of oxyhemoglobin
when the oxyhemoglobin comes into contact with tissues that need it, the O2 separates from the hemoglobin, is dissolved in the plasma, and diffuses into the cell for cellular respiration
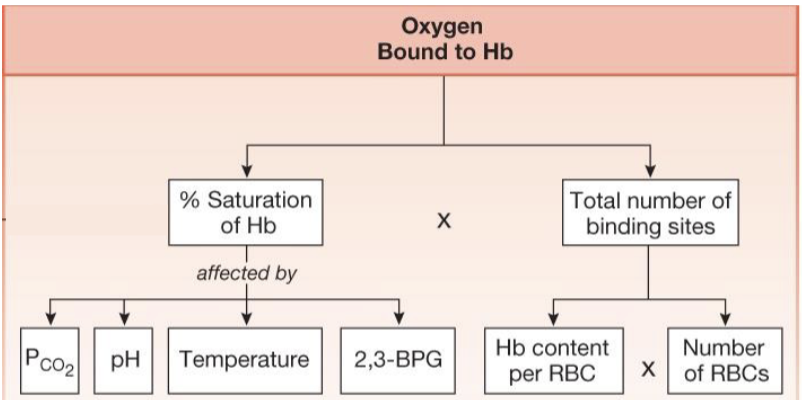
what does the amount of oxygen bound to Hb depend on
plasma O2 which determines the percent saturation of hemoglobin
amount of hemoglobin which determines the total number of Hb binding sites and is calculated from Hb content per RBC and number of RBCs
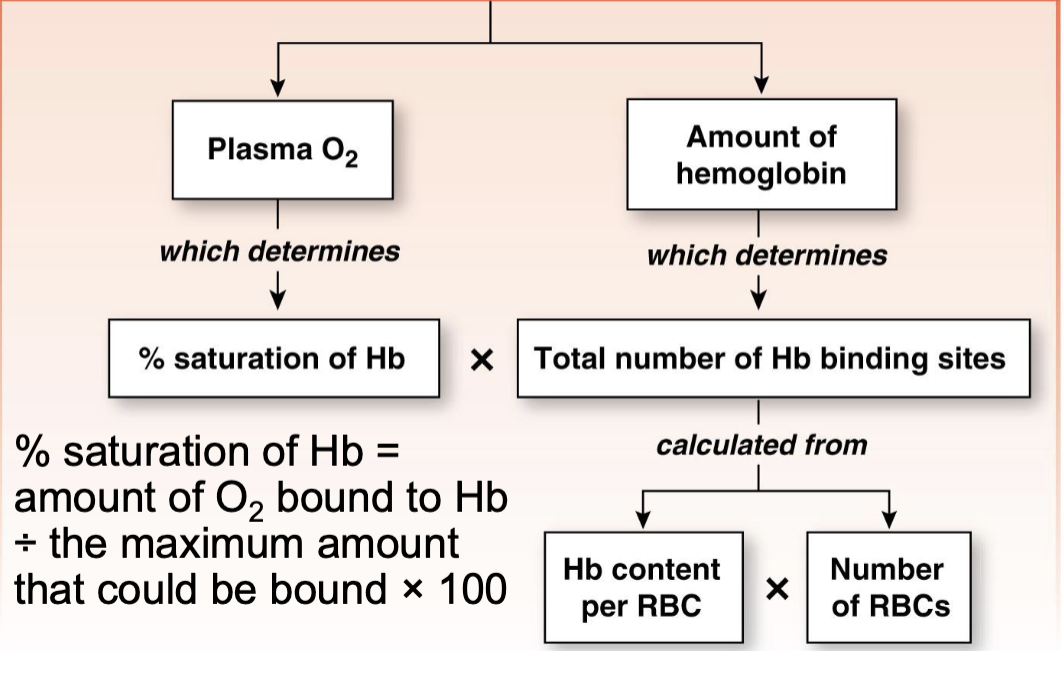
what is the equation to calculate the percent saturation of Hb
(amount of O2 bound to Hb) / (the maximum amount that could be bound) x 100
what is the percent of O2 unloaded by hemoglobin to tissues
25%
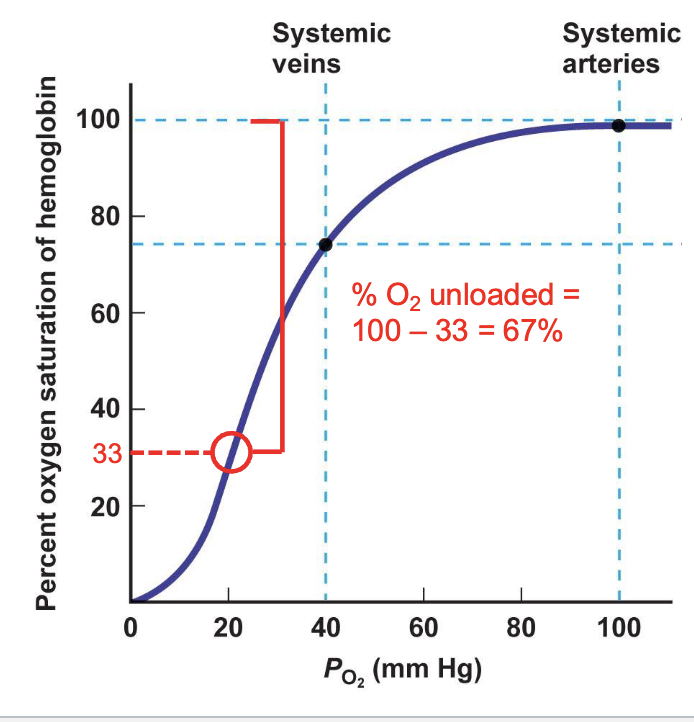
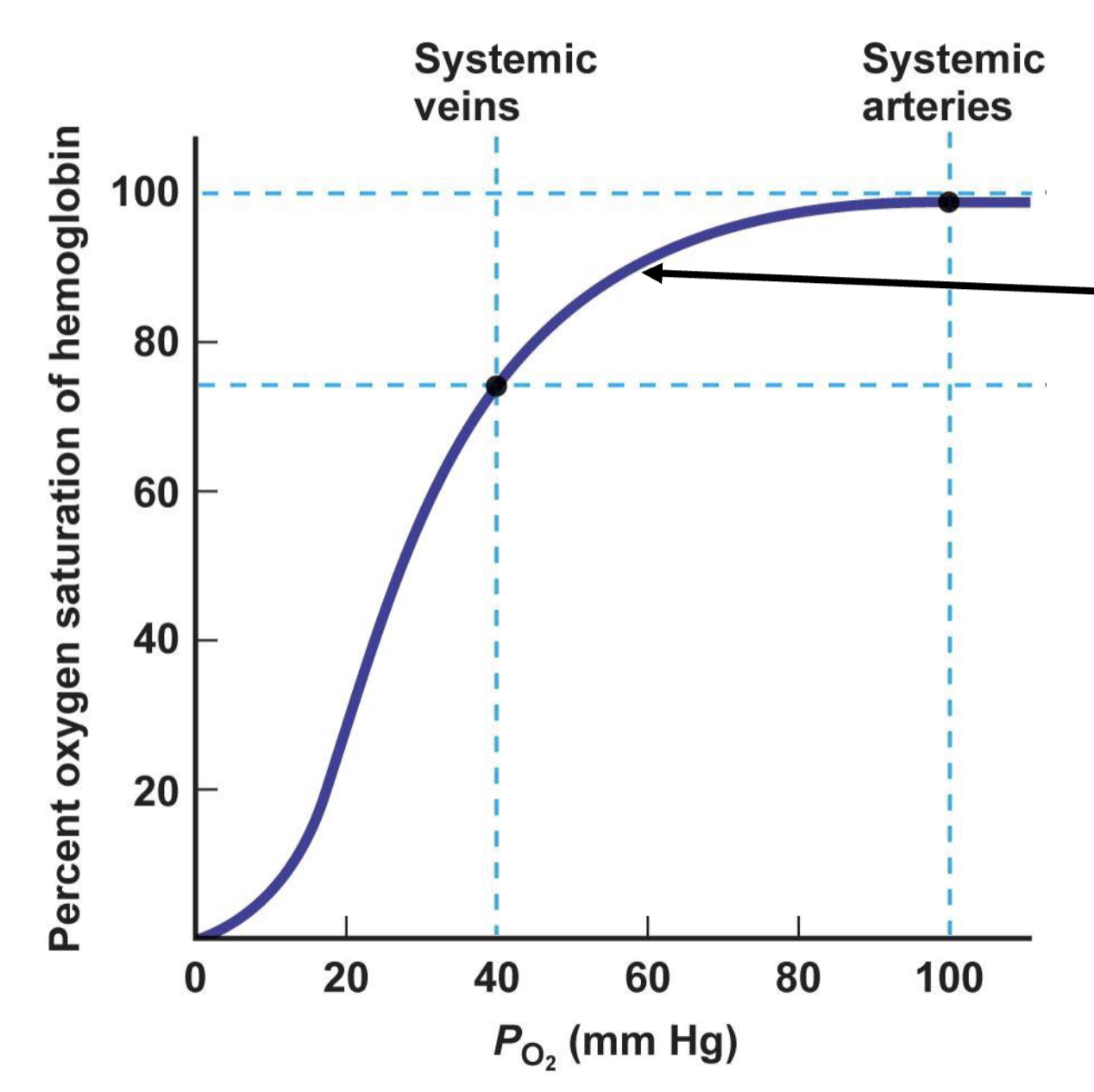
describe the oxyhemoglobin saturation curve
relationship is S-shaped
if atmospheric PO2 levels fall, Hb is still mostly saturated, so blood leaving alveoli is still largely oxygenated
as tissues become more active and use more O2, Hb can deliver increasing quantities of O2
chemoreceptors kick in to adjust the curve when it drops below 60
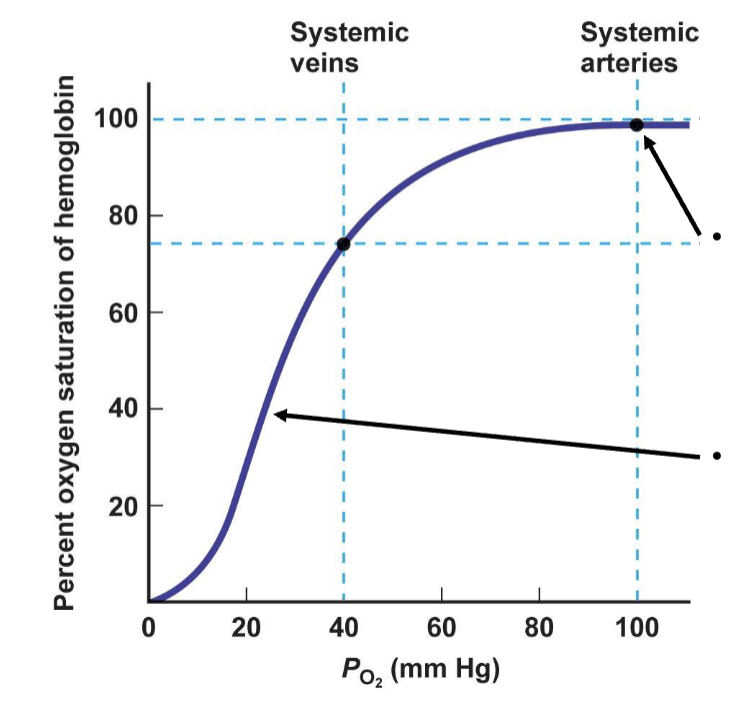
describe O2 delivery during exercise
as O2 use increases in active tissues (increased metabolism), PO2 in those tissues can drop to 20 mm Hg
percent oxygen saturation of hemoglobin drops
percent of oxygen unloaded drops
what are the different factors affecting O2-Hb Binding
traits of the internal environment impact the affinity of Hb to bind to O2 and help to intrinsically meet the body’s changing O2 demand
increasing affinity means higher %HbO2 at a given PO2
decreasing affinity means lower % HbO2 at a given PO2
what are factors that affect the percent saturation of Hb
PCO2
pH
temperature
2,3-BPG (metabolism biproduct)
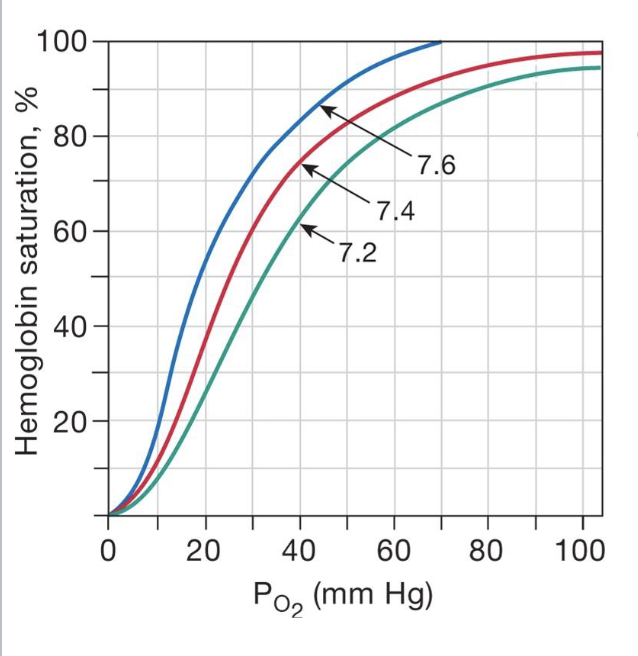
describe the effect of pH in the blood with regard to the Bohr Effect
causes for low pH
increase in muscle activity forces muscles to use anaerobic respiration, which results in an increase in lactic acid, H+, and C2
decrease in pH due to increased metabolism causes a right shift for the saturation of a PO2, meaning that at a given pressure, there is less hemoglobin saturation
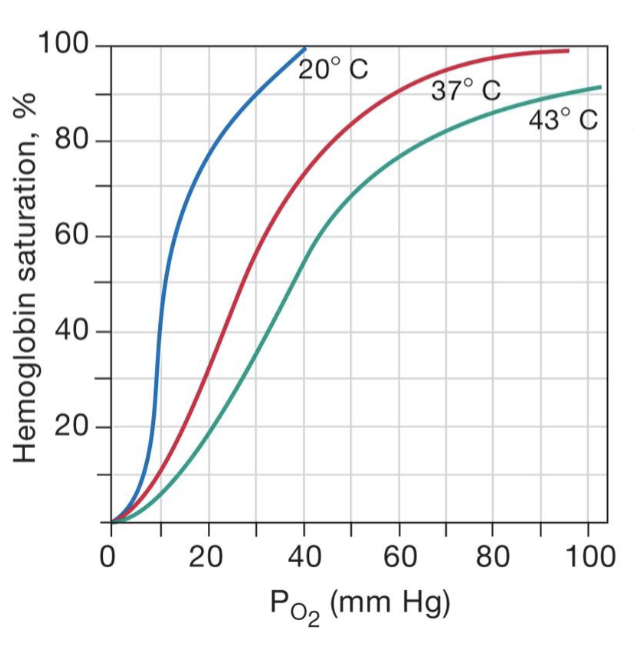
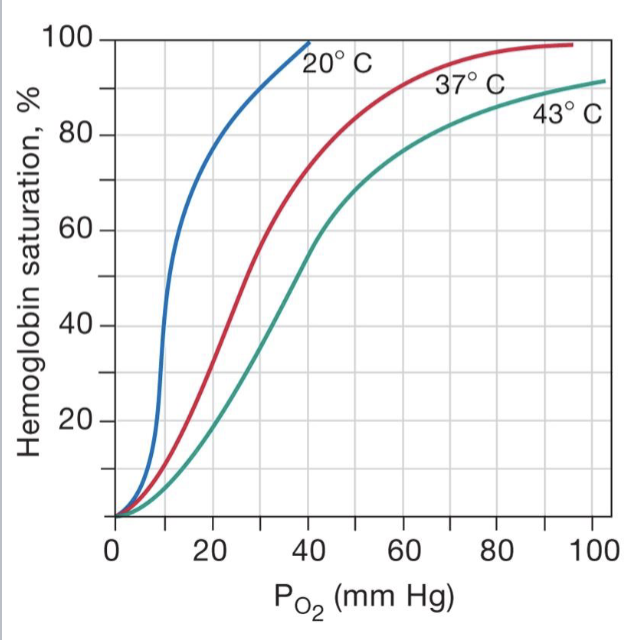
describe the effect of temperature in the blood
causes for increased temperature come from increased muscle activity, warming muscles up, and signals to body that they need more O2
there is more hemoglobin saturation (more O2) at lower temps
there is less O2 (hemoglobin saturation) at higher temps due to increased activity and increased heat/acidity
describe the effect of CO2 in the blood with the carbamino effect
at high PCO2, CO2 binds reversibly to Hb to form a carbaminohemoglobin molecule
causes for increased CO2 come from increased muscle activity that forces muscle respiration to increase which results in an increased CO2; or problems with ventilation
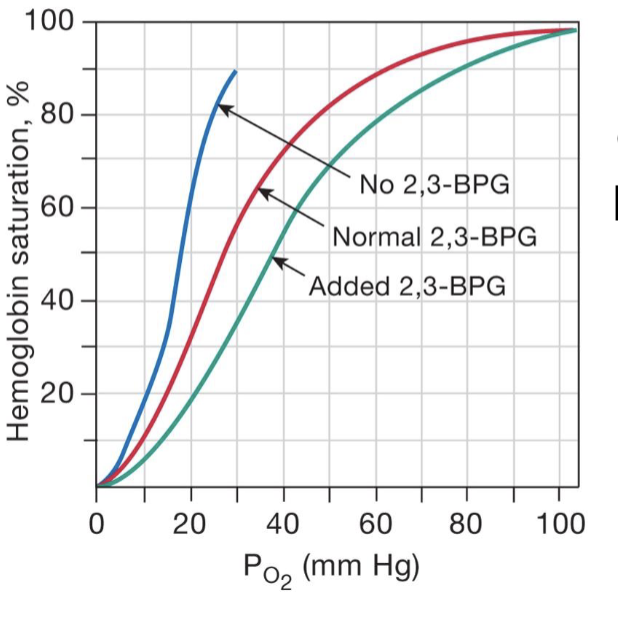
describe the effect of 2,3-BPG (DPG) in the blood
2,3-bisphosphoglycerate (an intermediary of the glycolysis pathway)
causes for an increase in BPG
chronic hypoxia from living at high altitudes
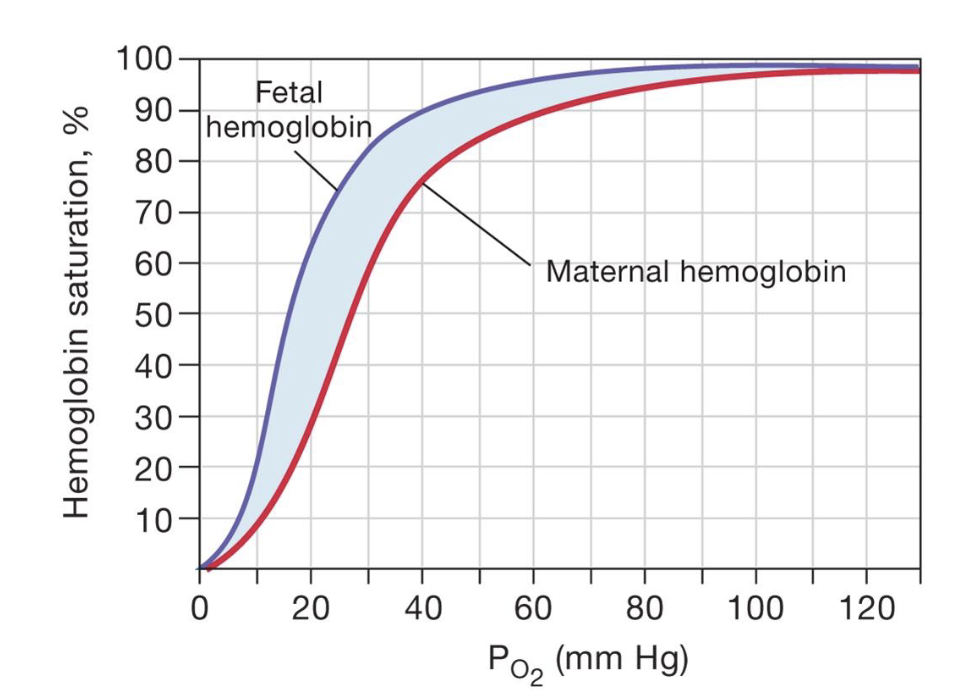
describe fetal vs maternal Hb
the fetal hemoglobin has a higher hemoglobin saturation which is why it is able to get O2 from the mom
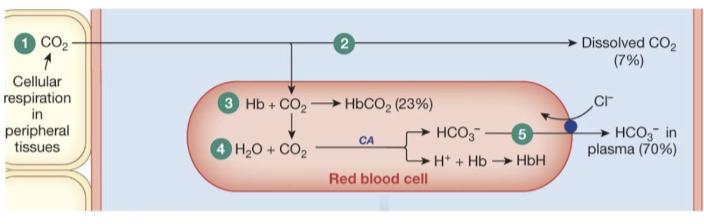
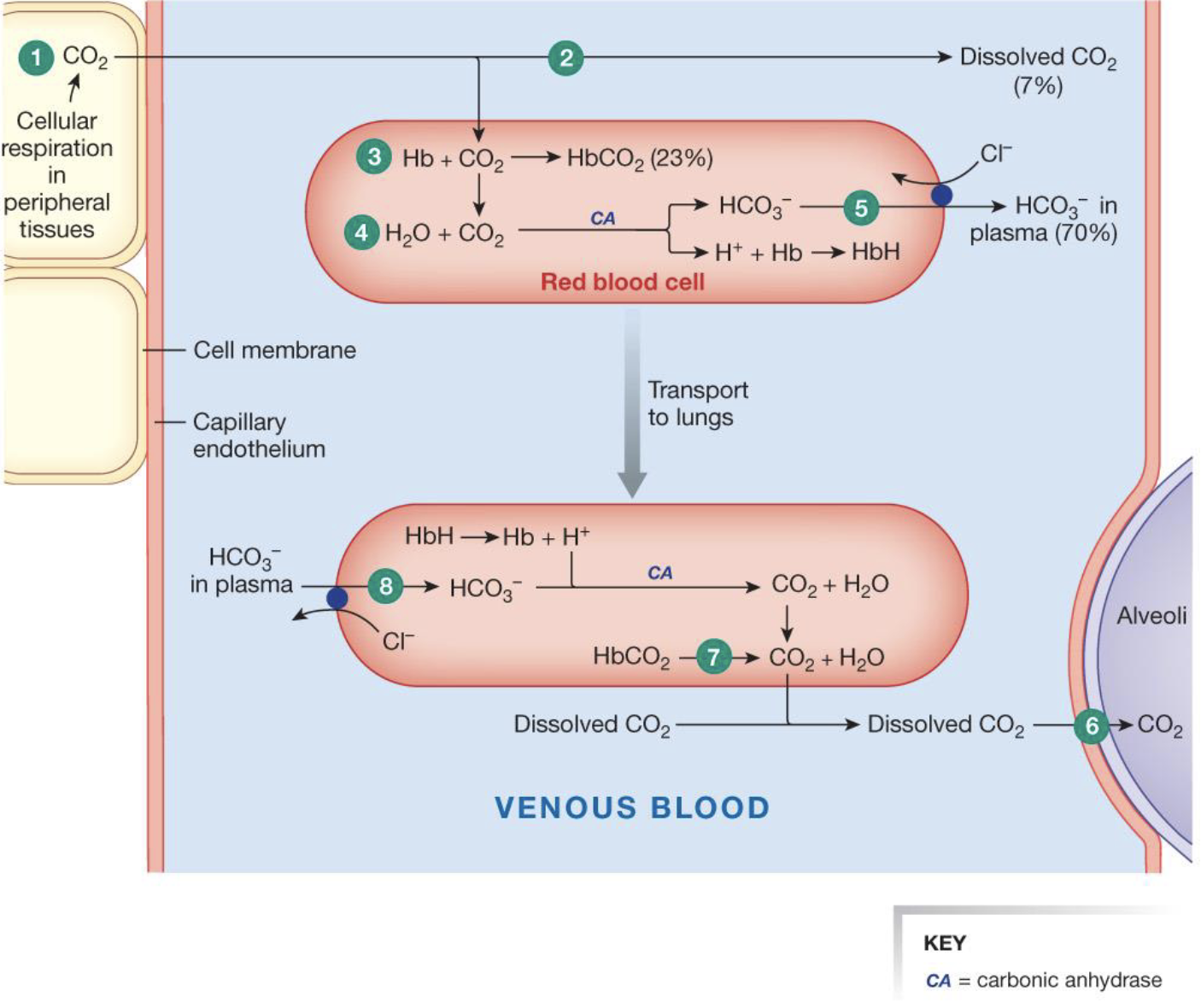
describe CO2 transport from the tissues to the blood
CO2 diffuses out of the cells into systemic capillaries
only 7% of the CO2 remains dissolved in plasma
nearly a fourth of the CO2 binds to hemoglobin, forming carbaminohemoglobin
70% of the CO2 load is converted to bicarbonate and H+ (hemoglobin buffers H+)
HCO3- enters the plasma in exchange for Cl- (the chloride shift)
what is HbH
hemoglobin bound to H+ that acts as a buffer to changes in pH
what is HbCO2
carbaminohemoglobin; hemoglobin bound to CO2
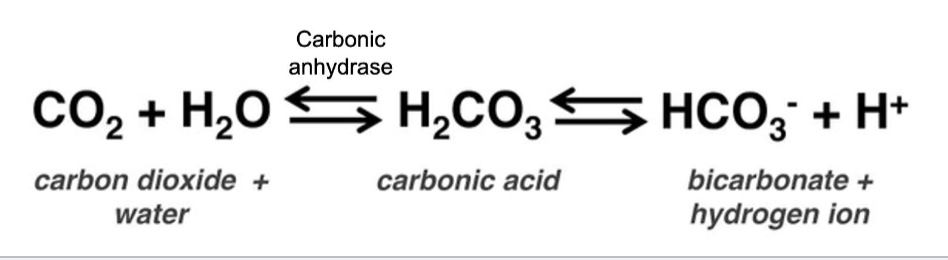
MEMORIZE this equation and know what to use it
when the solution is basic, right shift to free up H+
when the solution is acidic, left shift to convert to CO2
describe CO2 transport from blood to lungs
CO2 diffuses out of cells into systemic capillaries
only 7% of the CO2 remains dissolved in the plasma
nearly a fourth of the CO2 binds to hemoglobin, forming carbaminohemoglobin
70% of the CO2 load is converted to bicarbonate and H+ (hemoglobin buffers H+)
HCO3- enters the plasma in exchange for Cl- (the chloride shift)
at the lungs, dissolved CO2 diffuses out of the plasma
by the law of mass action, CO2 unbinds from hemoglobin and diffuses out of the RBC
the carbonic acid reaction reverses, pulling HCO3- back into the RBC and converting it to CO2
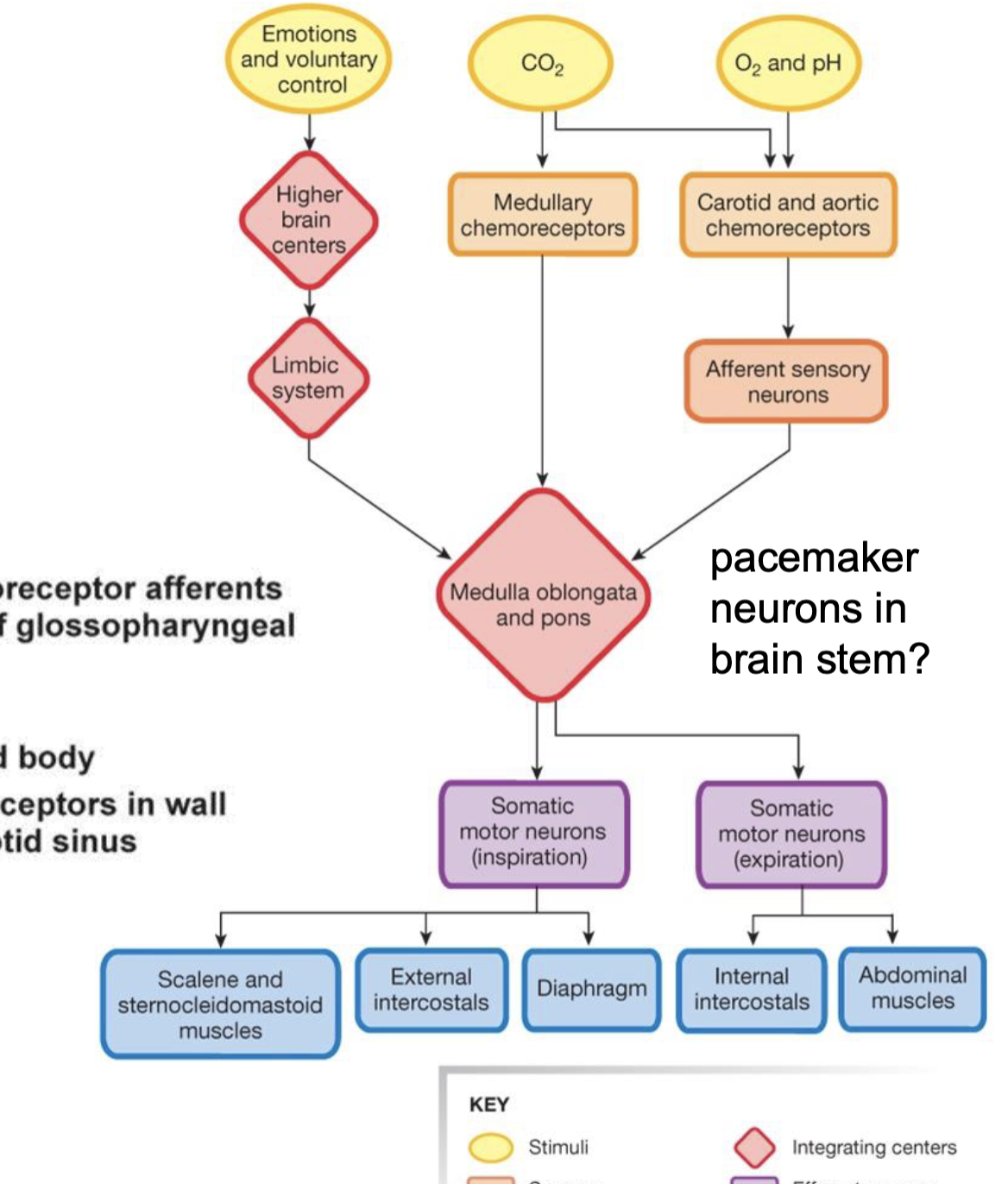
memorize this chart for the neural control of respiration
memorize this diagram for the chemoreceptor control of ventilation
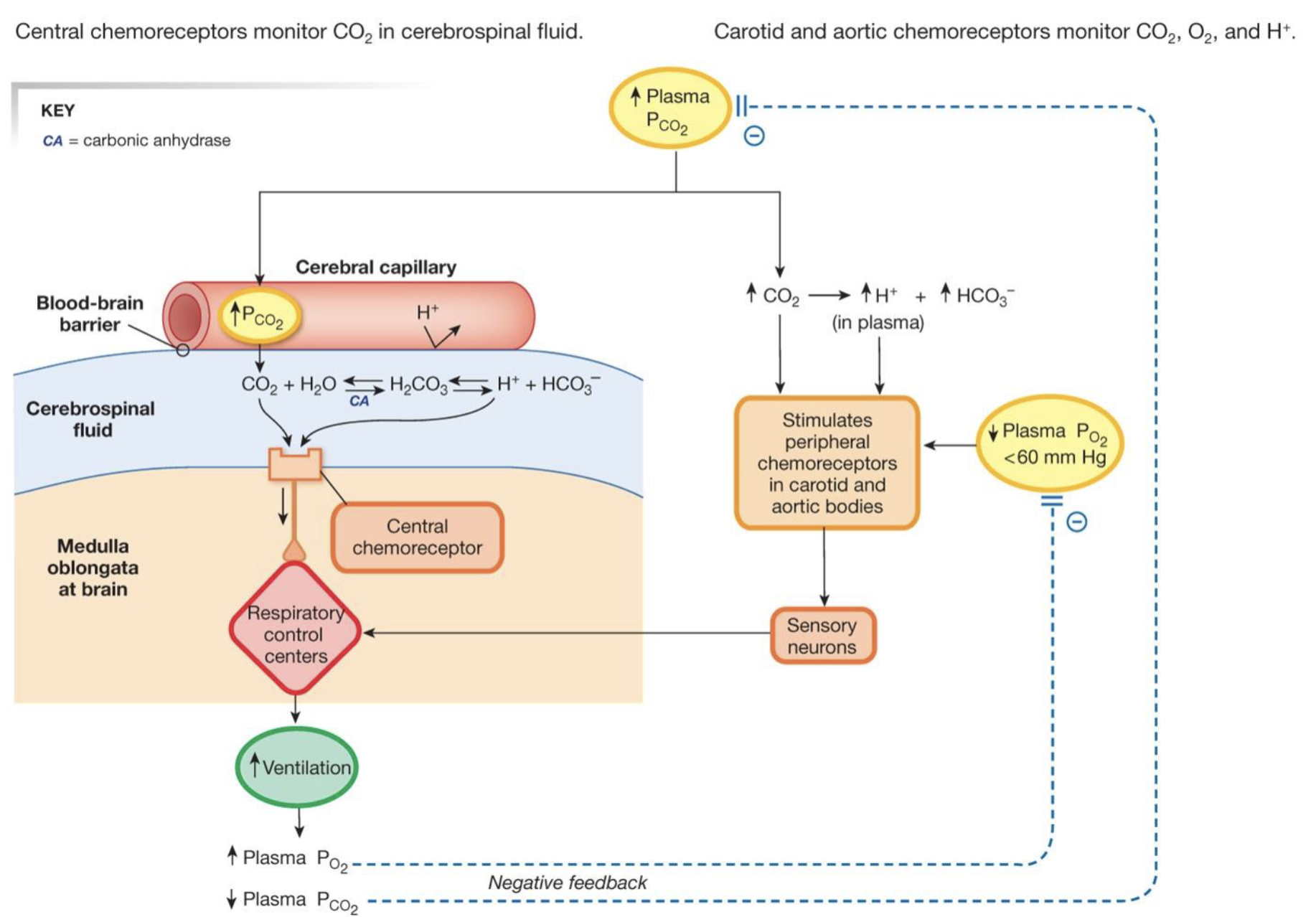
what do central chemoreceptors monitor
CO2 in the cerebrospinal fluid
what do carotid and aortic chemoreceptors monitor
CO2, O2, and H+
describe the hypoxic drive and the O2-Hb curve
when the PO2 is less than 60, it stimulates an increase in ventilation
this is important because it is right before the large drop in hemoglobin saturation at lower PO2
this is when the peripheral chemoreceptors kick in
describe lung compliance
the ability of the lung tissue to stretch and expand
describe lung elasticity
ability of the lung to shrink down and empty of air
what two factors affect the total arterial O2 content
oxygen dissolved in plasma
oxygen bound to Hb
what factors influence oxygen dissolved in plasma
composition of inspired air
alveolar ventilation
oxygen diffusion between alveoli and blood
adequate perfusion of alveoli
what factors influence alveolar ventilation
rate and depth of breathing
airway resistance
lung compliance
what factors influence the oxygen diffusion between alveoli and blood
surface area
diffusion distance (membrane thickness and the amount of interstitial fluid)
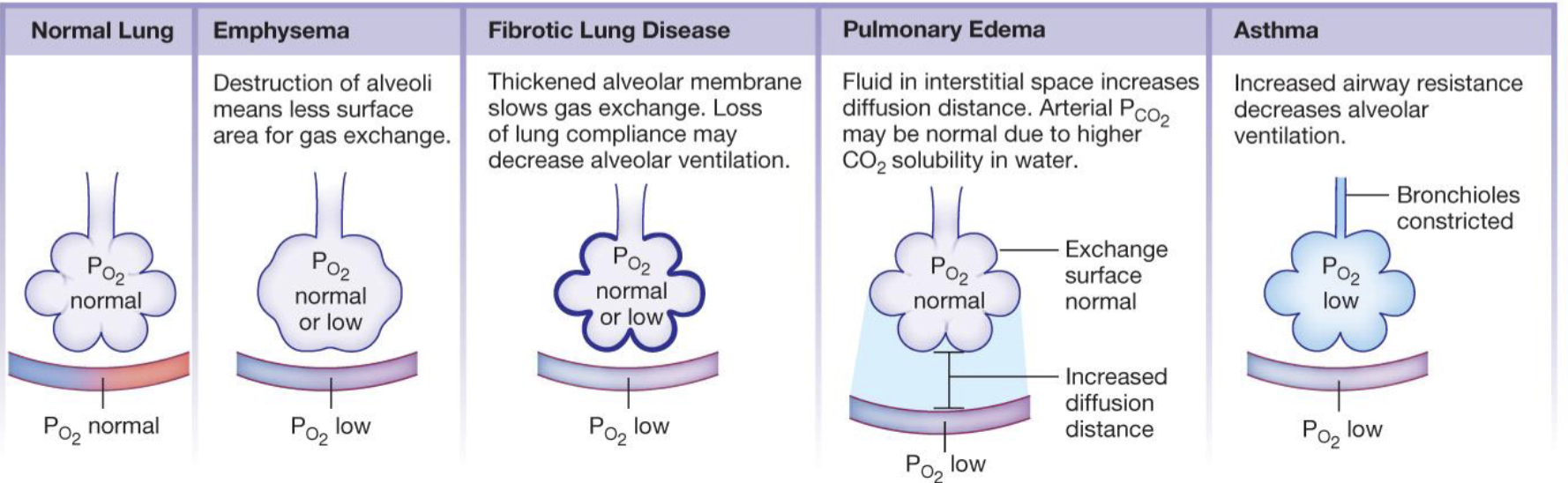
what are the different pathologies that cause hypoxia
emphysema (destruction of alveoli means less surface area for gas exchange)
fibrotic lung disease (thickened alveolar membrane slows gas exchange and loss of lung compliance may decrease alveolar ventilation)
pulmonary edema ( fluid in the interstitial space increases diffusion distance and arterial PCO2 may be normal due to higher CO2 solubility in water)
asthma (increased airway resistance decreases alveolar ventilation)
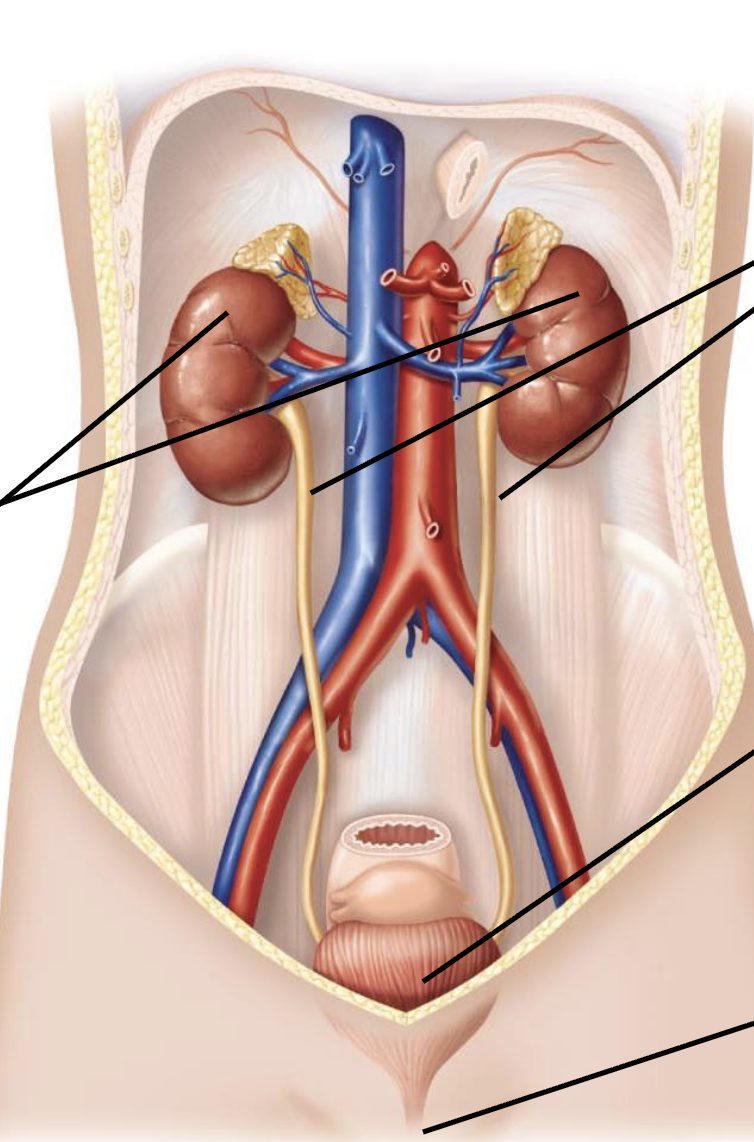
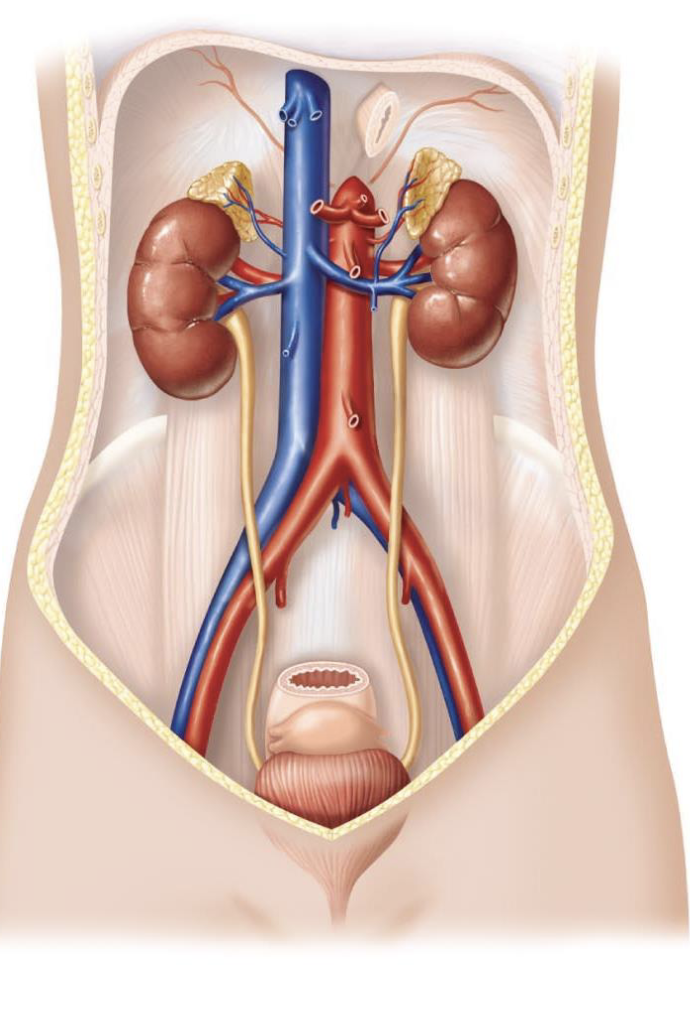
what are the parts of the urinary tract
paired ureters (carry urine from kidneys to bladder)
bladder (temporarily stores urine)
urethra (carries urine from bladder to the outside of the body)
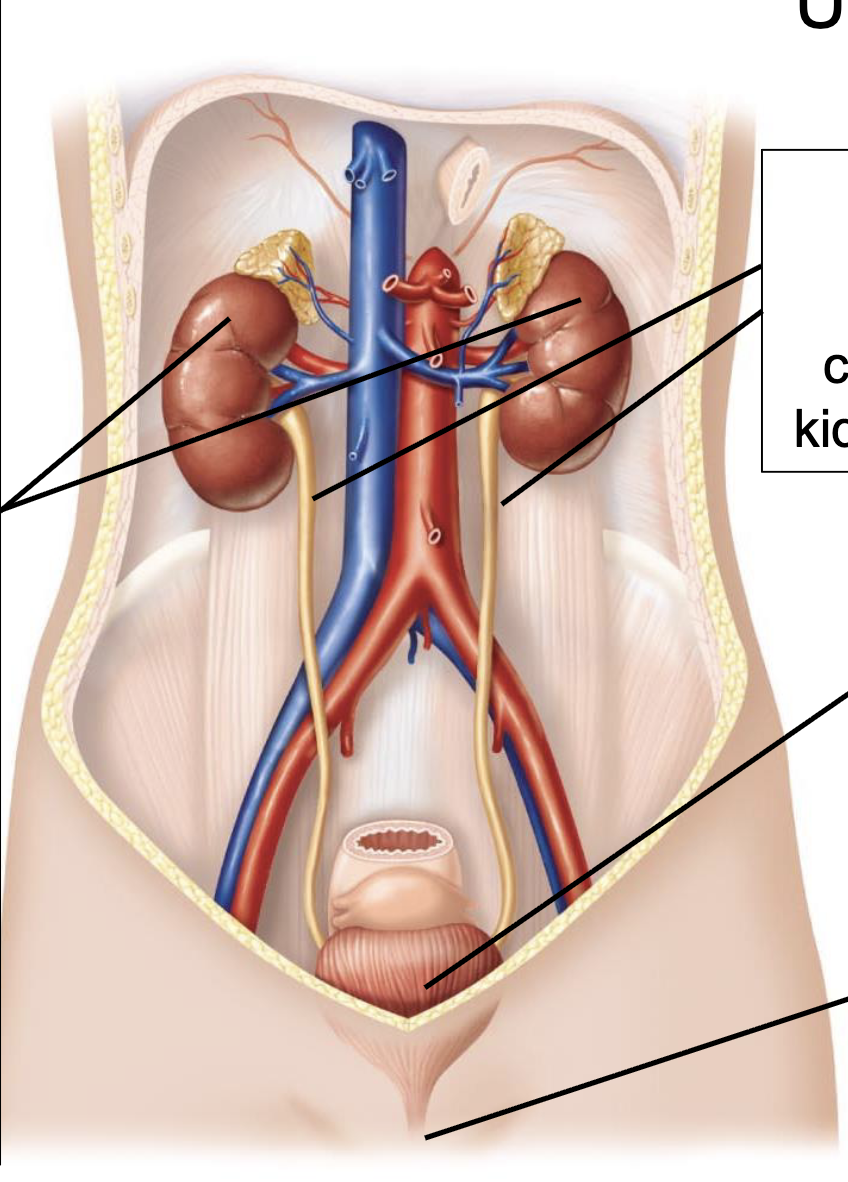
describe the paired kidneys
remove metabolic wastes and toxins (constantly filtering the blood in homeostatic range)
long term regulation of pH of the plasma
regulate osmolarity of solutes in body fluids (alter concentration and water composition to regulate blood pressure by adding/removing liquid)
regulate plasma volume
stimulate red blood cell production (sythesize and release a hormone called EPO that stimulates the production of more RBCs)
activate viatamin D3
synthesize glucouse from non-carbohydrates (gucogenesis)
release/degrade hormones (renin that is an enzyme that activates a hormone cascade)
describe how the kidneys maintain homeostasis
through a massive filtration rate
filter ~200 liters of blood daily
total plasma volume in an adult is 3-5 liters
filters entire plasma volume ~60x per day
this high filtration rate (glomerular filtration rate [GFR]) is essential for rapidly clearing wastes and precisely regulating bodily fluids (can be used to assess kidney function as a common clinical marker)
![<ul><li><p>through a massive filtration rate</p></li><li><p>filter ~200 liters of blood daily</p><ul><li><p>total plasma volume in an adult is 3-5 liters</p></li><li><p>filters entire plasma volume ~60x per day</p></li><li><p>this high filtration rate (glomerular filtration rate [GFR]) is essential for rapidly clearing wastes and precisely regulating bodily fluids (can be used to assess kidney function as a common clinical marker)</p></li></ul></li></ul><p></p>](https://assets.knowt.com/user-attachments/41bf7ef7-48ee-4eae-8153-ad545c2d53a3.png)
how can an individual survive with only 1/3 of one kidney being functional
not all of the kidneys work at the same time
illustrates the functional reserve of the kidney itself as they don’t work at 100% capacity all of the time and have the ability to ramp up the function
describe how the kidneys control blood volume and regulate plasma volume
add or remove the solute content to regulate the blood volume
add or remove water content of the blood to regulate the plasma volume
primary mechanism for long-term control of mean arterial blood pressure
through regulation of Na+ and water
describe how the kidneys regulate osmolarity
the kidneys maintain plasma osmolarity in a tight range (290-300 mOsm)
through regulation of water excretion, primarily through the action of antidiuretic hormone (ADH)
describe how the kidneys regulate the plasma pH
primary organ for long-term acid-base balance
excretion of H+ (fixed acids)
reabsorbtion and synthesis of HCO3- (can either pick up a proton or give up a proton depending on the direction of the pH disruption)
describe how the kidneys regulate ion balance
controls plasma concentration of key electrolytes
Na+, K+, Ca2+
describe the metabolic waste that is excreted by the kidneys
urea (nitrogenous waste from amino acid metabolism)
uric acid (from nucleic acids
creatinine (from phosphocreatine metabolism in skeletal muscles)
more muscles, more creatine
if high, it means that the kidneys are not filtering out at the rate that they are supposed to)
plasma creatine is a common clinical marker for estimating GFR but it is not the most accurate because someone who works out a lot or has more muscle mass is going to have higher amounts of creatine
describe the xenobiotics that the kidneys excrete
drugs
environmental toxins
food additives (food dye)
what are the different endocrine and metabolic functions of the kidneys
stimulation of red blood cell production
activation of vitamin D3
release/degrade hormones
gluconeogensis
ammonia synthesis
describe stimulation of RBC production as an endocrine and metabolic function of the kidneys
the kidneys synthesize and secrete the hormone erythropoietin (EPO) that makes more RBCs in response to low oxygen levels
describe the activation of vitamin D3 as an endocrine and metabolic function of the kidneys
carries out final hydroxylation step to convert inactive vitamin D into clacitriol
describe the release/degrade of hormones as an endocrine and metabolic function of the kidneys
major site for hormone degradation
releases the enzyme Renin, which activates the RAS system to raise blood pressure
describe gluconeogenesis as an endocrine and metabolic function of the kidneys
makes glucose from non-carbohydrate sources (amino acids) during prolonged fasting
describe ammonia synthesis as an endocrine and metabolic function of the kidnesy
kidneys synthesize ammonia (NH3) from glutamine, which acts as a urinary buffer to trap and excrete H+
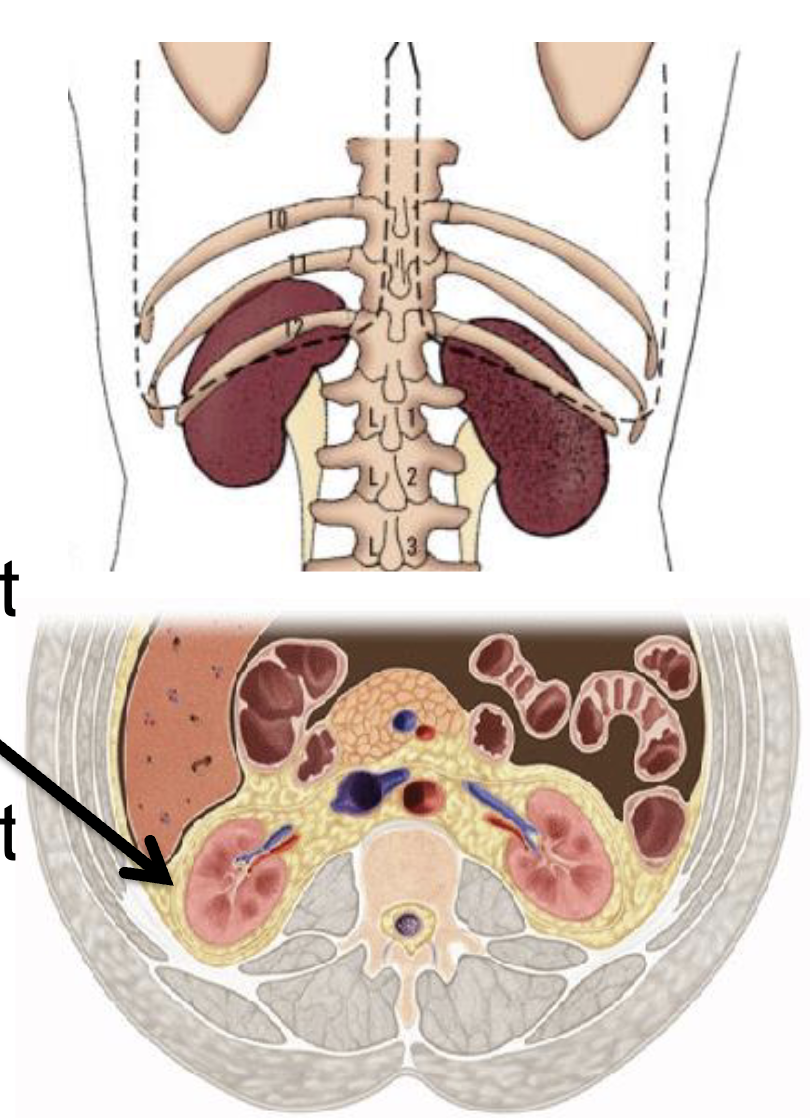
give a description of the kidneys
about the size of your clenched fist
posterior to the abdominal wall (behind ribs to back)
partially protected by ribcage (bottom floating ribs)
surrounded by perirenal fat to absorb mechanical shocks
receive 20-25% of CO but are only 0.4% of body mass (very high rate of blood flow!!)
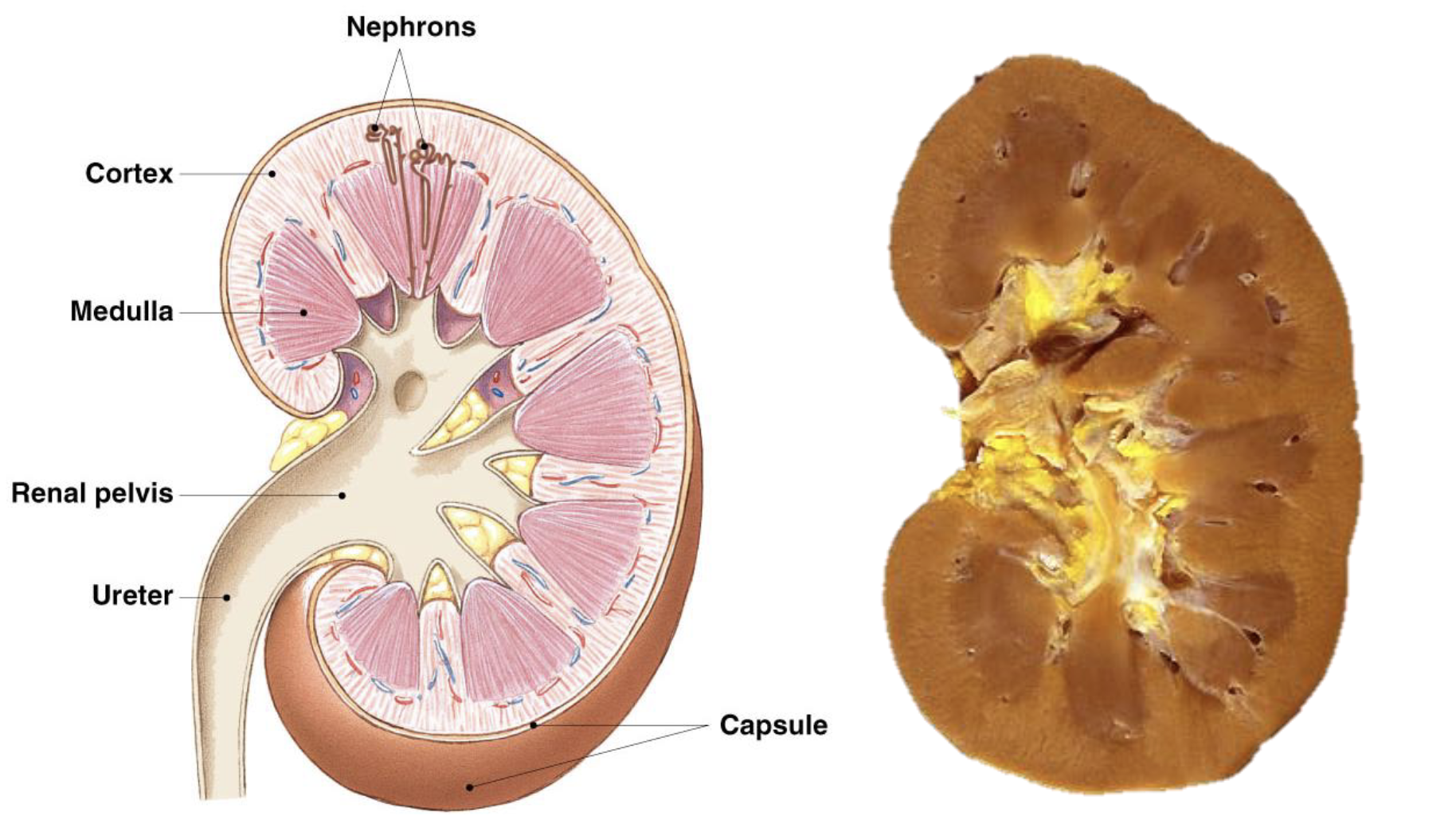
what is the morphology of the kidneys
cortex
nephrons
cortical nephrons in the cortex and have the most expression
Juxtamedullary nephrons in the medulla are fewer but play an important role
medulla (high salt content that help with purification, concentration, or very dilute urine)
renal pelvis where urine exits the collecting duct
ureter that sends the urine to the bladder
what are the four processes that urine forms through
filtration
reabsorption
secretion
excretion